
Abstract
Impact and adjustment to a drainage enterostomy are measured mainly through health indicators. To investigate the relationship between resilience and adaptation to the placement of a drainage enterostomy. Prospective observational study with a sample of 125 patients (64 men/36 women) with a temporary or permanent drainage enterostomy and a mean age of 66.72 years. High quality of life (mean, 80.5) and resilience (mean, 79.57) scores and a positive relationship between both were found. There seems to be a positive relationship with general quality of life and health-related quality of life. The logistic regression model shows that the main predictor as regards health-related quality of life is resilience.
Introduction
In recent decades, the concept of health has undergone important changes, chronic diseases becoming the main health problem. Advances in science and technology and the ageing of the population are two factors that have led to an increase in the number of people that live with chronic pathologies (Instituto Nacional de Estadística (INE), 2013; Vera et al., 2014). These include patients with colon cancer or inflammatory bowel disease, where intestinal drainage ostomy can often be found as the main consequence of their treatment. As proof of this increase, recent studies have shown that in Spain, there are about 70,000 people with ostomies and the incidence is growing at a rate of around 13,000 new cases per year (Cancio López et al., 2014).
In order to study how these patients adjust to their disease, it is necessary to understand that intestinal stoma surgery is a procedure in which the compromised part of the intestine is removed and a conduit is constructed through the intestinal wall to allow faecal matter to be discharged.
This surgical intervention is, therefore, an invasive procedure that often gives rise to digestive and hydroelectrolytic alterations. Coping abilities must, therefore, be developed to help patients deal with this situation of great stress and discomfort (Mathis et al., 2013)., Moreover, chronic diseases, as is the case of having an enterostomy, are defined as diseases that are prolonged in time, do not resolve spontaneously and are rarely fully cured. Hence, the chronic suffering of these patients is related to symptoms of disability that lead to different degrees of dependency and require long-term treatments, including initiatives aimed at helping patients to learn to live with the ensuing limitations and actions designed to control the clinical manifestations, as well as to prevent complications. Furthermore, having a drainage enterostomy entails an important behavioural shift in one’s daily routines, in addition to having to incorporate within one’s daily life a series of new behaviours related to personal care and hygiene that require a great deal of time and dedication. These conditions generate a high degree of stress and discomfort, with a large emotional burden that alters social aspects such as family relationships, friendships or leisure activities, among others (Weston and Jackson, 2014). All these changes, therefore, require a period of adaptation or adjustment to the new situation, in those patients who are able to do so.
Health professionals measure adjustment to a disease and make health decisions based on a series of health indicators. Hence, the quality of life (QL) of patients with a drainage ostomy is taken as one of the most important health indicators when it comes to predicting the level of psychological adjustment to the new condition (Black, 2010; Campillo and Zaragoza, 2014; Dabirian et al., 2011; Golicki et al., 2013; Hu et al., 2014; O’Connor, 2005; Shun et al., 2011). It should be remarked that QL refers to the subjective perception of important aspects of a person’s life; that is to say, it has to do with the significance that people attribute to it, and in this sense, it is a social construct. More particularly, health-related quality of life (HRQL) is the aspect of QL that refers specifically to the health of a person and is used to designate the particular outcomes of clinical evaluation and therapeutic decision-making (Fernández et al., 2010; Mezzich et al., 2011). Many studies conducted with patients with a drainage enterostomy use general QL as a health indicator (Anaraki et al., 2012; Geraldo et al., 2014; Krouse and Grant, 2003; Marquis et al., 2003). An increasing number of studies and researchers, however, are creating and using instruments to measure the specific QL for the condition of having a drainage enterostomy (Baxter et al., 2006; Marquis et al., 2003; Olbrisch, 1983; Prieto et al., 2005; Sprangers et al., 1999). These studies have shown that the QL of patients who have a drainage enterostomy is compromised (Cancio López et al., 2014; Grant et al., 2007). They have also revealed that the financial part of their QL is especially affected (Maydick, 2014). Other studies conclude that the social part is the most strongly disrupted, although the psychological part and management of the ostomy are also compromised, along with sexual relationships (Anaraki et al., 2012; Liao and Qin, 2014; Popek et al., 2010). Among the variables that have been seen to have a greater effect on the perception of the QL, those considered to have the strongest impact on the perception of HRQL are suffering some kind of complication; leaks and smells; clothing and change of image; and sleep disorders (Canova et al., 2013; Jansen et al., 2015; Liao and Qin, 2014; Person et al., 2012).
In this process of adapting to new stressful situations, as is the case of having a drainage enterostomy, it has been quite clear for many years that there are individual differences in the way people adapt to them. Understanding these differences in adaptation is addressed on an increasingly frequent basis from the resilience approach (Waaktaar and Torgersen, 2010).
All the definitions of the construct of resilience put forward by researchers in studies on resilience and health share a number of common points that are important when it comes to relating this construct with the health process. These common points are: for resilience to develop, it is necessary to have first undergone an adverse event; it is the ability to maintain good levels of health functioning or to return to normality despite adversity; and finally, factors from different systems are considered to be involved in resilience or it is understood as a dynamic process as opposed to a set personality trait (Johnston et al., 2015). Hence, this conception gave rise to a strong interest in studying resilience and examining its relationship with adjustment to chronic disease. Resilience can, therefore, be defined as the capacity of persons exposed to traumatic events to maintain relatively healthy and steady levels of psychological and physical functioning, as well as the capacity to generate positive experiences and emotions (Bonanno et al., 2008). In their studies conducted on people with severe diseases, these authors identified four prototypical patterns or long-term responses that most people present as in answer to the stress of suffering from such a disease, namely, the resilience, chronic dysfunction, recovery and delayed reaction patterns (Morin et al., 2017). They also highlighted the difference between recovery and resilience. In their view, recovery from traumatic events is associated with an increase in the number of psychological problems over a period of time, and the resilience pattern is characterised by seeking social support, getting on with life and accepting circumstances with hope (Bonanno and Diminich, 2013; Garcia-Dia et al., 2013; Ho et al., 2010).
