
Abstract
This study examined weight status and dietary restraint among same-sex couples using Actor–Partner Interdependence Models. Body mass indices and restrained eating behaviors (i.e., cognitive dietary restraint, uncontrolled eating, and emotional eating) were assessed for members of 144 same-sex couples (72 lesbian and 72 gay couples; mean age = 33.74 years, standard deviation = 11.27 years). Results indicated that both men and women who were relatively heavy and who had relatively thin partners were at particular risk of engaging in restrained eating. These findings extend our understanding of partner comparison processes within the context of same-sex relationships in determining men and women’s eating behaviors.
Keywords
Current sociocultural ideals emphasize the integral role of thinness and fitness in contributing to attractiveness. These ideals are all but completely unobtainable by both men and women and are a documented source of not only distress, but unhealthy eating and dieting practices, which may lead to restrained eating (Harrison, 2000; Kaminski et al., 2005; Stice et al., 1994). These eating behaviors do not occur in isolation, but in a social context, in which network members—particularly romantic partners—often have a substantial direct and indirect influence on each others’ eating behaviors and body size (Baltrus et al., 2005; Umberson et al., 2009). Thus, the focus of this study is to examine links among individuals’ body size, romantic partners’ body size, and restrained eating.
Restrained eating
Restrained eating is similar to, yet distinct from, dieting, in the sense that it reflects a pattern of “frequent dieting and overeating in the past rather than from a current state of dietary or cognitive restraint” (Lowe, 1993: 100). In other words, restrained eaters participate in the long-term deliberate restriction of food intake for the purpose of losing, maintaining, or avoiding the gain of weight, typically characterized by alternating episodes of restraint and binging. Furthermore, Herman and Polivy (1980) have noted that restrained eating “is defined more in terms of effort expended toward weight suppression than in terms of achieved success” (p. 223). Thus, the general construct of restrained eating is typically conceptualized to include three related practices: cognitive dietary restraint, uncontrolled eating, and emotional eating (Karlsson et al., 2000).
Although these three practices are related, they are distinct from each other, with cognitive dietary restraint being characterized by a conscious restriction of food intake and sometimes inhibiting intake completely and/or restricting intake to foods with relatively low caloric value (De Lauzon et al., 2004; Lowe, 1993). Uncontrolled eating describes a tendency to increase food consumption resulting from a combination of hunger and an inability to regulate intake (De Lauzon et al., 2004). Emotional eating indicates increased food consumption as a result of emotional cues such as emotional distress (De Lauzon et al., 2004). Each of these practices is often episodic in nature, and they collectively form a pattern of restrained eating over time (Lowe, 1993).
Extended periods of restrained eating may facilitate unhealthy weight fluctuations and cause detrimental physiological changes. Long-term patterns of alternating cognitive restraint, emotional eating, and uncontrolled eating cause individuals to become habituated to sensations of both hunger and satiation (Herman and Polivy, 1984). Restrained eaters even tend to salivate more than unrestrained eaters in response to the sight and smell of palatable food (Klajner et al., 1981) and eat significantly more after exposure to cognitive or olfactory food cues (Fedoroff et al., 1997), which indicates that the salivary responses of these individuals also becomes habituated to food cues as a result of their eating practices. In other words, restrained eaters’ efforts to consciously ignore their physiological hunger cues become less conscious over time, as their bodies adjust to their new eating patterns. This may cause them to reduce or lose their physiological ability to assess their own hunger and become less able to cognitively monitor their food intake through social or environmental cues (Herman et al., 1983).
Physiological changes result from restrained eating, but social interactions often predicate its practice. However, the majority of the literature regarding the influence of social relationships on eating behavior discusses these issues among adolescents within the context of their relationships with parents and peers. There has been relatively little consideration of the correlates of social relationships on the eating behaviors of adults. In the studies that have examined these issues, researchers (e.g. Drigotas et al., 1999; Markey and Markey, 2006; Markey et al., 2001; Sanchez and Kwang, 2007; Yancey et al., 2003) have found that influences from current romantic partners, such as a partner’s body size (i.e. body mass index (BMI)), significantly affect weight concerns and eating behaviors among men and women. For example, Markey and Markey (2010) found that heterosexual men and women in relationships with partners who had lower BMIs expressed more weight concerns, and that such concerns were most likely to be present among relatively heavy individuals who had partners with relatively low BMIs.
Markey and Markey (2012) replicated these findings among women in lesbian romantic relationships and proposed a “partner comparison model,” based on social comparison theory, to account for their results. Social comparison theory (Festinger, 1954) suggests that individuals tend to evaluate their own opinions, attitudes, and abilities in relation to those of others. Furthermore, this theory indicates that as the importance of a person’s chosen reference group grows, pressure to conform to that group grows as well. Markey and Markey (2012) extended this theory to the context of romantic relationships, asserting that individuals’ self-perceptions are influenced when they compare themselves to their partners. Therefore, if individuals view their significant others as exemplifying a more desirable trait such as lower weight status, they are more likely to express concern regarding their own weight status and a greater desire to conform to their partners’ weight status.
