
Abstract
The study goal was to determine whether partner’s level of unmitigated communion moderated the relation of partner communal coping to patient health. Couples in which one person was recently diagnosed with type 2 diabetes (n = 123) were interviewed separately and asked to discuss a diabetes-related problem. Communal coping behavior (from videotaped discussions) interacted with partner communal coping, such that partner communal coping was related to lower patient distress, higher patient self-efficacy, and higher patient medication adherence only when partners scored lower on unmitigated communion. The extent to which perceived emotional responsiveness and overprotective behavior mediated these relations was explored.
When one member of a couple is faced with a chronic illness, this stressor impacts the dyad broadly. Not only does the spouse affect how the patient responds to the illness, but the illness affects the spouse. One coping framework that recognizes the interpersonal nature of stressful life events is communal coping. Communal coping is defined as the appraisal of a stressor as shared (as opposed to individual) and activation of a collaborative approach to problem-solving (Lyons et al., 1998). Research on couples coping with chronic illness has shown that communal coping is adaptive for both patients and spouses.
Studies have examined the shared appraisal element of communal coping by examining the language partners use to appraise a stressor as shared. The use of first person plural pronouns, or “we-talk,” has been linked to better health outcomes for patients with chronic health problems. We-talk by both patients and spouses during the course of a couple’s intervention has been related to positive treatment outcomes in the context of smoking (Rohrbaugh et al., 2012) and alcohol use disorder (Hallgren and McCrady, 2015). When families of women with breast cancer were interviewed about how they coped with cancer, partner we-talk (but not patient or children we-talk) was related to reduced patient depression (Robbins et al., 2013).
A few studies have focused solely on the collaborative component of communal coping. In a 14-day daily study of men with prostate cancer and their spouses, daily collaboration (i.e. patient and spouse worked as a team) was related to more positive emotions in both husbands and wives (Berg et al., 2008). In a study that employed focus groups with people diagnosed with type 1 diabetes who were using continuous blood glucose monitoring, couples noted that the device worked best when couples collaborated on diabetes management (Ritholz et al., 2013). Conflict seemed to erupt when patients were completely responsible for managing diabetes.
One theory relevant to the construct of communal coping is Bodenmann’s theory of dyadic coping (Bodenmann, 1995, 1997). Their measure of dyadic coping reflects a number of positive and negative ways in which couple members relate to one another. A number of studies average across the positive dyadic coping strategies and average across the negative dyadic coping strategies and find links of the positive strategies to good health outcomes and the negative strategies to poor health outcomes (Bodenmann et al., 2006; Papp and Witt, 2010). However, this theory of dyadic coping includes many ways in which couples relate to one another, only one of which is relevant to communal coping. The common dyadic coping subscale reflects the collaboration aspect of communal coping but also includes some other couple behaviors (e.g. relaxation). A meta-analytic review of the literature on the dyadic coping scales (Falconier et al., 2015) found the strongest links to relationship satisfaction for the common dyadic coping scale (d = +.53)—the scale most similar to the collaboration component of communal coping. This dyadic coping theory, however, does not capture the shared appraisal element of communal coping.
Communal coping has been examined in studies of persons with diabetes using self-report measures that tap both shared appraisal (e.g., thinking about diabetes as “our problem” rather than “my/his or her problem”) and collaboration (e.g., working together to address diabetes problems). In one study, self-reported communal coping was related to greater support receipt from partners (Helgeson, 2017). In previous work with the present sample, self-report and behavioral measures of communal coping were linked to lower perceived stress and enhanced diabetes self-care (Zajdel et al., 2016) and greater progress in resolving diabetes problems following a discussion (Van Vleet and Helgeson, 2016). Some of this research seems to show that partner communal coping has stronger effects than one’s own communal coping on health outcomes (Helgeson et al., 2016; Robbins et al., 2013). Partner communal coping may be especially important for patient health, as partners are unlikely to become involved in disease management if they do not perceive the stressor as shared.
One question that research has failed to address is whether there are individual difference variables that moderate the relation of communal coping to patient outcomes. Does having a spouse with a shared illness appraisal and desire to collaborate always benefit patient health? One personality trait that may influence the relation of communal coping to relational and health outcomes is the partner’s level of unmitigated communion.
