
Abstract
Most health decision-making models posit that deciding to engage in a health behavior involves forming a behavioral intention which then leads to actual behavior. However, behavioral intentions and actual behavior may not be functionally equivalent. Two studies examined whether decision-making factors predicting dietary behaviors were the same as or distinct from those predicting intentions. Actual dietary behavior was proximally predicted by affective associations with the behavior. By contrast, behavioral intentions were predicted by cognitive beliefs about behaviors, with no contribution of affective associations. This dissociation has implications for understanding individual regulation of health behaviors and for behavior change interventions.
Weight control and energy balance are central to many pressing public health concerns. At present, over 60 percent of American adults meet clinical criteria for overweight or obesity (Ogden et al., 2014), and 16.6 percent of deaths in the United States are related to diet and physical activity (Mokdad et al., 2004).
Given the prevalence of obesity-related issues, it is not surprising that weight control is a concern for many individuals. Well over half of US adults (and an even higher percentage of women) have at some point in their lives formed a conscious intention to diet in order to lose weight (Jeffery et al., 1991, 2000). At any given point in time, about one-third of adults report a current intention to diet for weight loss (e.g. Paeratakul et al., 2002; Serdula et al., 1999).
Collectively, the prevalence of obesity and dieting intentions illustrates a paradox. A majority of Americans have at some time had an intention to change their eating behavior that was conscious enough and salient enough to be reported in a survey response. Given the prevalence of obesity, however, one is forced to conclude that most of those efforts do not translate into effective weight-loss behaviors.
This article focuses on the role that individual decision-making processes might play as predictors of dieting intentions and actual eating behavior. More specifically, our questions are as follows: Are the features of decision making that lead one to form an intention (such as deciding to make changes to one’s dietary behaviors) the same as those that guide one’s behavioral choices (such as actual food consumption)? Are health-related intentions and actions influenced by the same decision-making inputs or by separate and dissociable factors?
These questions are important for both basic and applied reasons. Most health decision-making models include an intentions component as a centerpiece to understanding behavior. Understanding the processes involved in intentions and when intentions do and do not predict behaviors is important. Most intervention approaches involve leading people to form an intention and/or to act on that intention to change behavior. Therefore, understanding these factors is also important for developing interventions to effectively encourage changes in health behaviors.
In this article, we report two studies examining this question. The conceptual framework guiding the research is the behavioral affective associations model (Kiviniemi and Duangdao, 2009; Kiviniemi et al., 2007).
We first briefly review evidence that intentions and behaviors might be predicted by different factors. We then review the behavioral affective associations model and evidence for its predictive utility in the context of actual engagement in health behaviors. We then present two studies addressing the question of the overlap between predictors of behavioral intentions and actual behavioral practices.
Planning and action in current health decision-making models
Many models of health decision making assume that individuals use cognitively based informational inputs (e.g. beliefs about costs and benefits of the behavior, perceptions of one’s own ability to carry out the behavior) to make a conscious decision to engage (or not to engage) in a particular behavioral pattern (Webb and Sheeran, 2006; Weinstein, 1993). It is then assumed that this intention is the proximal predictor of one’s actual behavior. This argument is most directly made in the theories of reasoned action/planned behavior (Ajzen, 1991; Ajzen and Fishbein, 1980), where intentions are a formally defined part of the model, but it is also implied in other models (for a further discussion, see Webb and Sheeran, 2006).
However, a variety of evidence suggests that intentions and behaviors are not necessarily functionally equivalent. Although intentions are associated with actual behavior, the strength of the relation is not nearly as high as one might expect. Meta-analytic examinations suggest that behavioral intentions account for only about 25 percent of the variance in behavioral practices (Godin and Kok, 1996).
Several independent lines of both empirical and theoretical works support the idea that intentions and actual behavior are not functionally equivalent and may have distinct antecedents. The prototype/willingness model (Gibbons and Gerrard, 1995) posits that planning may not always directly predict action. The model makes a distinction between behavioral intentions, conceptualized as a rational, planful guide to behavior, and behavioral willingness, the willingness to engage in the behavior under certain circumstances. Although the two share some common antecedents, they are distinct constructs, can independently influence behavioral choices, and may lead to different behavioral outcomes (Gibbons et al., 2003). Similarly, Gollwitzer (1999) distinguishes between intentions about a particular behavioral goal state and plans to implement and carry out those behaviors. There is evidence for the distinction for several health domains (Milne et al., 2000, 2002; Verplanken and Faes, 1999). In a related vein, Friese et al.’s (2011; see also Hofmann et al., 2008) work on impulsive processes in health behavior argues that health behavior can be guided by two independent systems: an impulsive system that is relatively automatic and a reflective system that involves self-control and cognitive processing to guide behavior. In addition, other lines of work suggest that actual engagement in behavior may, over time, become habitual and no longer involve active, effortful decision making, thus leading to a further dissociation in intention versus behavior processes (Ouellette and Wood, 1998; Verhoeven et al., 2012).
