
Abstract
This study found that children with a history of cancer had higher scores on certain measures of spirituality compared to their healthy peers. Health history was found to significantly moderate the relations among spirituality and outcome variables, such as depression and anxiety. Furthermore, parent–child dyadscancer had more highly correlated scores than parent–child dyadshealthy on both the Depression subscale and the Existential Well-Being subscale, whereas parent–child dyadshealthy had more highly correlated scores than parent–child dyadscancer on the Duality factor. Limitations and future directions are discussed.
Introduction
Children and their parents often seek religious or spiritual support from pediatric health care providers as they attempt to find meaning in life-threatening illness (e.g. Barnes et al., 2000; Kamper et al., 2010; Lima et al., 2013; VandeCreek et al., 2007). Spirituality can provide children with positive coping strategies to find meaning and purpose in the midst of trauma or illness (Lima et al., 2013; Walker et al., 2010). Spirituality can also play a role for children beyond the initial stage of cancer diagnosis into the stages of cancer survivorship (Morse and O’Rourke, 2009).
As more children are surviving cancer due to innovations in medical technology and treatment protocols (Canadian Cancer Society’s Advisory Committee on Cancer Survivor Statistics, 2014), researchers are investigating factors, such as spirituality, that may promote children’s well-being beyond a cancer diagnosis into survivorship (e.g. Hendricks-Ferguson, 2008; Morse and O’Rourke, 2009). A greater awareness of spirituality and its relation to psychological health can strengthen the health care professional’s therapeutic interventions with childhood cancer survivors (Moore et al., 2015; Smith and McSherry, 2004).
Some researchers have placed an emphasis on the positive outcomes that follow a childhood cancer diagnosis (e.g. Parry, 2003). For instance, Zebrack et al. (2012) used the Posttraumatic Growth Inventory (PTGI) to measure perceived positive impact (e.g. spiritual change, a new appreciation for life) in 6425 young adults who survived cancer as children. They found that these survivors were more likely to report perceptions of positive growth when compared to their healthy siblings. Similarly, Parry and Chesler (2005) found that a childhood cancer experience led to positive psychosocial outcomes in 50 young adults. In their qualitative study, they used the term psycho-spiritual growth to capture the deeply rooted changes reported in the participants’ interviews; such changes were often existential or spiritual in nature. Zebrack et al. (2012) and Parry and Chesler (2005) both observed spiritual growth at long-term follow-up with childhood cancer survivors. Others, however, place more importance on spirituality as a resilience resource (e.g., Reutter and Bigatti, 2014). Miller (2013) found that spirituality, defined as the valued and dynamic relationship with a higher power, is one of the most robust protective factors against depression in adolescence. Therefore, a better understanding of the role of spirituality in the lives of childhood cancer survivors and its relation to psychological health and coping could highlight potential sources of positive growth and protective factors for children facing the challenge of a cancer diagnosis.
However, despite its potential importance to pediatric care, few have examined spirituality and its role in the childhood cancer experience. Most research has focused on spirituality in adolescence and adulthood. Although some researchers have explored the role of spirituality in the lives of childhood cancer survivors qualitatively, quantitative studies are less common and have tended to use measures that are oriented toward adults or focused solely on religious practice (e.g. Houskamp et al., 2004), which do not adequately account for the complexity of children’s spiritual thoughts and ideas. Child-oriented measures that extend beyond religious practices would yield a richer study of children’s spirituality and have implications for supporting health care professionals in their interventions.
Given that the objective of this research is to examine spirituality in children living in a diverse Canadian context, ubiquitous spiritual characteristics (e.g. relationship with a higher power, purpose and meaning in life, spirit–body dualism; Barrett, 2011) that transcend cultures and creeds are of particular relevance. The intention is not to be reductive in relation to spirituality, but to explore broader spiritual experiences that appear across religious groups. In particular, the relationship with the sacred is of specific importance, as it is often deemed the most robust protective factor against negative psychological symptoms, such as depression (e.g. Miller, 2013). Fisher (2012) also found that a relationship with a higher power plays an integral role in spiritual well-being. Based on his review of 22 studies, he found that a relationship with the sacred accounted for the most variance in spiritual well-being. Thus, because one of the main objectives of this study is to examine spirituality in relation to psychological health outcomes and coping strategies, exploring the relationship with the transcendent is especially germane.
Despite playing an integral role in their spiritual development, parents’ perspectives of their children’s spiritual lives are not well-understood. Parent–child conversations can shape children’s moral (e.g. Recchia and Wainryb, 2014) and spiritual (e.g. Boyatzis and Janicki, 2003; Renaud et al., 2014) understanding. When children are ill, parents often place more importance on relationships (e.g. family relationships, spiritual relationships) that promote recovery, rather than an emphasis on achievements (e.g. achieving high grades at school) that require optimal health. Thus, parent–child conversation during this time may shift from discussions about a child’s accomplishments to discussions about spiritual concepts (e.g. Thayer, 2009). Parents may also engage in more conversations about their child’s thoughts and feelings, given that a serious medical diagnosis can prompt complex emotions and discussion about illness (e.g. Eiser and Morse, 2001). Thus, parents of childhood cancer survivors may have had more discussions with their children about their psychological health and may have a more accurate perception of their children’s spirituality when compared to parents and children who may not have had such an experience.
