
Abstract
A qualitative study among women living with HIV assessed the aspects of an evidence-based intervention targeting HIV transmission risk reduction (Women Involved in Life Learning from Other Women [WiLLOW]) that women valued and how their lives were impacted. Thirty-one women (80.6% African American) completed interviews. Women valued the personal stories and positive group dynamics (i.e. safety, trust, openness, getting feedback, bonding, and socializing). As a result of WiLLOW, women embraced a strong woman image, joined groups, changed behaviors, accepted their HIV status, became optimistic, and spoke up/advocated in their relationships and communities. Interventions for HIV-positive women may benefit from incorporating the sharing of stories in their curricula and factors that build positive group dynamics.
Introduction
In the United States, women represent 20 percent of all new HIV diagnoses and over 240,000 women are currently living with HIV (Centers for Disease Control and Prevention (CDC), 2015). The primary route of HIV infection for women is heterosexual contact (CDC, 2015). A myriad of psychosocial issues place women at risk of HIV, including poverty, childhood sexual abuse, interpersonal violence, mental health diagnoses, substance use, and sexual risk behaviors (Myers et al., 2003). Once infected, women living with HIV (WLH) are at risk of transmitting HIV to their partners. The CDC have noted that prevention strategies for lowering the incidents of new HIV cases should include interventions for lowering HIV transmission risk behaviors among individuals living with HIV as well improving their overall quality of life (CDC, 2013).
Interventions aiming to reduce sexual risk behaviors among people living with HIV (PLWHA) have shown promising findings. Johnson et al. (2006) conducted a meta-analysis on 15 randomized controlled trials (RCTs) for sexual risk reduction among PLWHA and reported that on condom use (not number of sexual partners) intervention participants reported lower sexual risk compared to control participants. Similarly, a more recent meta-analysis of 21 RCTs on interventions for sexual risk reduction among PLWHA by Yin et al. (2014) found a lower likelihood of unprotected vaginal or anal intercourse for intervention participants compared to the control participants. However, it is noteworthy that 20 of the 21 studies were conducted with majority male or all male samples.
There are limited interventions for HIV transmission reduction among women with HIV that have demonstrated efficacy and effectiveness (Collins and Diallo, 2010; Painter et al., 2010). However, interventions specifically designed for women are needed because of the unique issues and needs of women with HIV. For instance, the lives of WLH are impacted by gender-based violence, gender role expectations, poverty/unemployment, and power inequalities that also impact women’s ability to negotiate condom use and sex (Dale et al., 2014; Remme et al., 2014). A recent review of seven qualitative studies on the experiences of WLH and the role of support groups (Paudel and Baral, 2015) found five overarching themes of (1) HIV disclosure; (2) HIV-related discrimination and stigma; (3) internalized stigma; (4) rejection and differential treatment by family, providers, and friends; and (5) the benefit of support groups to combat stigma/discrimination. Participants described support groups as a venue for women to be among others with similar situation, rehearse for HIV disclosure, and increase their support network (Paudel and Baral, 2015). However, research is still needed to examine the efficacy of these support groups among WLH.
The only evidence-based intervention (EBI) for WLH included in the recent Yin et al. (2014) meta-analysis was the WiLLOW (Women Involved in Life Learning from Other Women) program developed by Wingood et al. (2004). It is a CDC-sponsored EBI for women with HIV that encourages gender pride, strong social networks, knowledge of HIV and sexually transmitted infection (STI) transmission, skills in communication and condom use, productive ways to cope with stress, and healthy relationships. In an RCT, WiLLOW demonstrated efficacy in significantly reducing unprotected vaginal intercourse, increasing the likelihood of using condoms, lowering the incidence of sexually transmitted bacterial infections, and improving HIV knowledge and social networks (Wingood et al., 2004).
Although WiLLOW has accumulated evidence in HIV transmission reduction, we are lacking a qualitative in-depth understanding of women’s perspectives on features/mechanisms of the group that they found valuable and ways in which they believed WiLLOW impacted them. The women’s perspectives may suggest possible mechanisms for change shown by the intervention as well as aspects of group interventions to highlight and foster in order to maximize women’s satisfaction and gain. The present qualitative study sought to gather information on the perspectives of women who recently completed a WiLLOW program.