Of special importance is the understanding of resilience and adjustment to disease in patients who have been diagnosed with some kind of cancer. As a consequence of a diagnosis that is seen to be potentially fatal, the levels of tension or stress rise in healthy persons, in addition to finding themselves with the need to cope with many changes in their life and to continue to adapt to them (Hou et al., 2010; Molina et al., 2014). The results of studies carried out on patients with cancer can be considered in the same line, since they show that resilience is positively correlated with health indicators such as emotional health and well-being (Lamond et al., 2008), life satisfaction, self-esteem, social adaptation (Benetti and Kambouropoulos, 2006; Peng et al., 2012) and social support (Clauss-Ehlers, 2008; Connor and Davidson, 2003; Van Dick et al., 2017). In contrast, negative correlations have been found with negative emotions (Burns and Anstey, 2010), depression and anxiety (Kawasaki et al., 2011; Peng et al., 2012), vulnerability to stress (Min et al., 2013) and distress and emotional stress (Ho et al., 2010).
Many studies provide scientific evidence that resilience is predictive of a lower level of distress, better adjustment and improved QL in patients with a chronic disease (Bowen et al., 2003; Costanzo et al., 2009; Haase et al., 2014; Harris et al., 2010; Lee et al., 2007; Liu et al., 2012 Molina et al., 2014; Ong et al., 2009; Rowland and Baker, 2005; Strauss et al., 2007; Temprado et al., 2019; Wu et al., 2015). In this study, we inquired into the relationship between resilience and QL factors (QL and HRQL) in patients with a drainage enterostomy. The objective of our research is to analyse the impact of a chronic process, as is the case of a drainage enterostomy, on the HRQL of these patients and to determine whether resilience has some kind of positive or negative relationship with it. Similarly, it also intends to analyse what types of clinical or sociodemographic variables have some kind of influence upon it. We believe that this knowledge and the results of this study can be very useful to carry out interdisciplinary intervention programmes aimed at improving resilience and self-care that would limit the occurrence of complications and improve the QL of these patients.
Method
We designed a multicentre correlational cross-sectional study to be conducted with colo/ileostomised patients over a period of 3 months, in hospitals with a digestive surgery service and a stoma therapy nursing unit in the province of Castellón.
Inclusion and exclusion criteria
Inclusion criteria
Participants in the study had to be of legal age. Following a criterion established in previous studies on the adjustment of patients with an enterostomy (De Frutos et al., 2011), they had to be colo/ileostomised patients with an enterostomy who had completed a post-surgery adaptation period of at least 3 months.
Exclusion criteria
Both patients in the terminal phase of their disease and those who had an insufficient command of Spanish were discarded from the study. Neither were patients with cognitive ability deficit included in it.
Ethical aspects
The decision rights, anonymity and confidentiality of the participants were safeguarded at all times, respecting the ethical principles described in the Belmont Report and the Nuremberg Code.
To be able to gain access to the sample, it was first necessary to obtain permission from two CRECs (Research Ethics Committees) and authorisation from the management committees of the four hospitals in the health department in which the study was conducted.
In order to comply with current data protection legislation, the study was completely anonymous and the patients were coded on being incorporated into the study. Hence, at no time do any data appear that could be used to identify them.
Participants and procedure
The initial sample consisted of a total of 185 patients who had had a drainage enterostomy for more than 3 months. After applying the inclusion criteria, the final sample included in the study consisted of 125 patients (n = 64 males and n = 36 females).