Affective associations and decision making
To the extent that intentions to engage in a behavior and actual behavioral practices are not functionally equivalent, it may be the case that the decision-making processes involved in forming an intention may be different from those involved in actually engaging in the behavior. To explore this possibility, we examined decision-making factors predicting actual behavioral practices and tested whether those factors also predicted relevant behavioral intentions. This was done within the context of the behavioral affective associations model, a decision-making framework that has been shown to successfully predict actual behavior in a number of health-related domains (Kiviniemi and Duangdao, 2009; Kiviniemi et al., 2007, 2014; Walsh and Kiviniemi, 2014).
Most formal models of health decision making focus on the cognitive beliefs one holds about the behavior. Cognitive beliefs include the information one associates with the behavior (e.g. benefits of engaging in the behavior) and perceptions of ability to engage in the behavior (e.g. self-efficacy). In addition, both anecdotal evidence and research findings suggest that individuals also have affective associations with particular behavioral choices. Anecdotally, most people have one or more “comfort foods” which they associate with positive affect. This association of positive affect with specific foods has been documented in the literature (Aikman et al., 2006; Wansink et al., 2003). Associations of affect with other health behaviors have also been documented (e.g. negative affective responses with novel foods, Birch and Marlin, 1982; affect associated with exercise, Frederick et al., 1996; embarrassment associated with condom use, Leary et al., 1994).
Past work has shown that affective associations relate to behavior choices (Blundell and Finlayson, 2004; Chapman and Coups, 2006; Lawton et al., 2007; Loewenstein and Furstenberg, 1991). Kiviniemi et al. (2007) recently developed and tested a decision-making model describing both the relation of affective associations to behavioral choices and the integration of affective associations with cognitive beliefs as a guide to decision making.
Two key tenets of the behavioral affective associations model are relevant here. First, affective associations guide behavioral choices; as affective associations become more positive, likelihood of engaging in the behavior increases. Second, affective associations serve as a proximal mediator of the relation between cognitive beliefs and behavior. The relation between cognitive beliefs and behavioral choices is mediated through affective associations. Figure 1 provides a pictorial overview of the model; a fuller explication of the tenets and supporting evidence from other domains can be found in Kiviniemi et al. (2007, 2009).
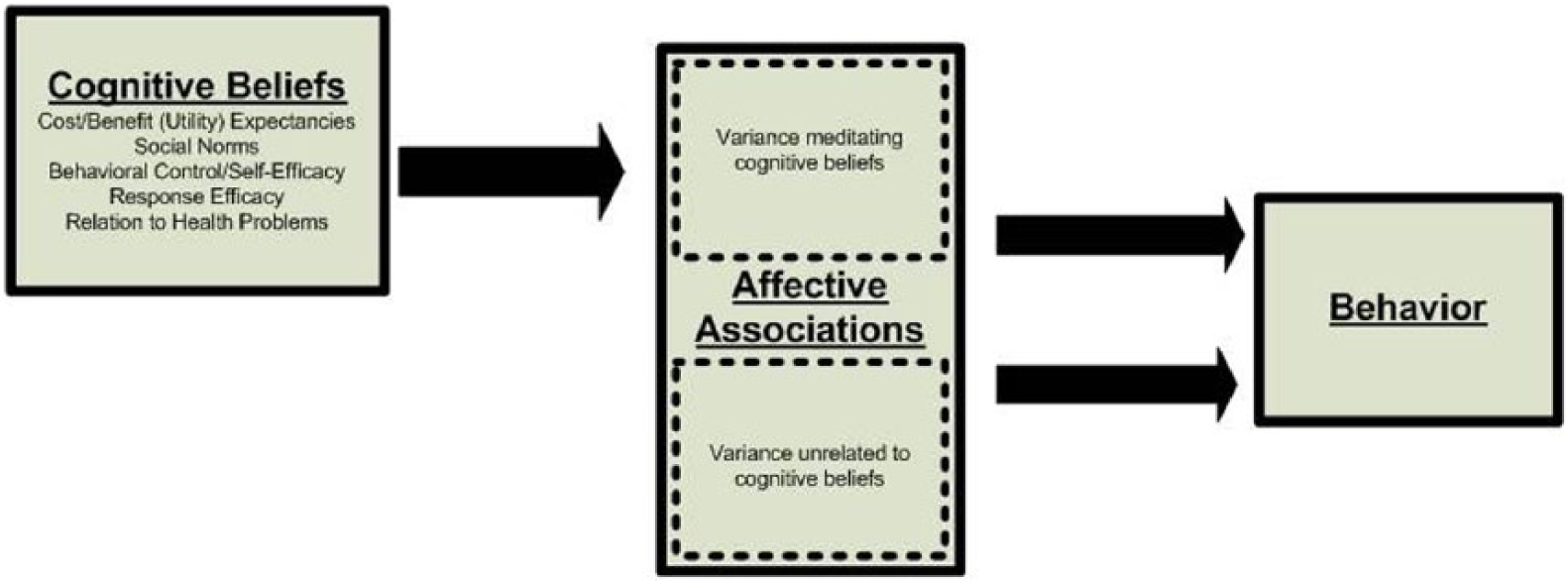
Behavioral affective associations model.