Methods
Participants and study design
Participants were graduates of an intervention for WLH (i.e. WiLLOW) at a large hospital in Boston, MA. The WiLLOW program consisted of four weekly group sessions (4–5 hours each), 8–10 women, a female lead facilitator, and a WLH peer facilitator. To participate in WiLLOW, participants had to identify as female, be living with HIV and be aware of their diagnosis for at least 6 months, speak English, and be over age 18. Any graduates who completed all four sessions of the WiLLOW program were eligible to participate in the current qualitative study. Forty participants were randomly selected for recruitment from a list of WiLLOW program graduates using Microsoft Excel. Selected participants first received an introductory letter from the WiLLOW Program Coordinator/Lead Facilitator (with whom they had a relationship) describing the study and notifying them that the research staff would be in touch. Research staff then contacted participants up to four times by telephone to see whether they were interested in completing an hour-long interview. We were unable to contact five women, and three women declined to participate. Interested participants were scheduled for an interview and received a reminder call the day before.
Thirty-two of the recruited participants agreed to participate and all completed the interviews. All interviews were conducted in a private room at the hospital by qualified research staff including a PhD-level associate faculty with expertise in qualitative research methods, a fifth-year Clinical Psychology PhD candidate with over a decade of experience in qualitative research methods, and a research assistant who was trained by the faculty and PhD candidate to conduct the interviews using a semi-structured interview guide. Participants gave their consent before beginning the interview and received a snack, drink, and US$25 gift card to a local store as incentives. One interview was excluded because the audio recorder did not record the interview. Thirty-one interviews were recorded, transcribed, and analyzed. The Boston University Medical Campus Institutional Review Board approved this study.
Measures
Socio-demographic variables
Information was obtained at WiLLOW baseline visits on participants’ marital status (never married, married, separated, divorced, or widowed), education level (eighth grade or less, some high school, high-school graduate/General Education Development (GED), some college, bachelor’s degree, or postgraduate), first language (English, Spanish, Portuguese, Haitian Creole, and others), ethnicity (not Hispanic/Latina, Hispanic/Latina, and don’t know), race (American Indian or Alaskan Native, Asian, Black or African American, Native Hawaiian or Pacific Islander, White, and don’t know), and age.
Interview protocol
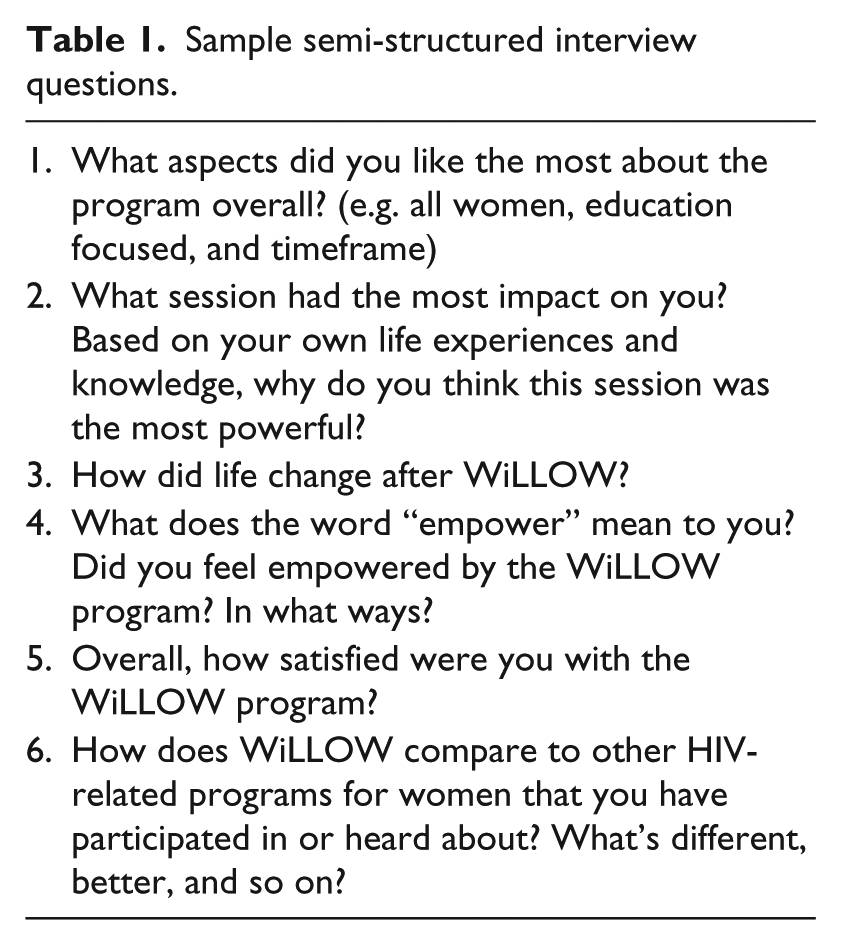
A semi-structured interview guide was used and interviewers were instructed to ask probing or follow-up questions as needed. The guide discussed areas including participants’ perspectives on the group and ways in which their participation in WiLLOW impacted their lives. Table 1 provides a list of semi-structured interview questions that were asked. Interviews were audio recorded and ranged from 15 minutes to over 1 hour.
