
Abstract
Prior research demonstrates that family history influences breast cancer prevention decisions among healthy women at elevated risk of the disease. Drawing on in-depth interviews with 50 African American and White women, this study reveals an important psychological mechanism of this relationship: exposure to cancer among loved ones. Four distinct categories of cancer exposure (Abstract, Generalized, Practical, and Traumatic), distinguished by the characteristics of women’s experiences with cancer among family members and close friends, are associated with differences in knowledge and decisions about breast cancer prevention options. Racial differences and distinct experiences among those with BRCA mutations are also discussed.
Keywords
For women whose genetic predisposition puts them at high (20%–80%) risk of breast cancer, specific medical interventions can reduce the risk or enable early detection and treatment (National Cancer Institute, 2013). These options include bilateral prophylactic mastectomies (preventive removal of both breasts) or oophorectomies (preventive removal of ovaries and often fallopian tubes), chemoprevention (anti-estrogen medication such as tamoxifen), and enhanced surveillance routines (early or frequent clinical breast examinations, mammograms, and/or magnetic resonance imaging (MRI) of the breast). Each method is used far less frequently than clinical guidelines recommend (Ozanne and Esserman, 2010), but the decision-making processes that underlie this pattern are poorly understood (Padamsee et al., 2017). This article focuses on one important influence on women’s prevention decision-making: the role of a woman’s exposure to the cancer experiences of family and friends in shaping her own perceptions, feelings, and choices.
Prior research has revealed important but complex relationships between family history and prevention decisions. Women with a more substantial family history of breast or ovarian cancer are generally more likely to undergo routine screening tests and more motivated to pursue genetic testing (Howard et al., 2009; Tracy et al., 2008). Both the existence and number of relatives with breast or ovarian cancer are strongly associated with the choice to undergo prophylactic mastectomy and may also be associated with prophylactic oophorectomy (Bradbury et al., 2008; Howard et al., 2009; Kim et al., 2013). Cancer deaths among close relatives, and particularly the death of one’s mother at a young age, predict mutation carriers’ use of risk-reducing surgery (Hesse-Biber, 2014; Singh et al., 2013). Studies have found no association between family cancer history and the uptake of chemoprevention, but family history may be associated with beliefs about and early discontinuation of chemoprevention (Roetzheim et al., 2015; Smith et al., 2015). Risk perception and cancer worry may be among the mechanisms that mediate relationships between family history and risk management decisions (Price et al., 2007; Singh et al., 2013; Van Oostrom et al., 2006). It may not be only the existence of a family history of breast or ovarian cancer that shapes preventive behavior, but women’s personal experiences with cancer among family members (d’Agincourt-Canning, 2005; Dean, 2016; Hesse-Biber, 2014; Price et al., 2007).
This body of important research suffers from several notable gaps, which this article aims to fill. First, studies have just begun to explore how family history affects decisions, and the relationships between objective features and subjective experiences of these histories. Second, most studies focus on one intervention choice at a time, but most women face several in tandem. Third, most studies focus on mutation carriers, a critical group but only a subset of the high-risk women who face important risk management options. Fourth, little prior research explores variation across race, socioeconomic status (SES), or other characteristics.
Data and methods
This study is based on 50 original semi-structured interviews with women at elevated risk of breast cancer—20 African American and 30 White. Participants were recruited from the high-risk and genetics clinics at a major Midwestern Cancer Center and two databases of research volunteers; participants were at least 18 years of age and had no prior cancer diagnoses. The study was conducted with approval of the Institutional Review Board of The Ohio State University Comprehensive Cancer Center.
The semi-structured research protocol solicited women’s stories in their own words, on the topics of breast cancer risk, prevention decision-making, and related thoughts and feelings. Transcriptions were analyzed using grounded theory methods: inductive generation of themes by multiple coders, organization of themes into broader nodes, systematic coding into these themes and nodes, and analysis of patterns using excel tables and analytic memos. This article focuses on findings related to a subset of nodes: exposure to the cancer of a loved one, perception of personal cancer risk, prophylactic mastectomy, prophylactic oophorectomy, chemoprevention, surveillance, and genetic testing. Both breast and ovarian cancer risk are explored because the familial risks of both are intertwined. Additional methodological details, including the demographic characteristics of the sample, are available in the Supplemental File.