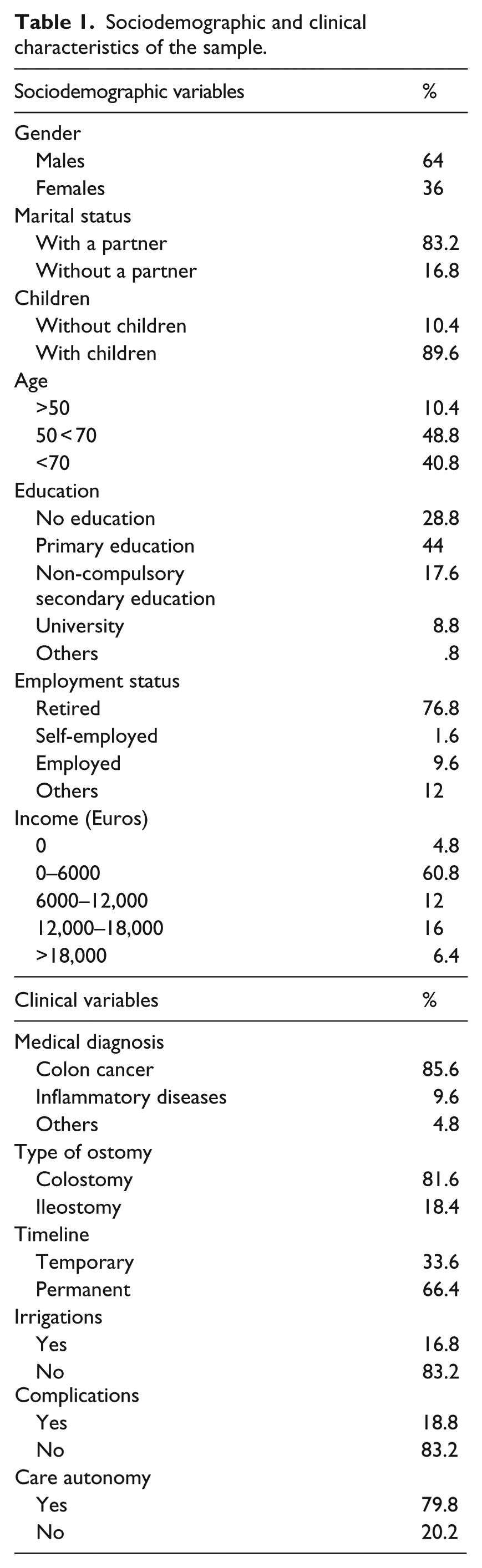
As can be seen in Table 1, their ages ranged from 36 to 87 years old, with a mean age of 66.72 years (standard deviation (SD) = 11.85). Of these, 85.6 per cent were patients diagnosed with colon cancer, 7.2 per cent of them had been diagnosed as suffering from an intestinal inflammatory disease (i.e. Crohn’s disease or ulcerative colitis), 3 per cent presented a diagnosis of diverticulitis and the remaining 4.2 per cent had undergone surgery due to other causes (i.e. endoscopic perforations, traumatic injury resulting from a road accident and intestinal infarction). With respect to the type of enterostomy, the majority of them had a colostomy (81.6%) versus 18.4 per cent who had an ileostomy. Most of the patients (80%) reported being autonomous when it came to caring for their stoma, and only 16.8 per cent of them performed irrigations on a regular basis. And, 83.2 per cent of the patients with an enterostomy reported never having had any kind of complication with it.
Sociodemographic and clinical characteristics of the sample.
Instruments and measurements
Demographic and basic medical information
The researchers collected sociodemographic variables through personal interviews with patients (sex, age, reference hospital, marital status, studies, labour activity, number of children and economic income), and clinical variables (date of the surgical operation, medical diagnosis, type of ostomy, whether it was temporary or permanent, stoma level, irrigations, autonomy in stoma care or stoma-related complications) were obtained from each patient’s medical history. The questionnaires used in this study were administered by the two main researchers, a psychologist and a nurse, with unified criteria, in personal interviews lasting between 45 and 60 minutes conducted in the respective hospitals. The appointments were arranged previously by telephone, after informing the patients of the objective of the study.
Resilience
This was measured by means of the Spanish version of the Connor–Davidson Resilience Scale (CD-RISC), translated from the original English by Bobes et al. (2001). The scale consists of 25 items measured by means of a Likert-type scale that ranges from 0 (Not at all) to 4 (Nearly always). The exploratory factor analysis performed by Connor and Davidson (2003) identified five factors that they called (1) personal competence, high standards and tenacity; (2) Trust in one’s instincts and tolerance of negative affect, and strengthening effects of stress; (3) the positive acceptance of change, and building secure relationships; (4) control; and (5) spiritual influences. The range of the scale is from 0 to 100. No cut-off point was established for it and, thus, the higher the score is, the higher the person’s level of resilience is.
General QL
This was measured by means of the Quality of Life Index (QLI)-Spanish version, which consists of 10 items each corresponding to a general QL indicator that are measured on a Likert-type response scale that ranges from 1 (Poor) to 10 (Excellent). These indicators are physical well-being, psychological and emotional well-being, self-care and independent functioning, occupational functioning, interpersonal functioning, social-emotional support, community and services support, personal fulfilment, spiritual fulfilment and overall perceived QL (Mezzich et al., 2011). The range of the scale is from 0 to 100. No cut-off point was established for it and, thus, the higher the score is, the higher the person’s level of QL is.
Specific QL for patients with an enterostomy, or HRQL
This was measured by means of the Stoma-QOL (Quality of Life Questionnaire for patients with colostomy or ileostomy) (Prieto et al., 2005). The questionnaire provides qualitative indicators that express the impact on QL and patient satisfaction. It consists of 20 questions with a Likert-type scale of four answers that are rated with a score of 1 to 4. The final score that was calculated gives us 80 per cent, so we must add 20 per cent to the total to achieve a tabulation of 100 per cent. From this total, three levels of measurement were considered: good QL (result of 70%–100%), moderate QL (result of 30%–70%) and poor QL (result of 0%–30%).
Data analysis
To adapt the measuring instruments referring to resilience and QL to this sample of patients, we followed the indications given by George and Mallery (2003) with regard to the values of Cronbach’s alpha coefficient (Excellent > .9, Good .8–.89, Acceptable .7–.79, Questionable .6–.69, Poor .5–.59 and Unacceptable < .5). Confirmatory factor analysis (CFA) was also performed by structural equation modelling (SEM) using EQS 6.1 and following the robust indices. Thus, the model was considered to fit when the Satorra–Bentler χ2 was not significant (p = .05), the BB-normed fit index (BB-NFI), BB-non-normed fit index (BB-NNFI), comparative fit index (CFI) and incremental fit index (IFI) were higher than .9 (if the NFI is not higher, the NNFI must be) and the root mean square error approximation (RMSEA) was below .08 (Herrero et al., 2011).
The following statistical analyses were performed with the software package SPSS v23. The level of statistical significance required was 5 per cent (p = .05).
A univariate descriptive analysis was performed for both the sociodemographic and the clinical variables. The continuous variables are, therefore, described by measures of central tendency and SD, and frequencies and percentages are used for the categorical variables.
