
Abstract
Under-reporting tobacco consumption is common, although there is lack of evidence whether under-reporting is associated with health risk perception. In this study, smoking topography from 110 smokers was recorded over 24 hours, aiming to capture a representative average of smoking behaviour. Participants significantly under-reported the duration of secondary exposure, and there was a significant interaction between self-report distortion type and risk perception. Analysis showed that smokers under-reporting puff number declared perceiving significantly less susceptibility to acquiring airway diseases, which is correlating significantly with the level of under-reporting. The present findings may suggest that under-reporting smoking behaviour has psychological functions beyond achieving social desirability.
Introduction
The World Health Organization (WHO, 2008) attributed nearly 100 million deaths to tobacco smoke in the 20th century, which is projected to increase to 1 billion deaths by the end of the 21st century. It is estimated that 500 million people who are alive today will die because of tobacco consumption and annual death toll may increase up to 8 million people by 2030 if effective tobacco control efforts are not implemented (WHO, 2008). A general consensus is that the majority of these deaths will occur in the developing world which is hosting around 80 per cent of world’s smoking population, and where multi-dimensional tobacco control efforts are not yet well established (WHO, 2008). This projection specific to developing countries may be an indirect result of increasingly strict tobacco control policies implemented in developed countries creating a positive effect (Etter, 2010; Gottlieb et al., 2004; Jarvis et al., 2003; Mendez and Warner, 2004; Peterson et al., 2005; Thun et al., 2012), which may in return influence international cigarette companies to adopt more competitive strategies in developing countries. This may be a particular concern for younger populations living in developing countries (Baška et al., 2009). Therefore, studying smoking behaviour in developing countries may have a higher impact for global tobacco control and contribute positively to tailoring treatment modalities in accordance with local cultures, as recommended by the WHO (2008: 30). The data in this study were collected in Turkey (listed among the developing countries by the Organisation for Economic Co-operation and Development (OECD) from 1997 onwards), aimed at contributing to understanding of smoking behaviour in a country with a long tradition of tobacco consumption to such extent, giving way to the expression: ‘smoking like a Turk’.
Understanding psychological processes related to smoking behaviour is an important dimension of tobacco control, and one of the important unknowns in health psychology is whether risk perception is influenced by formation of habitual smoking behaviours. Studies investigating the factors influencing risk perception in daily smokers have considered the effect of social desirability, whereby responding positively to meet clinicians’ expectations is proposed to be one of the key determinants (Vogt et al., 2010). Under-reporting exposure levels may influence associated health risks to be discounted; these may decrease the efficacy of cessation interventions and consequently may lead to relapse in the long term. This potential link is investigated by few studies showing that risk denial increases overall utility obtained from illicit drugs and leads to hyper-scrutiny of readily available preventive information, such that individuals with higher levels of risk denial require more information to consider the effects of illicit drugs as harmful relative to individuals with lower levels of risk denial (Peretti-Watel, 2006). Additional requirement for more information could be interpreted in tandem with smokers’ general tendency to seek more information about the constituents of tobacco products they are consuming before they can evaluate their risk levels accurately (Cummings et al., 2004). Similarly, smokers are shown to consider lower frequency of smoking as less harmful to such extent that it reduces willingness to quit smoking (Peretti-Watel et al., 2007). In nationwide surveys, it was shown that smokers optimistically believe that their risk for acquiring lung cancer (Weinstein et al., 2005), as well as suffering from heart attacks and stroke (Strecher et al., 1995) is lower relative to other comparable smokers. Previous studies showed that only when smokers’ self-assessment of their exposure levels (in smoking frequency and total years of smoking) converge to their knowledge of a stereotypical smoker’s exposure level, they are more likely to hold accurate risk perceptions about any potential negative health consequences of smoking (Hahn and Renner, 1998).