The utility of the model was originally demonstrated in a study examining decision-making predictors of physical activity behaviors (Kiviniemi et al., 2007). In this study, more positive affective associations were significantly related to higher levels of physical activity. Mediational analyses showed that the relation between the cognitive beliefs constructs from the health belief model and theory of planned behavior and activity behavior was mediated through the affective associations construct. In addition to physical activity, supporting evidence for the model has been shown for fruit and vegetable consumption (Kiviniemi and Duangdao, 2009), cancer screening (Kiviniemi et al., 2014), and research participation (Kiviniemi et al., 2013).
Current studies
The central topic of this article is whether the factors predicting actual engagement in a behavior will be the same as or different from the factors predicting behavioral intentions. On the one hand, the standard conceptualization of intention as a necessary mediational step that connects social cognitive factors to behavior leads to the prediction that factors associated with intentions and with behaviors would be the same. On the other hand, the literature reviewed above highlights a number of situations where behavior is not directly tied to intentions, leading one to predict that the determinants might be separate and distinct.
Using the behavioral affective associations model as a framework, we examine these two competing predictions in a series of studies examining the role of affective associations and cognitive beliefs as predictors of actual dietary behaviors and of intentions relevant to those behaviors. In Study 1, we examined current consumption of several specific foods and intentions to change consumption of those foods in the immediate future. In Study 2, we examined decision making for intentions to diet to lose weight and current consumption of high-fat foods. In both studies, we explored which factors (cognitive beliefs and/or affective associations) predicted actual consumption relative to those predicting intentions.
Study 1: cognitive beliefs and affective associations related to intentions to consume specific foods
In Study 1, we examined the role of affective associations with and cognitive beliefs about different foods (both general categories of foods, such as high-fat foods, and specific food items, such as pizza) as predictors of both behavioral intentions to consume those foods and current consumption of each food item. Because behavioral intentions and actual consumption were assessed at the same level of specificity, this study provides the most direct analogue to the situation specified by most decision-making models—if intentions guide behaviors and both are guided by the same set of decision factors, both should be predicted by the same pattern of affective associations and cognitive beliefs. By contrast, if intentions and behaviors are driven by different decision-making factors, different relations between affective associations and cognitive beliefs as predictors should emerge.
Method
Participants and procedure
166 participants (41 males, 121 females, 4 did not indicate; average age = 19.8 years, standard deviation (SD) = 1.84 years) took part in the study in exchange for extra course credit. Of participants, 38 percent said they were currently dieting. Participants completed the study in small groups of 3–5. Participants answered questions about their affective associations with and cognitive beliefs about both general categories of foods (high-fat foods, low-fat foods, fruits and vegetables, and desserts) and specific food items (low-fat yogurt, pizza, hamburgers, turkey sandwiches, carrots, and chocolate chip cookies). After completing the questionnaires, they received an educational debriefing.
Measures
Affective associations
For each food category or food item, participants answered six questions assessing their affective associations with that food. Each question consisted of the question prompt “When I think about eating ______, I feel” followed by either a positive or a negative affect word (positive: delighted, happy, joyful; negative: sorrow, sad, annoyed). These questions were modified from the affectively based attitudes scales developed by Crites et al. (1994). Participants responded to each question using a 9-point scale with endpoints of 0 = not at all true of me and 8 = very true of me. To create composite measures of affective associations for each food, negative affect items were recoded and the mean of the six items served as the measure of affective associations (average α = 0.84).
Cognitive beliefs
Cognitive beliefs about each food category or food item were assessed with six items assessing participants’ beliefs about the utility of eating each food. For each question, the stem “When I think about eating _____, I think of it as” was followed by either a positive (useful, beneficial, valuable) or a negative (harmful, worthless, useless) word. Participants responded on a 9-point scale with endpoints of 0 = not at all true of me and 8 = very true of me. These questions were modified versions of the Crites et al. (1994) cognitive components of attitudes scale. As with the affective associations measure, the mean of the items (with negative items recoded) served as the measure of cognitive beliefs (average α = 0.77).
Current behavior
Participants reported their current consumption of each food category or food item by writing a numerical response to the question “On average, how many servings of each of the following types of food do you currently eat each week?”
Intentions to change behavior
To assess intentions to change behavior, participants responded to the stem “Over the next month I think that my frequency of eating _____ will” for each food category or food item. Participants responded to each question using a 5-point scale with endpoints of 1 = decrease a great deal and 5 = increase a great deal.