Sample semi-structured interview questions.
Data analysis
Audio interviews were transcribed and managed in Microsoft word documents. Grounded theory was used to code for common themes and content. A small sample (n = 6) of transcribed interviews were read by multiple coders (a PhD-level faculty, a fifth-year psychology PhD student, a Master’s-level psychology student, and a senior undergraduate psychology student) who came to a consensus about how to define and recognize emerging themes and content. The master’s level and senior psychology students were trained to code the themes/content by the fifth-year psychology PhD student. Four meetings (2–3 hours each) were held over the course of 2 months, and four iterations of the manual were developed. Once the final coding manual was developed to define the themes/content and guide coding of all the transcriptions, the two coders coded each transcription independently and met with the fifth-year psychology PhD student to have discussions and arrive at a group consensus for each code. Meetings were held on a weekly to biweekly basis over the course of 18 months.
Results
Sample characteristics
Thirty-two women participated in the interviews. One interview was excluded from the analysis because it was not audio recorded. Of the 31 participants included in the analysis, 25 were Black or African American, five were White, one was American Indian or Alaskan Native, and two identified as Hispanic/Latina. A total of 84 percent of women (n = 26) were born in the United States, and 94 percent (n = 29) learned English as their first language. The mean age was 48 years, and 87 percent of women were unmarried at the time of the interview. A total of 27 percent of participants had less than a high-school degree, 32 percent had completed high school or a GED, and 38 percent had pursued education beyond high school. Additional details on sample socio-demographics are presented in Table 2.
Sample characteristics and socio-demographic statistics of 31 participants.
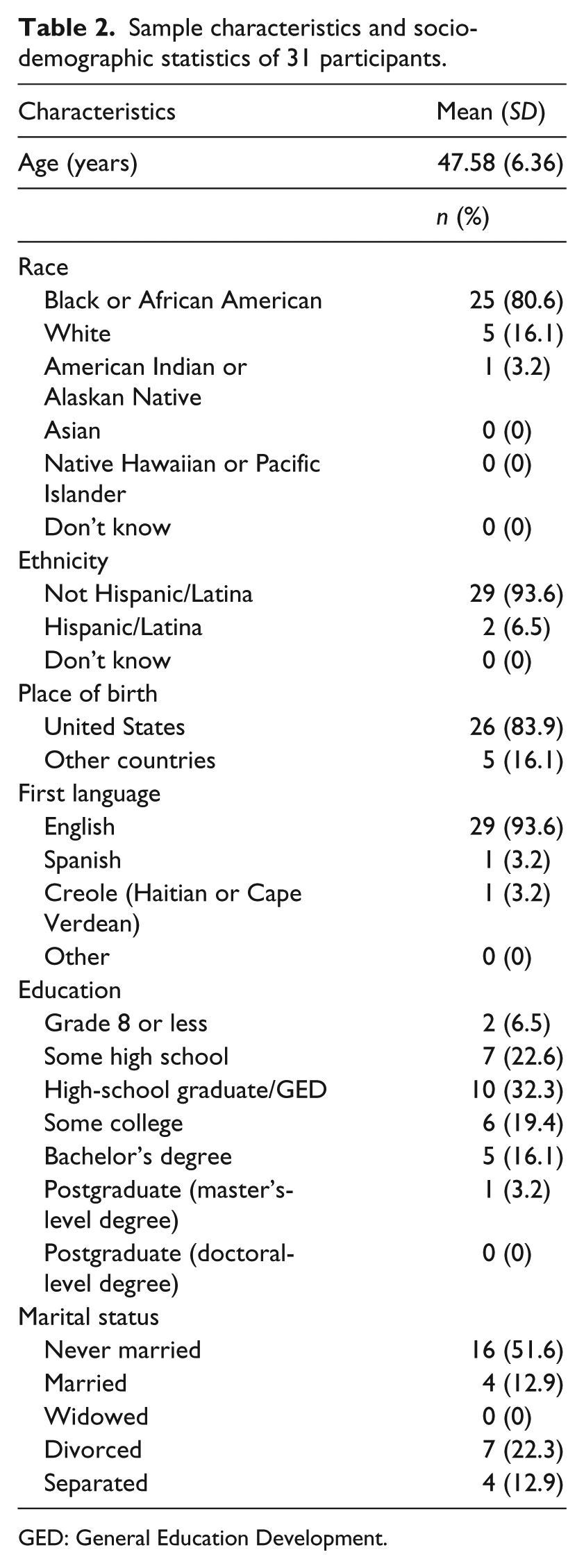
