
Abstract
This study investigated the association of illness representations, awareness of bodily states and health complaints to self-rated health in N = 150 consecutive patients with heart disease (ischaemic disease, heart failure and heart valve disease) and explored differences between ‘health optimist’ and ‘health pessimist’ patients. After controlling for medical variables, health complaints accounted for 14.2 per cent of patients’ self-rated health, and illness representations contributed for another 16.2 per cent; body awareness was not associated with self-rated health. Also, ‘optimists’ tended to see less negative consequences from their illness and perceived greater control over illness treatment compared to ‘pessimists’. Targeting symptoms and illness representations may optimize rehabilitation outcomes.
Introduction
Despite improvements in outcomes, cardiovascular disease remains the leading cause of death and morbidity worldwide, with 3.9 million deaths and a cost of €210 billion a year only in Europe (Wilkins et al., 2017). There has been growing recognition that cognitive and emotional factors play a significant role in adjustment and coping with this chronic illness (Chiavarino et al., 2012; Piepoli et al., 2010), yet challenges still exist in the identification of the best variables to be targeted to lead different types of patients towards positive change (Whalley et al., 2014).
Self-rated health (SRH), a simple measure of the overall perception of one’s own health, has been established as a statistically reliable predictor of mortality, morbidity and functional status (DeSalvo et al., 2005; Idler and Benyamini, 1997), even after adjustment for socio-demographic, clinical and behavioural risk factors (Van Der Linde et al., 2013). These findings also apply to the cardiological field (Bosworth et al., 1999; Havranek et al., 2001; Rutledge et al., 2010), where the SRH measure is currently used and recommended for use both as a complementary outcome measure in research trials (Bjorner et al., 2005) and as an additional routine indicator for risk assessment in clinical practice (Benyamini et al., 2014). The idea is that SRH conveys, in a way that is non-invasive and meaningful to patients, relevant information which is not fully captured by existing clinical measures (Mavaddat et al., 2014).
However, the debate is still open over exactly what information people incorporate – consciously or intuitively – into their self-ratings of health. There is accumulating evidence that besides socio-demographic and formal medical information (e.g. diagnoses or medication), SRH may convey the individual’s perceptions at two distinct levels: (a) the conscious representation of health complaints (e.g. fatigue, tiredness and weakness), as information reflecting the unmeasured severity of symptoms of which the individual is aware (Barsky et al., 1992; Höfer et al., 2005; Mikolajczyk et al., 2008; Molarius and Janson, 2002), and (b) the intuitive awareness of somatic reactions and interoceptive processes (e.g. heart beat), which are perceived by the individual as bodily sensations not necessarily related to health complaints and are interpreted as directly reflecting one’s health status (Craig, 2003; Jylhä, 2009; Unden et al., 2007).
In addition, research shows that when faced with the acute and chronic symptoms of a disease, the subjective perceptions that individuals develop about the disease itself are important determinants of different aspects of recovery. According to the Common Sense Model (CSM) by Leventhal et al. (1984, 1997), the dimensions that people take into account are experienced symptoms which are attributed to the illness (identity), beliefs about the factors responsible for causing it (cause), impact on quality of life and functional capacity (consequences), beliefs about time course and cyclicity (acute/chronic and cyclical timeline), perceived controllability through personal coping behaviours and medical treatment (personal and treatment control), presence of negative emotions related to the illness (emotional representations) and degree of overall understanding of the condition (coherence). These lay illness representations are guided by personal, cultural and environmental contexts and determine coping strategies. In patients with heart disease, illness representations have been shown to predict occurrence of in-hospital complications (Cherrington et al., 2004), physical functioning and disability after discharge (Juergens et al., 2010) and attendance to cardiac rehabilitation programmes (French et al., 2006). There have been a few reports of associations between illness representations and SRH (Houtum et al., 2013; Weinman et al., 1996), and one study found that illness representations were a significant determinant of SRH, accounting for 18 per cent of its variance after controlling for medical variables (but not for other psychological variables; Aalto et al., 2006). However, to the best of our knowledge, a comprehensive assessment including health complaints, awareness of bodily states and illness representations in relation to SRH has not been carried out yet. A constructive approach combining the contribution of so far rather disconnected lines of research may provide a useful basis for an integrated conceptualization of the subjective components of SRH.