Results
Decision-making factors predicting current behavior
We first examined whether the relation of affective associations and cognitive beliefs to current behavior for each of the 10 food categories or items matched predictions of the behavioral affective associations model. The model predicts that the relation between cognitive beliefs and consumption of a given food will be mediated by affective associations with the food. Table 1 reports the univariable and multivariable regression slopes for the relation between cognitive beliefs and affective associations as predictors of current behavior. As can be seen in Table 1, when examined separately in univariable analyses, both cognitive beliefs and affective associations are associated with current behavior; as both cognitive beliefs and affective associations become more positive, self-reported behavior increases. This pattern is consistent across all 10 of the behaviors.
Standardized regression weights of cognitive beliefs and affective associations separately and together predicting current behaviors (i.e. consumption) for each food, Study 1.
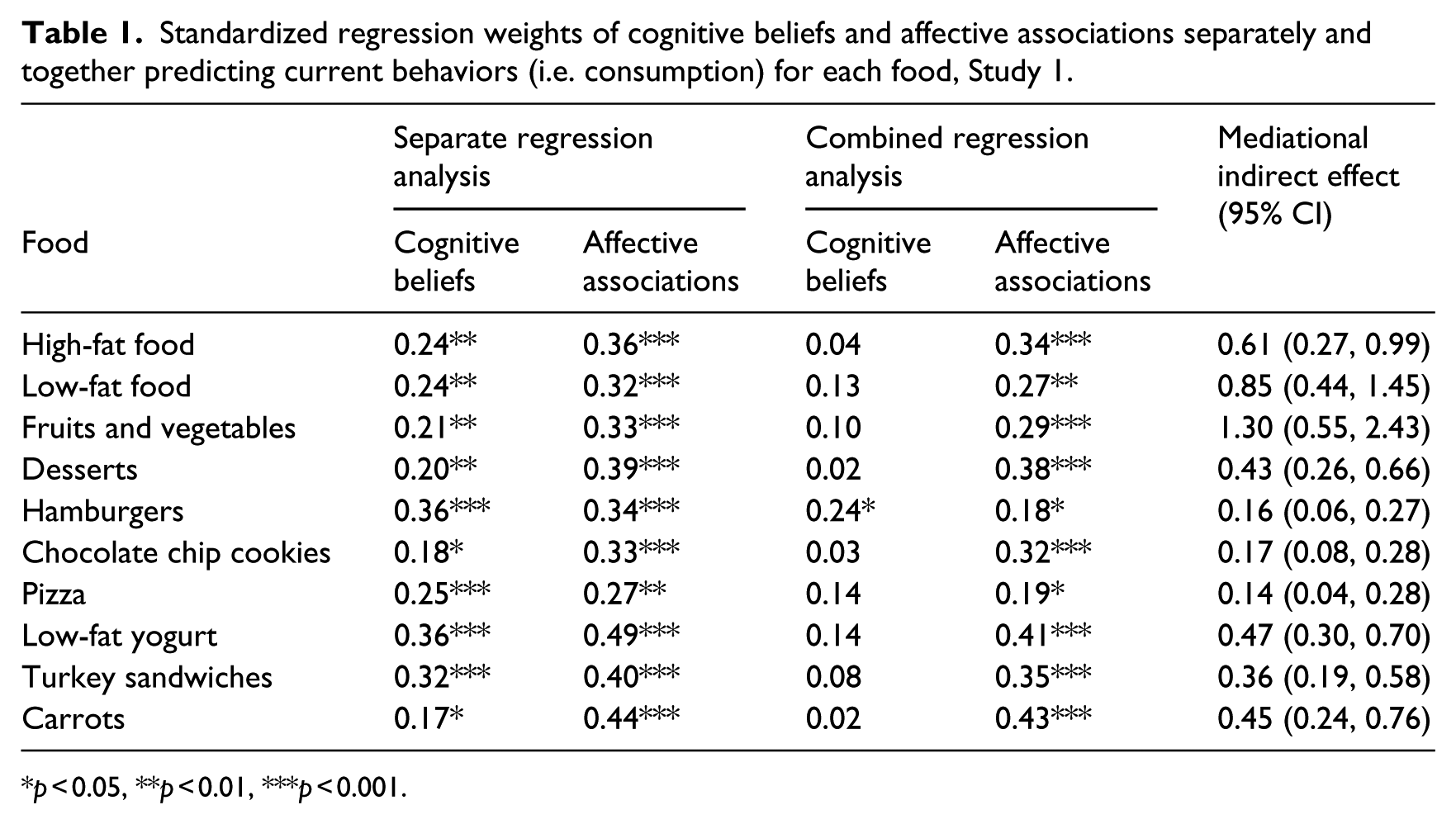
p < 0.05, **p < 0.01, ***p < 0.001.