The other side of this potential interaction is related to formation of behavioural habits during daily smoking. The use of the word ‘habit’ as a lay term within the context of cigarette smoking usually refers to descriptive aspects of smoking behaviour; such as the number of cigarettes smoked daily (Peixoto et al., 2005). However, in psychology, habits are defined as learned sequences of acts that have become automatic responses to specific cues (Verplanken and Aarts, 1999). As in Pavlovian conditioning, when an individual has enough chance for repetition, the cues may also carry enough power to motivate actions as they signal the presence of an opportunity to obtain the associated reward (Wood and Neal, 2007). Thus, rewarding behaviour becomes habitual through repetition where its tactile aspects gradually become unconscious (Tarr, 2008). In the case of cigarette smoking, although the craving for nicotine (which is assumed to create the immediate urge of lighting up a cigarette) may become temporarily conscious and reach awareness as an intrinsic motivator, the behaviours performed prior to and during smoking may remain to be unconscious, by becoming/remaining habitual. This lack of awareness for the level of exposure, as a result of gradual habit formation, may be important to understand why health risk perception is widely distorted in daily smokers (Strecher et al., 1995).
The present research investigates the habitual aspects of cigarette smoking, at the first level by comparing self-reported smoking behaviour with an objective measure of daily smoking activity as recorded by the CreSSmicro topography device. If daily smoking adheres to principles of habit formation: (1) daily smokers would be inaccurate in self-reports for the key features of smoking behaviour (e.g. smoke time, number of puffs and inter-puff interval (IPI)) and (2) self-reports would not be more accurate in smokers who smoke more frequently and for a longer time (by comparing heavy smokers (those who smoke 15 or more cigarettes per day) with light smokers (those who smoke less than 9 cigarettes per day); for the definitions see (Okuyemi et al., 2002)). At the second level of the present investigation, the relationship between self-report distortions (i.e. the difference between self-reported behaviour and CreSSmicro recordings) and perceived health risks is investigated. Although there is no directly comparable study in the literature, it is plausible to propose that self-report distortions may be related to underlying health concerns. Therefore, an a priori prediction that (3) self-report distortions in puff number, as a more direct predictor of exposure levels relative to IPI (see the section ‘Methods’), would be related to perceived health risks is tested. If this prediction is supported, assessment of self-report distortions against objective measures obtained from portable topography devices could be implemented in smoke cessation interventions to probe underlying subconscious attitudes about perceived health risks, whereby smoking behaviour is experienced more consciously, allowing cognitive distortion mechanisms to be targeted by clinical/psychological interventions. These in return may increase efficacy of smoke cessation interventions.
Methods and procedures
This study was approved by the Ethics Committee of the Marmara University Medical School, Istanbul, Turkey. Informed consent was taken from all participants orally during the phone screening stage, and in writing at the beginning of the first laboratory visit of the experimental protocol. All experiments were carried out in accordance with the terms of the ethical approval obtained for this study.
Participants
A purposive sample of cigarette smokers was recruited through advertisements in the local press as well as using flyers and posters on bulletin boards. Inclusion criteria consisted of being a regular smoker (at least five cigarettes daily and for at least 3 months continuously) and aged 18–65 years. Exclusion criteria included self-reported history of lung and heart disease and pregnancy.
Procedures
A telephone screening interview was conducted among people who responded to the advertisements, flyers and brochures, to assess their eligibility. Eligible subjects were then invited to the laboratory for two visits, 24 hours apart. All of the testing sessions took place between 3:00 p.m. and 8:00 p.m. (in order to collect representative tissue, urine and cigarette butt samples; data not reported here). During the first visit, participants gave informed consent and responded to questions assessing various aspects of their smoking behaviour. They were also asked to make an estimation regarding topographical features of their smoking behaviour descriptively such as how long it takes to smoke a single cigarette, how many puffs they would take on average and how much time passes between puffs (i.e. estimated IPI). Secondly, they were asked to rate their subjective accuracy for their self-reports (also see the section ‘Results’), and when not sure, participants were asked in which direction they think their self-reports would differ from the recordings of a portable topography device (by choosing between three categorical labels after making an explicit numeric estimation of topographical parameters: accurate, over-reported or under-reported).