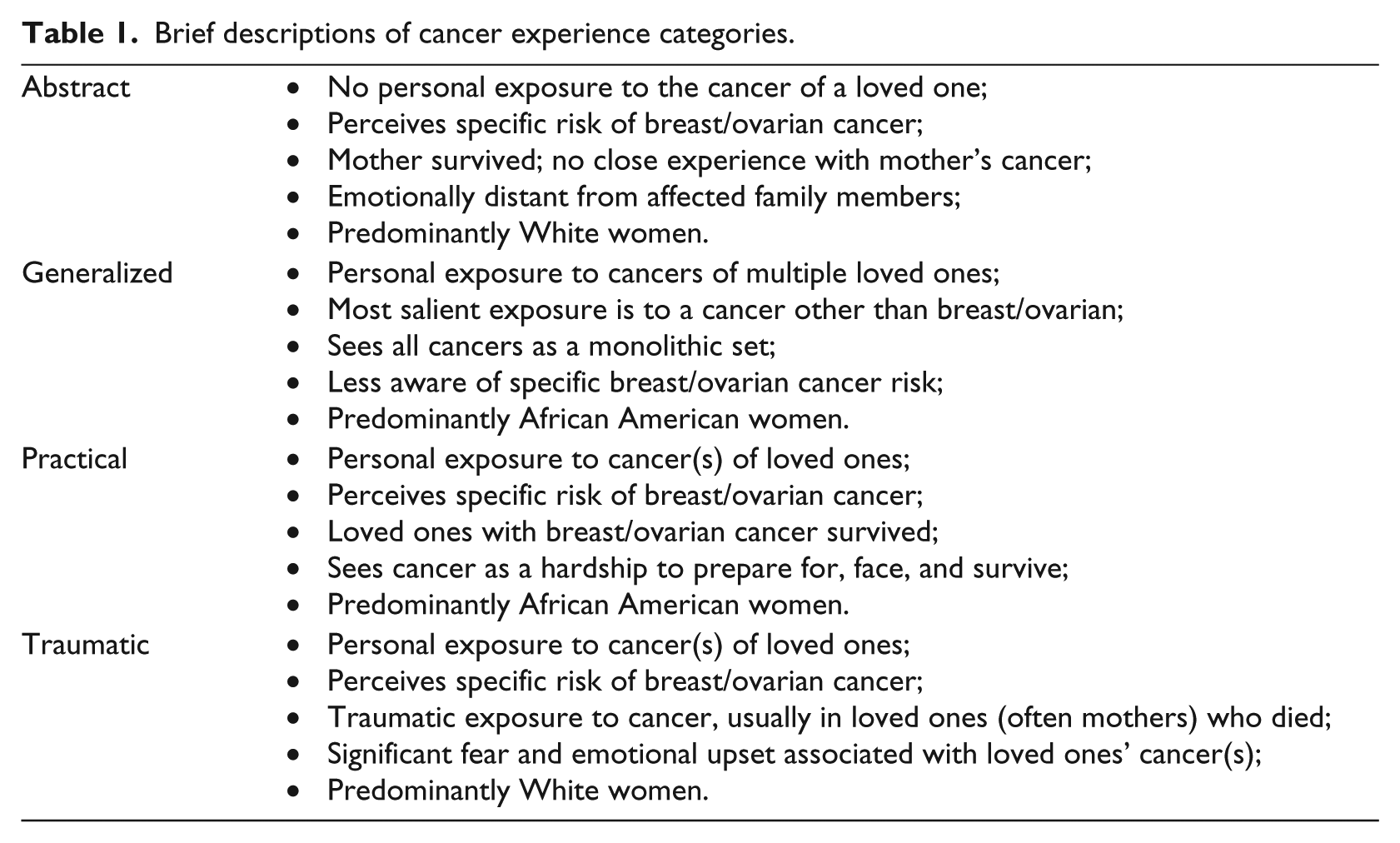
Participants often volunteered (usually unsolicited) stories about cancer diagnosis, treatment, recovery, and death among loved ones. Analysis of these reflections generated our concept of “cancer experience.” The category “loved ones” includes both family members and friends; friends are not relevant to objective (genetic) risk, but they do contribute to women’s broader experience of cancer and thus to their interpretations and behavioral choices. The women in this study were assigned to four categories of cancer experience: Abstract, Generalized, Practical, and Traumatic (Table 1). These groups were not preconceived but emerged inductively, as coding and analysis revealed commonalities and distinctions in women’s experiences. Women were assigned to groups using a flowchart-type approach (Figure 1), which involved assessing whether women had personal exposure to the cancer of a loved one, whether they experienced concern about breast/ovarian cancer specifically or about cancer more generally, and whether their personal experiences resulted in a lasting sense of cancer-related trauma.