The current study
The purpose of this study was to (a) describe spirituality in childhood cancer survivors compared to a healthy comparison group, (b) explore the correlations between spirituality and psychological health (i.e. depression, anxiety) and coping (i.e. positive, negative) when moderated by health history (i.e., healthy, cancer survivor), and (c) determine whether parent–childcancer dyads have more highly correlated scores on measures of spirituality and psychological health than parent–childhealthy dyads.
It was hypothesized that childhood cancer survivors would show higher levels of spirituality than children in a healthy comparison group. Furthermore, it was expected that spirituality, when moderated by health history, would be a predictor of lower depression scores, anxiety scores, and negative coping scores, and a predictor of positive coping strategies in the childhood cancer survivor group. It was also predicted that parent–childcancer dyads would have more highly correlated scores on spirituality measures and psychological health measures than parent–child dyadshealthy.
Methods
Participants
A total of 69 school-age participants (7–11 years) were recruited. In all, 43 healthy comparison children (Mage in months = 112.42, SD = 17.69, 56% females) and 26 childhood cancer survivors (Mage in months = 121.58, SD = 24.17, 50% females) participated. The age at the time of diagnosis ranged from 9 to 128 months (Mage at diagnosis = 59.77, SD = 34.26). The length of active treatment (e.g. chemotherapy, radiation, surgery) ranged from 3 to 48 months (Mlength of treatment = 25.04, SD = 17.33).
Inclusion criteria for the healthy parent–child dyads included no history of life-threatening illness or trauma for the child. Inclusion criteria for the childhood cancer survivor–parent dyads included children who had already undergone primary cancer treatment (e.g. primary induction) and were at least 6 months post-diagnosis. The majority of participants were leukemia cancer survivors (57.7%), whereas the remaining children survived other types of cancers (i.e. Ewing’s sarcoma, Wilms’ tumor, optic nerve glioma, lymphoma, neuroblastoma, bilateral retinoblastoma, and rhabdomyosarcoma). Four parents from the cancer survivor group who originally expressed interest in participating later declined for various reasons (e.g. death in the family, family too busy with medical follow-ups), and four other participants were excluded because the child did not meet the inclusion criteria (e.g. too young to participate).
With respect to the healthy parent–child dyads (90.7% mothers), parents reported how religious (not at all, 37.2%; somewhat, 48.8%; very, 14.0%) and how spiritual (not at all, 20.9%; somewhat, 55.8%; very, 23.3%) they perceived their families, as well as how often they frequented their place of worship (once a week, 16.3%; once a month, 14.0%; three to four times per year, 34.9%; once a year, 18.6%; not at all, 16.3%). Parents also affiliated their families with various religious traditions, including Christianity (79.1%), Judaism (11.6%), Islam (4.7%), Hinduism (9.3%), and None (23.2%); several parents reported more than one religious affiliation.
With respect to the childhood cancer survivor parent–child dyads (92.3% mothers), parents reported how religious (not at all, 23.1%; somewhat, 65.4%; very, 11.5%) and how spiritual (not at all, 3.8%; somewhat, 73.1%; very, 23.1%) they perceived their families as well as how often they frequented their place of worship (once a week, 15.4%; once a month, 15.4%; three to four times per year, 19.2%; once a year, 26.9%; not at all, 23.1%). Parents also affiliated their families with various religious traditions, including Christianity (61.5%), Judaism (11.5%), Islam (11.5%), Hinduism (3.8%), and None (11.5%); several parents reported more than one religious affiliation.
The GPower calculator version 3.1 was used to compute the sample size, given the effect size, alpha, and the desired power. A priori power analysis showed that a sample size of approximately 24 in each group was sufficient when using multiple analyses of variance to detect a clinically significant difference at 0.05, with an effect size of 0.25, and power of 0.80. These calculations were grounded in Cohen’s (1992) statistical guidelines and were based on the assumption that the measurements on the scale are normally distributed. To conduct a multiple linear regression, with an effect size of 0.15, a significant difference of 0.05, and power of 0.80, an overall total of 55 participants were needed. According to Harrell (2001), “in many situations a fitted regression model is likely to be reliable when the number of predictors (or candidate predictors if using variable selection) p is less than m/10 or m/20, where m is the limiting sample size” (p. 61). Thus, the current sample size (n = 69) is appropriate for the proposed analyses.
Materials and procedure
Ethics approval was obtained from a hospital in a large urban Canadian city. An oncology staff member approached parents with information about the study. Interested parents provided their contact information to be contacted by a researcher. Participating parents signed a parental consent form and were given a general information letter about the research upon study completion. Child assent was also obtained before completing the study.
Parent and child measures
All parents and children completed separately the Behavior Assessment System for Children-Second Edition (BASC-2), the Spiritual Well-Being Scale (SWBS), and the Children’s Spiritual Lives questionnaire. Additionally, parents completed a Demographic Questionnaire and a Medical History Questionnaire and children completed Kidcope-Younger Version questionnaire. Parents were instructed to answer all spirituality questions as if they were their school-age son or daughter. Questionnaires were read aloud to children. The study took approximately 1 hour.