For the correlation or bivariate analyses, first the normality of the quantitative variables was analysed with the Kolmogorov–Smirnov test in order to determine whether parametric or non-parametric tests should be used. For the non-parametric tests, the Mann–Whitney U or the Kruskal–Wallis H were obtained. In the case of the parametric tests, an Independent samples t-test was conducted with variables that only had two categories or levels, whereas a one-factor analysis of variance (ANOVA) was performed for variables with more than two categories or levels. In the cases in which the ANOVA revealed significant differences in the comparisons for variances, a Bonferroni post hoc test was conducted to determine which pairs of categories or levels had significant differences between them. In both Student’ t-test and ANOVA test, the null hypothesis that the population variances are equal (variance homogeneity) was tested by means of Levene’s test, and the study proceeded accordingly.
Finally, and in order to study the relation between variables and identify the predictive value of the variables in the perception of the QL related to the particular health problem under study (HRQL), a multiple regression analysis was performed following the stepwise method.
Results
Adaptation of the measuring instruments (CFA)
Adaptation of the CD-RISC by Connor and Davidson (2003) and translated into Spanish by Bobes et al. (2001). This instrument was adapted to the study sample by means of CFA followed by the corresponding SEM. This resulted in a questionnaire consisting of 17 items with a one-factor structure (Satorra–Bentler χ2 = .0488, BB-NFI = .709, BB-NNFI = .913, CFI = .926, IFI = .930, RMSEA = .043). It also had a Cronbach’s alpha coefficient that could be considered as Good (α = .836).
Adaptation of the Quality of Life Index-Spanish Version (QLI) (Mezzich et al., 2011). This instrument was also adapted to the study sample by means of CFA and then the corresponding SEM. This resulted in a questionnaire consisting of nine items with a one-factor structure (Satorra–Bentler χ2 = .2455, BB-NFI = .902, BB-NNFI = 924, CFI = .955, IFI = .957 and RMSEA = .075). It had a Cronbach’s alpha coefficient that could be considered as Good (α = .851).
Adaptation of the Stoma-QOL (Quality of Life Questionnaire for patients with colostomy or ileostomy) (Prieto et al., 2005). This instrument was also adapted to the study sample by means of CFA and its corresponding SEM (Satorra–Bentler χ2 = .1436, BB-NFI = .745, BB-NNFI = .915, CFI = .927, IFI = .929 and RMSEA = .048). This resulted in a questionnaire consisting of 18 items with a two-factor structure that was different from the original. It had a Cronbach’s alpha that was Good, both on the total scale (α = .860) and on two factors: factor 1, or personal (α = .793) and factor 2, or social, (α = .802).
Descriptive analyses
Table 2 shows the descriptive analyses of resilience (CD-RISC), the QLI and the Stoma-QOL after converting the scores of the data into scores out of 100. The data related to resilience obtained in our study sample are low, in comparison to the resilience of the US population (80.7), but somewhat higher than the clinical population (71.8) or that with post-traumatic stress disorder (52.8) (Connor and Davidson, 2003).
Intercorrelations of Pearson correlation, means, standard deviations on scores above 100 points on the CD-RISC, QLI and Stoma-QOL scales (N = 125).
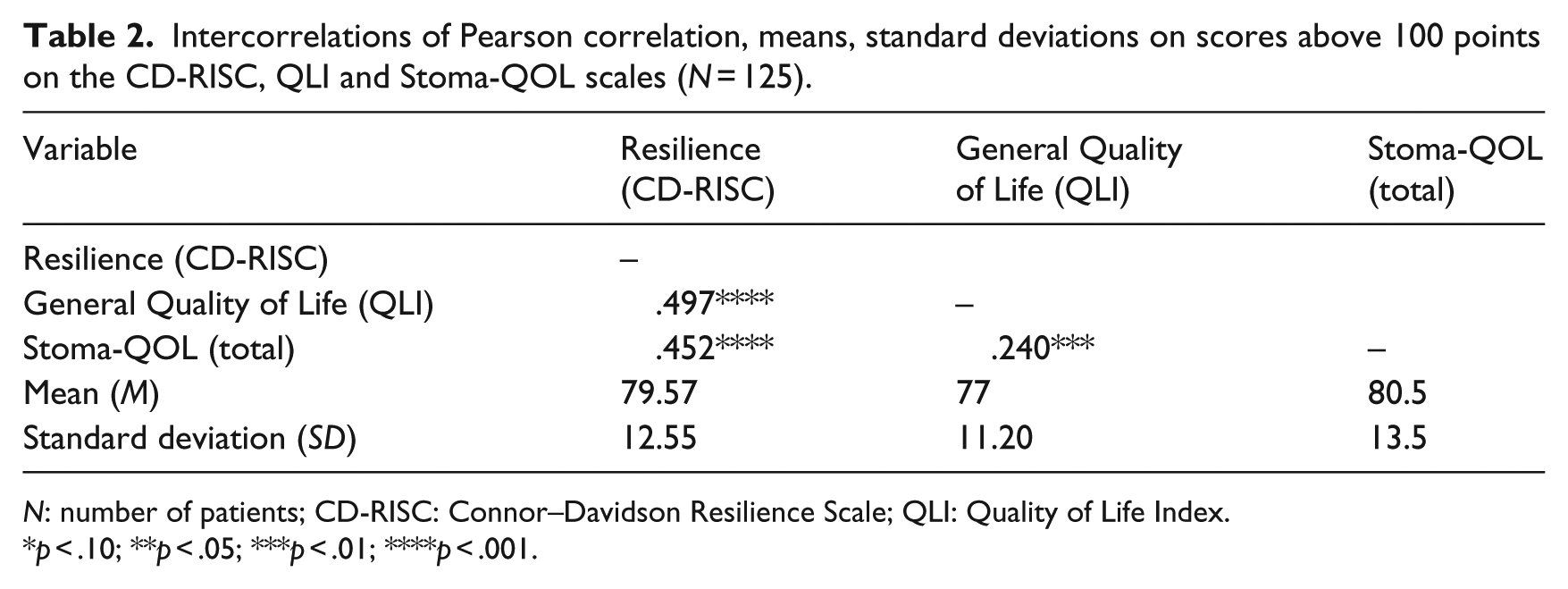
N: number of patients; CD-RISC: Connor–Davidson Resilience Scale; QLI: Quality of Life Index.
