
Abstract
Unexpected health-endangering events that lead to an emergency department visit may be perceived as “wake-up calls” and induce significant changes in health-related behavior (“health shock” effect). This study uses two waves of a survey of 826 adults with depression and finds that having an emergency department visit(s) increased medication adherence by 7.6 percentage points (p < 0.05) relative to non-emergency department visitors but had no significant effect on counseling attendance (0.02% points, p = 0.380). Emergency department visits may provide an opportune teachable moment to initiate targeted interventions for positive behavioral change in adults with depression.
Introduction and background
Unexpected health-endangering events that trigger emergent medical encounters such as an emergency department (ED) visit or hospitalization may be perceived as “wake-up calls” and induce significant changes in health-related behavior (“health shock” effect) while, at the same time, enhance receptivity to medical advice (“teachable moments”) (Dohnke et al., 2012; McBride et al., 2003; Monti et al., 1999). Demonstration of these health shock effects for multiple conditions in diverse clinical settings has led to development of interventions that capitalize on behavioral changes induced by such encounters (Monti et al., 1999). These interventions rely on the fact that health shocks “prime” individuals to adopt health-promoting behavior patterns that they otherwise may not be inclined to accept, thus creating teachable moments. In this study, we examined whether a potential health shock associated with an ED admission led to a similar priming effect in depressed adults by exploring the relationship between ED visit(s) within the past year and adherence to antidepressant medications and attendance of physician-recommended counseling sessions.
Despite the growing recognition of the ED as an important setting for behavioral interventions in mental health conditions, its role in improving depression self-management is not well understood. A key question is whether ED visits, either the visit themselves or the illnesses or injuries precipitating them, can induce sufficient behavioral change to improve depression treatment adherence. If ED visit(s) resulted in improved adherence to treatment in patients with depression, then ED-based interventions aimed at enhancing self-management skills of depressed patients may prove useful by reinforcing such positive, but potentially transient behavioral changes (Cohen et al., 2011; Lawson and Flocke, 2009; Stubblefield, 1986).
ED-based interventions for improving self-management of depression are potentially important for several reasons. First, the growing prevalence of depression in the United States continues to impose a significant burden of psychological illness, disability, and lost productivity, and threatens to impair an already strained mental healthcare delivery system (Cuijpers et al., 2012; Greenberg et al., 2003; Lépine and Briley, 2011). Non-adherence to effective treatment (e.g. selective serotonin reuptake inhibitor antidepressants), which some studies suggest may be as high as 50 percent (Cantrell et al., 2006; Lin et al., 1995), remains a crucial and modifiable factor in reducing disease symptoms and preventing morbidity (Chong et al., 2011; World Health Organization (WHO), 2003). Second, EDs are frequently acknowledged as de-facto providers of treatment of depression for many individuals with limited access to treatment in non-ED settings (Harman et al., 2004; Larkin et al., 2009; Merrick et al., 2010). Almost one-third of the psychiatric visits to an ED are due to depression (Merrick et al., 2010), and some estimates suggest that the incidence of silent depression and occult suicidality in ED patients may be as high as 30 and 13 percent, respectively (Claassen and Larkin, 2005). Third, studies have documented that even patients who have regular access to a primary care physician have poor rates of keeping scheduled follow-up appointments after inpatient psychiatric admissions (Boyer et al., 2000). Enhanced receptivity to medical advice following an ED visit could potentially be exploited to improve patient compliance with follow-up and thus the transition to outpatient mental healthcare.
Methods
Study population and data collection
Our data come from the two waves of the Aligning Forces for Quality Consumer Survey (AF4QCS) that was conducted as a part of the evaluation of the Aligning Forces for Quality (AF4Q) initiative funded by the Robert Wood Johnson Foundation and originally covering 14 diverse regions of the United States (Scanlon et al., 2012). The goal of AF4Q was to improve health and healthcare quality through multi-stakeholder collaboration at the local community level. The first wave of the AF4QCS, completed in 2008, was a random-digit-dial (RDD) survey of adults (18 years or older) who had visited healthcare professionals during the previous 2 years for the care of at least one of five major chronic conditions (diabetes, hypertension, asthma, chronic heart disease, and depression). The sample was designed to be representative of chronically ill adults living in the AF4Q regions. The response rate for the first wave was 27.6 percent by the American Association of Public Opinion Research (AAPOR) standard and 45.8 percent by the Council of American Survey Research Organizations (CASRO) standard. All of the respondents from the first wave were contacted for the second wave, which was completed in 2012 with a panel response rate of 63.3 percent. Our study used the longitudinal subsample of the 826 adults with depression, who completed both waves of the AF4QCS. All data collection procedures for this study were approved by the Office for Research Protections, Institutional Review Board of the Pennsylvania State University.