Brief descriptions of cancer experience categories.
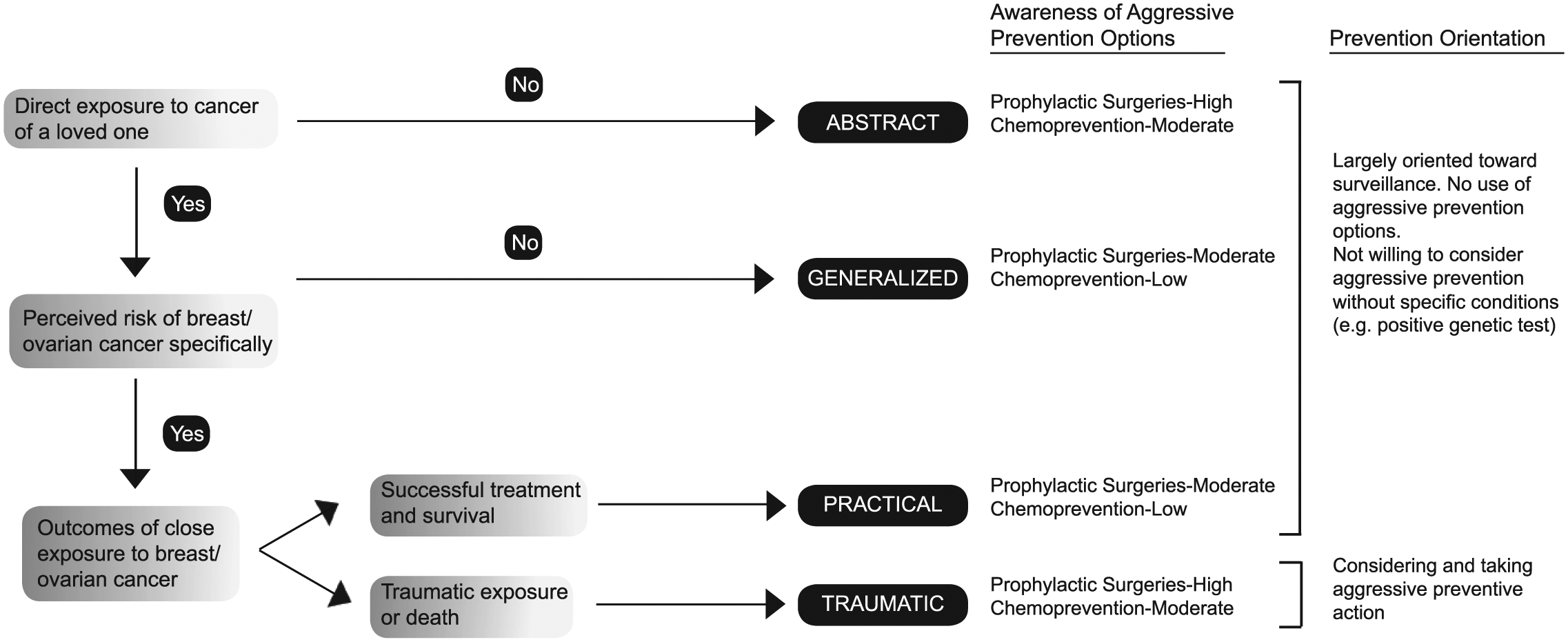
Cancer experience, awareness of prevention options, and prevention orientation among women without known BRCA mutations.