After this, participants completed a brief questionnaire on cigarette smoking and associated health risks. This questionnaire included items assessing participants’ history of smoking, the number of previous quitting attempts and duration of abstinence and intentions to attempt quitting in the near future. The health concerns which are the main focus of this article were particularly assessed by four items (i.e. worry about health risks, and perceived susceptibility to acquiring airway diseases (adapted from Shahab et al. (2011)), asked twice on different occasions: first items negatively framed, the second items framed negated positively). Example items are as follows: (1) how worried are you about the effects of smoking on your health? and (2) How likely do you think you will acquire airway diseases because of cigarette smoking? The participants responded to all questionnaire items by making a rating on a 1–7 Likert scale, with higher ratings indicating greater perceived health risk and/or worry. Following this, participants were given a CreSSmicro device which measures smoking topography and stores the information in its memory. Participants were asked to use this portable topography device for the following 24 hours, and they were asked to smoke all of their cigarettes through this device so that a valid average of their smoking behaviour can be recorded during this time interval. Thus, measures related to smoking topography in this article are based on the average of all cigarettes smoked using the CreSSmicro device for 24 hours.
At the end of the first interview, participants were asked to smoke their first cigarette under the observation of the researcher so that any difficulties in using the topography unit could immediately be addressed by the researcher (E.P.). All the participants used the CreSSmicro device for 24 hours. CreSSmicro devices were collected from the participants at the end of the second interview, and all the stored data were transferred to a computer for further analysis. The use of the CreSSmicro devices was verified by inspection of the topographical recordings from all the cigarettes the participants reported smoking during 24 hours. Additionally, the number of recordings from the CreSSmicro devices is checked against the number of cigarette butts the participants returned on their second visit to the laboratory (these were further analysed for technical specifications of the ventilation holes in the cigarette butts for a separate investigation independent of the present one).
Estimated smoke-related constituent exposure
Total amount of smoke exposure a person gets from a single cigarette in a closed hypothetical environment is a combination of direct and indirect exposure to constituent chemicals. One of the primary parameters defining the level of direct exposure to cigarette smoke is the number of puffs taken from a cigarette by the smoker. On the other hand, second-hand smoke (SHS) is defined as the level a non-smoker is being indirectly exposed to cigarette smoke due to being in the same closed environment with smokers (Öberg et al., 2011). One of the primary parameters for defining the level of SHS is the duration of time a non-smoker spends in the same closed environment with smokers. Applying these principles to someone who is smoking alone in a closed environment, the smoker’s total exposure to cigarette smoke (including both direct and indirect exposure) could be theoretically formulated by the simplified equation below

In this formula, (PN) is the number of puffs, describing the frequency at which smokers are directly exposed to constituent chemicals in smoke. During consumption of a single cigarette the number of IPIs is 1 less than the number of puffs (PN – 1). IPI is the total duration of exposure to SHS between each puff only in situations where a single person is smoking alone in a closed environment (for outdoor smoking, SHS may be negligible). Puffing and SHS would have different exposure severity coefficients such that
Statistics
All the statistical analysis was carried out by using Statistical Package for the Social Sciences (SPSS) 20.0. Appropriate general linear models (GLMs), independent samples t-tests and parametric correlations were used. Descriptive statistics were used to report sample characteristics. T-tests were used to compare the average CreSSmicro recordings with self-reports. The GLM was fitted in order to investigate the interaction between health risk perception and puff number/IPI distortion profiles (e.g. Group 1: both puff number and IPI under-reported (also see Figure 1); Group 2: puff number under- but IPI over-reported; Group 3: puff number over- but IPI under-reported; Group 4: both puff number and IPI over-reported). T-tests and parametric correlations were used in post-hoc analysis in order to identify GLM interactions.