Examination of the multivariable relations demonstrates a mediational effect. The indirect (mediated) effect for each behavior was assessed in a path-modeling approach with bootstrapped estimates of the indirect effect using Hayes’ PROCESS program (2012). For every behavior, the indirect effect of cognitive beliefs on behavior as mediated by affective associations was positive and significant (as indicated by a 95% confidence interval (CI) that does not include zero). For 9 of the 10 behaviors, there was no longer a significant direct effect in the multivariable model. For one behavior (hamburgers), the cognitive beliefs direct effect remained significant.
Behavioral intentions
Having demonstrated that the interrelation of affective associations and cognitive beliefs with dietary behavior follows the mediational pattern predicted by the behavioral affective association model, we examined whether this pattern would also hold for intentions to change behavior. We first examined the relations among cognitive beliefs, affective associations, and behavioral intentions for each food. To do so, we estimated regression equations in which cognitive beliefs and affective associations were entered as predictors, and intentions to change behavior served as the criterion variable. Because behavioral intentions may be dependent on current behavioral patterns, we included current consumption as a covariate in all analyses.
The results of these analyses can be found in Table 2. For 8 of the 10 foods, cognitive beliefs were significantly related to intentions to change food consumption, even when current consumption was taken into account; as cognitive beliefs became more positive, likelihood of intending to increase consumption increased. Unlike the relation with current behavior, however, this relation between cognitive beliefs and behavioral intentions was in no way mediated by affective associations with the behavior. For all eight foods that were significantly related to intentions, the cognitive beliefs–behavioral intention relation remained significant when affective associations were included in the model, and there was no predicted indirect effect. For 7 of the 10 behaviors, affective associations were not significantly related to intentions to change consumption.
Standardized regression weights of cognitive beliefs and affective associations separately and together predicting future intentions for each food, Study 1.
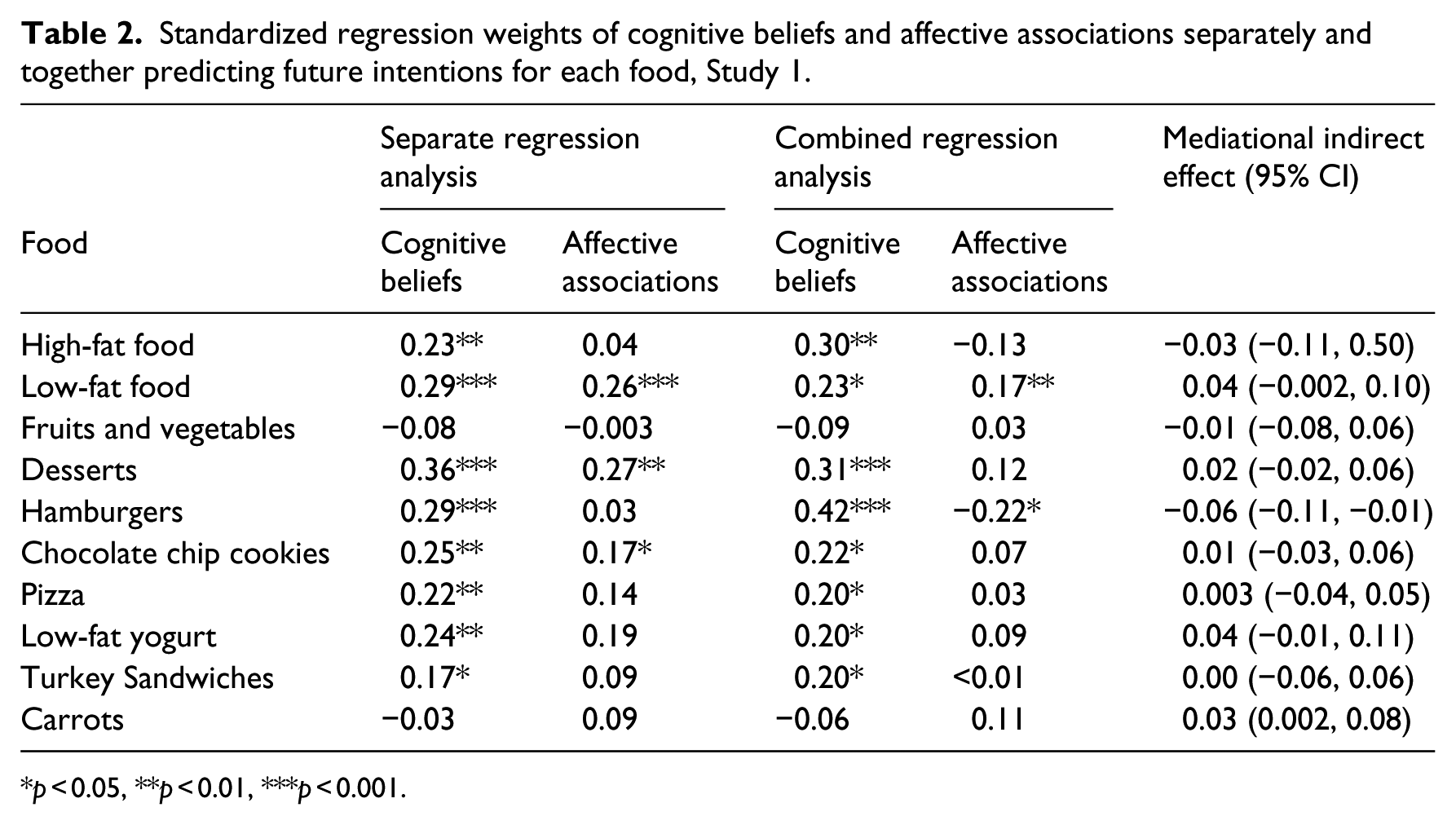
p < 0.05, **p < 0.01, ***p < 0.001.