Kidcope-Younger Version
The Kidcope-Younger Version is a 15-item measure that assesses children’s coping strategies. In this study, children were asked to identify a situation (i.e., not related to illness) that they found stressful (e.g. “I did poorly on a spelling test,” “I had a fight with my sister”) and identify particular coping strategies they used. Test–retest correlations ranging from 0.56 to 0.75 were obtained when children were asked to report their coping on the same reported situation 3 days apart (Spirito et al., 1988). It has two factors (Cheng and Chan, 2003): the Negative Coping factor consists of seven coping strategies (i.e. distraction, social withdrawal, self-criticism, blaming others, wishful thinking, resignation, negative emotional regulation) and the Positive Coping factor consists of four coping strategies (i.e. cognitive restructuring, problem-solving, social support, positive emotional regulation).
BASC-2
This measure has been used to assess behavioral, social, and emotional problems in children (Reynolds and Kamphaus, 2004); there is a parent and child version. The Depression and Anxiety subscales were chosen as the outcome measures due to the focus on the relation between spirituality and psychological health. Test–retest reliabilities had correlations in the 0.80 range for composite scores and between the 0.70 and 0.80 range for individual scales across all age groups (Reynolds and Kamphaus, 2004).
SWBS
This scale measures overall spiritual well-being, which is comprised of a Religious Well-Being subscale (e.g. relationship with God) and an Existential Well-Being subscale (e.g. a sense of purpose and meaning in life). The 20-item measure uses a 6-point Likert scale (e.g. 1 = strongly agree, 6 = strongly disagree). For the overall scale, scores range from 20 to 120 points; higher scores are indicative of greater levels of well-being. Internal consistency coefficients range from 0.82 to 0.94 for the Religious Well-Being subscale, 0.78 to 0.86 for the Existential Well-Being subscale, and 0.89 to 0.94 for the overall scale. Reliability between 1 and 10 weeks of testing ranges from 0.82 to 0.99 (Bufford et al., 1991).
Children’s Spiritual Lives
This measure was developed by Moore et al. (2016) for children between 6 and 12 years of age and was largely based on a qualitative study by Moore et al. (2012). The measure consists of three main factors (e.g. Comfort (factor 1), Omnipresence (factor 2), Duality (factor 3)) and was designed for children from a variety of religious and cultural backgrounds in North America (see Moore et al., 2016).
Results
Summary of analyses
Multivariate analyses of variance (MANOVAs) were computed to examine whether childhood cancer survivors will show higher levels of spirituality than their healthy peers. To examine whether spirituality will predict lower (a) depression, (b) anxiety, (c) negative coping, and higher (d) positive coping in the childhood cancer survivor group, moderation analyses were conducted. Pearson correlations were computed in order to examine the relation between parent and child reports on spirituality, depression, and anxiety. More specifically, examining whether or not parents of childhood cancer survivors had more highly correlated scores with their children’s spirituality, depression, and anxiety scores than parents of healthy children were explored using Fisher’s z transformations.
Assumptions, correlations, and differences on measures
All presented analyses were computed using SPSS, version 20.0. Assumptions of normality and parametric statistics (i.e. linearity, outliers) were examined, and no violations were detected. Table 1 shows the correlations between cognitive measures, and Table 2 shows any differences on measures of health history (i.e. cancer, healthy).
Correlations between variables.
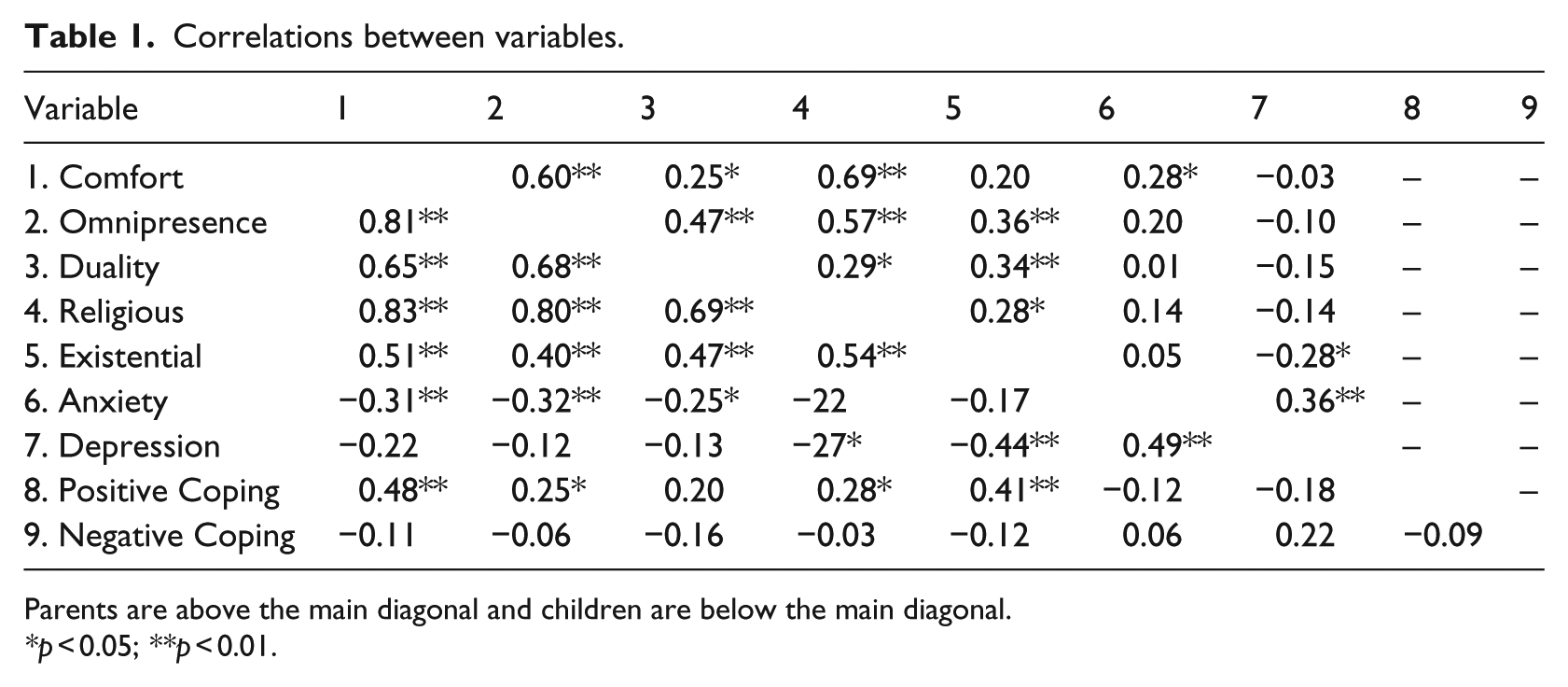
Parents are above the main diagonal and children are below the main diagonal.