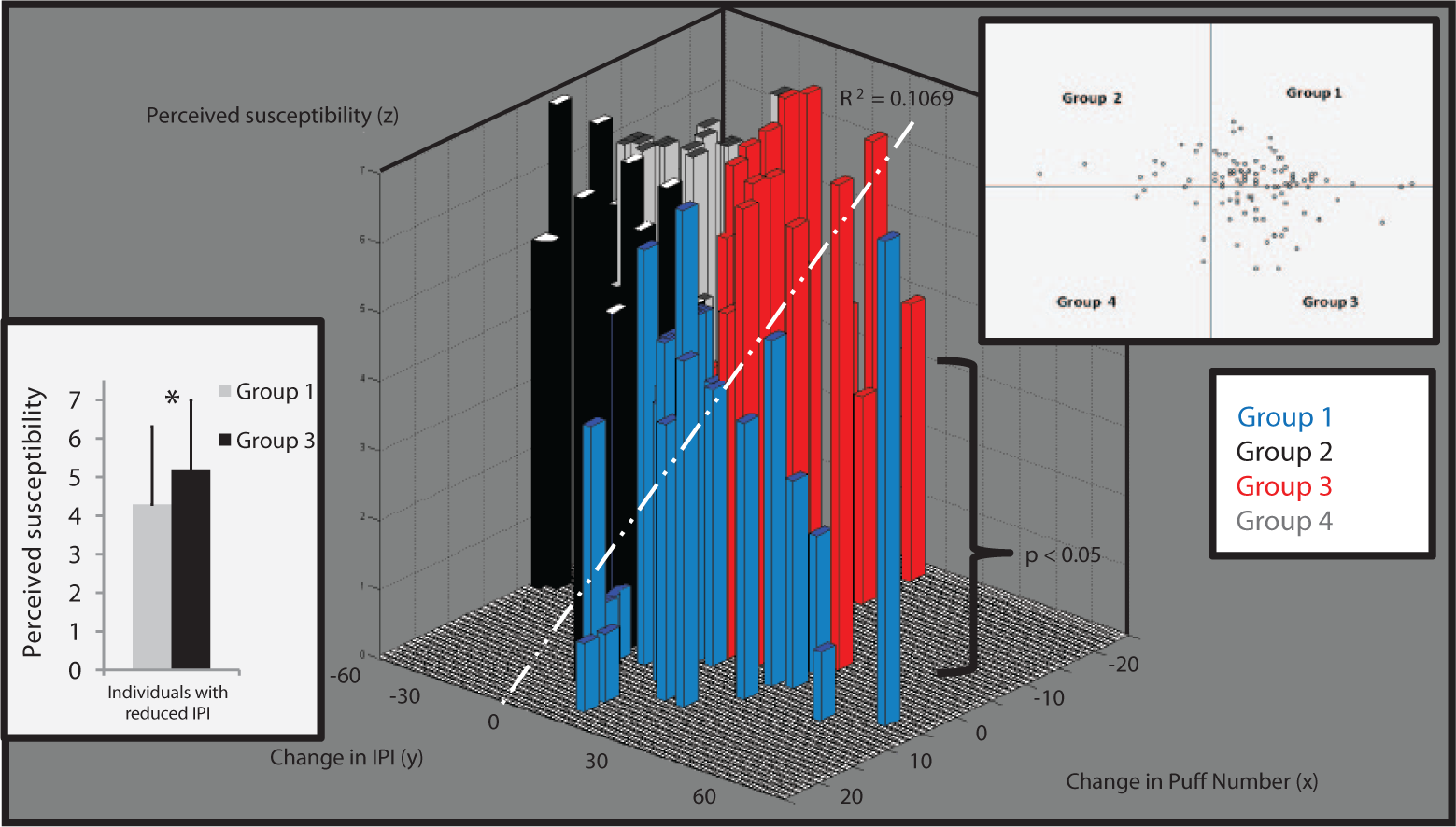
Three-dimensional scattered bars showing the distribution of the sample population (scatter plot shown at the top right corner). Heights of bars show ratings for perceived susceptibility to acquiring airway diseases (Z-axis). Positive values on bipolar X- and Y-axes indicate under-reporting. Colour of bars refers to grouping information. Group 1 (in blue: puff under-reporting) reported significantly lower susceptibility to acquiring airway diseases relative to Group 3 (in red: puff over-reporting; p < 0.05; also in bottom left corner). Linear regression line shows a significant negative correlation between perceived susceptibility and degree of under-reporting puff numbers in Group 1 (p = 0.01).