Given that the health implications of social relationships are less clear among gay and lesbian versus heterosexual individuals, these influences merit particular consideration when studying the many factors that contribute to their potentially maladaptive eating behaviors and attitudes. Although such research examining heterosexual couples is important, no research has yet examined restrained eating within the context of same-sex romantic relationships. This oversight is unfortunate as some studies suggest that body ideals and preferences among gay and lesbian individuals may differ from those of heterosexual people (e.g. Brand et al., 1991; Kelly, 2007; Martins et al., 2007; Wagenblach, 2004), thus indicating different attitudes toward eating habits and weight. For example, among lesbian couples, BMI has been found to predict preferences of physical attractiveness differently than preferences for heterosexual women, with lesbians preferring partners with higher BMIs and heterosexual women preferring partners with lower BMIs (Swami and Tovee, 2006). These findings indicate that identification with lesbian subculture may counteract otherwise-detrimental effects of mainstream Western cultural ideals for many women, thus protecting and encouraging more positive body ideals.
Conversely, gay men have been found to experience disturbances in body image and eating practices more often than their heterosexual peers (Martins et al., 2007). A study by Swami and Tovee (2008) asked gay and heterosexual men to rate photos of males based on physical attractiveness. They found that gay men tended to favor males with lower waist-to-chest ratios, indicating preference for a more exaggerated Y-shaped body type, which suggests a desire for a muscular partner with a relatively lower BMI. Additionally, Yelland and Tiggemann (2003) found that gay men exhibited a significantly higher drive for muscularity than heterosexual men and women, and that their drive for thinness was significantly higher than that of heterosexual men (but not heterosexual women). Furthermore, Levesque and Vichesky (2006) found that gay men who engaged in greater social comparison and had higher BMIs were more likely to experience body dissatisfaction than those who had lower BMIs. These findings collectively indicate that gay men not only prefer leaner body types, but they also tend to idealize muscularity more than heterosexual men, which may result in greater body dissatisfaction, specifically because achieving more muscularity is likely to come at the cost of maintaining a low BMI.
Although extensive research is available concerning body image and restrained eating among adolescent and adult females, the amount of empirical knowledge becomes increasingly sparse when approaching the present topic of interest. There are abundant sources of information on restrained eating among women, fewer regarding eating practices among lesbian women and gay men, fewer still regarding restrained eating within the context of romantic relationships, and no studies to our knowledge regarding restrained eating practices among women and men in same-sex romantic relationships. There is a need to identify whether or not the effects that have been found for men and women in heterosexual relationships may generalize to men and women in same-sex relationships. Such an examination would be extremely beneficial, not only to further an understanding of same-sex relationships and subculture, but to gain a more complete understanding of all kinds of romantic relationships and how their dynamics contribute to health. Identification of correlates that may be specific to sexual orientation or romantic involvement would also provide researchers with a better understanding of the concept of restrained eating and the social and sexual dynamics that may promote or inhibit its practice.
Actor–partner interdependence models
Because this study utilizes data from both partners of a romantic dyad who are indistinguishable from each other in terms of gender (i.e. both partners are either men or women), traditional statistical techniques are not appropriate. Therefore, Actor–Partner Interdependence Models (APIMs; Kenny et al., 2008) will be employed in order to account for the dependency in these data. APIMs are statistical methods that make it possible to examine how Person A’s criterion variable simultaneously and independently relates to his or her own predictor variable as well as to his or her partner’s (Person B’s) predictor variable.
In the current context, an APIM can be used to examine how different facets of restrained eating (cognitive dietary restraint, uncontrolled eating, and emotional eating) are uniquely related to interpersonal variables that exist among romantic partners. First, the associations between Person A’s weight status and Person A’s restrained eating (using the three subscales separately) can be estimated. The APIM denotes this as an “actor effect” (see Figure 1). Second, the association between Person B’s weight status and Person A’s restrained eating (using the three subscales separately) can be estimated. The APIM denotes this as a “partner effect” (see Figure 1).
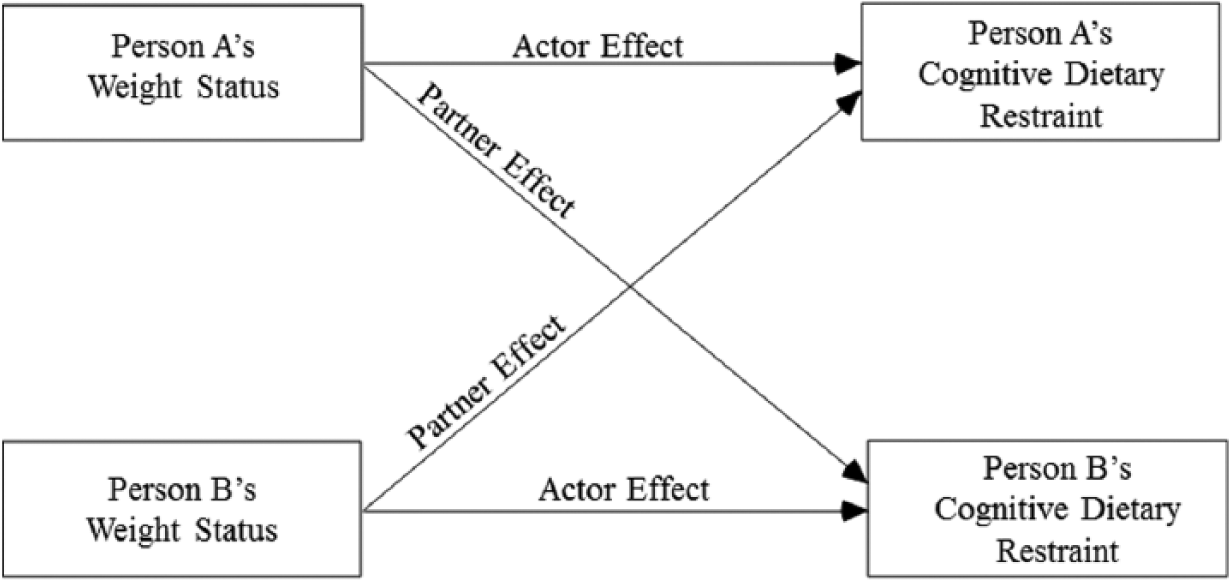
Actor–Partner Interdependence Model (APIM) for weight status predicting cognitive dietary restraint.