p < .10; **p < .05; ***p < .01; ****p < .001.
The authors of the instrument QLI do not propose any cut-off point, but we can see that the perception of QL presented by the mean of our sample is high. As regards the Stoma-QOL, the level of QL perceived by the patients who participated in the study could be classified, according to the criterion of the authors, as Good (result of 70%–100%) (Juul and Prieto, 2008).
In Table 2, we can also see the values of the Pearson correlation among the factors from the CD-RISC, QLI and Stoma-QOL scales. As expected, the results of the Pearson correlation show that there is a significant positive correlation between resilience and both general QL and HRQL.
Relationship between the sociodemographic and clinical variables and the general and specific QL (HRQL)
We then inquired into the existence of significant differences in the level of perception of the general QL, specific HRQL and resilience, depending on the different sociodemographic variables (i.e. gender, marital status, education, labour activity and income), as well as the clinical variables (i.e. diagnosis, type of ostomy, whether it was temporary or permanent, irrigations, complications and care autonomy).
As can be observed in Tables 3 and 4, with regard to the sociodemographic variables, significant differences were only obtained in the cases of children and income. For children, significant differences were seen in specific QL for health and in resilience (p = .001; Mann–Whitney U test, in both cases). Patients with children presented better scores on HRQL (Stoma-QOL
Parametric and non-parametric tests: Student’s t-test for independent samples QLI.
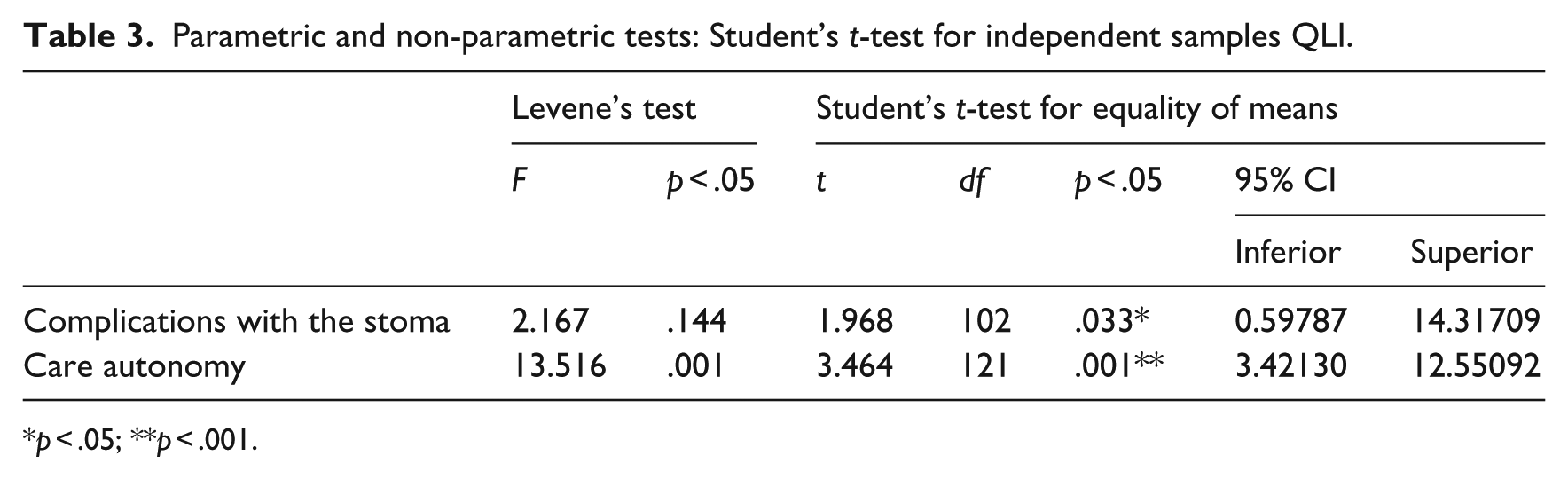
p < .05; **p < .001.
Non-parametric tests for independent samples: Stoma-QOL and CD-RISC.