ED visit(s)
Survey respondents were asked the following question: “In the past 12 months, how many times did you go to the emergency room to get care for yourself?” We dichotomized the responses and created an indicator for each respondent in both waves of the survey, for whether there was at least one ED visit reported. We refer to those who visited the ED at least once in the past 12 months as “ED users”, and others as “non-ED users”.
Adherence to depression treatment
We examined adherence to two aspects of depression treatment: medication and counseling. In two separate questions, the survey asked the respondents how often they took depression medications as their doctor recommended, and whether they were able to attend all counseling sessions as exactly recommended. Two indicators were created, respectively, for medication adherence (“always” = 1; “usually,” “half of the time,” “rarely,” or “never” = 0), and for counseling attendance (“all sessions” = 1; “most,” “some,” “few,” or “none of the sessions” = 0). These two indicators capture “perfect” medication adherence and “perfect” counseling attendance.
Empirical approach
We analyzed the relationship between depression treatment adherence and ED visit(s) using linear probability models with individual-level fixed effects. This allowed us to account for the time-invariant confounding factors that are not observed in the data. Our model also controlled for a number of important time-varying factors, including education, income, employment, health insurance type, self-reported health, comorbid chronic condition(s), having usual source of care, and number of primary care visits in the past 12 months. Our model is specified by the following equation

For respondent i, at time t, Y is the outcome (adherence to treatment for depression), ED is a binary indicator for ED use, X is a vector of time-varying individual characteristics, γ is the individual-level fixed effect, η is the time effect, and ε is the error term. The key coefficient in the model is α, which captures the impact of ED visits on adherence to depression treatment. Specifically, we tried to assess, for respondents who did not report ED visit(s) in the first wave of the survey, whether their adherence improved when they reported at least one ED visit in the second wave of the survey, compared with the other respondents who did not report any change in ED use. Standard errors were clustered to adjust for correlations across repeated observations.
Sensitivity analyses
Although our main empirical model controlled for all time-invariant factors, there still may be time-varying factors confounding the results. In this context, such unobserved time-varying factors are likely to cause negative bias in our estimates. For example, respondents who have improved self-efficacy over time (which is not observed in the data) are less likely to use the ED in the second period, but are more likely to also have improved adherence over the same period. Therefore, our estimate of the key coefficient is conservative and the magnitude of the true impact is potentially larger. Although we cannot directly test the potential bias due to unobserved time-varying factors, we provided some evidence for the direction of the bias by estimating the same linear probability model without fixed effects. Assuming that the unobserved time-invariant factors and the unobserved time-varying factors have similar confounding effects, we expect our estimate to be smaller and less significant if we remove the fixed effects from the model.
A key element of a health shock is its unexpected nature, which often induces re-evaluation of personal habits and behaviors that may have implications for future health (Lawson and Flocke, 2009). Individuals with repeated ED visits, especially after the initial one, would be less likely to perceive such events as unexpected. Consequently, when ED visits become more frequent, teachable moments will less likely form. We, therefore, hypothesized that respondents with a single ED visit would be more susceptible to behavioral changes due to health shocks and analyzed the differential impacts of ED visits depending on the frequency. Specifically, we trichotomized the ED use variable—those who did not visit ED, those who visited ED only once (infrequent users), and those visited ED more than once (frequent users)—during the past year and re-estimated our model.
Results
Table 1 shows the socio-demographic, health status, and healthcare-related characteristics for survey respondents with depression. Compared to non-ED users, ED users were more likely to be African American, have less family income, have no college education, be publicly insured, and have poorer self-rated health status. Although these respondents were less likely to have a usual source of healthcare, they had higher average number of visits to healthcare providers in the last 12 months.