Discussion
The results of Study 1 demonstrate a consistent dissociation between the decision-making processes relating to engagement in actual dietary behavior relative to those relating to behavioral intentions about specific behaviors. When examining engagement in actual behavior, the proximal predictor of individuals’ decisions was affective associations with the behavior. Affective associations mediated the relation between expected utility beliefs and behavior. By contrast, intentions to change behaviors were associated with more “purely” cognitive factors; by and large, affective associations did not relate to plans to change consumption of foods, and in no case was the relation between cognitive beliefs and intentions mediated by affective associations. This dissociation between factors related to behavioral intentions, and actual behavior was found across multiple dietary practices and for both general, global categories of behavior and specific dietary choices.
Although this pattern of dissociation suggests a reason why plans to change behavior do not always translate into actual behavioral practice, these findings differ in an important way from the way that individuals may plan behavior change. Specifically, in Study 1, the intentions assessed were about changes in specific food choices (either categories of foods or specific individual foods). By contrast, much of the focus in the weight control arena is on more global intentions (e.g. “I plan to diet”; “I plan to lose weight”). Although there certainly are situations where one forms intentions for specific food types (e.g. being told by a physician to reduce red meat consumption), individuals are likely to form their weight control intentions at a more global level, as when forming an intention to diet in order to lose weight. Thus, an important question for this line of inquiry is whether the decision factors that predict more global plans to diet to lose weight are similar to those predicting one’s actual behavioral practices.
We examined this question in Study 2. In Study 2, we examined factors relating to weight-loss plans and those relating to consumption of high-fat foods. Participants reported their feelings about consuming high-fat foods, perceptions of advantages and disadvantages of high-fat food consumption, current high-fat food consumption, and intentions at both a specific level (plans to change high-fat food consumption) and a more global level (plans for weight loss). Moreover, to ensure that the results in Study 1 were not due to methodological features specific to the measures, conceptually distinct operationalizations of cognitive beliefs, affective associations, intentions, and current high-fat food consumption were used. As with Study 1, both cognitive beliefs and affective associations with high-fat foods were examined as factors relating to both current behavior and behavioral intentions.
Study 2: cognitive beliefs and affective associations related to intentions to diet
Method
Participants and procedure
Participants were 104 young adults (25 males, 79 females; average age = 20.2 years, SD = 2.79 years) who took part in the study in exchange for extra course credit; 49 percent of participants said that they were currently dieting. Participants completed a questionnaire about their affective associations with and cognitive beliefs about high-fat foods, current consumption of 13 high-fat foods, intentions to reduce high-fat food consumption, and intentions to diet to lose weight. Participants received an educational debriefing at the conclusion of the study.
Measures
Affective associations
Affective associations with high-fat foods were assessed using a single-item measure. Participants reported how much they enjoyed eating high-fat foods using a 9-point scale with endpoints of 0 = I do not enjoy them at all and 8 = I enjoy them a great deal.
Cognitive beliefs
Participants indicated their cognitive beliefs by completing a single-item measure of their perceptions of the relative advantages and disadvantages of eating high-fat foods. Participants responded on a 9-point scale with endpoints of 0 = the disadvantages greatly outweigh the advantages and 8 = the advantages greatly outweigh the disadvantages.
Current behavior
High-fat food consumption was assessed using a 13-item closed-ended measure developed by Coates et al. (1995). Participants were given a list of 13 different types of high-fat foods (e.g. “In the past 4 weeks, how often did you eat French fries or fried potatoes?”) and reported behavior using a 4-point scale with the following response options: 0 = never, 1 = at least once per month, 2 = at least once per week, and 3 = at least once per day. Responses were summed to create a measure of high-fat food consumption.
High-fat food consumption intentions
Participants responded to three items concerning their intentions to reduce high-fat food consumption (e.g. “I intend to eat fewer high fat foods in the future”; modified from Povey et al., 2000). Participants responded using a 9-point scale with endpoints of 0 = definitely do not and 8 = definitely do. The mean of the three items served as a measure of high-fat food consumption intentions (α = 0.89).