In addition to examining actor and partner effects, APIMs also make it possible to examine the extent to which dissimilarity among Person A and Person B’s BMI predicts restrained eating. This “dissimilarity effect” can be investigated by examining the simple interaction between Person A’s BMI and Person B’s BMI. Finally, participants’ gender can be used to both predict restrained eating and to examine whether it moderates actor, partner, or dissimilarity effects of BMI. For example, the interaction between gender and BMI in assessing an actor effect would determine whether or not the BMIs of gay men have a different association with their restrained eating than does the weight status of lesbian women. The same analyses will be conducted to examine all three components of restrained eating: cognitive dietary restraint, uncontrolled eating, and emotional eating.
Hypotheses
Although not considered a clinical eating disorder, restrained eating is often a precursor to disordered eating, which can lead to negative physical and psychological consequences (Lowe, 1993). Therefore, the ability to isolate the factors that contribute to or prevent these practices has critical implications for interventions, future research, and general public health. Prior studies have firmly established the connection between BMI and restrained eating (e.g. De Lauzon-Guillain et al., 2006; Heaven et al., 2001; Herman and Polivy, 1984), but this has rarely been investigated within the context of romantic relationships, which are an important and pervasive component of most adults’ eating environments. Furthermore, the issues addressed in this study have not yet been explored within the context of same-sex romantic relationships. Thus, this study aims to extend previous research on BMI and restrained eating by examining these behaviors among men and women in same-sex relationships using APIMs.
Specifically, we propose the following hypotheses:
Actor effect. An individual’s BMI will be positively related to his or her cognitive dietary restraint, uncontrolled eating, and emotional eating (actor effect). Therefore, a person with a higher BMI will be more likely to practice cognitive dietary restraint, uncontrolled eating, and emotional eating.
Partner effect. An individual’s partner’s BMI will be negatively related to his or her cognitive dietary restraint, uncontrolled eating, and emotional eating (partner effect). Therefore, a person whose partner has a low BMI will be more likely to practice cognitive dietary restraint, uncontrolled eating, and emotional eating.
Dissimilarity effect. Each participant’s BMI will interact with that of his or her partner when predicting restrained, uncontrolled, and emotional eating (interaction effect). Specifically, individuals with higher BMIs who have partners with relatively low BMIs will be most vulnerable with regard to cognitive dietary restraint, uncontrolled eating, and emotional eating.
Gender. Analyses concerning the main effect of gender and its possible moderating effects on actor BMI, partner BMI, and the dissimilarity effect are exploratory, and thus no specific predictions were made. These analyses make it possible to determine whether these main effects differ for male and female same-sex couples.
Method
Participants and procedures
A total of 288 participants (72 gay couples and 72 lesbian couples; mean age = 33.74 years, standard deviation (SD) = 11.27 years) with varying socio-economic and ethnic backgrounds were recruited for this study. A total of 70 percent of the sample was European-American, 14 percent was African American, 10 percent was Hispanic, 3 percent was Asian, and 3 percent was of an “other” ethnic background. All couples were required to have maintained an exclusive, monogamous relationship for at least 6 months. The majority of the couples in our sample were cohabitating (76%), and couples had been romantically involved for 5.55 years, on average.
Participants were recruited from a northeastern university campus and the surrounding area by advertising in diverse periodicals and through local health and advocacy groups located in nearby urban areas. These couples were participants in a larger study examining predictors of relationship quality and health (cf. Markey and Markey, 2013) among gay and lesbian couples. Participants were placed in separate rooms in the researchers’ laboratory while they completed the measures used in this study. All procedures were approved by the Institutional Review Board at the host university, participants provided voluntary consent, and each couple was compensated with US$100 (US$50 per participant).
Measures
Weight status
In this study, weight status was operationalized using BMI scores (weight (kg)/height2 (m2)). Based on the recommendations of Lohman et al. (1988), three height and weight measurements were collected from each participant by a trained research assistant. Participants’ average weight and height (across the three measurements) were used to calculate their BMIs. In this study, women’s average BMI was 29.38 (SD = 8.23) and men’s average BMI was 26.28 (SD = 5.58). These mean BMIs are considered overweight but are similar to the national average for men and women 20 years and older (which is 27.8 and 28.1, respectively; Center for Disease Control and Prevention (CDC), 2004). Furthermore, romantic partners tended to have fairly similar BMIs; pairwise intraclass r (142) = .38, p < .01.