GED: General Education Development.
Themes
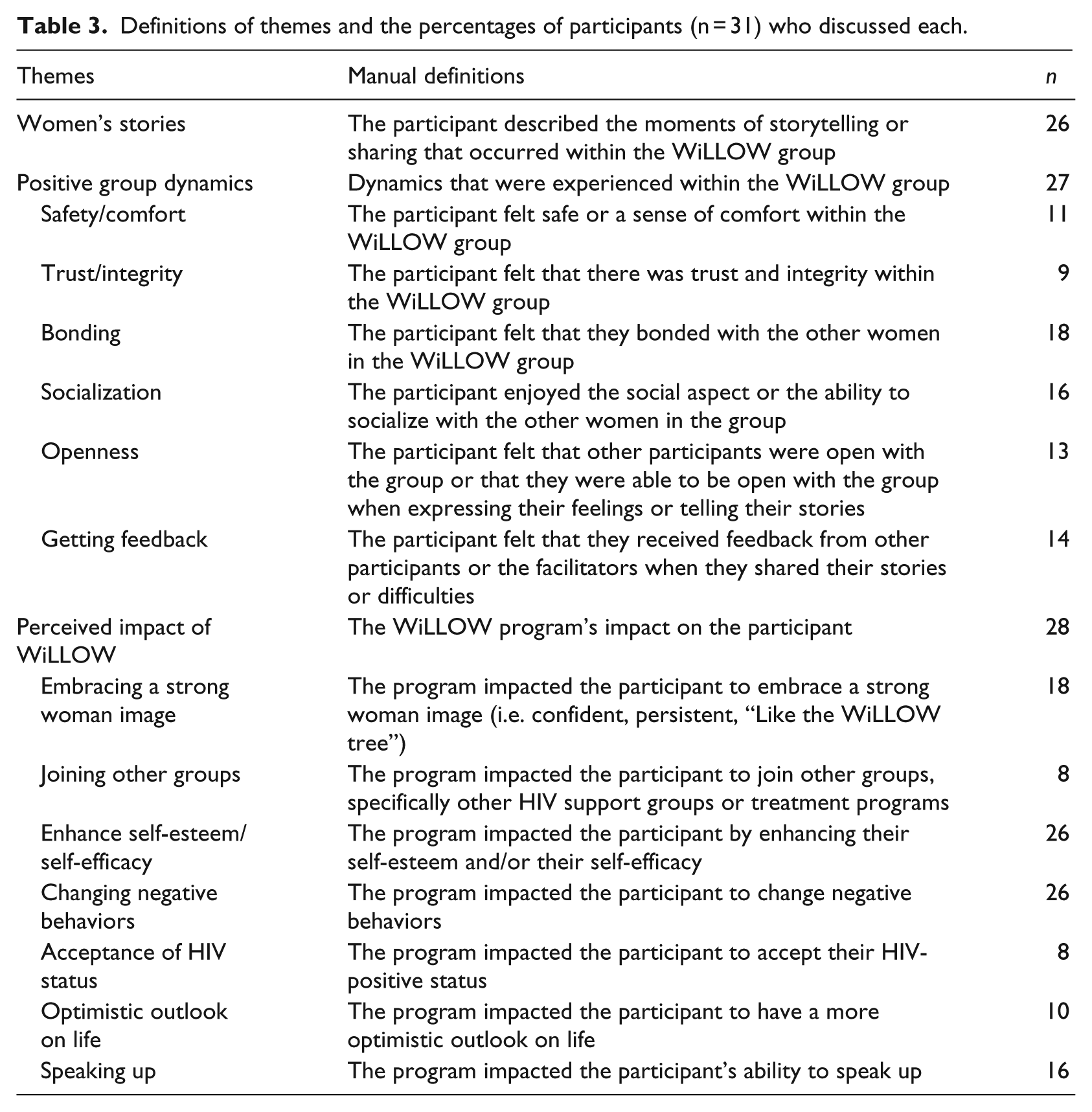
There were three overarching content areas that emerged from the women’s interviews—women’s stories, group dynamics, and the impact of WiLLOW. Women discussed the importance of hearing other women’s stories in group sessions, the value of having positive group dynamics such as trust, and the ways in which WiLLOW impacted self-views and behaviors. Within the content areas of group dynamics and WiLLOW impact, additional subthemes also emerged. Table 3 provides a list of the content areas/themes and the number of participants who discussed each.
Definitions of themes and the percentages of participants (n = 31) who discussed each.
Women’s stories
The overwhelming majority of participants talked about listening to, identifying with, and valuing the stories told by other women in the group. Listening to each others’ stories provided opportunities to support each other around their experiences. According to two participants,
“Being in a group with women, we shared issues. They shared what they were going through; we all just shared in the group” and “we all could help one another out, even just by talking to one another, which is good.”
In each others’ stories, women also heard things that resonated with their own life journey and struggles: “I’m hearing other people’s stories, and I’m nodding, I’m tearing up with them and it clicked with me.”
Even in instances where women did not share a common experience, they felt touched by other women’s stories. One participant talked about not having a history of substance use, but feeling moved by other women’s stories of substance abuse and recovery. As she stated,
I love the women in the group, they know how to be honest with themselves, they came clean about their stories. So when I listened to their stories, they were powerful, powerful stories they tell. When I told my story they were like “wow, you don’t do drugs? You don’t smoke cigarettes, You don’t do any of it” … They’re trying to stop smoking, but it’s not easy for them.