Dieting intentions
Participants were asked a single yes/no question about whether they were currently trying to lose weight (modified from Wardle et al., 2004). Participants who answered yes were asked how much weight (in pounds) they were trying to lose. The combination of these two items was used to create a measure of intended weight loss in pounds, with those indicating that they did not intend to lose weight receiving a score of 0 pounds.
Results
Current behavior
We first examined separate regression models with cognitive beliefs and affective associations as predictors of current high-fat food consumption. All analyses included gender and weight as covariates because these variables were related to food intake. Controlling for these variables did not alter the pattern of results. As predicted by the behavioral affective associations model, both cognitive beliefs and affective associations were significantly and positively related to consumption of high-fat foods; for both, as beliefs/associations became more positive, high-fat food consumption increased, cognition β = 0.21, affect β = 0.33, t(90) = 2.05 and 3.28, respectively, both ps < 0.05. Furthermore, cognitive beliefs about and affective associations with high-fat foods were significantly and positively correlated, r(97) = 0.46, p < 0.001.
We then conducted mediational analyses to determine whether the relation between cognitive beliefs and behavior was mediated through affective associations. When affective associations were included in a regression model with cognitive beliefs as a predictor and high-fat food consumption as the criterion, the relation between cognitive beliefs and behavior became non-significant, β = 0.07, t < 1, ns, whereas affective associations remained significant, β = 0.30, t(86) = 2.77, p < 0.01. Bootstrap modeling of the indirect effect showed a significant indirect effect of cognitive beliefs on behavior mediated by affective associations; indirect effect = 0.40 (95% CI = 0.09, 0.85).
Intentions to change high-fat food consumption
We next examined the relation of cognitive beliefs and affective associations to participants’ intentions to change their high-fat food consumption. We estimated separate regression models with the decision-making variable (either affective associations or cognitive beliefs) as a predictor and intentions to change high-fat food consumption as the criterion variable. As with Study 1, given the likely constraints placed on behavioral intentions by current consumption, we controlled for reported current consumption of high-fat foods in these analyses.
Examination of the relation between cognitive beliefs and intentions to change high-fat food consumption revealed that as beliefs about the relative utility of high-fat food consumption became more positive, individuals had lower intentions to decrease consumption of high-fat foods, β = −0.44, t(89) = −4.55, p < 0.001. By contrast, affective associations with high-fat food consumption were unrelated to intentions to decrease high-fat food intake, β = −0.19, t(89) = −1.79, ns.
Intentions to diet to lose weight
Finally, we examined the relation between cognitive beliefs, affective associations, and intentions to diet to lose weight. As with intentions to change high-fat food consumption, this was done by estimating separate regression models with cognitive beliefs and affective associations as predictors of intentions to diet to lose weight. As with intentions to change high-fat food consumption, cognitive beliefs about high-fat foods were significantly and negatively related to intentions to diet to lose weight; as one’s cognitive beliefs about the utility of high-fat foods became more positive, intended weight loss decreased, β = −0.23, t(92) = −2.22, p < 0.05. By contrast, affective associations with high-fat foods were unrelated to dieting intentions, β = −0.09, t < 1, ns.
Discussion
Consistent with Study 1, the results of Study 2 also demonstrate a dissociation between the pattern of decision-making inputs that relate to actual behavioral engagement relative to those that relate to intentions. As in Study 1, individuals’ actual consumption of high-fat food was associated with a cognition–affect mediation model. The proximal predictor of behavior was affective associations, and the relation between cognitive beliefs and behavior was fully mediated through those affective associations, consistent with the predictions of the behavioral affective associations model. By contrast, intentions were associated with cognitive beliefs alone. Moreover, Study 2 extends this notion of differential impact by examining intentions at two levels of specificity, specific intentions to change consumption of high-fat foods and more global intentions to diet for weight loss. Both types of intentions replicate the Study 1 findings, thus providing more generalizable support for the notion of a dissociation between predictors of planning versus action.
General discussion
Collectively, these studies demonstrate a robust difference in the decision-making processes associated with intentions to engage in dietary behaviors relative to those processes associated with actual engagement in the behaviors. In each study, intentions to engage in behaviors were primarily related to the cognitive beliefs individuals held about the behavior in question. This was true when intentions were assessed at the level of consumption of individual foods (Study 1), broader food categories (Studies 1 and 2), and overarching intentions to lose weight (Study 2). This was also true for three separate and distinct ways of framing the operational question about intentions. By contrast, affective associations play a central role in the decision-making process involved in behaviors, including both individual foods (Study 1) and broader categories of foods (Studies 1 and 2), and across two different ways of operationalizing the behavioral measures.