Prior cancer experience and its impact on prevention decision-making
The typology of cancer experience types presented here categorizes women in terms of the mental frame they bring to prevention decision-making. This “cancer experience” frame can also be conceptualized as a cognitive/emotional schema or a mindset. It encompasses types of exposure to cancer in family members or friends, involvement with those cancer cases, emotions these experiences evoked, and lasting impressions about what having cancer is like and how one should think about cancer risk, prevention, and treatment.
“Abstract” cancer experience
The 14 women (10 White, 4 African American) in our “Abstract” category were well aware of their elevated risk due to substantial family history, but—unlike women in the other categories—had no close up experience with breast or ovarian cancer. Both of Tessa’s grandmothers had breast cancer, for instance, but she had only vague knowledge of their situations: [My paternal grandmother] got breast cancer when I was in high school ….I don’t remember her going through the treatment. [When my other grandmother was diagnosed], she lived [far away]. And I don’t even know if they did much because of her age and her health. (Tessa—White, High Risk)
Physically or emotionally distant from affected family members, or too young to be part of their experiences, many expressed no strong feelings in connection with their stories of familial cancer. Only five had mothers who were diagnosed with breast cancer; none experienced it close up, and all their mothers survived.
Two of the women in this category carried a diagnosed BRCA mutation; their uniquely aggressive approach to breast and ovarian cancer prevention is discussed below. Of the other dozen women with Abstract cancer experience, 10 started cancer screening earlier than recommended for the general population due to their elevated risk. Many were also exceptionally meticulous about conducting breast self-exams (BSEs) (more than once/month) or getting breast exams from a physician (more than once/year). All 12 were aware that genetic testing was an option; 5 had been tested or specifically planned to do so.
Abstract category women were aware that surgical prevention options exist: 11 of the 12 women without known mutations had heard of prophylactic mastectomy, and 10 had heard of prophylactic oophorectomy. None had yet pursued either surgical option, however, and many articulated specific reservations: I have heard [of prophylactic oophorectomy but] … I’m still not sure if I’m done having babies, so it’s not something I would do right now … I would rather get screened more carefully if possible than rush out and put myself into early menopause …. (Sharon—White, High Risk)
About half said that they would consider a surgical option under specific future conditions—most commonly, receiving a positive genetic test result, but also when they were older, had completed childbearing, or if a doctor specifically recommended it. In contrast, fewer than half had heard of chemoprevention, and even those who had did not consider it to be personally relevant.
“Generalized” cancer experience
Despite their high risk of breast/ovarian cancer, the nine women (seven African American, two White) in the “Generalized” cancer experience category perceived themselves to carry not this specific cancer risk, but an unusually high risk of cancer in general. These women were distinct in thinking about all cancers as a set: Then my mom’s turn came in 1999. She got colon cancer at 64 … Then she turned around and got ovarian cancer …. Because of her brothers and sister and her, and my cousin who had the breast cancer, and then my grandma, I’ve always thought I was high-risk for some type of cancer. The type of cancer I’m really not sure because everyone died of so many different types of cancer. (Tanya—African American, High Risk)
Women in the Generalized category each had close experience of at least one cancer in a loved one, and they were usually involved in caring for this person. Their accounts all contained multiple references to cancers other than breast or ovarian, however, and their most salient and wrenching experiences were often of loved ones afflicted with other malignancies. Although five had mothers who survived breast/ovarian cancer and two were their mothers’ caregivers, none lost her mother to breast/ovarian cancer.