Another interesting issue in the study of perceived health concerns health congruence, that is, the relation of patients’ self-evaluations of health with measures of doctors’ evaluations (Chipperfield, 1993). Agreement rates are not very high, ranging from 50 to 68 per cent, which is not surprising in light of the above-mentioned evidence that patients’ SRH encompasses valuable information which cannot be captured either by objective clinical data nor by physician’s routine assessment (Mavaddat et al., 2014). More noteworthy is the finding that individuals reporting worse health than their doctor (the so-called health pessimists) show increased mortality rates and worse functioning, whereas ‘health optimists’ experience lower mortality and enhanced functioning, even after adjusting for objective health data (DeSalvo and Muntner, 2011; Kivinen et al., 1998; Ruthig et al., 2011). It has been suggested that the difference between health optimists and health pessimists may lay in their dissimilar cognitive and emotional attitude towards health (Borawski et al., 1996; Geest et al., 2004; Kivinen et al., 1998), and indeed, it has been shown that health optimism is associated with stronger perceived control over one’s condition (Hong et al., 2005; Ruthig and Chipperfield, 2007), attitudinal and behavioural (vs physical) health attributions (Borawski et al., 1996) and higher emotional well-being (Hong et al., 2004). However, no study to date has explored whether health optimist and health pessimist patients specifically differ in terms of health complaints, awareness of bodily states and illness representations.
This study had two specific aims. First, to investigate the association of (a) subjectively perceived health complaints, (b) awareness of body processes and reactions and (c) illness representations, with SRH in a sample of patients with heart disease. It was postulated that illness representations would be associated with SRH and explain further variance beyond the other two variables. Second, we aimed to explore differences in the same three variables between health optimists (patients giving a more positive evaluation of their health compared to their doctor’s) and health pessimists (patients giving a more negative evaluation of their health compared to their doctor’s).
Methods
Participants
All the patients consecutively admitted over a 2.5-year period to the Cardio-respiratory Rehabilitation Unit of the Humanitas Clinical Institute (Milan, Italy) were screened for participation in the study (N = 500). Inclusion criteria were a diagnosis of heart disease (ischaemic disease, heart failure, and heart valve disease), age not over 75 years, completion of primary education and good comprehension of written and spoken Italian language. Exclusion criteria were presence of concurrent pathologies affecting short- and medium-term prognosis (such as serious infection, cancer or significant organ dysfunction) and any history of stroke or psychotic illness. N = 327 patients did not meet the inclusion criteria or met one or more exclusion criteria, and N = 8 declined participation in the study.
Thus, 165 patients were enrolled in the study. Of these, 15 did not return the questionnaires. Of the 150 participants who completed all the required steps and were included in the analyses, 70.7 per cent were male. The mean age was 60.9 ± 11.0 years, and the mean education was 10.8 ± 4.0 years. The socio-demographic characteristics of the patients are shown in Table 1. The study was approved by the Ethics Committee of the Humanitas Clinical Institute (protocol ICH1036). All the participants were informed of their rights and signed an informed consent form before joining the study.
Patients’ socio-demographic characteristics (N = 150).