Results
Participants
A total of 110 cigarette smokers (59.1% males, n = 65) participated in the study. The mean age for the population is 28.15 years (±9.40). The average number of cigarettes smoked per day was 15.79 (±6.21), and on average participants had smoked their current brand for 53.50 months (±52.89). Although participants smoked less number of cigarettes than they said they would using the CreSSmicro device (mean 11.96± 4.7, t = 5.131, df = 217, p < 0.001), smoking frequency difference was to a lesser degree after controlling for salivary cotinine levels between visits 1 and 2 (t = −2.140, p = 0.034; full biomedical exposure data for this cohort are reported elsewhere (paper in press)). More than half of this population (53.6%) were heavy smokers who smoked more than 15 cigarettes a day. The average age at which participants started smoking daily was 17.91 years (±4.16). In this sample population, 49.1 per cent reported that they had made at least one attempt to quit smoking in the past 5 years.
Self-reports
In this sample population, 41.8 per cent of our participants stated that their self-reported smoking behaviour would be accurate against the readings of the CreSSmicro device. Of the remaining participants, only 12.7 per cent reported that they might have over-reported their self-reports, whereas 45.5 per cent reported that their self-reports may be under-reported in comparison to the measurements of the CreSSmicro device. On a 7-item Likert scale ranging from ‘not confident at all’ to ‘very confident’, participants’ self-report accuracy ratings had a mean of 5.15 (±1.32). Table 1 summarises the results of t-test comparisons between self-reports and the recordings of the CreSSmicro device.
Summary of self-report and CreSSmicro comparisons.
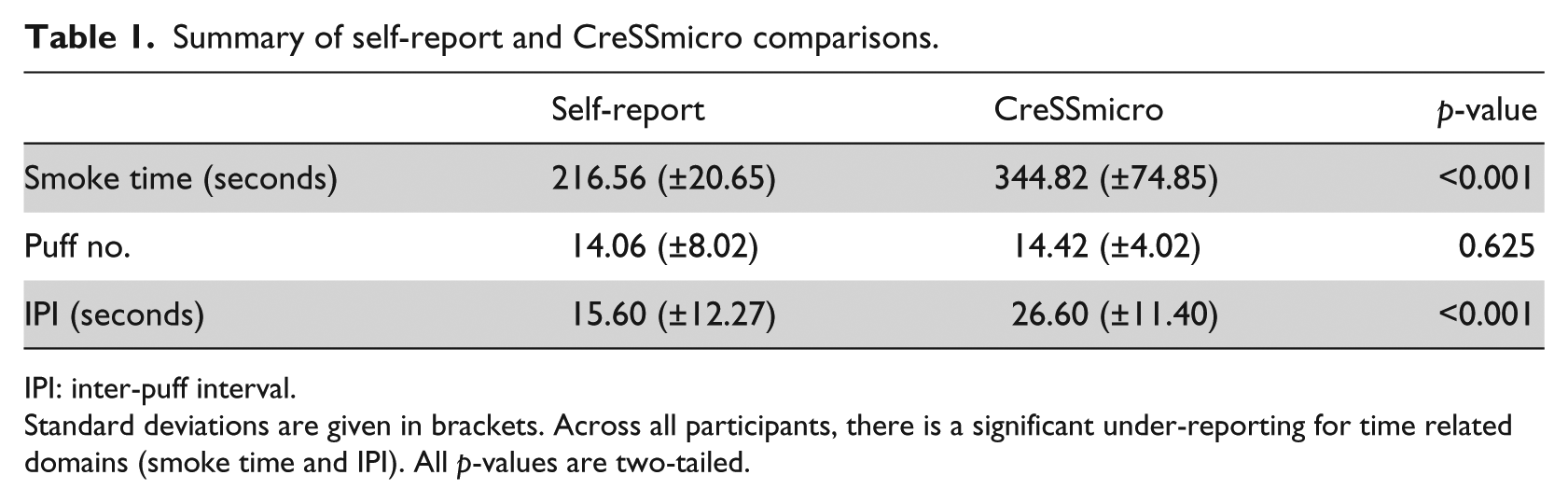
IPI: inter-puff interval.