In addition, women felt that there were lessons that they learned from and taught each other through their stories. For instance, one woman talked about how she identified with and benefited from hearing other women’s stories:
You learn a lot, I heard stories that opened my, you know, my thinking, you know? Why I’m doing this if I’m not comfortable, you know? I got, you know, because I used to use so much years, I thought I was not worth it, for nothing, you know? And talking with other women you realize it. You, you are soldier, you know? I survived in the streets and jail and everything, you know, and learning from other women and I thought things happen was the worst or what happened the worst, it happened to me. And hearing the stories of the WiLLOW women they, some of them are worse than me, you know? And they, they ok, and they doing it.
Another participant talked about sharing and listening to stories as a way to teach and learn techniques: “You know we all in the same category and we can help each other with different techniques or you know my story might help her, her story might help me in something.”
Positive group dynamics
In addition to valuing each other’s stories, women discussed aspects of the group dynamics that made the group memorable. Specifically, women discussed safety/comfort, trust/integrity, openness, getting feedback, bonding, and socialization. Participants shared how they felt safe and a sense of comfort within the WiLLOW group. According to one participant, “If our answer is wrong nobody don’t judge us.” The sense of safety was also associated with a theme of trust/integrity that emerged. Participants expressed feeling that there was trust and integrity among the women in the group. As one person explained, “People have opinions, people’s opinions, people’s input, which is great. Instead of just saying, ‘No, I don’t like that person, or what they’re saying’. Everybody is accepted equally on what they have to say, how they’re dealing with life.”