As a result of experiencing many cancers of varying types, women in the Generalized category often expressed the perception that “cancer is all over the family.” For some, this resulted in a degree of normalization or desensitization: they took risk for granted, expressing caution but not strong worry: I probably [would] say that it’s not “if” [I get cancer, but] “when.” But [I’m] not …doomed and gloomed about it … It’s just in the front my mind here and there, not all the time, not obsession, not depressed. (Karen—White, High Risk)
Close experience of cancer and a perception of generalized cancer risk shaped these women’s approaches to cancer screening and prevention. Most were willing to undergo genetic testing if recommended and affordable. Compared to women in the Abstract group, somewhat fewer of these women started (or planned to start) cancer screening early; many nevertheless emphasized early detection specifically because they did not believe these cancers could be prevented. Less than two-thirds had heard of the surgical interventions that might be appropriate for women in their situation, only two of the nine had heard of the chemoprevention option, and none were currently considering any of them. If specific conditions were to arise (e.g. getting a positive genetic test result or having a doctor recommend it), these women were more likely to consider a preventive surgery than chemoprevention.
“Practical” cancer experience
Nine women (six African American, three White) can best be described as taking a “Practical” perspective out of their experiences with cancer. These women had both experienced the cancer of a loved one directly, like those in the Generalized category, and had a psychological focus on familial risk of breast/ovarian cancer specifically, like those in the Abstract category. They had not, however, experienced traumatic suffering or death. They generally perceived of cancer as a hardship they must be ready to deal with, but that could be survived. Two-thirds of these women had mothers who were affected by but survived breast or ovarian cancer. These memories were both clear and influential: When [my mom] had breast cancer … I was … something like 12, 11 … I wasn’t particularly afraid of the cancer; I was afraid that my mom couldn’t handle the stress because she was going through a lot of treatments. …[My perspective] is all predicated on the fact that my mom has come through it very well. I’m sure I’d have a different story if she didn’t. (Kim—White, High Risk)
About half were closely involved with a loved one other than a mother who also survived their illness; none had substantial contact with a relative who died.
Like women in the Generalized category, women in the Practical category were generally consistent about mammograms and MRIs (if recommended). It was also their norm to conduct regular BSEs and some—such as Roxy, who examined her breasts every time she showered—were unusually proactive in this regard. More than half were willing to undergo genetic testing and some had already done so.
The proportion of Practical group women aware of breast cancer prevention options was slightly higher than in the Generalized group, but lower than in the Abstract group. Like women in both prior groups, these women did not consider chemoprevention or prophylactic surgery to be personally relevant. Most summarily dismissed the chemoprevention option. Just under half of those who knew about preventive surgeries would consider them under some imaginable condition—this was a similar proportion to women in the Abstract category, and fewer than in the Generalized category. Consistent with their general orientation toward surveillance over aggressive prevention, however, most Practical group women expressed serious reservations about prophylactic surgery: You’re being preventative, and active in getting mammograms and things like that. If you catch it early enough, you can deal with it, then you don’t have to [preventively] remove your breasts. (Sophia—White, High Risk)
“Traumatic” cancer experience
A total of 18 women (15 White, 3 African American)—associated breast and/or ovarian cancer with traumatic past experiences, and approached prevention quite differently from women in the other three groups. They had experienced breast/ovarian cancer close up, and their sense of personal risk was specific to those cancers. Women categorized in the “Traumatic” group were thus similar to those in the Practical group, with one critical distinction: they had each suffered through at least one particularly difficult cancer experience with a loved one. In most cases, the loved one died of their cancer, but a few women experienced long-lasting fear and emotional upset as the result of cancer experiences with family members who survived.
The harrowing experience of a mother’s cancer had striking impact on most of the women in this group. They described their personal histories as “traumatic” and “horrible,” and repeatedly expressed determination not to go through what their mothers did, not to die as their mothers did, and not to put their children through what they experienced. Many were caregivers of mothers who died, leaving them with haunting memories: …I’m not dying the way she died … It got into her bones. She stood up once and her thigh bone snapped in half … They medicated her with so much morphine that her mind went. There’s no point in living like that. I’m not gonna go out like that. (Carol—White, High Risk)
For those who were too young to be caregivers, emotional recollections of childhood fear and grief evoked determination not to expose their own children to these feelings. Also, common were influential stories of illness and death among grandmothers, sisters, favorite aunts, uncles (with rare male breast cancer), and even close friends. Many of these women had lived through not one but multiple difficult cases, and the pain of breast/ovarian cancer could also be a multi-generational experience.