*p < 0.05; **p < 0.01.
Differences in variables between healthy and cancer groups for parents and children.
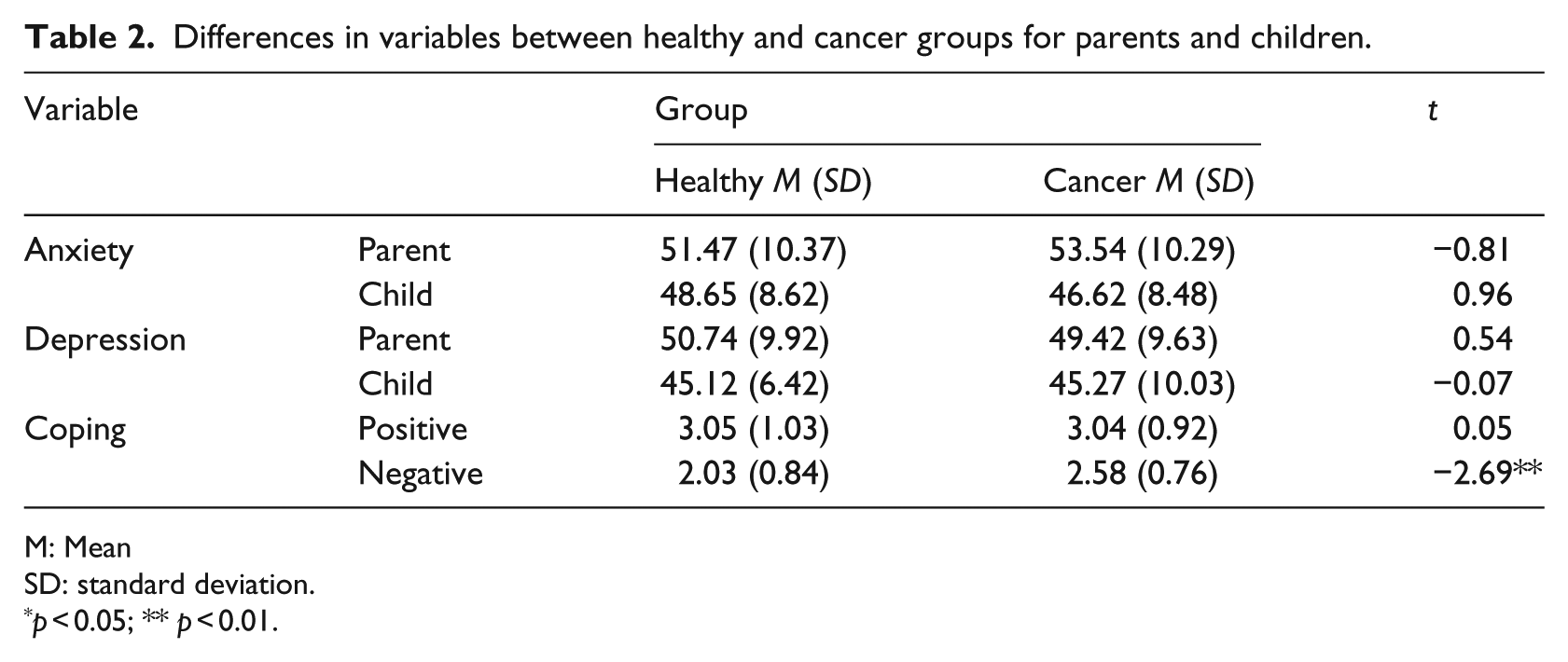
M: Mean
SD: standard deviation.
p < 0.05; ** p < 0.01.
Children’s spirituality
Children’s reported spirituality (i.e. Children’s Spiritual Lives, SWBS) was examined in relation to health history (i.e. healthy, cancer) and gender (i.e. male, female). In both analyses, age and parents’ reports of the family’s religiosity and spirituality were all entered as covariates.