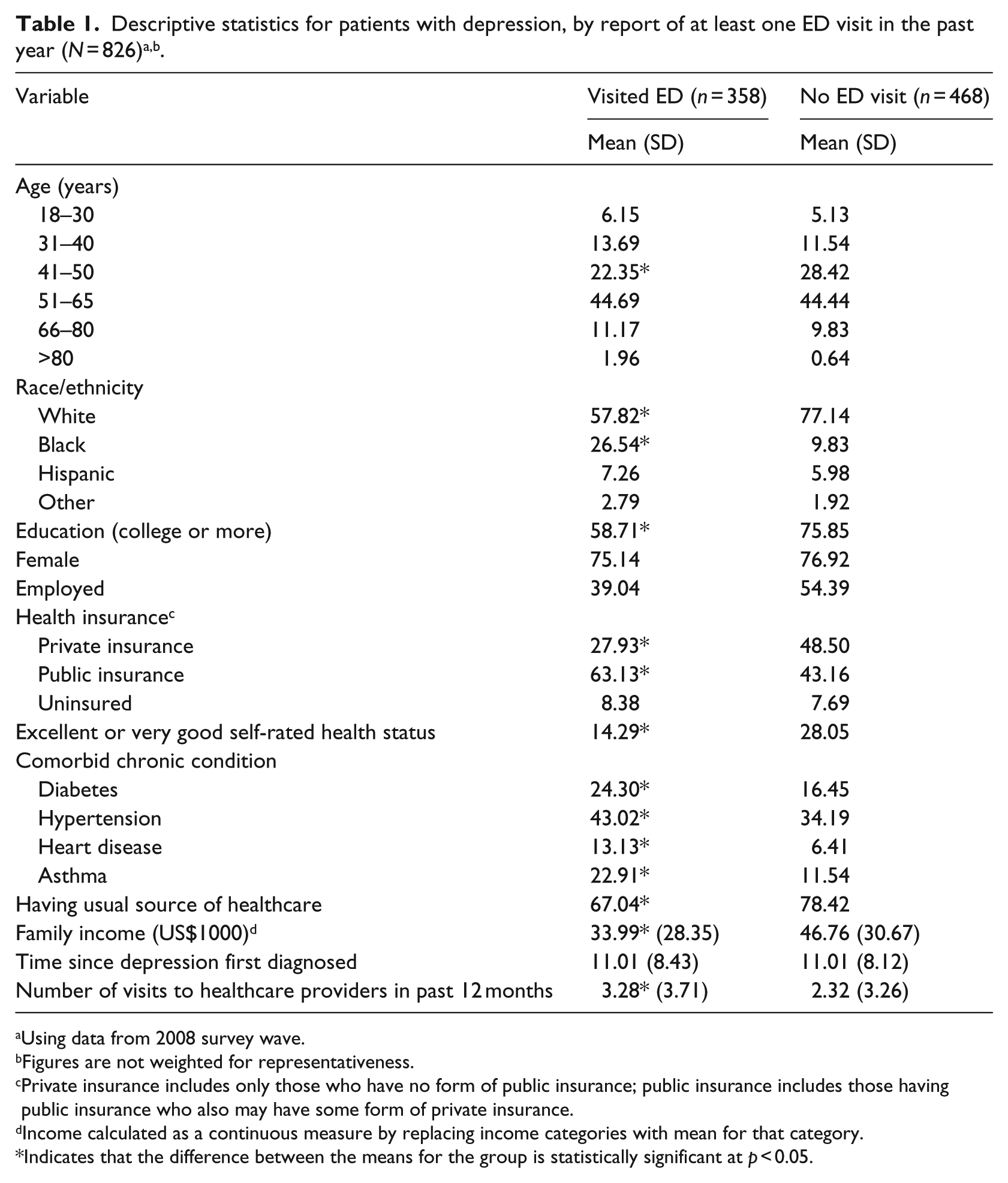
Using data from 2008 survey wave.
Figures are not weighted for representativeness.
Private insurance includes only those who have no form of public insurance; public insurance includes those having public insurance who also may have some form of private insurance.
Income calculated as a continuous measure by replacing income categories with mean for that category.
Indicates that the difference between the means for the group is statistically significant at p < 0.05.
Table 2 presents the results from the linear probability models with fixed effects (columns 2 and 4) and without fixed effects, showing the sensitivity of our main estimates to removal of fixed effects (columns 3 and 5). When we controlled for fixed effects, having ED visit(s) was associated with a significant increase in the probability of perfect adherence to depression medication (7.60% points, p < 0.05). Without controlling for fixed effects, the association between ED visit(s) and adherence to depression medication became smaller and insignificant. We did not find significant association between ED visit(s) and perfect attendance at counseling.
Effect of ED visits on adherence to antidepressant medications and attendance at psychological counseling sessions (baseline analyses).
