
Abstract
Issues concerning competence of practicing psychologists have not been critically investigated in Ghana. This study used the three-dimensional cube model of core competencies as a framework to explore competencies of professional psychologists in active clinical health practice in Ghana. Sixteen clinical psychologists with 1 to 20 years of practicing experience were interviewed on adequacy of their graduate training for practice as well as maintaining post-training competence. The results suggested that training equipped the practitioners mainly for research and teaching but less so for clinical practice. Reflective practice was underdeveloped leading to critical challenges in emotional and cultural competencies. Structural support for continuous professional development was limited. Implications for professional psychology training, research and practice are discussed. This study is the first to explore competence issues in professional psychology practice in Ghana, and it contributes to the global discourse on continuous competence in psychology.
Competence is a key issue in contemporary professional psychology training and practice (Hilton and Johnston, 2017; Nelson, 2007; Rodolfa et al., 2013, 2014). It goes beyond mere completion of academic or training programmes to the assessment of one’s demonstrable skills, attitudes, abilities and practices across the career span. Competency involves ensuring that educational programmes produce competent graduates and that only competent professionals become licenced (Fouad et al., 2009). It further involves assurance that clients receive professional psychological services from competent practitioners (Forrest, 2010).
Professional incompetence may be exhibited when individuals lack adequate training, education or experiences; are unable or unwilling to acquire professional standards and integrate them into professional behaviours; fail to respond to feedback; and do not continuously grow or make specific progress (Fouad et al., 2009; Rodolfa et al., 2013). Individuals who lack self-awareness and exhibit prejudicial attitudes, lack high levels of integrity and face personal problems, emotional reactions or distress as a result of substance abuse, mental health difficulties, personality disorders and cognitive challenges may show poor professional functioning (Bemak et al., 1999). These forms of incompetence can be detrimental to the welfare of clients who use psychological services (Kaslow et al., 2007). It can lead to loss of trust in the field by clients and the general public and to legal action against professional psychologists (Forrest, 2010). There is therefore the need to develop and share best practices for management of these problems at various stages of professional psychology development.
There are several benefits to be gained for assessing competence in professional psychological training and practice. Forrest (2010) states that assessing competence fosters learning for both students and trainers (e.g. educators and supervisors). Feedback from assessment of competence provides trainees the ability to track their progress in their practice over time. Trainers also benefit by evaluating their progress, and they can use the findings from such assessments to contribute to the re-structuring of curriculum and training programmes. Doing so ensures that training programmes produce competent professionals who can meet the growing demands for competent professionals by consumers seeking psychological services (Hilton and Johnston, 2017; Kaslow, 2004). Ultimately, studies on competence in professional psychology training and practice can be used to advance the field of psychology as it helps protect the public from incompetent professionals.
There is an established body of work on competence in professional psychology in North America and Europe. We have limited knowledge of the context of competence for practicing psychologists in African settings. In Ghana, there have been no systematic attempts to evaluate the training programmes that produce professional psychologists. Recent overviews of the history and context of psychology in Ghana have offered preliminary evidence on the scope and challenges of building capacity in psychology teaching, research and practice (de-Graft Aikins, 2018; de-Graft Aikins et al., 2014; Oppong Asante and Oppong, 2012; Oppong et al., 2014). Two studies have examined cultural challenges faced by Ghanaian psychotherapists trained outside Africa (Owusu-Ansah and Donnir, 2016) and on ethical dilemmas faced by clinical psychologists (Oppong, 2014). Studies that explore competency issues in Ghana are needed to provide information on what psychologists are doing in their professional capacities and also to address some of the questions and misconceptions the general public have about the profession.
The aim of this study was to examine issues of competence in education and practice as experienced by psychologists in clinical settings in Ghana. We explored two research questions: (1) To what extent does training received by professional psychologists equip them to be functionally and foundationally competent for clinical work in Ghana? and (2) How do practicing psychologists in Ghana maintain competence post graduate training?