Restrained eating
The revised version of Stunkard and Messick’s (1985) Three-Factor Eating Questionnaire (TFEQ) was used to measure cognitive dietary restraint, emotional eating, and uncontrolled eating. The TFEQ-18 was developed by Karlsson et al. (2000) and has successfully been used with general populations of teenagers, young adults, and middle-aged adults by De Lauzon et al. (2004). The measure consists of 18 items designed to assess cognitive dietary restraint (restraint of food intake; “I deliberately take small helpings as a means of controlling my weight”; Cronbach’s alpha = .77), uncontrolled eating (addressing episodes of binge eating; “when I smell delicious food, I find it very difficult to keep from eating even if I have just finished a meal”; Cronbach’s alpha = .81), and emotional eating (addressing feelings toward food and hunger; “I get so hungry that my stomach often seems like a bottomless pit”; Cronbach’s alpha = .76). Total scores for each subscale were standardized on a 0 to 100 scale with high scores indicating that a participant reported high levels of cognitive dietary restraint (M = 42.29, SD = 21.03), emotional eating (M = 39.85, SD = 29.20), or uncontrolled eating (M = 37.55, SD = 21.30).
Results
Cognitive dietary restraint
Multilevel modeling was first used to test an APIM predicting cognitive dietary restraint from the level-2 variable gender (coded 0 = female dyad; 1 = male dyad) and the level-1 variables: actor effect for weight status and partner effect for weight status. This model simultaneously tests the unique contributions of gender, actor BMI, and partner BMI in predicting cognitive dietary restraint. In other words, this model tests for each effect (actor or partner BMI) while controlling for the other effect (actor or partner BMI). Table 1 displays the resulting APIM effects when predicting cognitive