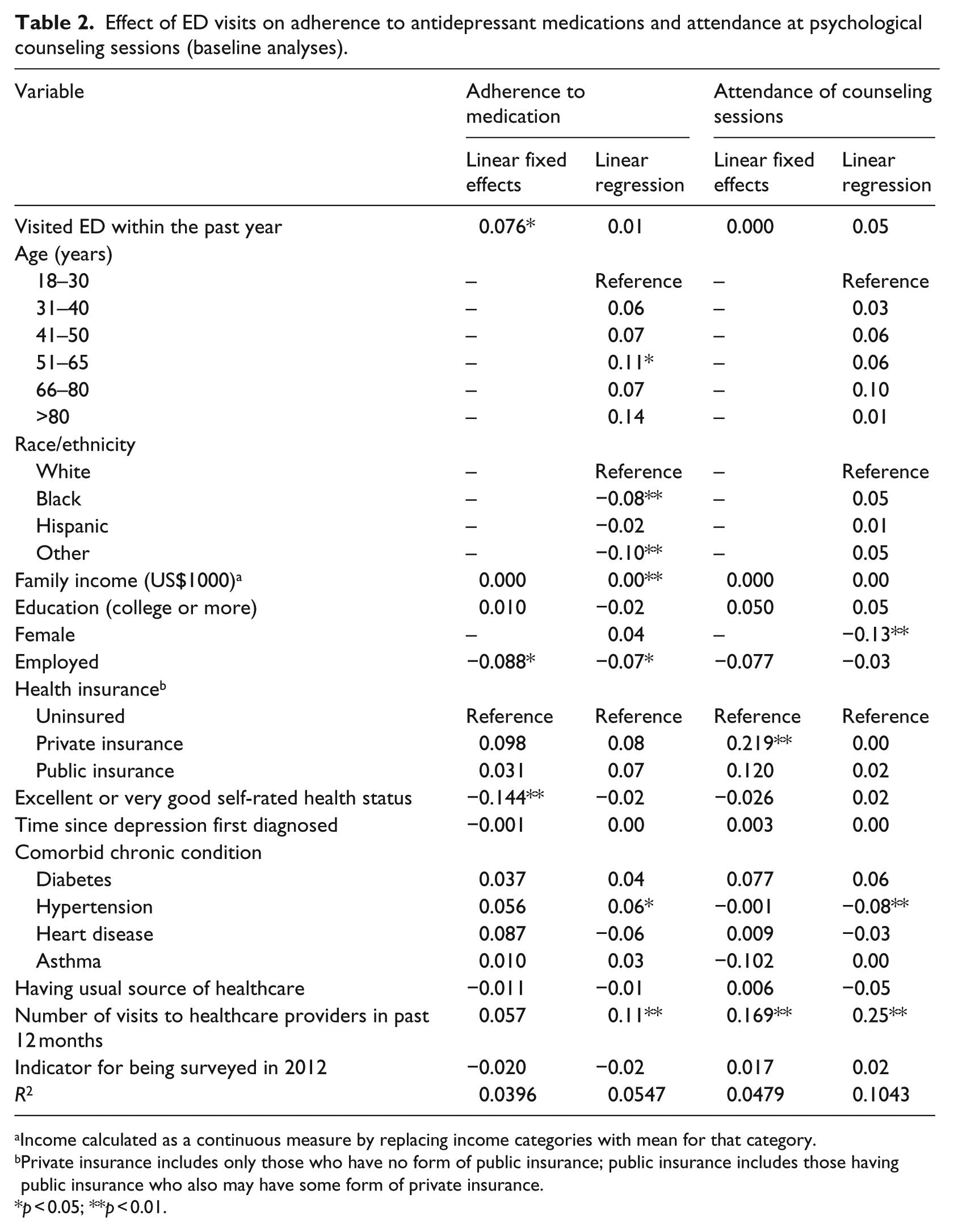
Income calculated as a continuous measure by replacing income categories with mean for that category.
Private insurance includes only those who have no form of public insurance; public insurance includes those having public insurance who also may have some form of private insurance.
p < 0.05; **p < 0.01.
Additionally, our sensitivity analyses examined differential impacts of single versus repeated ED visits. Our results (supplementary table available at: http://hpq.sagepub.com/) indicated that the effect of ED on medication adherence was large and statistically significant only for the subset of patients who visited ED just once in the past 12 months (9.5% point increase in likelihood of adhering with antidepressant medication, p < 0.05), while no such impact was found for patients who visited ED more than once over the same period.