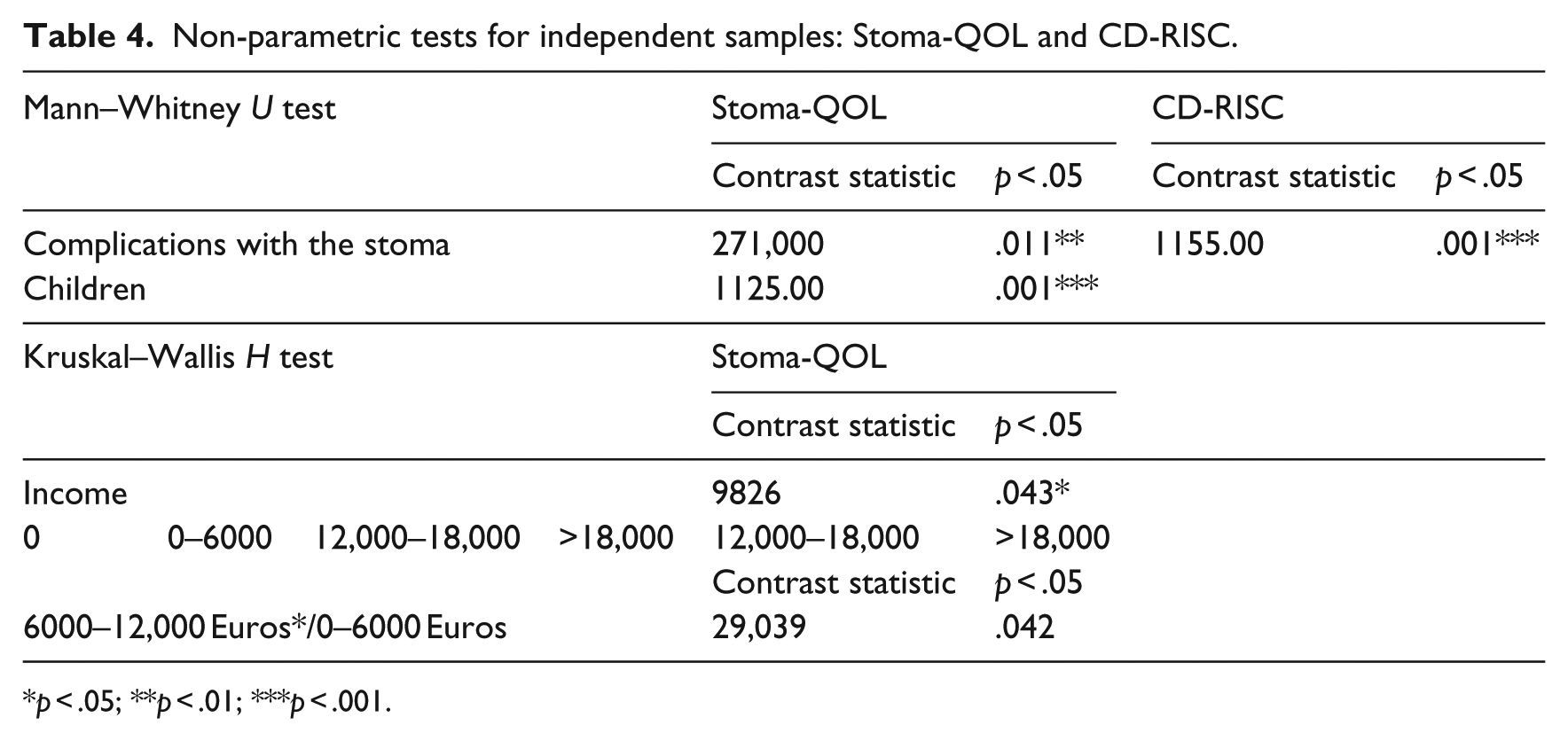
p < .05; **p < .01; ***p < .001.
With regard to income, significant difference were obtained on HRQL (p = .004, Kruskal–Wallis H test) between patients with a level of income of 0 to 6000 Euros per year and those in the group with an annual income of between 6000 and 12,000 Euros. The group of patients that earned from 0 to 6000 Euros per year presented a higher mean score (Stoma-QOL
Of the clinical variables, we obtained significant differences with the variables stoma complications and care autonomy. In the case of stoma complications, we observed that there were significant differences in the general QL (QLI) according to the independent samples t-test (tdf = 1.968, p = .05) and in the HRQL (Stoma-QOL) (p = .011; Mann–Whitney U test). Patients without any complications (QLI
With the variable care autonomy, the result of the Independent samples t-test showed that there were significant differences in general QL (QLI) (tdf = 2.651, p = .001). Autonomous patients (QLI
Multiple linear regression analysis to predict the perception of QL
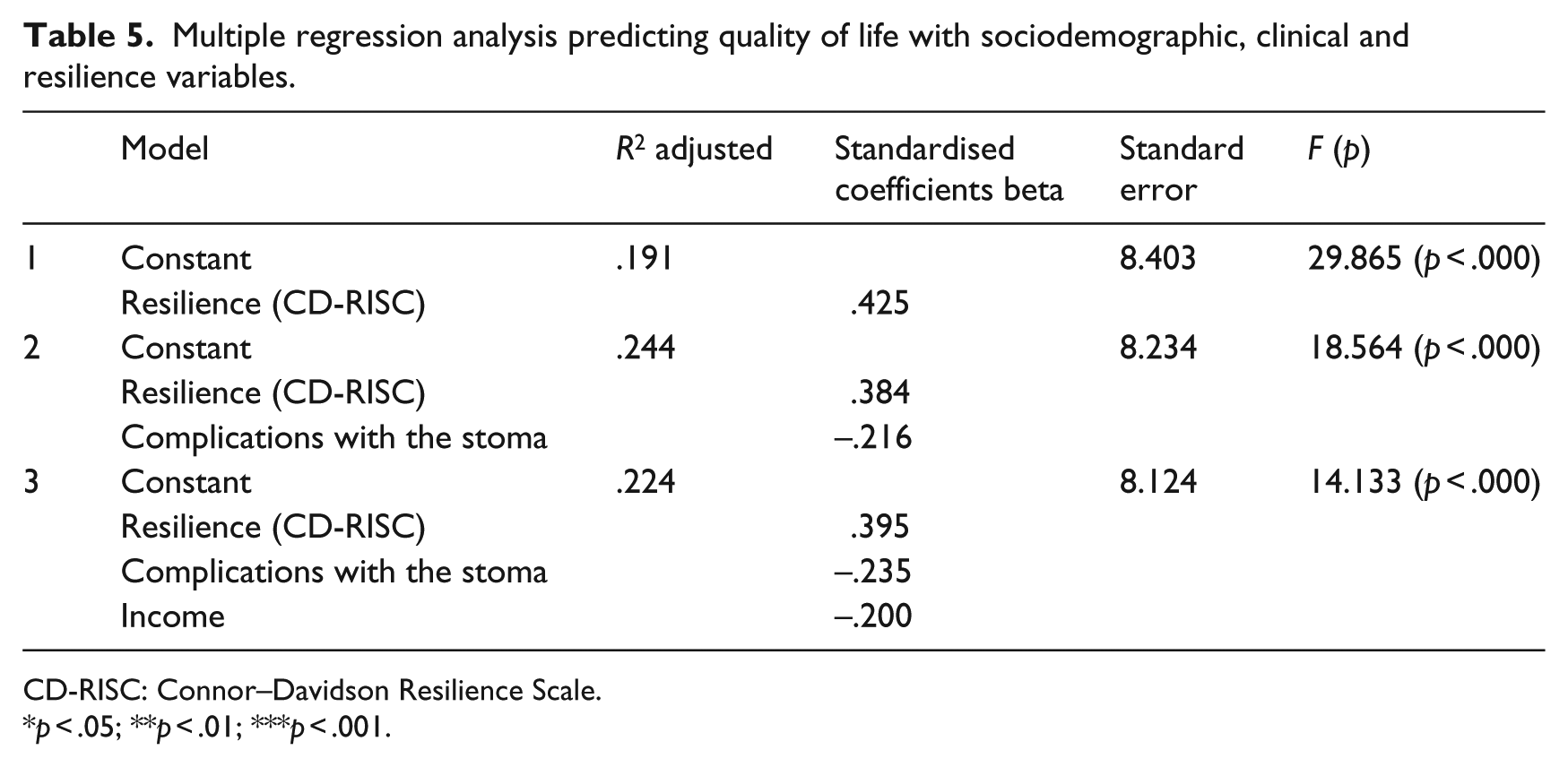
When performing the multiple linear regression, following the stepwise method, a significant regression equation was obtained in which the predictive variables were resilience and the presence of stoma-related complications. Hence, the higher resilience (main predicting factor) and the lower the percentage of complications (second predictive factor), the higher the overall score on specific HRQL will be in patients who have undergone an enterostomy. This regression model predicts a variance of 24.4 per cent with both variables (see Table 5). According to the criterion proposed by Cohen (1988), in one-factor ANOVA models, this factor would have to account for at least 10 per cent of the variance of the dependent variable for the factor for it to be considered as having clinical relevance; a value of around .25 (25% of the explained variance) would indicate a high or clinically very relevant magnitude. Given these indications, we can say that our regression model has very high clinical relevance in explaining the HRQL of patients who have undergone an enterostomy.
Multiple regression analysis predicting quality of life with sociodemographic, clinical and resilience variables.
CD-RISC: Connor–Davidson Resilience Scale.
p < .05; **p < .01; ***p < .001.
Discussion