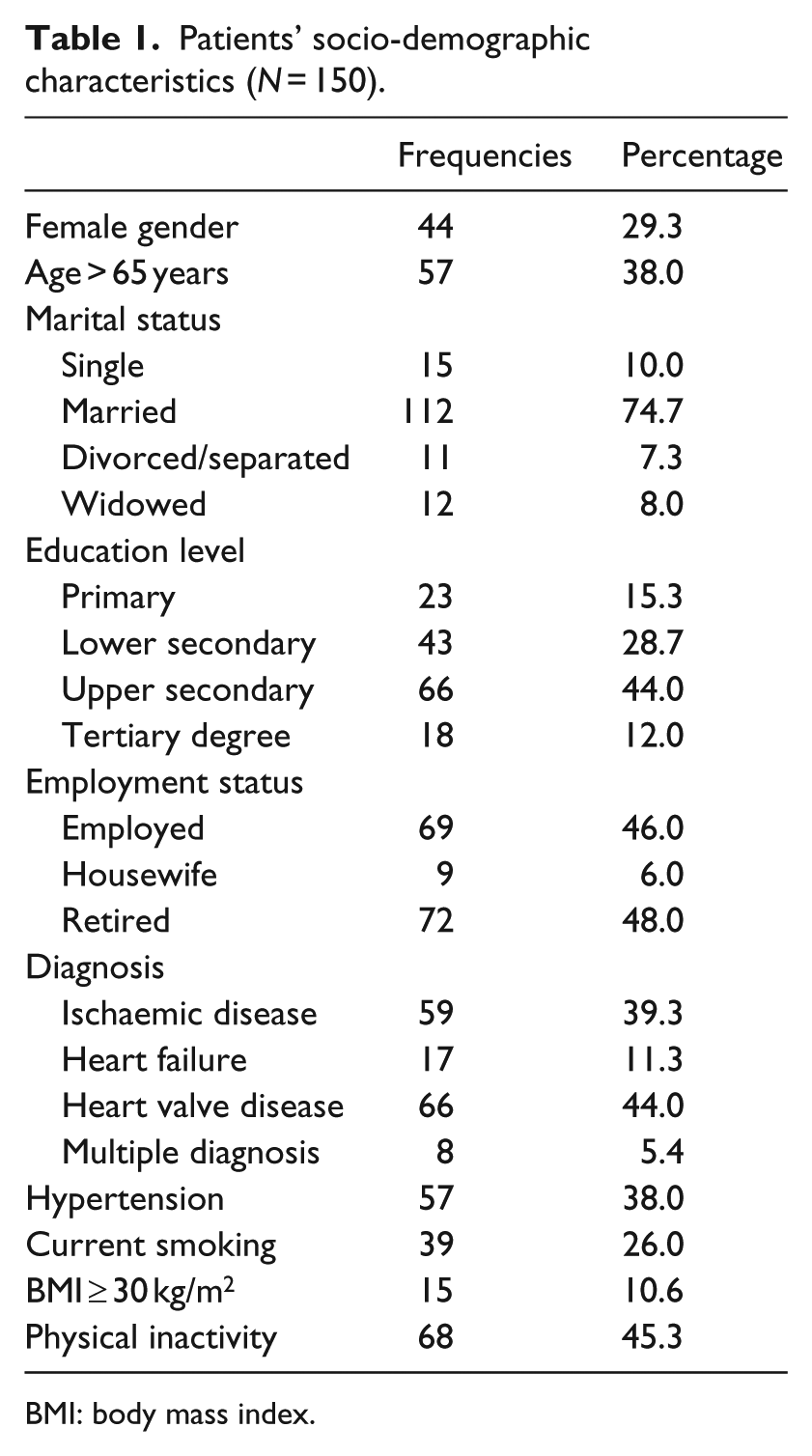
BMI: body mass index.
Measures and procedures
Eligible patients were informed about the study by the clinic’s psychologist and then completed the following instruments, preceded by a brief demographic section:
Self-rated Health–Self-evaluation (SRH-S). Participants were asked the question: ‘How is your health in general?’, with responses on a 5-point Likert scale ranging from 1 = very bad to 5 = very good (Robine and Jagger, 2003; World Health Organization, 1996).