With regard to the Children’s Spiritual Lives (i.e. factor 1 (Comfort), factor 2 (Omnipresence), and factor 3 (Duality)) as the outcome measure, there was a significant difference with respect to gender, Wilks’ λ = 0.871, F(3, 60) = 2.96, p = 0.040. However, this was likely a spurious finding as there were no between-subjects effects; thus, there was a probable weak multivariate effect, which was not detected in the univariate analyses (Tabachnick and Fidell, 2013). There was a significant difference between health history, Wilks’ λ = 0.803, F(3, 60) = 4.91, p = 0.004. Between-subjects analyses showed that the Comfort factor, F(1, 62) = 4.81, p = 0.032, and the Omnipresence factor, F(1, 62) = 13.40, p = 0.001, accounted for this significant difference between groups; the Duality factor was not significant. Parents’ reports of their family’s religiosity was found to be a significant covariate, Wilks’ λ = 0.852, F(3, 60) = 3.48, p = 0.021 (Table 3). Age and parents’ reports of their family’s spirituality were not significant covariates.
Between-subjects effects of children’s health history and gender on spirituality in relation to Comfort, Omnipresence, and Duality factors and Existential and Religious subscales.
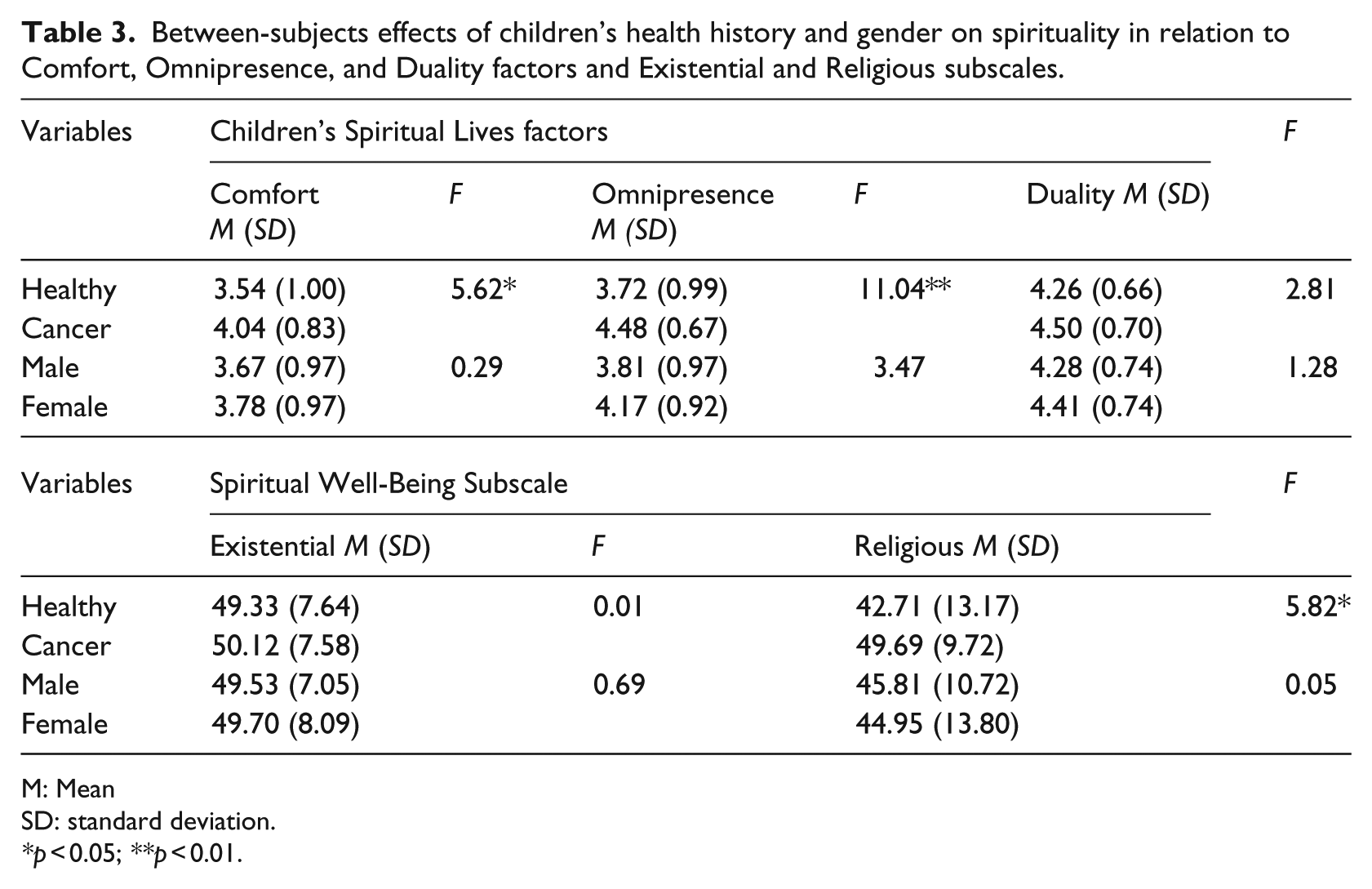
M: Mean
SD: standard deviation.
*p < 0.05; **p < 0.01.