Discussion
We found that having an ED visit(s) was associated with a 7.6 percentage point increase in the likelihood of perfect adherence to medications among adults with depression. Moreover, when we separated infrequent ED users from frequent users, this effect became stronger for the infrequent users (9.5 percentage points), but disappeared for the frequent users. However, we did not find any significant changes in attendance at counseling sessions related to having ED visit(s) within the past year. Overall, these results suggest a significant “health shock” effect of ED visit(s) in improving medication adherence among depressed patients and point to ED visits as a potentially valuable “teachable moment” for depression self-management. Although there may be unobserved time-varying factors that are not controlled in the analysis, as we discussed earlier, these factors (e.g. self-efficacy) are likely to be correlated with ED use and medication adherence in opposite directions and thus, negatively bias our key coefficient estimates. In addition, past literature also shows that poor adherence is systematically related to increased risk of having an ED visit and/or hospitalization (Pittman et al., 2010; Sokol et al., 2005). Therefore, both reverse causality and confounding factors in the context of this study may lead to underestimating the true effect of ED visit(s). Since our estimate of the key coefficient was positive and significant, the actual effect of ED visit(s) on medication adherence among depression patients may be even larger than what we found. This was consistent with results from the sensitivity analyses. After dropping the fixed effects from the model, the coefficient of ED visit(s) became smaller and insignificant. Assuming that the impact of unobserved time-varying factors is similar to that of unobserved time-invariant factors, we are likely to find larger effects if we can control for both types of factors in the analysis.
The concept of a “health shock” (Lawson and Flocke, 2009) provides a framework for understanding the mechanisms by which an ED visit may impact adherence. A variety of psychological, affective, motivation-related, and self-efficacy-related factors are thought to mediate the relationship between an adverse health event (resulting in an ED visit) and a health-beneficial behavioral change (e.g. adherence to medication; Cohen et al., 2011; Hochbaum, 1958; Monti et al., 1999). A heightened perception of personal risk and a greater perceived benefit of remedial actions, coupled with cueing events (e.g. access to healthcare-related information) in an emergent setting such as the ED, may trigger changes in self-care behavior, even without the benefit of interventional support (e.g. by self-linkage of a newly salient concern with adverse health behavior). However, these behavioral changes may be transient and vulnerable to relapse (Cohen et al., 2011; Lawson and Flocke, 2009; Stubblefield, 1986) unless an educative and emotionally supportive interventional framework is in place to fulfill the potential of such moments.
While we do not view the ED visit itself as an “intervention” to improve adherence, it is instructive to compare the magnitude of our effect size (7.6%) with results of studies that examined primary care-based interventions aimed at improving adherence to antidepressant therapy. These studies examined a broad variety of interventions composed of educational (audio-visual, telephonic, and by mailed materials), behavioral (pharmacy refill monitoring, mailed reminders), affective (motivational interviewing), and provider-directed (primary care physician education, pharmacist-led medication review, and management) elements. A recent review of this literature showed that the likelihood of adhering to antidepressant medication increased on average by 9.27 percent when patients were exposed to primary care-based interventions ((authors’ calculations) (Chong et al., 2011). Hence, our findings point to the unique opportunity available in an ED setting to potentially capitalize on the enhanced receptivity of patients by initiating interventions to improve adherence to depression medication. In particular, brief interventions that have a behavioral (e.g. reinforcing behavioral patterns that foster compliance such as using memory aids) and/or an educational component (e.g. providing educational material on depression treatment) may be effective when initiated in an ED setting (followed by transitioning to an outpatient site to ensure regular access and follow-up).
We found no significant relationship between ED use and attendance at counseling sessions for depression. This may partly be due to problems with access to psychotherapy for depression. Although the overall coverage for mental illnesses has become more generous over the past several years (Marcus and Olfson, 2010), studies have found declining rates of psychotherapy for depression treatment over the past decade; these trends have been partly attributed to carveouts of psychotherapy from managed-care contracts, and increased cost-sharing for psychotherapy for patients with mental disorders (Martin et al., 2000). This is consistent with our descriptive results which indicate that attendance at psychotherapy sessions was much lower than medication adherence for both ED visitors and non-ED visitors. Another reason the correlation is missing may be that adherence to recommended psychotherapy is more difficult and time-consuming than simply taking medication at the proper time, and may be especially vulnerable to recidivism absent proper educational and emotional support. For example, existing evidence suggests that consistent application of psychotherapeutic options (e.g. cognitive behavioral therapy) require attention to both adherence to theoretical protocol and skill in delivery, which often involves affective bonding between patient and provider (Choo et al., 2012).