Revised Illness Perception Questionnaire (IPQ-R; Moss-Morris et al., 2002). This self-report instrument investigates patients’ cognitive and emotional representations of their illness based on Leventhal’s CSM (1997, 1997, 1997; Leventhal et al., 1997, 1984). It comprises nine subscales: Identity (symptoms attributed to the illness), Consequences (beliefs about negative effects of the illness), Timeline acute/chronic (beliefs about duration of illness), Personal control (perception about controllability of the illness), Treatment control (perception about efficacy of the treatment to manage illness), Cause (beliefs about causes of the illness), Timeline cyclical (perception of illness/symptoms occurring in cycles), Illness coherence (extent to which individuals understand their condition) and Emotional representations (presence of negative emotions about the illness). The Identity subscale has a yes/no response format, while the other subscales are rated on a 5-point Likert scale ranging from 1 = strongly disagree to 5 = strongly agree. The IPQ-R has good internal reliability, test–retest reliability and predictive and discriminant validity (Moss-Morris et al., 2002). In this study, items of the Cause scale were considered individually as each represented a specific belief about the cause of the illness; for the other subscales, Cronbach’s alpha ranged from .65 to .86.
Body Awareness Questionnaire (BAQ; Shields et al., 1989). The BAQ is an 18-item questionnaire used to assess self-reported sensitivity to normal (i.e. not typically related to emotion or somatic complaints), body processes into four domains, which are not scored separately: sensitivity to body cycles and rhythms, sensitivity to small changes in normal functioning of body processes, ability to anticipate body reactions and ability to predict the onset of illness. Responses range on a 7-point Likert scale from 1 = not at all true to 7 = very true. It has good internal reliability, test–retest reliability and convergent and discriminant validity (Shields et al., 1989). In this study, Cronbach’s alpha for the BAQ was .82.
Health Complaints Scale (HCS; Denollet, 1994). This is a 24-item disease-specific questionnaire comprising two scales: a Somatic complaints scale assessing cardiac symptoms (cardio-pulmonary problems, fatigue and sleep problems) and a Cognitive complaints scale measuring feelings of disability (worries about health and concern about functional status). Patients rate how much they suffer from a particular symptom on a 5-point Likert scale ranging from 0 = not at all to 4 = extremely. The HCS has good internal reliability, test–retest reliability and construct validity (Denollet, 1994). In this study, Cronbach’s alpha was .89 for the Somatic Complaints Scale and .94 for the Cognitive Complaints Scale.
Self-Rated Health–Doctor-evaluation (SRH-D). Participants’ doctors were asked the question: ‘How is [name of patient]’s health in general?’, with responses ranging on a 5-point Likert scale from 1 = very bad to 5 = very good.
Statistical approach
Simple regression analyses were conducted to assess the relation between the study outcome (patients’ SRH-S) and the psychological variables (health complaints, awareness of bodily states and illness representations); for the Cause scale of the IPQ-R, only the three most frequently endorsed causal beliefs were considered (those with the highest percentage of participants assigning a score of 4 or 5): hereditary factors (48.6%), stress or worry (42.1%) and smoking (40.5%). A hierarchical multiple linear regression analysis was then performed with SRH-S as the dependent variable. Gender, age, hypertension, smoking, body mass index (BMI) and physical inactivity, which have been reliably associated with SRH (Johansson and Sundquist, 1999), were entered together in the first block of the analysis. In the following blocks, the variables of interest were entered: subjective perception of health complaints (block 2), awareness of bodily states (block 3) and illness representations (block 4). The order in which the blocks of variables were entered in the regression model was meant to identify the specific influence of illness representations on SRH after controlling for all the other factors possibly affecting the dependent variable.
Subsequently, a kappa statistic was calculated to assess overall agreement between patient-evaluated (SRH-S) and doctor-evaluated (SRH-D) health. In total, three groups of patients were then formed: health realists, that is, patients who had the same view of their health as their doctor’s (SRH-S score = SRH-D score); health optimists, that is, patients with a more positive view of their health compared to their doctor’s (SRH-S score > SRH-D score); and health pessimists, that is, patients with a more negative view of their health compared to their doctor’s (SRH-S score < SRH-D score). Univariate analyses of variance (ANOVAs) were used to explore the differences among the three groups of patients relative to health complaints, awareness of bodily states and illness representations.