Participants also talked about openness as a positive aspect that added to their group experiences. Participants felt that other participants were open with the group and that they were able to be open with the group when expressing their feelings or thoughts. For instance, one participant said,
Well, the conversations. Being around a bunch of women and learning how to open up and just be free to say what you really feel about yourself and the situations that you’re in. Basically, just, I guess the females, being able to talk and really gettin’ some of your gut feelings out and everybody you know they’re listening and they really understand.
Getting feedback was another factor that participants recalled appreciating in the group. Participants felt that they received useful feedback from other participants and the facilitators when they talked about their issues and difficulties. One participant said, “I liked the program, you know, talk about even among us to understand that, you know, they have the same disease I have, you know? Give me some feedback.” Another woman spoke about helpful advice she received regarding her relationship:
The women would be like girl you don’t have to go home and cook, you go home and bring yourself something home to eat, he’ll eat, and it was those little kinda things that that they stood up for that I listened to and learned how to take him on.
Women also felt that they bonded with other women in the group in a way that was very special to them. As one participant described,
And that was, that was you know that everybody in there would take time and give you hugs, and we understand each other. You know, it’s, it’s the embracing ok, the love, there’s so much love in that room, that one room. Get every and you know whatever goes on in there stays in there but there was—it was so much that we listened to each other’s stories and what people going through and it’s like we just bonded, like a sister, you know it wasn’t like we was outside well this a friend, I don’t feel comfortable—no we just bonded, that bonding, that bonding was very very very special. Very special. And we all actually cried when we got ready to go home [laughter] everybody started crying cause there’s a lot of love there. That’s that bonding, yup, that’s that bonding.
Another woman spoke about how that bond lasted beyond the actual group as she would recognize other WiLLOW women based on the WiLLOW bags given at graduation:
WiLLOW had a lot to do with it but it also connected me to other people I know when I see who it is, in one of those bags sister, you know, hey. They know, you know but I believe that HIV positive people in general men and women we have a different kind of bond.
Participants also enjoyed the opportunity to socialize with the other women in the group. As one participant stated, “So when I got into WiLLOW I loved it. Yeah, it was fun, I loved the group. We did all kinds of stuff, played games, you know you get to talk amongst each other and it’s all women.”
Perceived impact of WiLLOW
In response to queries about how women believed that their participation in the WiLLOW program impacted them, participants discussed embracing a “strong woman” image, joining other groups, changing negative behaviors, accepting their HIV status, having an optimistic outlook on life, and learning to speak up on issues. Women talked about how through WiLLOW and fellow members they began to value the traits (e.g. confidence, persistence, and self-love) of strong women and see strength within themselves. One woman explained how she observed strength, hard work, and self-love in other participants: “Seeing the stages of work that women had done to be stronger women and be able to say without hesitation that they were HIV positive and that they loved themselves.” Another participant described how attending WiLLOW made her recognize her own strength as a WLH: “I learned that I am a strong positive woman, and before that I just wasn’t. I didn’t feel strong until I started coming and it gave me a lot to look at.”
Completing WiLLOW also encouraged participants to join other groups, specifically other HIV support groups or treatment programs. For instance, one participant noted that “It made me want to start getting more involved in other groups, and I’ve done one group since I completed WiLLOW and I graduated from that.” Women also shared their thoughts on how the program helped them to change behaviors such as relationship interactions with children and partners. One woman said, “Well, I think it made my relationships better with my boyfriend and my kids and it allowed me to look at other relationships that I had, like my relationship with my mother.” Another woman talked about returning to school as a result of WiLLOW: “Well, actually I started school, but I had to put it on the back burner because I was dealing with some court issues, but I’m going back to school in September.”
Similar to the “strong woman” image that participants discussed, participants also talked about how WiLLOW enhanced their self-esteem and/or their perceived self-efficacy in working on their goals. One participant shared how attending WiLLOW increased her self-esteem and self-efficacy to stay sober from substance use: “And every time I come to group, it made me stronger. It made me say, ‘oh I can do it’, I don’t have to keep relapsing and falling and getting back up, I can just stay on and stay.” Another woman said, “And the WiLLOW group showed me that I’m a capable woman and a woman that can be loved again you know and that stuck with me you know.”