Unmitigated communion reflects a focus on others to the exclusion of the self. It has been linked to increased psychological distress, poor health behavior, and poor adjustment to chronic disease (Danoff-Burg et al., 2004; Helgeson and Fritz, 1999, 2000; Helgeson and Palladino, 2012; Trudeau et al., 2003). Unmitigated communion is associated with a set of interpersonal difficulties that reflect overinvolvement with others, such as being intrusive, overly nurturant, overprotective, and establishing relationships by putting others’ needs before one’s own (Fritz and Helgeson, 1998; Helgeson and Fritz, 1999). Unmitigated communion is also associated with a constellation of interpersonal problems that reflect self-neglect, such as difficulties asserting one’s needs and inhibiting self-expression to avoid conflict with others (Buss, 1990; Fritz and Helgeson, 1998; Helgeson and Fritz, 1999). In short, people with high levels of unmitigated communion have problematic relationships with network members (Helgeson and Fritz, 1998, 2000).
Thus, there are reasons to believe that involvement in disease management by a partner with high levels of unmitigated communion might not benefit patient’s health. When unmitigated communion individuals help others, their overtures may be perceived as intrusive or excessive. Thus, the first question this research addresses is whether partner unmitigated communion moderates the relation of communal coping to patient health, such that communal coping is beneficial only when partners are low on unmitigated communion.
A second objective of this research is to examine potential mechanisms that could explain why communal coping by high unmitigated communion partners is not beneficial. One possibility is that their communal coping efforts are not perceived as responsive to patient needs. Those characterized by unmitigated communion are very willing to help others, but their helping is motivated more by egoistic rather than altruistic concerns (Helgeson and Fritz, 1998). That is, their help is motivated by a need to enhance one’s own esteem in the eyes of others rather than to meet others’ needs. Perceiving that partners are responsive to needs appears to be critical to the health benefits of social support (Fekete et al., 2007). Indeed, perceived emotional responsiveness seems to be at the core in explaining the link of a number of relational processes to both healthy relationships and personal well-being (Reis and Gable, 2015; Slatcher et al., 2015). Thus, one reason that communal coping may not be associated with good patient outcomes when partners are high in unmitigated communion is that their collaborative efforts are not responsive to patient needs.
A second reason that communal coping might not be linked to good patient outcomes when provided by those high in unmitigated communion is that the support is overbearing or excessive in nature. That is, communal coping might be translated into overprotective behavior when coming from a high unmitigated communion spouse. In studies of persons with cancer, partner overprotective behavior has been linked to more negative feelings about the relationship (Hagedoorn et al., 2000), more patient distress, and less patient control (Kuijer et al., 2000).
In this study, we examine whether the effectiveness of partner communal coping is moderated by an individual difference variable that is central to support provision—unmitigated communion. When someone who scores high on unmitigated communion offers support to others, it is unclear whether they do so to meet the needs of others or to improve their own self-esteem (Bassett and Aube, 2013; Helgeson and Fritz, 1998). The goal of the study was to examine whether partner unmitigated communion moderated the relation of partner communal coping to patient outcomes. To the extent that this was the case, we examined two potential mechanisms for those associations—perceived partner responsiveness and partner overprotective behavior.
Method
Participants
Participants were 123 couples in which one person was recently diagnosed with type 2 diabetes. Demographics for the entire sample are shown in Supplemental Table 1. Just over half of patients were White (59%), and 41 percent were African American. Slightly over half of patients were male. In this diverse community sample, 23 percent of patients and 28 percent of partners completed a college degree, and 42 percent of couples reported a family income below US$40,000. The majority of couples were married; remaining couples cohabited. The vast majority of couples were heterosexual; one gay couple and two lesbian couples were included in the sample. Age was normally distributed in patients and partners; average ages were in the mid-50s; patient age ranged from 32 to 82, and partner age ranged from 31 to 82. Patient glycemic control was very good, as they had to be recently diagnosed to be eligible for the study.