Results
Simple regression analyses showed that among the psychological variables, there were significant unadjusted associations with SRH-S for health complaints (respectively, r2 = .089, p < .001 and r2 = .123, p < .001) and for all the dimensions of illness representations, including smoking as causal belief (Identity r2 = .036, p = .035; Timeline acute/chronic r2 = .071, p = .001; Consequences r2 = .116, p < .001; Personal control r2 = .063, p = .002; Treatment control r2 = .077, p = .001; Coherence r2 = .068, p = .001; Timeline cyclical r2 = .043, p = .012; Emotional representations r2 = .088, p < .001; Smoking as causal belief r2 = .039, p = .016). No significant results were instead observed for awareness of bodily states, nor for hereditary factors and stress/worry as causal beliefs (all r2 < .008, all p > .283). The results of the hierarchical multiple linear regression analysis are reported in Table 2. The medical variables (gender, age, hypertension, smoking, BMI and physical inactivity) accounted for 7.5 per cent of the variance of SRH-S and somatic and cognitive complaints for an additional 14.2 per cent. Consistent with the hypothesis, illness representations significantly contributed for another 16.2 per cent. Instead, awareness of bodily states was not associated with SRH-S (<0.1%). The tolerance values for all the independent variables were >0.10, and the variance inflation factor never exceeded 2.6, suggesting that multicollinearity between our variables was low (Belsley et al., 1980).
Results of the hierarchical multiple linear regression analysis with patients’ SRH-S as outcome variable.
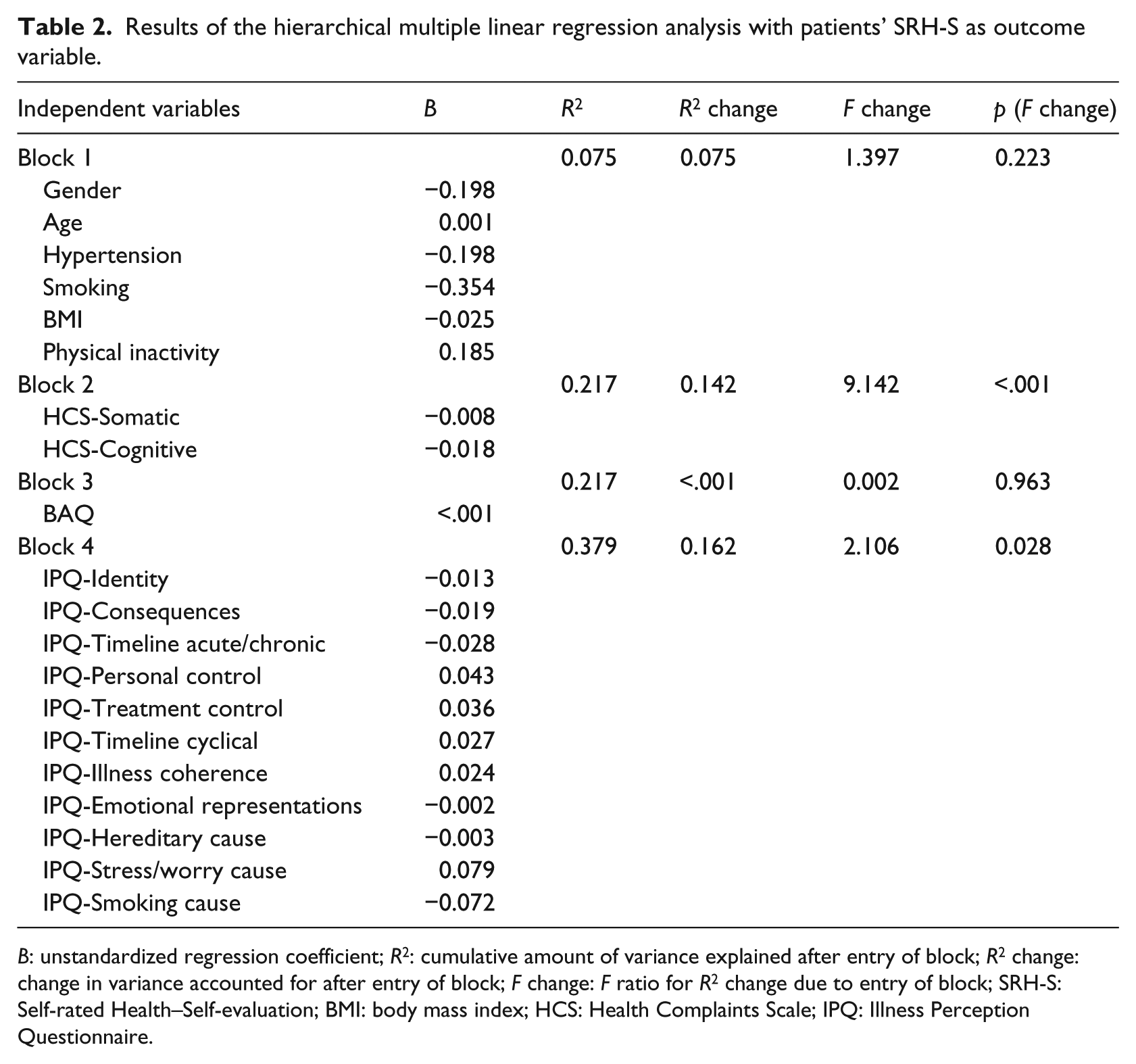