On analysing the sociodemographic characteristics of the sample, we can see that they are similar to those of other studies conducted with patients who have had an ostomy (Campillo and Zaragoza, 2014; Cancio López et al., 2014; Erlen et al., 2011; Lin et al., 2009; Mahjoubi et al., 2012; Marquis et al., 2003; Pittman et al., 2008, 2009). In our sample, we found that patients are mostly males (64%) with a mean age of 66.72 years, which is consistent with the most important studies that have been conducted recently in our community health setting (Campillo and Zaragoza, 2014; Cancio López et al., 2014), and coincides with the latest figures on the prevalence of colon cancer published by the Spanish Society of Medical Oncology (Ferlay et al., 2013).
This allows us determine the typical profile of the patients in our sample: ‘Male patient between 65 and 75 years, diagnosed with colon cancer and with a permanent colostomy, married, retired, with primary education, and autonomous in the care of his stoma’.
With respect to complications, the percentage of patients who do not present any stoma-related complications (83.2%) is very similar to those of other studies conducted with ostomised patients, in which the percentage of patients who do not report any complications stands at around 80 (Cancio López et al., 2014; Liao and Qin, 2014). The patient’s autonomy in terms of changing the device and stoma care is also important. In this regard, 79.8 per cent of the patients in our study are autonomous when it comes to care, a figure that is higher than those obtained in similar studies conducted with Spanish populations, such as the Stoma Life study by Campillo in 2014 and the cost-effectiveness study of the Antae Institute carried out by Cancio López et al., also in 2014; in both cases, the autonomous patients were 75 per cent.
On analysing the relation between resilience and both general and specific HRQL, we find that there is a positive relationship with general QL, a result that is in agreement with many studies that provide scientific evidence showing that resilience predicts a lower level of distress, better adjustment, better QL and better levels of self-care in patients with a chronic disease (Bowen et al., 2003; Costanzo et al., 2009; Haase et al., 2014; Liu et al., 2012; Molina et al., 2014; Ong et al., 2009; Rowland and Baker, 2005; Strauss et al., 2007; Wu et al., 2015). In line with this, the results of our study also indicate that resilience is related to the specific level of QL in patients with a drainage enterostomy. These results suggest that people with a high level of resilience have a greater ability to grow in situations such as chronic illness, which probably allows them to adapt successfully to their new situation (Amar et al., 2013; Ho et al., 2010; Johnston et al., 2015; Lam et al., 2010; Luthar et al., 2000; Molina et al., 2014; Quiceno and Vinaccia, 2011; Wu et al., 2015).