Recruitment
Participants who were diagnosed with diabetes within the last 5 years were recruited from the community via mass transit advertisements, community health fairs, and placement of flyers and brochures in physician offices. Because one of the overall study goals was to compare Caucasian and African American couples, African Americans were oversampled. Interested persons contacted the study director, were screened for eligibility, and, if eligible, scheduled for the in-person interview. Of the 397 people who contacted us, 256 were deemed not to be eligible for participation, largely because they had been diagnosed more than 5 years ago. Of the remaining 141, 4 refused without us being able to determine eligibility, 12 refused after screening, and the remaining 125 agreed and completed the initial interview. However, two couples were removed from the analyses, one because the couple was intoxicated during the study and the other because the researchers learned upon verification of medical records that the patient had type 1 diabetes. Thus, the final sample size consisted of 123 couples. 1
Procedure
Institutional Review Board approval was obtained from both Carnegie Mellon University and the University of Pittsburgh. Prior to study commencement, both patients and partners signed informed consent forms. The majority of couples were interviewed in their homes (80%), but some chose to come to the university (20%). Patients and partners were interviewed separately. Interviews were structured and consisted of the administration of measures of relationship quality and psychological well-being. To prime couples to think about difficulties in coping with diabetes, patients and partners individually completed a 12-item questionnaire in which they rated the difficulty of several diabetes issues (e.g., exercising, resisting food temptations). Then, patients and partners were reunited and instructed to talk about how they could resolve diabetes difficulties with the goal of coming up with a solution to the problem. The vast majority of these discussions centered on diet and exercise. The 8-minute interactions were videotaped and later coded by independent raters for communal coping.
Instruments
Communal coping
Two trained research assistants coded communal coping in patients, and another two trained research assistants coded communal coping in partners. For patients, communal coping was defined as: “Extent to which the current situation seems to be a joint problem, from the patient’s point of view. Patient talks about the problem in a way that indicates diabetes is viewed as a joint problem. ‘We statements’ may be indicative of communal coping (e.g. ‘we watch what we eat; we exercise; we took that class’). A low score would indicate that the problem is currently perceived to be the patient’s problem only or a behavior in which the patient engages in by him/herself.” Partner communal coping was defined in the same way, except from the partner’s point of view. Thus, coders took into consideration the “we-language” that the person use to talk about the problem but also the content of those statements as to whether they reflected joint or collaborative problem-solving. Coders evaluated the entire exchange between couples to determine whether each person seemed to consider diabetes to be the patient’s problem or a joint problem. Communal coping behavior was coded for patients and partners separately on a single 5-point scale, ranging from 1 = no evidence to 5 = consistent and highest quality evidence. See Supplemental material for further detail on the coding scheme. Inter-rater reliability, measured by the intra-class correlation coefficient, was .79 for patients and .80 for partners. This behavioral measure of communal coping has been correlated with self-report measures (Zajdel et al., 2016).
Partner unmitigated communion
The 9-item unmitigated communion scale was administered to partners (Helgeson and Fritz, 1998). Partners were asked to indicate the extent to which they agreed or disagreed with each statement on a 5-point scale (e.g. I always put the needs of others above my own, I worry how other people get along without me when I am not there). The internal consistency was .78.
Patient relationship quality
We adapted the 5-item Quality of Marriage Index (QMI; Norton, 1983; α = .91) for cohabiting couples (i.e. “We have a good marriage” changed to “We have a good relationship”) and administered the 6-item emotional intimacy subscale from the Personal Assessment of Intimate Relationships (PAIR) scale (Schaefer and Olson, 1981; α = .84). Because the two scales were strongly related (r = .70, p < .001), we standardized them and took the average.
Patient distress
We administered three measures of psychological distress to patients. First, we administered the Center for Epidemiological Depression Scale (Radloff, 1977) to measure depressive symptoms (α = .92). Second, we used Diener’s Life Satisfaction Scale (Diener and Larsen, 1984; α = .86). Third, we administered the 4-item abbreviated Perceived Stress Scale (Cohen et al., 1983; α = .77). Because these three scales were highly correlated (r’s ranged from .65 to .70, all p’s < .001), we reverse scored the life satisfaction scale, standardized the three scales, and took the average to form a psychological distress index.
Patient diabetes outcomes
We used the Multidimensional Diabetes Questionnaire (Talbot et al., 1997) to measure self-efficacy (α = .88). Patients rated how confident they were on a scale ranging from 0 to 100 percent that they could execute seven self-care behaviors (e.g. follow diet, exercise regularly). The measure demonstrates adequate internal consistency, construct validity, and is correlated with self-reports of exercise and diet and lower levels of depression among persons with type 2 diabetes. We measured self-care behavior with the Summary of Diabetes Self-Care Activities (Toobert and Glasgow, 1994), which measures dietary intake, exercise/energy expenditure, and medication adherence. The reliability was good (α = .80). Finally, both patients and partners completed the 4-item Medication Adherence Index with respect to patient compliance (Morisky et al., 1986; α = .70 patient; α = .83 partner). This instrument has good reliability and concurrent and predictive validity over 2 and 5 years. Because the index was correlated between patients and partners (r = .44, p < .001), we averaged the two for our index of medication adherence.