With the SWBS (i.e. Existential Well-Being subscale, Religious Well-Being subscale) as the outcome measure, no significant gender differences were found. There were significant differences between health history, Wilks’ λ = 0.881, F(2, 61) = 4.12, p = 0.021. Between-subjects analyses revealed that the Religious Well-Being subscale, F(1, 62) = 5.82, p = 0.019, accounted for this significant difference between groups, whereas the Existential Well-Being subscale was not significant (see Table 3). Age was a significant covariate, Wilks’ λ = 0.871, F(2, 61) = 4.53, p = 0.015. Parents’ reports of their family’s religiosity and spirituality were not significant covariates.
Spirituality and psychological health
Moderation analyses were conducted to examine whether spirituality, when moderated by health history, would predict lower scores on the (a) Depression subscale, (b) Anxiety subscale, (c) Negative Coping factor, and higher scores on (d) Positive Coping factor in the childhood cancer survivor group. Age and parents’ reports of the family’s religiosity and spirituality were entered as covariates.
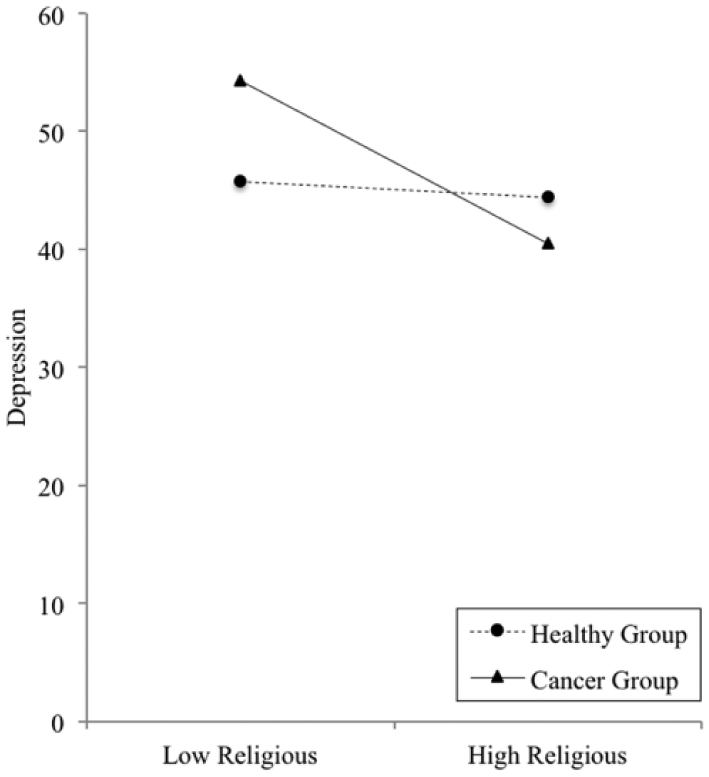
With the Children’s Spirituality Lives as the predictor of the Depression subscale, the Comfort factor was significant, F(6, 62) = 2.43, p = 0.036. Higher scores on the Comfort factor predicted lower Depression subscale scores (M = 45.17, SD = 7.91, β = 1.32, p < 0.05). This significant relationship was moderated by health history; that is, only childhood cancer survivors showed this significant relationship (see Figure 1).
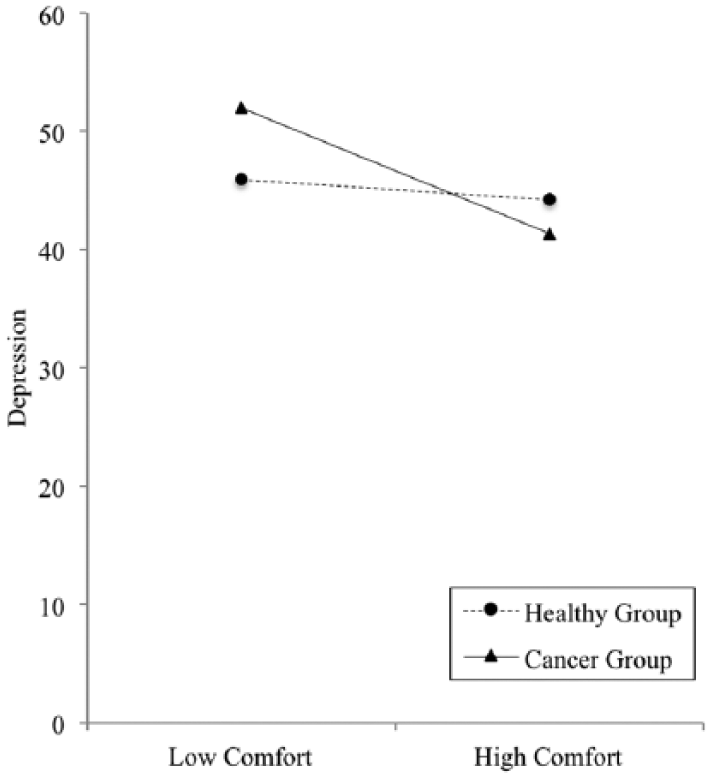
Plot of the moderating effect of health history on the relationship between the Comfort factor (Children’s Spiritual Lives) and the Depression subscale.