Professional psychology training in Ghana
Psychology, as a discipline and profession, has a young but dynamic history in Ghana. Before the teaching of psychology at the university level in 1963, some professionals, in the fields of education and medicine, applied psychological knowledge to their practice (Danquah, 1987; de-Graft Aikins, 2018). Since 1967, when psychology was established as an independent academic discipline at the University of Ghana, psychology has evolved steadily as a professional discipline (de-Graft Aikins et al., 2014; Oppong Asante and Oppong, 2012). Currently, major psychology sub-fields in Ghana include industrial, clinical, social, developmental, educational, community, health and counselling. Psychology is taught at undergraduate level at the University of Ghana and at three other public and two private universities (de-Graft Aikins, 2018; de-Graft Aikins et al., 2014; Oppong et al., 2014). It is a popular undergraduate major at the University of Ghana, with the discipline alone taking just over 10 per cent of the total student population annually in recent years (Mate-Kole, 2013). In private universities, psychology is offered as a standalone course as well as an adjunct course to degrees such as business (Oppong et al., 2014).
Professional training in psychology begins at the postgraduate level. Graduate-level training, however, does not reflect the national undergraduate trends. University of Ghana offers graduate training at the masters’ and doctoral levels. Besides the University of Ghana, two other public universities – University of Cape Coast and University of Education, Winneba – offer postgraduate programme in Guidance and Counselling. Two private universities – Methodist University College and Regent University College – offer masters training in Guidance and Counselling and Human Development, respectively.
Professional psychologists (especially clinical psychologists) in Ghana contribute to health service delivery. The Ghana Mental Health Act, Act 846, was introduced in 2012 (de-Graft Aikins, 2018). This Act allowed clinical psychologists to be employed by the Ghana Health Service under the Ministry of Health to provide mental health services to clients in teaching at regional and district hospitals (de-Graft Aikins, 2018). Clinical psychologists hired by both public and private hospitals engage in clinical practices such as assessment, diagnoses and providing psychotherapy. Very limited research has been done to examine how the training the professionals receive equips them for their clinical practice. Three recent reviews of the history of professional psychology in Ghana highlighted the challenge of low numbers of practicing psychologists and the lack of culturally appropriate models of practice (de-Graft Aikins, 2018; de-Graft Aikins et al., 2014; Oppong et al., 2014).
Issues of professional competence in psychology have not received much attention in Ghana. Oppong (2014) investigated ethical dilemmas experienced by twenty clinical psychologists in Ghana. The research participants shared a number of dilemmas related to competence such as lack of training opportunities and cultural competence. They were concerned about their lack of in-depth knowledge and skills in handling difficult clinical cases. The lack of continuous training was perceived as a significant impediment for competence. For example, Oppong’s (2014) study participants reported that their training was biased towards the application of western theories and instruments, which were culturally insensitive and affected competence in practice. The professionals also noted that the lack of a culturally specific code of ethics for Ghanaian psychologists further undermined the integrity of their practice. Owusu-Ansah and Donnir (2016) presented case studies that emphasised some of the challenges faced by Ghanaian psychotherapists practicing in Ghana. The studies revealed that psychologists who receive training in European and North American cultural contexts were challenged when clients used spiritual beliefs to explain their illness experience. Spiritual causal theories of chronic physical and mental illness have been associated with healer shopping from traditional healers, pastors and traditional shrine priests (de-Graft Aikins, 2005, 2015; Opare-Henaku and Utsey, 2017). Psychotherapists whose training excluded the cultural nuances of illness attributions and practices in Ghanaian and African contexts had difficulty in providing culturally appropriate client-centred care.
The limited number of studies suggests that practicing psychologists in Ghana (whether trained in or outside Ghana) face different challenges that can influence competence and practice. The lack of information on professional psychological practice in Ghana hampers effective training, research and practice. It also excludes the Ghanaian experience from the important global discourse on professional competence in psychology. As a profession that is steadily gaining legitimation in Ghanaian society, it is imperative to investigate whether professional training and skills acquired by professional psychologists make them competent to provide needed services to clients. This study addresses the gap in the literature by exploring the impact of training on competencies among practicing psychologists. The study also seeks to illuminate the problems professional psychologists face in delivering their services in different Ghanaian settings. Findings can be useful for training institutions, the Ghana Psychology Council (the body responsible for licencing professional practice of psychologists in Ghana) and the Ghana Psychological Association. Furthermore, the study will contribute to the global discourse on competencies in professional psychology.