Four Traumatic category women had been diagnosed with a BRCA mutation—their prevention behavior is discussed below. The prevention behavior of the remaining 14 was distinct from that of women in the three cancer experience groups above. All were aware of genetic testing as an option, and most were positively disposed toward it. Five had already been tested, and six others were in some phase of planning to test. Traumatic category women expressed a uniquely high level of anxiety about screening, sometimes wanted earlier or more frequent mammograms than their doctors recommended, and expected that sooner or later a screening test would reveal a cancer.
The Traumatic group is the only cancer exposure category within which women without known genetic mutations were seriously considering, and even taking, aggressive preventive action. A total of 5 of these 14 women had been advised of prophylactic oophorectomy as an option and were inclined to pursue it. A total of 12 had heard of preventive mastectomy, and 7 considered it an option to be seriously considered. As Ramona (African American, High Risk) articulated, “I don’t know if I have that gene, but, if I had the gene, that would be something I would definitely consider … I think I would be comfortable living without breasts for the rest of my life.” This openness to prophylactic mastectomy was distinct among women in the Traumatic group; of the 30 women without known BRCA mutations in the other three groups, only 1 had seriously considered it, and 12 others said they would consider it under some imaginable future condition.
These women also approached chemoprevention in a relaxed and accepting manner notably distinct from women in the other three groups. Of the six Traumatic group women who had heard of chemoprevention, two had already taken it and two would seriously consider it under specific conditions.
The cancer experience exception: women with known BRCA mutations
Six of the women in this study had been diagnosed with BRCA mutations, which put them the highest category of breast and ovarian cancer risk. Based on cancer experience, two fell into the Abstract group, and the other four into the Traumatic group. Knowledge of their mutations strongly drove their prevention behavior regardless of cancer experience, however, and all six were unified by a clear commitment to aggressive preventive action. Five had already chosen to have their ovaries removed; the sixth had been more recently diagnosed as a BRCA mutation carrier and was leaning toward this same choice. Three had also chosen to have their breasts removed, two others said they might consider doing so in the future, and the only woman disinclined toward prophylactic mastectomy was leaning toward chemoprevention.
Three women responded to the news of their high cancer risk by undergoing both risk reduction surgeries. This decision was straightforward for some, supported by both personal experience and medical recommendations for BRCA mutation carriers: If I found out that I had the mutation, I [was] getting a mastectomy. I already knew. I got a hysterectomy [and oophorectomy] because of my mother’s [ovarian cancer] …it’s a no-brainer for me. They’re boobs. It’s not like cutting off my hands and I can’t write anymore, you know? (Lainie—White, Severe Risk)
For others, it was fraught with grief and pain. Kathryn received the devastating news of her BRCA1 mutation as her mother was dying of a second cancer. Kathryn’s husband advocated mastectomy that very evening, saying “we absolutely need you around for the kids.” Kathryn initially resisted but soon changed her mind: When I found out I was positive, it changed me forever. I couldn’t sleep …. I was on the Internet all hours of the night … It’s just what cancer does to people … It’s just unfathomable. I was in a bad place … I had the mastectomy. (Kathryn—White, Severe Risk)
Kathryn subsequently gave birth to another child, and then had her ovaries removed as well.
The other three mutation carriers were also strongly motivated to take whatever preventive action was necessary, but less certain about the best path to risk reduction. For Lucy (White, Severe Risk), uncertainty about future childbearing, fears of early menopause, and the feeling that “I’m pretty attached to my body parts” made oophorectomy a decision fraught with anxiety and fear—something she avoided for years but felt she must eventually do because, “I cannot … put my kid in the same position I was in.”