Based on our findings, EDs may be an important venue for providing behavioral and educational interventions designed to increase adherence among patients with depression. However, our results also show that effective ED-based intervention may need to target infrequent (or first time) ED users. ED-based mental health interventions are debated in the literature (McKay et al., 2009). On one hand, the ED may be suboptimal for delivering even brief interventions because of high workload of ED physicians and their primary focus on stabilization of critically ill patients (Allen et al., 2002; Derlet and Nishio, 1990; Grumbach et al., 1993; Reeder and Garrison, 2001; Young et al., 1996). Indeed, many studies have documented excess wait times for ED patients and “boarding” of sick patients in ED hallways waiting for inpatient beds to become available, resulting in “overcrowding” (Le and Hsia, 2014; Schuur, 2014). On the other hand, a substantial proportion of ED visits for mental health conditions are by patients who are uninsured and poor, and who face a host of problems (e.g. low education, low health literacy) accessing community-based or office-based services, leading to poor transitioning to the primary care setting after a simple referral from an ED visit; hence, the ED may provide a crucial point for health behavior-targeted interventions in these patients for whom it may be the only source of care and who otherwise may be lost at follow-up (Chun et al., 2013; Larkin et al., 2009; Stone et al., 2012). Furthermore, for those ED users who have a regular access to an outpatient provider (e.g. primary care physician), the enhanced receptivity to medical advice may be exploited to ensure greater compliance with outpatient referrals, potentially leading to a timely follow-up and regular treatment at a mental healthcare facility. Hence, although we acknowledge the limitations of EDs as an interventional setting (e.g. provider burden, overcrowding), we generally concur with researchers (Larkin et al., 2009) who argue that EDs may be an important setting to reach subgroups that are especially vulnerable and unlikely to have access to effective medications/psychotherapy.
Our study has some important limitations. First, since the survey respondents were not asked about the specific reason for ED visits, we were unable to attribute the visits to depression or its complications. However, as noted above, a sizable proportion of patients who visit the ED for physical complaints also have mental health problems such as occult depression and suicidality (Claassen and Larkin, 2005). Moreover, our results remained unchanged when we ran our analyses on the subset of patients who reported having depression without any other chronic illness (a group more likely to visit the ED for complications related to depression). Second, studies have found that self-reported adherence may yield higher estimates than adherence measured by more objective methods. However, self-reported measures of adherence have been validated in many studies (Nguyen et al., 2014). Moreover, if tendency to report inflated estimates due to social desirability biases do not change significantly over time, it will be largely controlled in our fixed effects model. Third, our survey respondents were not asked whether an ED visit resulted in overnight hospitalization or about the precise timing of these events. Since hospitalization may also lead to behavioral changes, our results may partly capture the effect of being hospitalized and, hence, should be interpreted in light of this limitation of our data. Finally, our data lacked information on whether an ED visitor received any ED-based intervention or post-ED primary care intervention to improve self-management of disease. However, this may apply to only a small number of patients in our study sample since, to our knowledge, no ED-based interventions for depression self-management currently exist and the outpatient follow-up rates following referral from EDs after acute care for mental illness remain low (Currier et al., 2010).
In conclusion, we found that ED visit(s) result in improved adherence to antidepressant medication but not in improvement in attendance of psychotherapy sessions. Based on our results, we suggest that an ED visit may provide an opportune moment to initiate targeted interventions for positive behavioral change.
Supplemental Material
ED_Paper_Supplementary_Table – Supplemental material for Impact of emergency department visit on disease self-management in adults with depression
Supplemental material, ED_Paper_Supplementary_Table for Impact of emergency department visit on disease self-management in adults with depression by Neeraj Bhandari, Yunfeng Shi, Larry R Hearld and Megan McHugh in Journal of Health Psychology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded as a part of evaluation grant for Aligning Forces for Quality (AF4Q) program by the Robert Wood Johnson Foundation. Robert Wood Johnson Foundation had no role in the design and conduct of the study; collection, management, analysis, and interpretation of data; preparation, review, or approval of the article; or decision to submit the article for publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.