On testing for significant differences according to the sociodemographic and clinical variables in QL, HRQL and resilience, differences were only obtained in the variables children, income, stoma-related complications and being autonomous with regard to care. Significant differences were obtained with respect to the variable children, patients with children being those that presented better scores on HRQL and resilience. This could be accounted for by the fact that they had greater social support than patients without children (Luo et al., 2014). In the variable income, significant differences were observed between patients with income levels of 0–6000 Euros per year and those in the group that earned between 6000 and 12,000 Euros, those in the first group being the ones with better QL indices. This is a result that somewhat contradicts those of previous studies with ostomised patients, as the positive correlation obtained between income and QL was so clear that they concluded that interventions have to be geared towards helping to cover the costs arising from having an enterostomy (Krouse, et al., 2009; Maydick, 2014; Sun et al., 2014). One plausible reason explaining why the results of our study do not run in the same line as others is that in our setting the public health service bears all the costs deriving from this condition and a recent study conducted on a Chinese population found that patients whose income has been modified as a consequence of the illness that led them to have an ostomy are the ones who report significantly poorer QL (Li et al., 2012) Perhaps, it would have been necessary to take into account whether the process and the condition of undergoing an enterostomy had given rise to a change in income in order to better understand this result.
With regard to the clinical variables, significant differences were only found in the variables complications and autonomous care, which we will go on to discuss in the following. With the clinical variable of presence or absence of complications, a significant deterioration of HRQL was seen in patients who present stoma-related complications. These results coincide with those from other studies (Campillo and Zaragoza, 2014; Cancio López et al., 2014; Lin et al., 2009; Simmons et al., 2007) that also find a significant relationship with the presence of complications and a lower level of adjustment to the self-care agency. All this seems logical in view of the discomfort resulting from the different complications, while a decline in the level of self-care also has an influence on vulnerability to suffering more complications.
As regards the variable care autonomy, it was found that patients who are autonomous in their stoma care display better general QL indices. This can be explained by the fact that the disease process and the subsequent ostomy is a devastating event, mainly due to all the changes involved in losing the functioning of the sphincter on being replaced by the drainage enterostomy. This entails the need to change daily life routines together with special care of both the stoma and all the material that must be used. As a result, patients who are autonomous with regard to their stoma care display a better adjustment to the chronic illness in a number of aspects, such as having a more proactive attitude and improving their self-care agency and their perception of QL (Marina and Angarita, 2014; Stephenson et al., 2013). Many authors, therefore, claim that it is essential to educate patients in the proper management of their ostomy with the aim of their becoming autonomous in caring for it (Di Gesaro, 2012; Ferlay et al., 2013; O’Connor, 2005; Williams, 2012).
Finally, as regards the model that best predicts the perception of HRQL, the first is the variable resilience, followed by stoma-related complications and finally income. We have already discussed the fact that both the variables stoma-related complications and income are important factors in the process of adjusting to the illness. As shown in this model, resilience is one of the variables that correlate with HRQL. Hence, and regarding the relationship between resilience and health indicators, many studies provide scientific evidence showing that resilience predicts a lower level of distress, better adjustment, better QL and higher levels of self-care in patients with a chronic illness (Bowen et al., 2003; Costanzo et al., 2009; Haase et al., 2014; Liu et al., 2012; Molina et al., 2014; Ong et al., 2009; Rowland and Baker, 2005; Strauss et al., 2007; Wu et al., 2015). In line with this and as noted above, the results of our study also show that resilience is related to the specific level of QL in patients with a drainage enterostomy. This would explain why people with a high level of resilience display the capacity to grow in the face of adversity, as is the case of suffering from a chronic illness, which leads them to a successful adaptation to their new situation (Amar et al., 2013; Ho et al., 2010; Johnston et al., 2015; Lam et al., 2010; Luthar et al., 2000; Molina et al., 2014; Quiceno and Vinaccia, 2011; Wu et al., 2015). Resilience is, therefore, a mechanism that protects against disease-related processes that negatively affect physical and psychological health (Connor and Davidson, 2003) by improving people’s psychological status (Lü et al., 2014). The results of this study and previous research show that resilience can be a key factor in adjusting to stressing situations and thus to chronic (Shi et al., 2015).
Limitations of the study
Among the limitations of the research, it is necessary to mention that, although the methodology allows the main objectives to be reached, the number of patients included in the research is smaller than was initially estimated. The main reason for this was the low number of ostomised patients who met the inclusion criteria. Some patients complained about the duration of the personal interviews and others felt uncomfortable when dealing with intimate aspects related to their sexuality or hygiene related to the stoma and their intestinal eliminations. Additional studies should be performed with larger samples in order to generalise the results to ostomised patients as a whole.
Practical implications
Finally, as a general conclusion from our study, we can say that in ostomised patients, resilience plays an important role as a predictor of variables of adjustment to the disease, such as HRQL, together with clinical variables, such as stoma-related complications. It is necessary to design multidisciplinary intervention programmes, based on scientific evidence, which contain knowledge and practices to promote the resilience process together with measures to prevent possible complications. This would allow better adjustment to the disease and a higher HRQL.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.