Discussion
Direct exposure to the cancers of loved ones, whether or not the cancers were predominantly breast/ovarian, and the health outcomes among these loved ones’ cases delineate distinct categories of prior cancer experience among women at elevated risk of breast cancer. As the filter through which women approach prevention decision-making, cancer experience seems to shape women’s understanding of their prevention options, their use of cancer screening and genetic testing, and their degree of inclination to take aggressive preventive action in the form of prophylactic surgery or chemoprevention (Figure 1). Women who already know they carry a BRCA mutation are substantively different than other high-risk women in this sample, however, manifesting a commitment to definitive preventive action regardless of their prior experiences with the cancers of loved ones.
Despite their lack of direct contact with the experience of cancer, women in the Abstract category had heard of chemoprevention and prophylactic surgeries about as often as women in the Traumatic category, and more frequently than those in the Generalized and Practical groups. This is a counterintuitive pattern, given that women in all other categories clearly described direct experiences of cancer among loved ones as motivating their interest in prevention and early detection. It may be partially explained by a racial effect, as Abstract category women are more often White than women in the Generalized and Practical groups; by their educational levels, which are marginally higher than those in all the other groups; or by differences in other features of their family history or clinical relationships. A larger dataset would make it possible to investigate these possibilities more thoroughly. For whatever reason, however, these data suggest that lack of direct contact with cancer is not as much of an impediment to prevention option awareness as lack of specific perception of breast/ovarian cancer risk.
Among women in the Generalized category, perceived risk of all cancers does not match biological risk of breast/ovarian cancer specifically. Some may carry high familial risk of other cancers as well, but in our sample, their general sense that all cancers are equally likely is associated with less understanding of prevention options than any other group and undercuts their willingness to take risk-reducing actions. It is also important to note that while some of these women have had traumatic experiences with non-breast/ovarian cancers in loved ones, they are markedly less likely to have taken or be considering aggressive preventive action than women in the Traumatic group.
For women in the Practical category, it was often a question of “when” they would get cancer, not “if.” As a result, they perceived of cancer as a disease to screen for vigilantly, catch early, and treat promptly. Women in this category were mostly African American—a surprising pattern worth confirming in future investigations, given that African American breast cancer patients tend to suffer worse outcomes than White women (Newman and Kaljee, 2017).
In all three of these groups—Abstract, Generalized, and Practical—women were strongly oriented toward surveillance and generally open to genetic testing. They were not currently considering any form of aggressive preventive action, but at least half were willing to consider prophylactic mastectomy or oophorectomy under conditions such as finding out they carry a BRCA mutation. Few were willing to consider chemoprevention under any circumstances.
In our sample, Traumatic category women were substantially different than those in the other three groups, in terms of both cancer experience and prevention behavior. Having lived through harrowing cancer experiences with loved ones, they were as vigilant about surveillance as others, but also expressed a high degree of anxiety about regular screening as a method of coping with risk. They were the only women without known genetic mutations engaging in aggressive preventive actions, usually viewing preventive surgery as an obvious choice and even considering chemoprevention—the least popular prevention method in all groups. Witnessing the death of a mother, mother-figure, or close friend exerted particularly strong traumatic impact, as did serving as primary caregiver or being exposed to death as a child. These findings extend those of Hesse-Biber (2014), who also found that seeing someone die affected women’s choices, that seeing someone survive gave the impression that there is no need for extreme preventive measures, and that experience with mothers’ cancers exacerbated these effects.
For women with known BRCA mutations, the import of cancer experience was replaced by the known risk implications of the genetic test result, which produced an urgent determination to protect themselves and their children by taking aggressive preventive action. This strong orientation of women with known mutations toward aggressive prevention is consistent with the fact that women in all four cancer experience groups indicated that they would be inclined to pursue such action if they were found to carry a genetic mutation. It is also consistent with the facts that women undergoing genetic testing may have more financial resources to devote to prevention than others and that they have often already mentally committed to take actions to both prevent cancer and manage medical uncertainty if the test comes back positive (Dean and Davidson, 2018; Landsbergen et al., 2010; Van Dijk et al., 2008).