Standard deviations are given in brackets. Across all participants, there is a significant under-reporting for time related domains (smoke time and IPI). All p-values are two-tailed.
Despite this initial confidence in the accuracy of self-reports, among smokers who said their self-reports would be accurate against the measurements of the CreSSmicro only around 4 per cent were accurate in their estimation, whereas more than 65 per cent had in fact under-reported their smoking parameters. In the subsample of smokers who said that they might have under-reported their smoking parameters, only 56 per cent estimated such bias accurately.
In order to test the prediction that the accuracy of self-reports would not improve by more frequent smoking, a correlation analysis was performed between self-report discrepancies and the measurements of the CreSSmicro device. In total, recordings from 1304 cigarettes were included in the analysis. In order to investigate the relationship between self-report distortions and health risk perception in an unbiased way, 8 participants were excluded from the sample population who gave accurate self-reports (i.e. no self-report discrepancy) to either one of three measures (smoke time, puff number and IPI). All of these 8 participants gave accurate puff number estimations. In this subsample, the mean number of daily cigarettes was 15 (± 5.6), susceptibility to acquiring airway diseases rating was 6.1 (± 0.6) and worry about consequences of cigarette smoking rating was 5.5 (± 0.8). As a result of excluding these participants, the sample population for further analysis contained 102 individuals for the second level.
The second level analysis showed that there is a positive relationship between total number of months of smoking and self-report differences for smoking time per cigarette (r = 0.282, p < 0.01, two-tailed), and the number of cigarettes smoked per day and self-report differences for IPI (r = 0.246, p < 0.05, two-tailed). The heavy (>15) and light smokers (<9; categorised on the basis of self-reports) did not differ significantly for perceived health risks and accuracy of self-reported smoking topography (all p > 0.125). When the categorisation was made on the basis of the number of cigarettes smoked during the 24 hours with the CreSSmicro, the heavy and light smokers remained comparable for all variables apart from perceived susceptibility to acquiring airway diseases, which was marginally elevated in the heavy smokers group (t = −1.802, df = 55, p = 0.08). Across 102 participants, there is a marginally significant (0.05 < p-value < 0.1) relationship between averaged perceived susceptibility to airway diseases and health concerns associated with smoking (assessed by two 7-item Likert scales each; p = 0.057, two-tailed).
Distortions in self-reports
One of the a priori predictions of this study (prediction 3 in the section ‘Introduction’) was that different combinations of self-report distortion profiles may interact with smoking-related health concerns. In order to test the a priori prediction, the sample is divided into four groups (i.e. 2 × 2 combinations of puff number and IPI discrepancies; for example, puff number over-reporting and IPI under-reporting; see Figure 1). A 2 × 4 GLM is fitted to the data (i.e. 2 averaged ratings of health concerns by four groups). The result indicated a significant health concern by group interaction (F(3, 98) = 3.056, p = 0.032), but no main effects of health concern or group.