Women also talked passionately about how WiLLOW impacted their acceptance of their HIV-positive status as echoed in the words of the participant below:
Yeah, it was really good for me though. Like I used to shy down and shut down from people. Now, I be like I don’t care, like [friend’s name] kept saying “Why you talking so loud about your medication” and I said “Because it’s my medication!” She’s like you talk too loud. But I don’t care who knows, and that’s something the group taught me too, like don’t be ashamed like you know what, there’s a whole bunch of people walking around with the same thing, just haven’t got checked. … All you can do is deal with it and go on with your life.
According to the women, the WiLLOW program also impacted them to have a more optimistic outlook on life and their health. Two participants described how being in WiLLOW and being supported by the other women helped them to view their HIV status and health more positively and to take the measures needed to stay healthy. One woman said,
It’s a hopeful story I think, because I believe that I’m gonna beat this thing I’m gonna be around for a very long time I’m not going anywhere you know um, I do what I’m supposed to do I take my meds, I listen to what I’m told from people who have had it fifteen almost sixteen years you know, I try to follow them, in their footsteps and see what they do to stay on top you know so … it’s me.
Another participant stated,
And plus it helps us to help ourselves. It help us to help ourselves, just like that motto says. We are women, and it I—it helps me. I don’t know about anyone else but it helped me, it helped myself, and they were there when I needed them the most. I mean I was going down and down more and more like getting suicidal don’t go anywhere, don’t got no friends, I’m dealing with this here, that’s what make me give up on my meds. And then I got in WiLLOW I went totally back. The girls put me back on cause see my body’s breaking down because I’m on chemo and dialysis so I eventually I have to get back on it but as long as I keep doing what in WiLLOW, she said if you keep doing what you’re doing, whatever you’re doing, and you get healthy, I don’t see no reason to put it on you yet.
Women also discussed speaking up more regarding their HIV status and other views related to sex to family and others. The words of the participant below describe how she spoke to her son about safe sexual behaviors and disclosed her HIV status to others including her church congregation:
Yes, there’s changes because like I thought I was going to be, I feel like I can be stronger with my son, say “Don’t have sex without condom.” And I teach him, I take the condom, I said, “(name), how can you …,” “Ma, those are too small for me, I need the X.” And I said, “You need? And I do, because we do that in here make a fist, and have the condom fit, I do it for him and I tell him, “Any girl that who want to go with you, without it, there’s the woman one’s. If they don’t want you to put it, then have them put it for themselves. It gotta be like that way. If it’s not, no sex.” And I say it and like I planned it and he goes, “Yes, Ma. I know that you love me, mommy, give me a hug.” I said, “That’s why your father is gone. You don’t have him anymore.” I mean, I disclose in a heartbeat. I do. [laughs]. I do. And maybe, it’s, I’m too outgoing with it. But, that’s me. I mean you don’t, don’t do me, but that’s me. I’ll tell you in a heartbeat, my status. I will tell you my status, even if you didn’t ask. I’ll tell to you. [laughs]. So, you know, you take me as you are. In my church, I stood up and let you know, this is me, I’m HIV positive.
Discussion
Among WLH who completed the WiLLOW program, we found that when asked to reflect on their group experiences, women highlighted the value of hearing/sharing each other’s stories, positive group dynamics, and areas in which they felt that WiLLOW impacted their lives. Through each other’s stories, women were able to identify with other women’s experiences, feel validated on their own issues, and learn lessons on how to address situations and cope. Women’s stories were told within a group context that benefited from positive dynamics including safety, trust, openness, giving/getting feedback, bonding, and socializing. In a group of other women with HIV, women felt that they were safe to share, trusted each other, could be open with their thoughts and emotions, received and gave helpful feedback, socialized with each other, and formed a strong bond that often lasted beyond the group sessions. According to the women, participating in WiLLOW impacted them in ways directly consistent with the contents taught in WiLLOW. Women attributed embracing a “strong woman” image, changing some old behaviors, and speaking up more within interpersonal relationships to participating in WiLLOW. The WiLLOW program emphasized gender pride, skills in communication, and healthy relationships. However, WiLLOW also impacted women in ways beyond the specific content of the WiLLOW program including accepting their HIV status, having an optimistic outlook on life, improved self-esteem/self-efficacy, joining other groups, and advocating within their communities.