B: unstandardized regression coefficient; R2: cumulative amount of variance explained after entry of block; R2 change: change in variance accounted for after entry of block; F change: F ratio for R2 change due to entry of block; SRH-S: Self-rated Health–Self-evaluation; BMI: body mass index; HCS: Health Complaints Scale; IPQ: Illness Perception Questionnaire.
Agreement between patient-evaluated (SRH-S) and doctor-evaluated (SRH-D) health was found in 43.4 per cent of the participants (kappa = .13, p = .014). Results of the ANOVAs showed that health realist (N = 63), health optimist (N = 46) and health pessimist (N = 36) patients only differed in two dimensions of the IPQ-R, namely, the Consequences scale (F(2, 141) = 3.1, p = .047) and the Treatment control scale (F(2, 143) = 5.1, p = .008). There was also a marginally significant difference in the Personal control scale (F(2, 143) = 2.7, p = .074; all other F < 1.7, all p > .184). Least significant difference (LSD) post hoc comparisons revealed that health optimists tended to see less negative consequences from their illness and to perceive greater sense of controllability through personal coping behaviours compared to both health realists (p = .029 for Consequences, p = .038 for Personal control) and health pessimists (p = .036 for Consequences, p = .063 for Personal control); also, health pessimists tended to perceive lower sense of control over illness treatment compared to both health realists (p = .003) and health pessimists (p = .008). Means and standard deviations for all the comparisons are provided in Table 3.
Mean ± standard deviation of each psychological variable for the three groups of patients.