Patient perceived partner emotional responsiveness
Patients were asked to consider how responsive partners were to their needs. Specifically, patients were asked to think about how their partner typically responds when they are upset about their diabetes and then to rate how this response made them feel. There were four positive items (really understood, respected, supported, better), and four negative items were reverse coded (ignored, worse, rejected, judged or evaluated). Each was rated on a 4-point scale, ranging from 1 = not at all to 4 = a lot. The internal consistency was good, α = .77.
Partner overprotective behavior
Partner overprotectiveness was measured with four items taken from Coyne and Smith (1991) and modified by Hagedoorn et al. (2000). Patients were asked how often in the past month spouses: thought you can’t take care of yourself, tried to do everything for you, thought that he or she needed to be around for you to take proper care of your diabetes, and continuously kept an eye on you. Responses were made on a 4-point scale, ranging from 0 = none of the time to 3 = most of the time. Partners used the same scale to report on their own behavior. Internal consistencies were good for patients (α = .73) but somewhat lower for partners (α = .64). Because the two scales were correlated (r = .45, p < .001), we averaged the two to form an index of partner overprotective behavior.
Results
First, we examined if any variables needed to be statistically controlled in the analyses. Neither partner communal coping nor partner unmitigated communion were related to patient age, race, education, couple marital status, glycemic control, or length of illness. Thus, none of these demographic variables were statistically controlled in these analyses.
There was a sex difference in partner unmitigated communion, F (1, 121) = 9.72, p < .01, eta2 = .07. Consistent with previous research, female partners scored higher on unmitigated communion (M = 3.60; SD = 0.68) than male partners (M = 3.20, SD = 0.74). There was also a marginally significant sex difference in partner communal coping, F (1, 120) = 4.77, p = .05; eta2 = .03. Female partners were rated as higher in communal coping (M = 2.68; SD = 1.17) than male partners (M = 2.28; SD = 1.04). Thus, we statistically controlled for partner sex in all analyses. On an exploratory basis, we also examined whether the predicted interaction between partner unmitigated communion and communal coping interacted with partner sex. This interaction appeared for one dependent variable, which we describe below.
Means and standard deviations, as well as the intercorrelations, of study variables are shown in Supplemental Table 2. Of note, partner unmitigated communion was not related to communal coping reports of partners but was modestly related to greater reports of communal coping by patients. The regression analyses reported below and shown in Table 1 were conducted by entering partner sex, patient communal coping, partner communal coping, partner unmitigated communion, and the interaction between partner unmitigated communion and partner communal coping. Main effects were centered before computing interaction terms, and only centered variables were used in the analysis. Because we coded both patient and partner communal coping separately, we entered both variables in the analyses. However, the variable of interest is the interaction between partner unmitigated communion and partner communal coping. Significant interactions are displayed in figures (Supplemental material) by showing the relation of communal coping (+ or –1 standard deviation) to outcomes for people who scored at the 25th, 50th, and 75th percentile on unmitigated communion.
Unmitigated communion and communal coping as predictors of outcomes and mediators.