Our findings here are consistent with themes highlighted by previous qualitative studies on the experiences of WLH (Lawless et al., 1996; Liamputttong et al., 2009; Medeley et al., 2009; Paudel and Baral, 2015). For instance, prior qualitative studies have noted that support groups may help WLH to address internalized HIV-stigma, HIV-related discrimination and stigma, and HIV disclosure (Lawless et al, 1996; Liamputttong et al., 2009; Medeley et al., 2009). A major theme in our analyses was increased acceptance of HIV status, which might occur simultaneously with a reduction in internalized stigma. Furthermore, women who talked about accepting their HIV status also shared that they more openly disclosed and spoke about their HIV status. WLH in this study also talked about advocating within their communities and sometimes this meant advocating for themselves or others in the context of HIV-related stigma and discrimination.
Some of the positive group dynamics that women noted and areas of impact are also supported by general research findings on group processes and the benefits of having a group of similarly identified individuals (Buckingham et al., 2013). In addition, in some group-based interventions such as Alcoholics Anonymous, members share personal stories as a method of obtaining support and motivating others to engage in healthy behaviors (Volker, 1994). Furthermore, oral traditions and storytelling have a strong history in the African American community and the majority of participants identified as African American (Banks-Wallace, 2002).
Implications for intervention and research
Findings from this qualitative study support the importance of fostering positive group dynamics and highlight specific factors that build group cohesion. Providers delivering group interventions for women with HIV can try to enhance some aspects noted by the women in their groups such as sharing of stories (e.g. incorporate story sharing in the intervention curriculum and have it modeled by the facilitators) and socialization (e.g. create downtime before or after group for women to engage with each other). Our findings also emphasize that the target outcomes of a particular intervention (e.g. reduction in sexual risk) may not be the changes that the graduates recall and value the most. Women in this study seem to especially value their new sense of pride around their identities as WLH. In addition, the women’s words echoed the high level of acceptability and impact that the WiLLOW program may have among women with HIV.
There are several implications for future research. One, studies are needed to evaluate women’s personal views on other group interventions beyond WiLLOW that are targeting WLH. Comparing the findings from each intervention might help us to further understand ways to increase the acceptability and level of impact of interventions for women with HIV. Two, it might be interesting to investigate whether the primary outcome targets of interventions for women with HIV are the same as the outcomes that women value the most. Three, it may be beneficial to examine how the relationships that women form with each other in a group intervention such as WiLLOW are maintained over time and relate to health outcomes longitudinally.
Limitations
The findings from this study might be limited by a few factors. First, participants were recruited from a medical center in the Boston area and therefore their views might not generalize to women in other geographic locations. Second, participants who were in this study may have agreed to participate because they had a positive experience in WiLLOW. However, we selected participants to contact at random from the list of women who completed WiLLOW. Third, women’s views about WiLLOW may not easily apply to other group interventions for WLH.
Conclusion
Despite the few limitations, findings from this qualitative study among WLH who completed the WiLLOW program highlighted the importance of hearing/sharing each other’s stories, positive group dynamics including safety and openness, and the variety of ways in which women believed that WiLLOW impacted their lives beyond the targeted outcomes of the intervention such as accepting their HIV status and advocating within their communities. Our increased understanding from this qualitative inquiry suggests possible group dynamics and features to foster in order to maximize the satisfaction and gain in group interventions for WLH. To end with the words of one participant,
I learned how to be a positive strong woman, I learned not to be ashamed of what I have or who I am, like to stand up for myself, don’t let nobody put me down or low rate me as a woman.
Footnotes
Acknowledgements
The authors are grateful to the research participants in this study and to research staff Andrea Roisten who assisted with recruitment and data management.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was partially funded by the Centers for Disease Control and Prevention, contract no. PS10-1003. Some of Sannisha Dale’s time was covered by 1K23MH108439-01 from the National Institute of Mental Health.Funding agencies had no role in the design or conduct of the study or in the collection, management, analysis, or interpretation of the data.