Implications for understanding health decision making and health behavior
These results suggest a potential answer to the question raised earlier—why does there seem to be so little connection between intentions to diet to lose weight and successful weight control? If dieting intentions are not mediated by affect (and indeed, not associated with affect at all), then one answer to the question may be that the factors leading people to form intentions to diet may be at least partially distinct from those factors influencing their dietary behavior. In particular, there are two important distinctions to be made. First, as with our previous work (Kiviniemi and Duangdao, 2009; Kiviniemi et al., 2007), these results indicate the importance of distinguishing between cognitive beliefs about the behavior and affective associations with the behavior. Second, consistent with the distinction between planning and action (e.g. Gollwitzer, 1999), our results suggest the need to distinguish between decision planning systems chiefly centered around cognition and action systems with affective associations as a central input.
Perhaps more importantly, our results demonstrate that there is a dissociation in how decision-making inputs are used to form intentions to engage in behaviors relative to their use for determining actual behavioral practices. Why might such a dissociation exist? It seems safe to assume that the decision-making process involved in forming behavioral intentions is one that (a) takes some cognitive effort on the part of the decision maker; (b) tends to take place at times when the decision maker has the cognitive resources available to sustain that cognitive effort; and (c) takes place when the decision maker is motivated to put forth the necessary cognitive effort.
By contrast, decisions about actual behavioral engagement, especially on-the-spot decision making about what to consume at a particular meal, may be influenced by whatever immediate personal and environmental circumstances influence the decision maker’s motivation and ability to engage in effortful cognition. Thus, there may often be times when, because of time pressures, stress, lack of motivation, or other factors, the reasoned, effortful process required for cognitively based health decisions may not take place. Because most models of affect and decision making assume that affective systems operate automatically, the affectively based decision system would not be limited by such personal and environmental circumstances and thus would be more likely to guide actual behavioral engagement. Such automatic, affective processes may become even more pronounced influences on actual behavior when the behavior becomes habitual and is therefore not subject to ongoing, active decision making (Ouellette and Wood, 1998; Verhoeven et al., 2012).
Additionally, our data suggest a possible explanation for one of the intriguing patterns found in the distinction between intentions and actions. Orbell and Sheeran (1998) have demonstrated that the predominant reason for a lack of relation between intentions and action is due to a group termed inclined abstainers, individuals who form a behavioral intention but then do not translate that intention into actual behavior. Our findings suggest that one reason for the phenomenon of inclined abstention might be that affective associations do not predict decisions about behavioral intentions but do predict actual behavioral engagement.
Limitations
There are, of course, limitations to the current studies that should be noted. Most notably, the behaviors examined here were all common, frequently enacted behaviors (indeed, few participants reported never engaging in the behaviors addressed). As such, they may be behaviors for which individuals have formed behavioral habits, which might reduce the influence of more effortful cognitions, especially those related to behavioral intentions, on actual behavior. For habitual behavior, habits predict behavior more strongly than intentions, whereas for more novel behaviors, intentions predict better than habits (Ouellette and Wood, 1998). Our findings might therefore be more applicable to well-ingrained behavioral choices than to novel action domains. Arguably, though, most health behavior self-regulation issues concern ongoing patterns of behavior like those studied here.
Second, it should be noted that the measures were paper-and-pencil and included retrospective reports of ongoing behavioral practices. As such, the assessments were made in ways and at times which did not include factors such as the presence of food and time pressures. Thus, the behavioral reports are somewhat divorced from the actual decision-making context. However, such factors are likely to exacerbate rather than ameliorate the role of affective associations in behavioral decision making, and thus, we might find even stronger effects in more naturalistic settings. Nonetheless, it is important to note this difference between our studies and naturalistic decision-making contexts. Finally, the measures were self-reported and used specific operationalizations and scale points. As with all self reports, there is a potential for biased reporting of behavior. As with all closed-ended measures, different scale point choices may modify results.
In addition, the nature of the study design and of the measures used should be considered in assessing the results. The study design was cross-sectional and therefore the behavioral reports involved retrospective reporting of past behavior, whereas the intention measures involved future behavior. Longitudinal work in which cognitive and affective measures are used to predict both future intentions and future behavior would be a valuable addition.
Conclusion
Collectively, the two studies presented here demonstrate a persistent and marked disconnect between the decision-making factors predicting individuals’ engagement in dietary behaviors relative to those which account for intentions relevant to those behaviors. Given the strong trend of rising obesity rates in the United States and the failures of dieting intentions to successfully counter weight gain, these findings have strong implications for addressing the public health concerns associated with the obesity epidemic. To the extent that existing intervention strategies target cognitive components which may influence planning but may not directly influence actual consumption, individuals may persist in dietary strategies which contribute to suboptimal energy balance and thus weight gain in spite of intervention attempts.
Footnotes
Funding
This research was supported by US National Cancer Institute grant CA106225 to the first author (M.T.K.).