dietary restraint. As seen in the table, the partner effect of BMI was negatively related to cognitive dietary restraint. In other words, individuals in romantic relationships with a thin partner were likely to report cognitive restriction of their food intake. To determine whether or not the interaction between individuals’ and partners’ BMIs predicted cognitive dietary restraint, a new variable was created, which was the product of the actor’s BMI and their partner’s BMI. As suggested by Aiken and West (1991) and Kenny et al. (2008), BMI was centered when computing the interaction term. This interaction term was then included as an independent variable, along with the actor and partner main effects from the previous analysis in a second APIM. As seen in Table 1, the resulting interaction term between actor BMI and partner BMI was significant in predicting cognitive dietary restraint.
Summary of Actor–Partner Interdependence Models predicting cognitive dietary restraint, uncontrolled eating, and emotional eating.
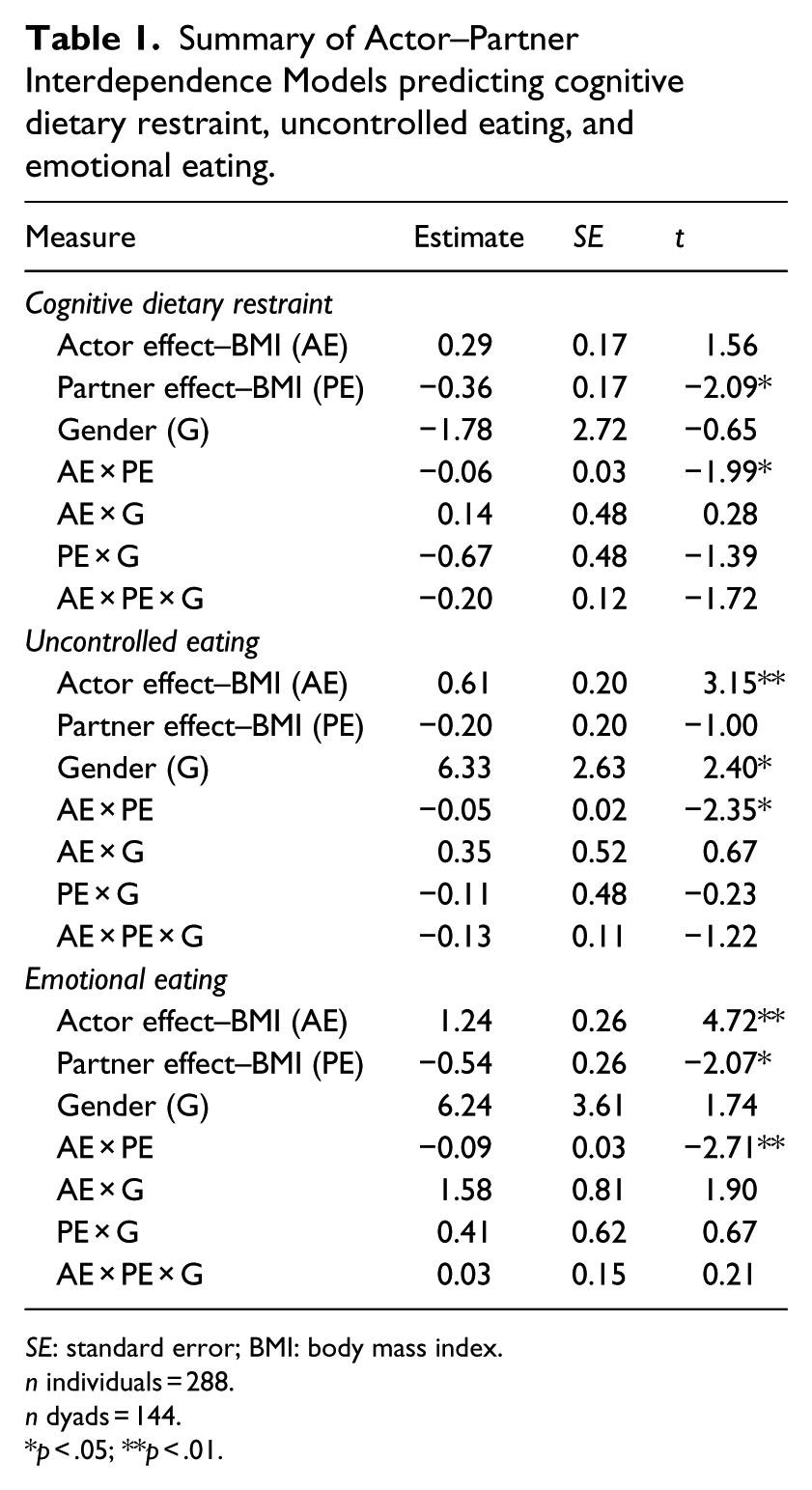
SE: standard error; BMI: body mass index.
n individuals = 288.
n dyads = 144.
p < .05; **p < .01.
In order to illustrate this interaction, Figure 2 presents a graphical representation derived by calculating simple regression equations corresponding to individuals scoring at the mean, 1 SD above the mean, and 1 SD below the mean for each predictor variable (Aiken and West, 1991). Consistent with the hypothesis, individuals who were relatively heavy and who had partners who were relatively thin were at particular risk of engaging in cognitive dietary restraint.
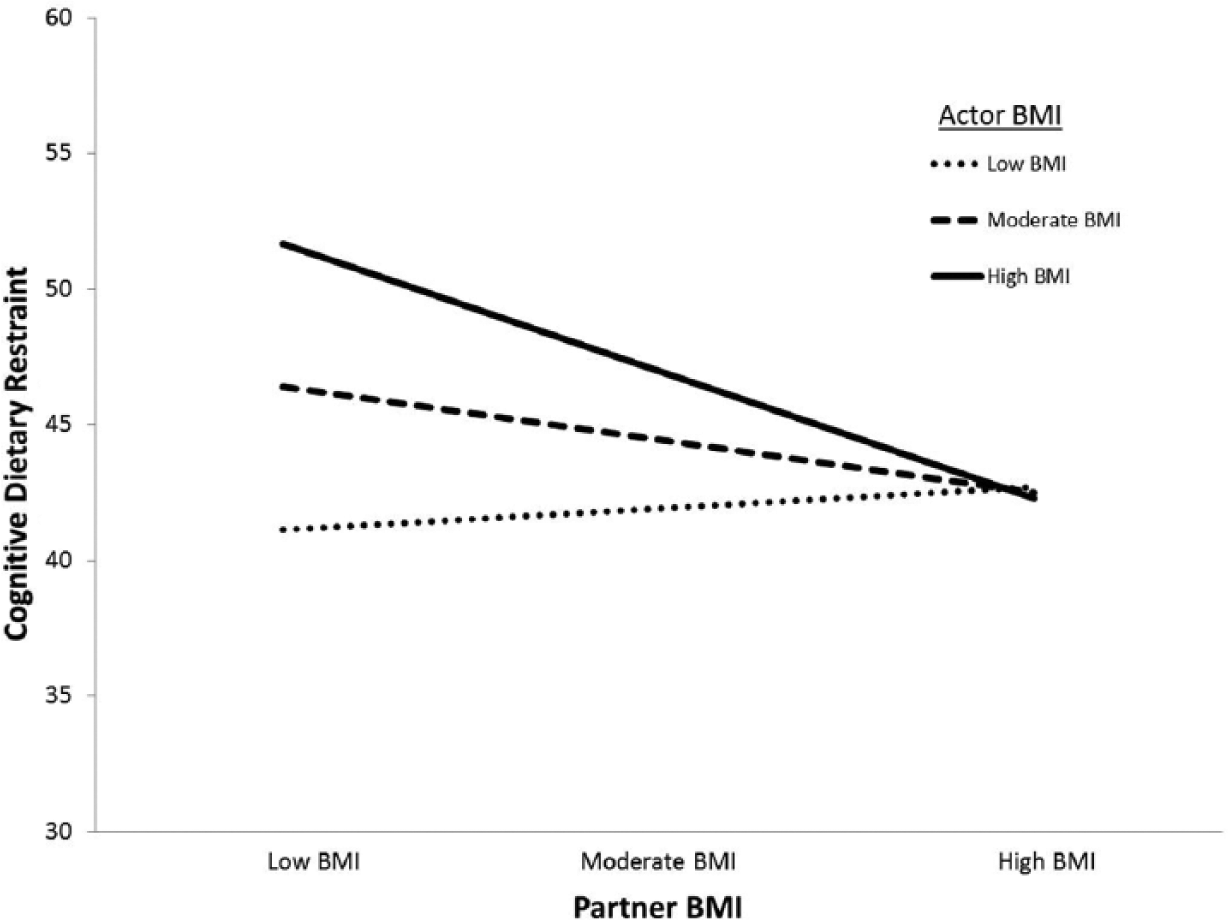
Graphical representation of the dissimilarity effect showing the interaction between actors’ body mass index (BMI) and their romantic partners’ BMI when predicting cognitive dietary restraint.