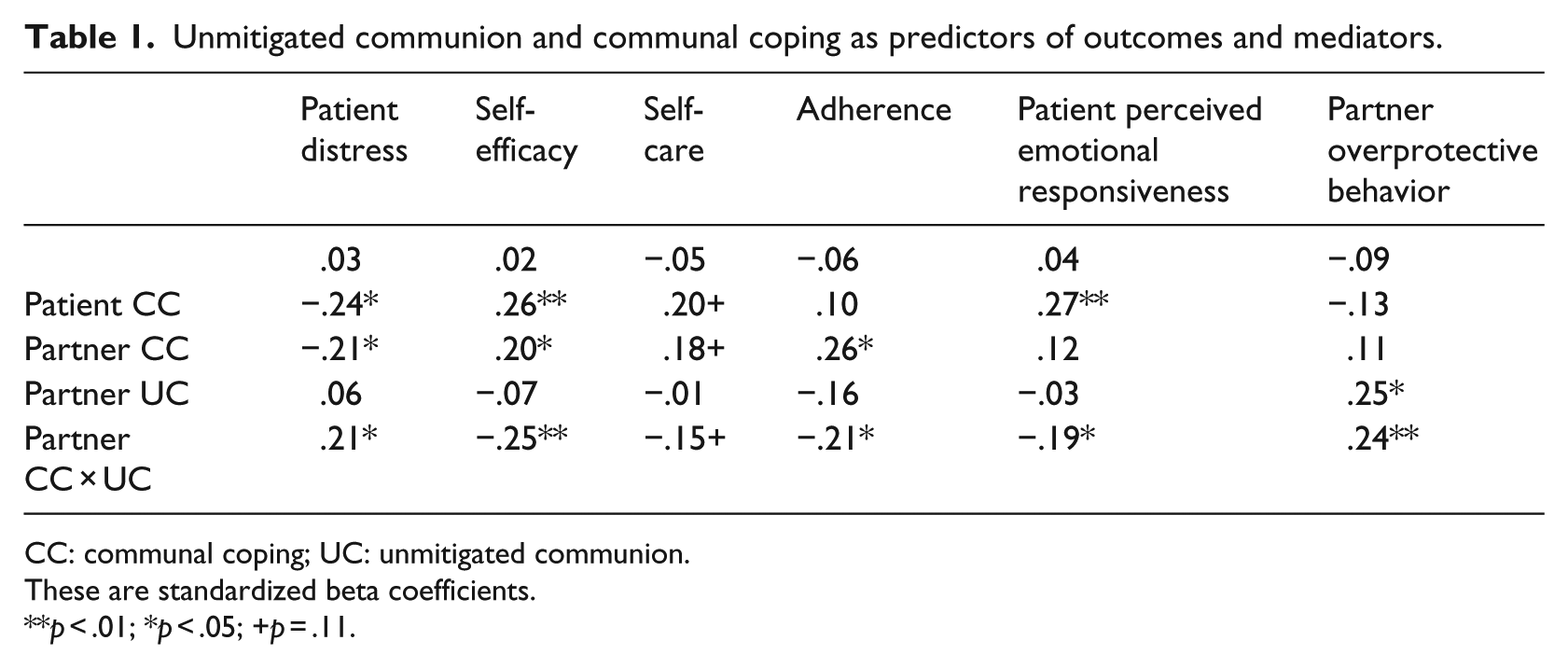
CC: communal coping; UC: unmitigated communion.
These are standardized beta coefficients.
p < .01; *p < .05; +p = .11.
Relationship quality
Although patient and partner communal coping were modestly related to relationship quality (see Supplemental Table 2 correlations), the interaction between partner communal coping and partner unmitigated communion did not predict relationship quality.
Distress
As shown in Table 1, the partner communal coping by partner unmitigated communion interaction was significant in predicting patient distress. Partner communal coping was related to reduced patient distress, especially when partners scored low on unmitigated communion (see Supplemental Figure 1a). Our exploratory post hoc analysis also revealed a partner sex by partner unmitigated communion by partner communal coping interaction (beta = .78, p < .05). The interaction revealed that the two-way interaction was limited to female partners; for male partners, communal coping was related to reduced distress in all cases.
Diabetes outcomes
The partner communal coping by partner unmitigated communion interaction was significant for self-efficacy but only marginally significant for self-care behavior. Partner communal coping was related to higher self-efficacy for those who scored low but not high on unmitigated communion (see Supplemental Figure 1b). The pattern of the interaction for self-care behavior corresponded to that shown for self-efficacy.
The partner unmitigated communion by communal coping interaction was significant for medication adherence. Similar to the interaction for self-efficacy, partner communal coping was related to higher levels of medication adherence only when partners scored lower on unmitigated communion.
Potential mechanisms
As shown in Table 1, the partner unmitigated communion by communal coping interactions were significant for both patient perceived emotional responsiveness and partner overprotective behavior. Partner communal coping is only related to patient perceived emotional responsiveness when partners score low on unmitigated communion (see Supplemental Figure 2a). Partner communal coping was only related to higher partner overprotective behavior when partners scored higher on unmitigated communion (see Supplemental Figure 2b).