As predicted, the puff number discrepancies correlated significantly with perceived susceptibility ratings (r = −0.237, p = 0.016) but only marginally with worries about smoking-related health risks (p = 0.08). In order to confirm the specificity of the influence of puff number distortions as the main indicator of primary exposure to smoke constituents, Groups 1 and 3 in Figure 1 (keeping the IPI distortion in the same direction in each group) were compared for perceived susceptibility to airway diseases. The analysis lends support to the finding that perceived susceptibility is significantly lower in the puff number under-reporting group (df = 85, t = −2.058, p < 0.05, two-tailed, see Figure 1). A post-hoc correlation analysis across all individuals who under-reported puff number (n = 67) suggested a negative correlation between the level of under-reporting and perceived susceptibility to acquiring airway diseases (r = −0.272, p = 0.026, two-tailed) such that individuals under-reporting puff numbers to a greater degree perceived lower susceptibility to acquiring airway diseases. This relationship is observed more strongly in those participants who also under-reported IPI (n = 57; r = −0.327, p = 0.013, two-tailed, see Figure 1). On the other hand, worry about health risks associated with smoking was marginally elevated in the puff under-reporting group (p = 0.09), providing additional support for the hypothesis that under-reporting primary exposure parameters may indeed be related to subconscious intentions to neutralise worry associated with long-term consequences of cigarette smoking.
Discussion
This article investigated the distortion of self-reports in smoking behaviour and tested the prediction that distortions in reported average puff number would be related to perceived susceptibility to acquire smoking-related airway diseases. The key findings are: (1) smokers do not have an accurate perception of descriptive aspects of their smoking behaviour, especially in time related domains such as giving an estimation of how long it takes to smoke a single cigarette and how much time elapses between each puff (i.e. IPI). The study finds (2) a significant relationship between under-reporting puff number and perceived susceptibility to acquiring airway diseases.
Self-reported distortions in time related domains may have neurobiological origins. In the literature, habit formation is associated with the loss of control of an internal clock (Cheng et al., 2007), and it has been suggested that interval timing sensitive to seconds-to-minutes range, mostly relies on inputs from serotonergic 5-hydroxytryptamine (5-HT)1A and 5-HT2A receptors (Asgari et al., 2006). Dopamine agonists such as nicotine can also cause horizontal left-ward shifts in time perception which correspond to clock-speeding (Buhusi, 2003; Buhusi and Meck, 2005). Considering that salivary cotinine, which is a biomarker of nicotine, has a half-life of approximately 20 hours and the fact that in the present protocol the participants were at least on 45 minute abstinence at the time of the interview when they estimated the descriptive aspects of their smoking behaviour, it is hard to make conclusive judgments about the neuropharmacological effects of nicotine on this process. Although there is some evidence that experimental manipulation of nicotine in healthy subjects and abstinence in smokers lead to disruptions in time interval estimation (Klein et al., 2003), this could only affect highly addicted individuals within the 45-minute abstinence interval in the present protocol.
If performing habitual behaviour more frequently led to higher awareness of the tactile aspects of the habit, one would assume that the individuals who smoke more frequently and for a longer time would be more accurate in their self-reports (an expected negative relationship). On the contrary, the present results showed that participants who smoke more frequently and for a longer duration give less accurate self-reports in time related domains of smoking behaviour such as total smoke time and IPI (i.e. a positive relationship). This finding conforms to the processes in the formation of habits, such that habitual behaviour becomes bodily unconscious through frequent repetition (Peretti-Watel et al., 2007). Although, the present findings seem to support the hypothesis on neuropharmacological effects of nicotine on time perception, it warrants further investigation as the present data did not show any significant differences between heavy and light smokers on measures related to time perception.
The other key finding is the relationship between puff number distortions and perceived susceptibility to acquiring airway diseases. Under-reporting in both illicit and illegal drug use may be a general trend (Mensch and Kandel, 1988), but in cessation interviews it is considered as a way of giving the socially desirable answer (Verplanken and Aarts, 1999). Recent evidence suggests that attitudes towards smoking are gradually changing whereby smoking becomes less socially desirable, and consequently the level of under-reporting of smoking prevalence is gradually increasing (Gallus et al., 2011). Such self-report distortions could lead to more serious health risks in special populations like pregnant women where under-reporting of smoking frequency is also observed (Bakker et al., 2011; Land et al., 2012). However, so far there is no directly comparable study which investigated puff number and IPI distortions, and their relationship with attitudes towards smoking associated health risks. In clinical health psychology, psychodynamic approach posits that such self-report distortions would be related to underlying health concerns, whereby these concerns are neutralised through cognitive distortion and repression (Mund and Mitte, 2012). The present data seem to support this point of view, such that reporting lower levels of direct exposure (i.e. puff number) influenced perceptions about susceptibility to acquiring airway diseases. Consequently, the group under-reporting puff numbers did not report elevated worry about health risks associated with smoking, but on the contrary the worry ratings were lower. A small subsample of daily smokers, however, made an accurate estimation for the frequency of direct exposure per cigarette (n = 8). These individuals reported higher worry and susceptibility to acquiring airway diseases. However, it is not possible to formulate a causal relationship between self-report distortions and attitudes towards health risks in the present experimental procedure. Considering the paucity of evidence in the literature, this issue warrants further experimental research.