A final APIM examined whether or not any of the effects examined (actor, partner, actor × partner) were moderated by gender. As before, these interaction effects were tested hierarchically; none were significant (see Table 1). This result suggests that the effects reported earlier are not different for women versus men in same-sex relationships.
Uncontrolled eating
A new set of hierarchical APIMs was then used to examine the actor and partner effects of BMI when predicting uncontrolled eating. As seen in Table 1, there was a significant actor effect and gender effect when predicting uncontrolled eating. In other words, both men and individuals who were heavy were at particular risk of engaging in uncontrolled eating. More central to the main focus of this article, a significant actor × partner interaction was also found. In order to illustrate this interaction, Figure 3 presents a graphical representation derived by calculating simple regression equations corresponding to individuals scoring at the mean, 1 SD above the mean, and 1 SD below the mean for each predictor variable (Aiken and West, 1991). Consistent with the hypothesis, individuals who were relatively heavy and who had partners who were relatively thin were at particular risk of engaging in uncontrolled eating.
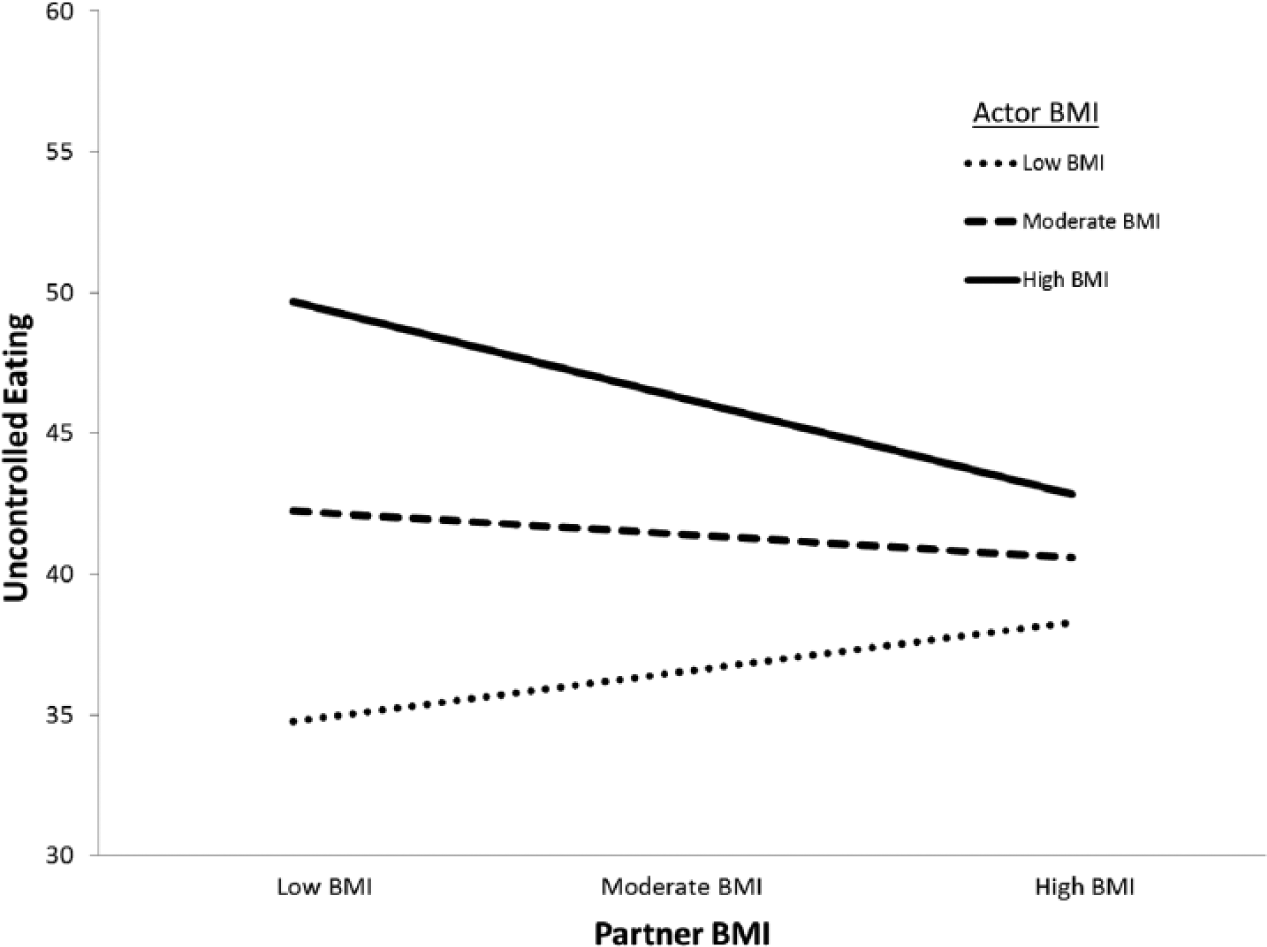
Graphical representation of the dissimilarity effect showing the interaction between actors’ body mass index (BMI) and their romantic partners’ BMI when predicting uncontrolled eating.