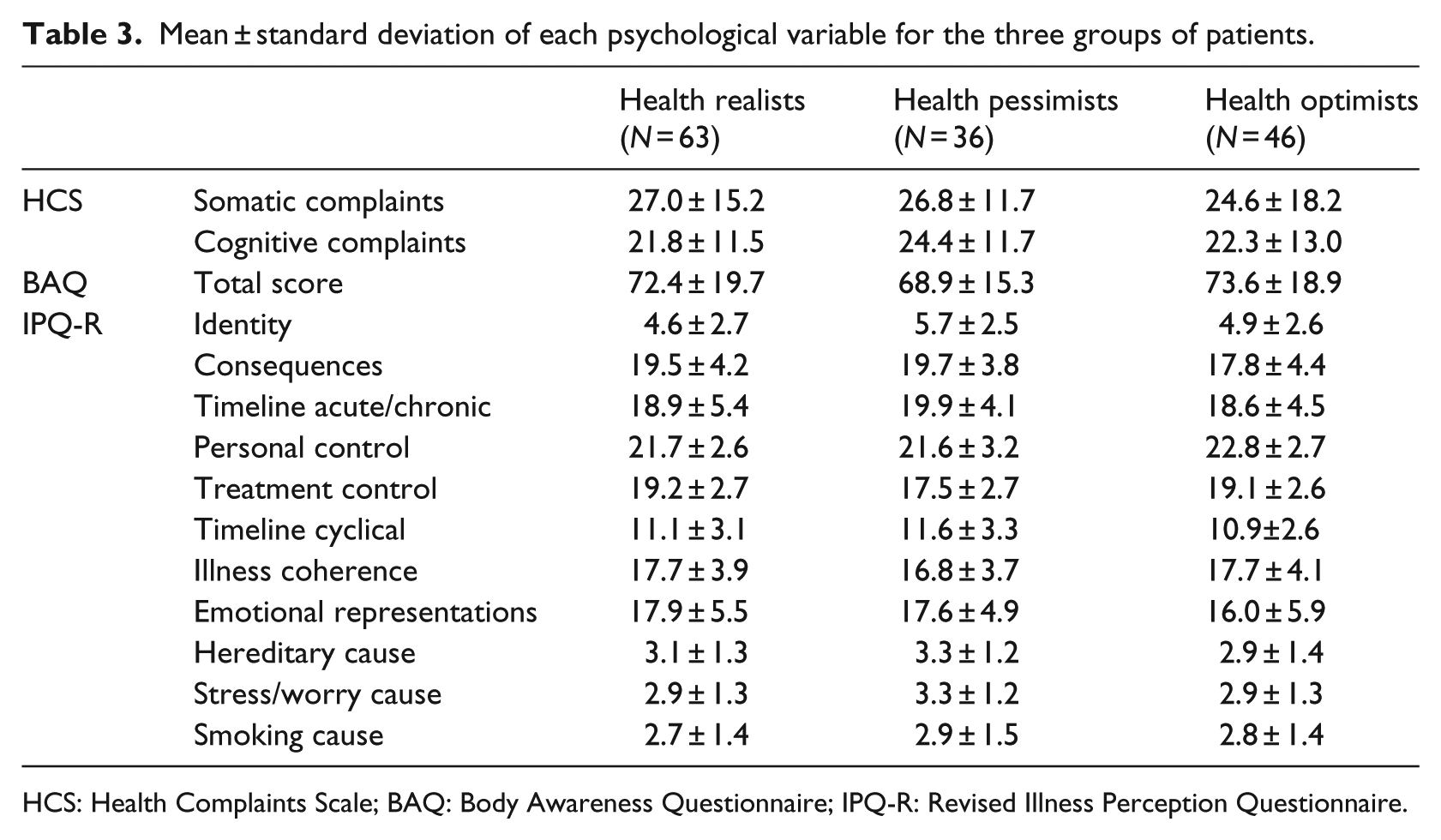
HCS: Health Complaints Scale; BAQ: Body Awareness Questionnaire; IPQ-R: Revised Illness Perception Questionnaire.
Discussion
Research has shown that important prognostic information is contained in an individual’s global subjective health evaluation and that SRH may, therefore, be a useful screening tool for risk assessment (Benyamini et al., 2014). This study adds to this literature by jointly assessing the contribution of health complaints, awareness of bodily states and illness representations to SRH judgments in patients with heart disease.