Self-report distortions may have negative long-term consequences whereby health risks associated with smoking may be underestimated (Peixoto et al., 2005) and smoking may be perceived as a relatively ‘harmless’ daily activity, reducing motivation for quitting as previously documented (Tarr, 2008). Therefore, assessing differences between actual and perceived smoking/exposure is important to promote awareness about how self-report distortions may be related to underlying worry about facing negative consequences of smoking on one’s health. Consequently, this may lead to forming a distorted health risk perception. Using portable topography devices as a part of smoke cessation interventions would enhance awareness about the tactile aspects of smoking behaviour (as commonly reported by participants in this cohort; see below) which would otherwise remain to be unconscious and habitual. This approach would also give clinicians objective data from their patients to address underlying negative cognitive associations which may otherwise remain undetected due to factors such as social desirability.
The main limitation of our study is the use of an artificial topography device to measure smoking behaviour. CreSSmicro is a portable smoking topography measuring device which is half the size of a cigarette box. In our population, 21.1 per cent of participants said that the device did not change their smoking behaviour at all, whereas 63.3 per cent said that it changed a little bit and the remaining 15.6 per cent said it changed their smoking behaviour a lot. At this extreme, 11 smokers reported taking more and 6 smokers reported taking less number of puffs than they would had they not been using the topography device. This would suggest that using the topography device did not change participants’ behaviour systematically in a single direction. We did not fully investigate how these changes occurred quantitatively, but we asked our participants to give us a qualitative account of their experiences with using the device. The qualitative reports converged on themes such as difficulty in using the device in public places due to increased attention from others, difficulty in using while driving, making cigarettes taste more bitter than usual and making the smoking experience more conscious than it usually is. Although I do not know the true impact of the device on the variables that were assessed here, it may have caused longer IPIs particularly if the participants wanted to observe the device to understand how it works. Another limitation of this study may be related to recruitment of participants; they were recruited by a purposive sampling approach without aiming to reflect the nationwide prevalence and demographical features of the smoking population.
In conclusion, this study investigated habitual aspect of smoking behaviour and self-report distortions. Here, self-report distortions of smoking behaviours were objectively validated with the use of a handheld topography recording device over 24 hours. Using a handheld topography device for 24 hours may indirectly increase awareness about the tactile aspects of smoking behaviour. When self-reports are compared with such objective measures of smoking topography, it would be possible to address the role of cognitive distortion mechanisms which may relate to underlying attitudes about associated health risks. Integrating this approach to clinical/health psychological interventions may allow giving a higher level of individually tailored feedback to those smokers who are trying to quit. Combined with feedback on exposure levels, such as expired air carbon monoxide measures (Shahab et al., 2011), such multi-dimensional approaches may increase the efficacy of stop smoking interventions. Replicating these findings in a representative sample in different contexts should be considered for future research.
Footnotes
Acknowledgements
The author designed the study, recruited participants, collected and analysed the data, and wrote the article. The author would like to thank to Professors Ann McNeill and Rebecca Elliott; and Drs Anna Murphy and Martyn McFarquhar for their helpful comments on an earlier version of this manuscript, and Mrs Berna Kalkan for providing help with recruitment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Cancer Research UK, grant number C25586/A8324.