African American and White women—as aggregate groups—do seem to cope differently with prevention decision-making. Members of both racial groups were present in each cancer experience category, but African American women comprised most members of the Generalized and Practical groups and were correspondingly under-represented in the Abstract and Traumatic groups. Although they bring distinct mental frames to the process of prevention decision-making, Generalized and Practical group women are behaviorally quite similar—in prevention option awareness, use of surveillance and genetic testing, and willingness to consider aggressive prevention action. If race sorts women into cancer experience groups through biological and social processes, White and African American women may be set up for different life experiences with cancer, which subsequently shape their orientations toward breast cancer risk reduction.
Limitations of the study stem primarily from characteristics of its sample. The inductive analytic approach to in-depth, open-ended data is uniquely well suited to generate findings like those reported here. Larger samples, and survey-based datasets amenable to statistical analysis, could now be used to test these relationships more rigorously. Both wider and finer grained information about women’s objective risk status, and data documenting clinical interactions, may shed additional light on how women form impressions of their breast cancer risk and prevention options, and the level of concordance between women’s objective risk status, the information they are given, and the prevention decisions they make. In addition, this sample contains few mutation carriers, few women of Ashkenazi Jewish descent, and insufficient variation in race-ethnicity, geographic region of origin, and SES; a larger and more representative sample would allow deeper exploration of unique patterns associated with these characteristics.
Our findings suggest several directions for future research. First, follow-up interviews and longitudinal research could help map the dynamic process of prevention decision-making. Second, further analysis of qualitative datasets is necessary to understand why women are disinclined to use chemoprevention and whether it has any future role in applied breast cancer prevention. Third, future analyses of women’s stories may shed light on the prevalence of barriers to carrying out one’s decisions (once made). Intervention design studies will be important as well, to support better awareness of prevention options and follow-through with informed decisions. Finally, designing new continuing medical education courses may be necessary, if clinicians are to use information about high-risk women’s cancer experiences to help improve prevention decision-making.
Implications for policy and clinical practice
This study has a range of implications for policy and clinical practice. First, spending the time to understand a woman’s cancer experience could enlighten clinicians about the mental frame she brings to conversations about risk, prevention, and early detection. Patients in the Abstract category may be most amenable to logically presented information focused purely on risk and prevention options. Women with Generalized experience may benefit from clarification of their biological risks beyond breast/ovarian cancer, support related to their worry about all cancers, and discussions of which prevention behaviors may generate the best overall risk reduction. Those with a Practical orientation may be particularly likely to adhere to enhanced surveillance routines and may need additional information in cases where more aggressive preventive action is strongly indicated. Patients who have had Traumatic experiences are more likely to be fearful or anxious, less likely to tolerate extended surveillance routines, and highly motivated to do what is necessary to prevent cancer.
Second, considerable work remains to be done in educating women about the prevention options from which they might benefit; the broader population of high-risk women may have even more limited awareness than those in this self-identified sample. Third, if the racial distinctions documented here are confirmed, it might be useful to raise clinician awareness that African American women are likely to bring certain mental frames to their decisions, while White women bring others. Finally, practical changes that facilitate women’s access to genetic testing (through education and/or insurance coverage) could have substantial impact because many women may choose to behave differently with the benefit of that information.
Conclusion
Women’s stories about cancer experience range from distant knowledge of the cancer of a grandmother who eventually recovered and thrived to intimate knowledge of a mother’s profound suffering and death. The impact of these events on the women in our sample differs across the cancer experience typology, from pragmatic determination to be vigilant about screening mammograms, to daily awareness of breast cancer as a frighteningly likely diagnosis that could leave one’s children without a mother. This study demonstrates that family history is more than just the biological relationships that determine objective risk; it is also a critical category of subjective experience that helps forge women’s risk perceptions and prevention decisions. Exploring family history and providing prevention information cannot therefore be a “one size fits all” process; taking cancer experience into account will facilitate tailored support to help set high-risk women on the road to informed and empowered prevention decisions.
Footnotes
Acknowledgements
The authors would like to thank Anne Esacove and Lisa Fein for their comments on drafts of this manuscript and the research contained herein, and to acknowledge excellent recruitment, coding, and editorial support from Tiffany McCoy, Rachel Meadows, and Megan Hils.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the generous support of the National Cancer Institute, Grant # K01 CA181547.
Supplemental material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.