Mediation
We tested whether patient perceived emotional responsiveness and partner overprotective behavior mediated the interaction between communal coping and unmitigated communion on the three outcomes (distress, self-efficacy, medication adherence) reported in Table 1 with mediated moderation in Mplus. Bias-corrected bootstrapping was used to examine the indirect effects of the two mediators. Perceived emotional responsiveness was a marginally significant mediator of the partner unmitigated communion by communal coping interaction on patient distress (indirect effect = .08, p = .09) but did not mediate the interaction effect on the other two outcomes. Partner overprotective behavior was a marginally significant mediator of the partner unmitigated communion by communal coping interactions on patient distress (indirect effect = .05, p = .05) and medication adherence (indirect effect = .05, p = .08). Thus, there was only modest support for mediation.
Discussion
Previous research has linked communal coping in couples to good patient health outcomes in the context of chronic disease. However, researchers have failed to examine whether there are boundary conditions to this theory. Is communal coping good in all circumstances and for everyone? We suggested in this article that support providers characterized by the specific personality trait of unmitigated communion might not be best equipped to engage in communal coping and that their efforts might be less successful. Findings suggested that this indeed was the case.
Partner communal coping was linked to reduced patient distress and enhanced medication adherence, but these relations were clearly stronger when partners scored low on unmitigated communion. In the case of partner distress and patient diabetes self-efficacy, the relations of communal coping to good outcomes were limited to the case in which partners scored low on unmitigated communion.
Why is partner involvement and collaboration in patient disease management not related to good outcomes when partners are characterized by unmitigated communion? We investigated two possibilities. First, partners who are high in unmitigated communion may not be responsive to patient needs when they become involved in disease management. Unmitigated communion has been linked to having difficulties in interpersonal relations and to being more strongly connected to the mission of providing support rather than meeting the needs of others (Helgeson and Fritz, 1998). Thus, unmitigated communion individuals may be working with patients in a way that is not wanted by patients or not regarded as helpful by patients. Indeed, partner communal coping was related to patients perceiving that partners were responsive to their needs but only when partners scored low on unmitigated communion. When partners scored high on unmitigated communion, communal coping was unrelated to patient perceptions of being responsive to needs. That being the case, however, perceived emotional responsiveness did not seem to explain the unmitigated communion by communal coping interactions on health outcomes.
There was modest support for the idea that overprotective behavior would explain why communal coping was not linked to good health outcomes for patients when partners scored high on unmitigated communion. Partner involvement in patient disease management seemed to be viewed as overextending itself and construed as overprotective behavior when displayed by a high unmitigated communion partner. By contrast, partner communal coping was not viewed as overprotective when displayed by low unmitigated communion partners. Thus, communal coping (i.e. involvement in disease management) may be viewed differently when it comes from someone who has a general tendency to be intrusive and become overinvolved in others’ lives versus someone who is not.
Before concluding, there are several study strengths and limitations that deserve mention. A major study strength is the recruitment of a diverse community sample, in which 41 percent of participants were African American and only 23 percent were college graduates, which increases the generalizability of our findings. Other strengths of the study include the targeting of a group of people who are recently diagnosed with type 2 diabetes, the use of an observational measure of communal coping, and the inclusion of both patient and partner reports of a couple of outcomes. Limitations include the cross-sectional nature of the data which undermines our ability to draw causal inferences.
This is the first study to identify a boundary condition of communal coping that focuses on a personality trait in the partner. Communal coping, in general, has been linked to good patient health outcomes—especially communal coping on the part of partners. However, it may not be the case that all persons’ communal coping efforts will be perceived as helpful. Partner communal coping may not be helpful for patients when their involvement becomes overprotective and/or is unresponsive to needs. Intervention efforts aimed at couples in which one person has a chronic illness should consider equipping partners with skills to become involved in disease management in a way that is helpful to both couple members.
Footnotes
Acknowledgements
The authors extend their thanks to Gianna Davis and Tiona Jones for interviewing the vast majority of these patients, to Pamela Snyder for overseeing the project and the analyses, and to the participants in this study who gave their time to support our efforts.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institutes of Health grant R01 DK095780 and received recruiting assistance from the University of Pittsburgh Clinical & Translational Science Institute which is supported by the National Institutes of Health Grant UL1TR000005.
Supplemental material
Supplemental material is available for this article online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.