Our results confirm prior work suggesting that SRH conveys information about somatic and cognitive perceptions related to health complaints (Höfer et al., 2005; Mikolajczyk et al., 2008). More importantly, they show that illness representations are a further significant contributor to SRH, explaining 16.2 per cent of its variance. Similar findings on the association of illness representations with SRH have been described in only one other study, in which, however, there was no adjustment for any additional subjective component of SRH (Aalto et al., 2006). Perceived consequences of the illness in day-to-day life, presence of negative emotions related to it and beliefs in its controllability were the most relevant illness perceptions, consistent with findings from previous studies on patients with heart disease (Aalto et al., 2006; Juergens et al., 2010). Instead, we did not find evidence that awareness of one’s bodily states may be significantly associated with SRH. One possible reason for this null finding is that in this study we focused on patients’ ability to detect ‘normal’ sensations from inside the body, that is, sensations not typically associated with somatic complaints. It is, therefore, possible that a different instrument, which requires the respondent to focus on interoceptive information related to inflammatory processes and/or physiological dysregulations, may yield different results (Bjorner et al., 2005).
Even though the cross-sectional design prevents causal conclusions from being drawn, this study provides a valuable comprehensive assessment of the subjective components of SRH in patients with heart disease, from very concrete perceptions of bodily states and symptoms, to quite abstract cognitive and emotional representations of illness. Concurrently, gathering and interpreting data from different sources of information goes in the solicited direction of overcoming the weaknesses of single models towards an integrated approach to the concept and measure of illness and symptom perception (Petersen et al., 2011).
About health congruence, the low level of concordance between patients’ and doctors’ assessments of health observed in this study is consistent with prior literature (DeSalvo and Muntner, 2011). More interestingly, the results of the comparison between health optimist and health pessimist patients confirm the key role of illness perceptions in SRH judgements that emerged in the hierarchical multiple linear regression analysis. Health optimists perceived less negative consequences and greater controllability of the illness. These results are in line with findings that the beneficial effects of health optimism on health outcomes are at least partially attributable to higher perceived control (Hong et al., 2005; Ruthig and Chipperfield, 2007) and that health optimists tend to perceive their attitude and behaviour as determinants of their health ratings (Borawski et al., 1996). Also, we found that health pessimists perceived lower sense of control over illness treatment, which has been related to the risk of non-attendance to cardiac rehabilitation (French et al., 2006).
In light of the evidence that SRH is modifiable and that a positive modification leads to better cardiological outcomes (Benyamini et al., 2014), it has been recommended that people reporting poor SRH should be targeted with additional strategies to identify and address the reasons underlying their health perception (Van der Linde et al., 2013). The reported findings hint to the possibility that symptoms and illness representations may be one such reasons and that exploring them may enhance the focus on patient-centred care. Indeed, there have been reports that cardiac rehabilitation may improve health complaints (Denollet, 1994) and illness representations (Petrie et al., 2002), and the present results further indicate that jointly targeting these two factors may optimize the outcome of rehabilitation programmes. Since admission procedures to the Cardio-respiratory Rehabilitation Unit of the hospital in which the study was performed conform to national and international guidelines, the study sample may be considered representative of the general cardiac patient population, providing support to the external validity of the findings. However, longitudinal designs are needed in order to directly investigate the role of illness representations and health complaints in improving adjustment and coping to the disease.
Also, no differences between men and women were found in the study sample for any of the constructs (all t < 1.5, all p > .148), but exploration of gender inequalities is an important direction for future research. Gender differences have been found in illness perceptions in other chronic diseases (Edelstein et al., 2012), and in coronary heart disease, dissimilarities have been reported in the clinical manifestation of the illness (Hochman et al., 1999), as well as in adjustment and coping, with women reporting lower quality of life compared with men (Martin et al., 2005).
Finally, another fruitful area for future research is the investigation of representations of heart disease in the general population, in order to examine their relationship to health-related behaviours (e.g. not smoking, maintaining a healthy diet and exercising). Preliminary findings suggest that the general population lacks a clear perception of heart disease, with weak associations between illness representations and health behaviours (Cherrington and Lynd, 2007). In light of the notion that following a healthy lifestyle may prevent up to 80 per cent of cases of coronary artery disease (Waxman and Norum, 2004), these data are highly significant and point to the need to enact wide-scale strategies to promote public awareness.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.