With the SWBS as the predictor (i.e. Religious Well-Being and Existential Well-Being subscale), the Religious Well-Being subscale was significant, F(6, 62) = 3.23, p = 0.008. Higher scores on the Religious Well-Being subscale predicted lower Depression subscale scores (M = 45.17, SD = 7.91, β = −1.51, p < 0.01), but was only significant for childhood cancer survivors (see Figure 2).
Plot of the moderating effect of health history on the relationship between Religious Well-Being subscale (Spiritual Well-Being Scale) and the Depression subscale.
With the Children’s Spiritual Lives measure as the predictor of the Anxiety subscale, there were no significant results. With respect to the SWBS, the Religious Well-Being subscale was a significant predictor of the Anxiety subscale, F(6, 62) = 3.66, p = 0.004. Higher scores on the Religious Well-Being subscale predicted lower Anxiety subscale scores (M = 47.88, SD = 8.56, β = −1.39, p < 0.01), but was only significant for childhood cancer survivors (see Figure 3). The Existential Well-Being subscale as a predictor of the Anxiety subscale was not significant.
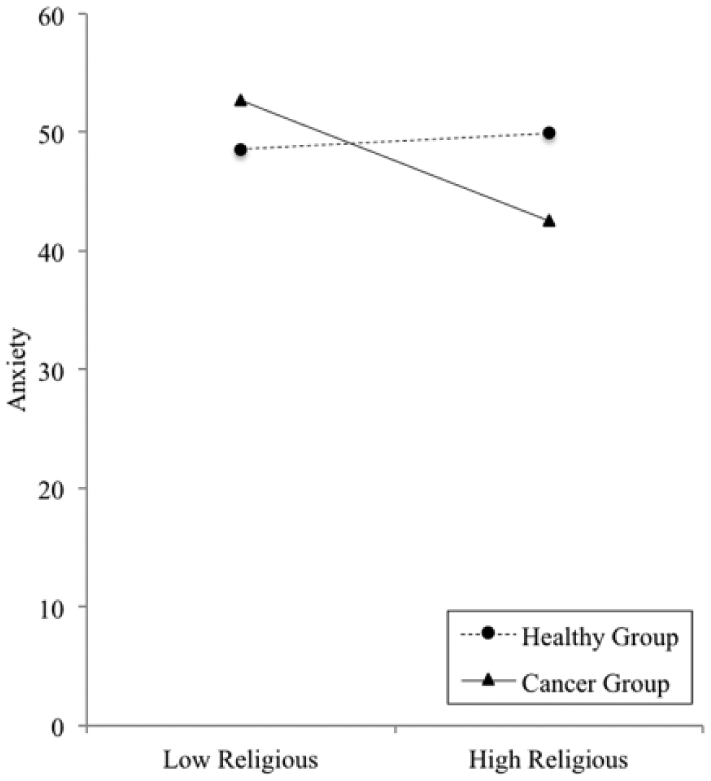
Plot of the moderating effect of health history on the relationship between Religious Well-Being subscale (Spiritual Well-Being Scale) and the Anxiety subscale.
Neither the Children’s Spirituality Lives measure nor the SWBS predicted Positive or Negative Coping factors; no significant findings were found in relation to health history. Notably, a simple comparison t test revealed that childhood cancer survivors had higher negative coping scores than their healthy comparison group (see Table 2). There were no other significant results.
Parent–child dyads
Fisher’s z transformations were used to examine whether or not parents of childhood cancer survivors had more highly correlated scores with their children’s spirituality, depression, and anxiety scores versus parents of healthy children. The results revealed that the correlations between parent–child dyadscancer (r = 0.576) were significantly higher than correlations between parent–child dyadshealthy (r = −0.134) on the Depression subscale (z = −6.31). The correlations between parent–child dyadscancer (r = 0.584) were significantly higher than correlations between parent–child dyadshealthy (r = 0.380) on the Existential Well-Being subscale (z = −2.47). Parent–child dyadshealthy (r = 0.314) were significantly more correlated than parent–child dyadscancer (r = 0.161) on the Duality factor (z = 2.08). There were no other significant differences.
Discussion
Spirituality and psychological health
As prognoses continue to improve with medical advances, the number of childhood cancer survivors continues to grow (Canadian Cancer Society’s Advisory Committee on Cancer Survivor Statistics, 2014). Although new and effective medical treatments continue to emerge, researchers have only begun to explore the post-treatment needs of children. The current findings suggest that some dimensions of children’s spirituality are correlated with reduced anxiety and depression for children after surviving cancer in childhood; these findings align with the findings of qualitative studies that also find positive outcomes related to spirituality (e.g. Kamper et al., 2010; Morse and O’Rourke, 2009; Woodgate and Degner, 2003). This study builds on past research by adding a much-needed quantitative perspective using spirituality measures and a healthy comparison group.
Compared to healthy peers, childhood cancer survivors had higher spirituality scores on the Comfort and Omnipresence factors of the Children’s Spiritual Lives measure and on the Religious Well-Being subscale of the SWBS; these factors and subscale all draw on a similar construct (i.e. relationship with a higher power, thoughts related to a higher power). In this study, children prayed to God for help, strength, and comfort (i.e. Comfort factor). Moreover, they felt that God was always ubiquitous and always listening (i.e. Omnipresence factor). Similarly, Kamper et al. (2010) found that the majority of pediatric cancer patients indicated wanting to feel close to God and praying to God for help.