Emotional eating
A final set of hierarchical APIMs was used to examine the actor and partner effects of BMI when predicting emotional eating. As seen in Table 1, there were significant actor and partner effects when predicting emotional eating. It appears that individuals who were relatively heavy tended to engage in emotional eating, and individuals who had relatively thin romantic partners also engaged in this activity. As before, and consistent with the hypothesis, a significant actor × partner interaction was also found. As seen in Figure 4, and consistent with the other restrained eating scales, individuals who were relatively heavy and who had partners who were relatively thin were at particular risk of engaging in emotional eating.
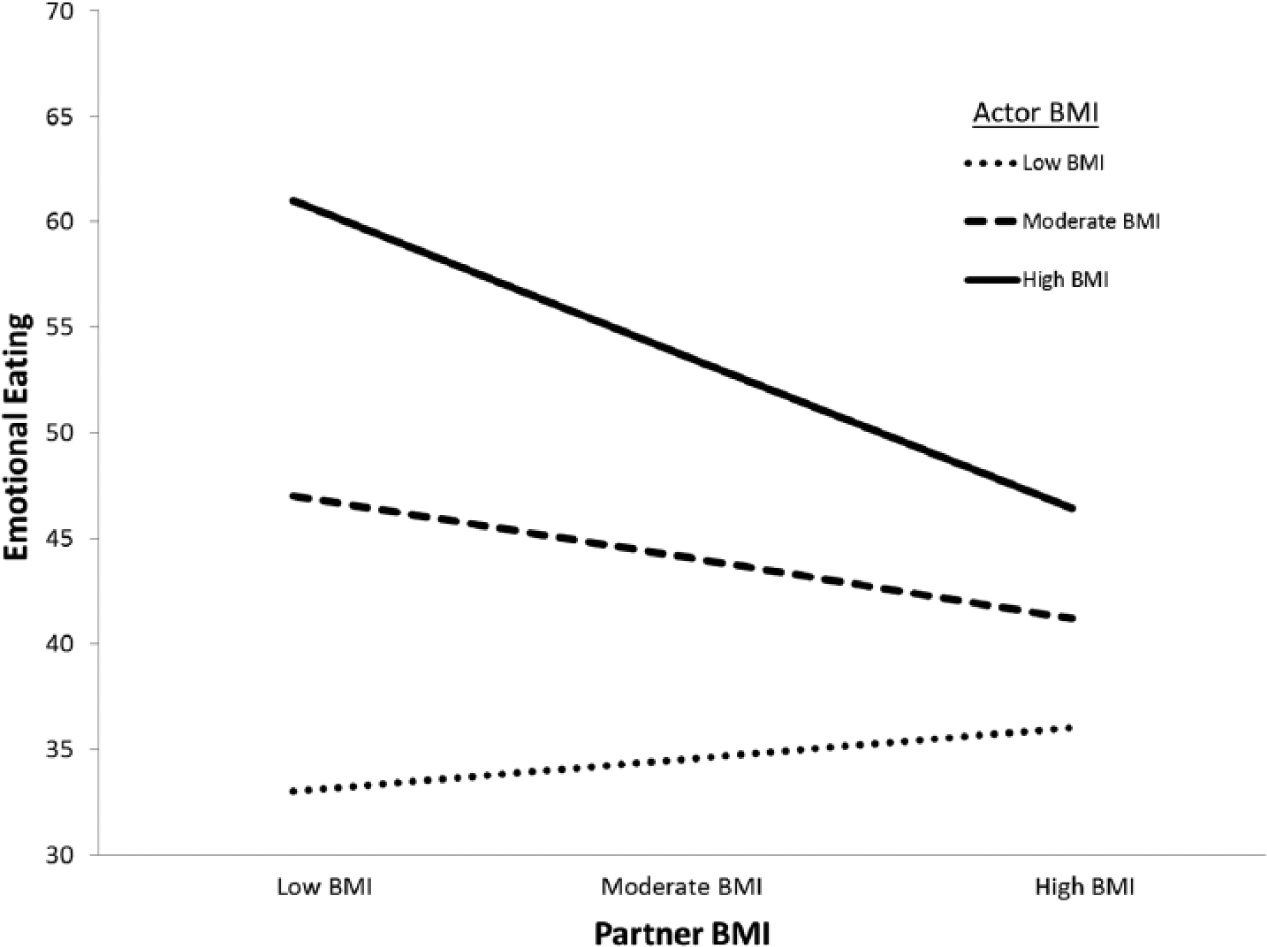
Graphical representation of the dissimilarity effect showing the interaction between actors’ body mass index (BMI) and their romantic partners’ BMI when predicting emotional eating.