Spirituality and coping
In this study, both positive and negative coping scores were not related to children’s spirituality in the moderation analyses. However, childhood cancer survivors had higher negative coping scores than the healthy comparison group. Due to frequent hospitalizations, children with a cancer diagnosis may miss school, and their social interactions may often be limited to family and hospital staff (Vance and Eiser, 2002). Upon recovery and survivorship, they may slowly integrate back into their social networks. Due to their possibly limited experience navigating peer social situations, it can be conjectured that they may resort more often to negative coping strategies (e.g. blaming others, wishful thinking, social withdrawal) when dealing with challenges in various relationships. To better support these children into survivorship, further investigation is needed to explore why childhood cancer survivors may resort to the use of more negative coping strategies.
Parent–child dyads
Parents’ understanding of their child’s spirituality was also of interest in this study. Parent–child dyads in the childhood cancer survivor group had more highly correlated scores than healthy parent–child dyads on Depression and Existential Well-Being subscales. Parents who have shared in their children’s cancer journey may be more aware of their children’s depressive thoughts, and the focus of the parent–child relationship may have shifted from concerns about achievement (e.g., school successes) to a greater emphasis on relationships and trying to find meaning in adversity (Thayer, 2009). With respect to the Existential Well-Being subscale, which includes questions related to thoughts about purpose and meaning in life (e.g. “I believe there is a real purpose for my life”), it is possible that parents and children may have more time to discuss these more meaning-oriented topics that might not have surfaced had their children not been diagnosed with a life-threatening illness such as cancer.
Healthy parent–child dyads, in fact, had more highly correlated scores than parent–child dyads of cancer survivors only on the Duality factor (e.g. “Every person has a body and something inside of them like a soul or a spirit”). Parent–child dyads with childhood cancer survivors may not have as many conversations about Duality because it concerns the idea of soul and spirit, which may evoke thoughts of mortality. It can be speculated that the thought of mortality may be too much of an anguishing prospect for childhood cancer survivors and their parents. Indeed, parents and children may engage in mutual pretenses (see Bluebond-Langner, 1978) when it comes to ideas of the soul, afterlife, and the possibility of death.
Limitations and future directions
The newly developed Children’s Spiritual Lives measure used in this study is still in early stages of development and has not yet been validated by a confirmatory factor analysis; thus, the current results that use this measure are exploratory in nature. Continued exploration of the scale’s strengths and weaknesses is warranted to ensure that it is appropriate to use with children from a diversity of faith and cultural backgrounds living in a pluralistic society. Although this measure is meant to be used with children from a wide variety of faith orientations, a better understanding of which factors are strongest or weakest in different faith groups would be helpful in future phases of the measure’s development. In addition, it is important to note that the SWBS used in this study is an adult-oriented measure and there are limitations in using such a measure with children (e.g. some difficult language).
Another limitation concerns the issue of inclusion criteria for the childhood cancer survivor participants. Given the challenges in recruiting childhood cancer survivors, the inclusion criterion concerning the number of months/years post-diagnosis was broad. Childhood cancer survivors with several different types of cancer at different stages of survivorship participated in this study. With a larger sample size, different types of cancer across stages of survivorship could have been explored. For instance, assessing children immediately after the diagnosis and later during the evolution of the disease, including survival, would be helpful to understand the child’s perception of spirituality throughout diagnosis, treatment, and survivorship. Certainly, examining children’s understanding of spirituality at different time points across the cancer experience may help researchers to capture, with more precision, the possible changes in spirituality due to the presence of cancer in childhood. These changes can then be more closely examined and compared to the experience of healthy children across various developmental time points.
Notably, children who survive cancer may have a much more positive report of spirituality than those children who receive a more negative prognosis (e.g. palliative care) or children who suffer permanent consequences (e.g. loss of a limb). Childhood cancer survivors who have fewer long-term side effects may have an overarching feeling of gratitude for their survivorship, whereas children with incurable cancer or impairing or permanent consequences from their cancer treatment may have a less positive report of spirituality. Researchers could explore these possible differences by refining inclusion criteria.
A future direction for research with significant implications for psychologists would be to closely examine the types of interventions (e.g. psychotherapy, medical play, group therapy, pastoral support) childhood cancer survivors receive over the course of their treatments. It would be important to determine whether there is any link between the type of intervention received and its relation between spirituality. Interventions that support spiritual expression (e.g. narrative therapy practices; see Moore et al., 2015) could be more closely examined in relation to psychological health. Children could also be interviewed to better understand how they perceive these interventions with respect to meeting their spiritual needs. Given this budding area of study, future researchers have many opportunities to investigate potential factors that may promote well-being throughout phases of childhood cancer survivorship.
Conclusion
In summary, this study found that children with a history of cancer had higher scores on certain measures of spirituality compared to their healthy peers, suggesting that spirituality is likely relevant for children who have survived a serious illness. Health history was found to significantly moderate the relations among spirituality and outcome variables, such as depression and anxiety. Furthermore, parent–child dyadscancer had more highly correlated scores than parent–child dyadshealthy on both the Depression subscale and the Existential Well-Being subscale, whereas parent–child dyadshealthy had more highly correlated scores than parent–child dyadscancer on the Duality factor.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Canadian Institutes of Health Research (CIHR) Doctoral Research Award.