Discussion
The pressure that men and women in Western society face, which encourages them to pursue exceedingly unrealistic body ideals, is an unfortunate reality. Side effects of these pursuits are myriad and include negative self-perceptions, dieting, and even disordered eating behaviors (Martins et al., 2007). The goal of this study was to contribute to an understanding of restrained eating among an understudied population: same-sex romantic couples. To do so, we examined potential links among individuals’ BMIs, their romantic partners’ BMIs, and restrained eating. Understanding a potentially important context of restrained eating—same-sex romantic relationships—is an unexplored area of research; however, a clear understanding of associations among these variables has the potential to provide information that may prove invaluable for effectively treating potentially deleterious eating behaviors.
The majority of the hypotheses were supported by the data. As predicted (Hypothesis 1), an individual’s BMI was positively related to his or her tendency toward emotional and uncontrolled eating. Consistent with Hypothesis 2, partners’ BMIs exhibited a significant negative relationship with emotional and cognitive dietary restraint. Finally, as expected (Hypothesis 3), significant actor × partner BMI interactions were found to predict all three restrained eating subscales: cognitive dietary restraint, emotional eating, and uncontrolled eating. Taken together, these results extend past work on heterosexual relationships and are consistent with the partner comparison effect found in past research (e.g. Markey and Markey, 2012).
One possible explanation for these results is that in same-sex relationships, individuals feel pressure to conform to the body ideals of close reference groups (romantic partners). This tendency may be exacerbated when one’s partner is of the same gender and body comparisons are more meaningful (i.e. a woman in a relationship with a man is unlikely to compare her body to her partner’s body and aspire to achieve the same body size). In this study, “partner comparisons” appear relevant to all aspects of restrained eating (i.e. cognitive restraint, emotional, and uncontrolled eating), but these comparisons seem to be most potentially problematic for partners with relatively high BMIs (see Figures 2 to 4). Such findings are intuitive in that individuals who are not maintaining socially desirable weight statuses may be more affected by comparisons to a relatively thin partner who is maintaining a socially desirable weight status (Markey and Markey, 2012).
Expanding upon previous studies examining weight concerns among heterosexual couples (Markey and Markey, 2010; Markey et al. 2001), our results suggest that one’s own BMI and the BMI of one’s partner may predict restrained eating practices among same-sex couples as well as opposite-sex couples. Specifically, cognitive restraint, emotional eating, and uncontrolled eating were most prevalent among heavy individuals who were in romantic relationships with relatively thin same-sex partners. Such a finding indicates the possible need for developing couples-based intervention methods targeting healthier eating practices and more positive esteem building for relatively heavy individuals in romantic relationships with relatively thin partners who struggle with their eating behaviors. Partners’ eating behaviors are likely to affect each other as they spend time planning, preparing, and sharing meals (especially if they cohabitate). This effect may be positive or negative as social comparison processes may be relevant to not only partners’ body sizes but also to what food partners consume.
Limitations and conclusions
Although this study provided novel and useful information about the restrained eating behaviors of gay men and lesbian women in the context of their romantic relationships, further investigation into the similarities and differences between same-sex and heterosexual couples is warranted. The present sample was cross-sectional in nature, which limits the utility of these findings. Cross-sectional data can provide a snapshot of these practices among multiple participants at different life stages, but a longitudinal study would more accurately portray the ways in which individuals’ eating behaviors and social influences evolve throughout their lives. Because we cannot conclusively determine the direction of effects, we are unable to say with certainty whether BMI actually causes restrained eating; there is likely a reciprocal relationship between these two variables. Furthermore, the existence of a selection effect among this sample should be considered. It is possible that restrained eaters may harbor certain body image ideals that encourage them to choose a partner whose physical appearance or behavior corroborates with these ideals. It is hoped that future researchers extend this research in order to better understand the causal directions of these effects and issues related to body image, body ideals, and perhaps even perceived attractiveness among individuals in same-sex relationships.
Men and women often equate thinner body types with increased health and sexual attractiveness, which may be erroneous, and cause misconceptions about how to obtain a healthy body type (Stevenson et al., 2007). These conceptions may, in turn, promote unhealthy dieting and restrained eating practices. The importance of delineating exactly which factors may affect such eating practices cannot be overstated. Romantic partners play an important role in the majority of adults’ health (Waite, 1995); therefore, the ways in which they contribute to health behaviors such as eating behaviors may provide useful insight into ways to promote more healthful habits among partners. Those who identify as gay or lesbian may be affected differently by societal standards for body ideals than heterosexual individuals, but our findings show that they experience social comparison in romantic relationships similarly. We have identified that a connection between BMI and restrained eating exists among same-sex couples in the context of their romantic relationships. However, a greater understanding of these interactions will help researchers and practitioners devise more effective prevention and treatment methods, such as couples-based interventions and education programs, in addition to generally promoting more healthy eating behaviors among women and men alike, regardless of their sexual orientation.
Footnotes
Funding
This research was supported by a grant from the Lesbian Health Fund of the Gay and Lesbian Medical Association awarded to the 2nd author. Further, a Faculty Research Grant from Rutgers University awarded to the 2nd, 4th, and 5th authors helped to support this research.