Cube model of competency: a conceptual framework
The study was guided by the three-dimensional cube model of core competencies developed by Rodolfa et al. (2005). Rodolfa and colleagues conceptualise competency as having knowledge or skills in a field and also being qualified, capable and able to understand and take action in an appropriate and effective manner. As Epstein and Hundert (2002) note, competence is the ‘habitual and judicious use of communication, knowledge, technical skills, clinical reasoning, emotions, values and reflection in everyday practice for the benefit of the individual and community being served’ (p.226). Competencies integrate different elements, including discrete knowledge, skills and attitudes; certain domains of competency are emphasised to reflect the integrated knowledge, skills and attitude that are used in the professional practice of psychology (Kaslow, 2004).
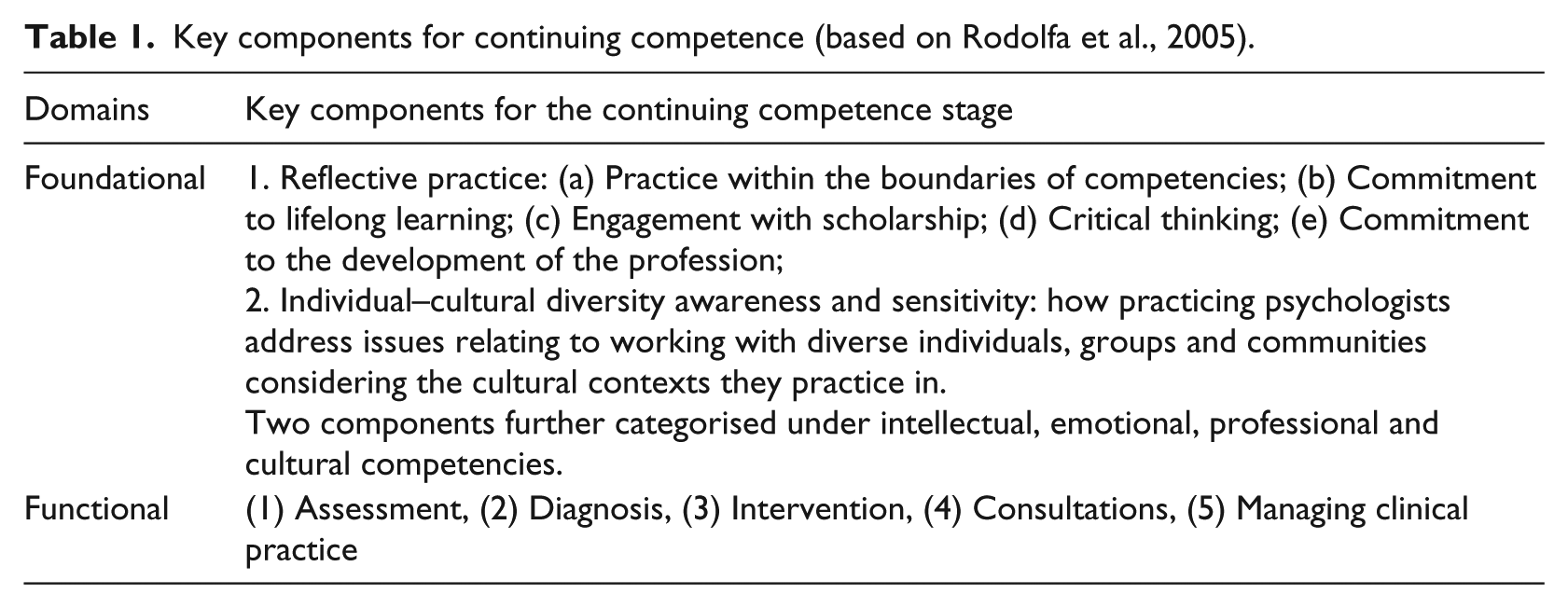
Rodolfa et al. (2005) describe competency development in professional psychology by providing two domains of professional competency: foundational and functional competency. The foundational competency domains conceptualise what professional psychologists do, including reflective practice–self-assessment, scientific knowledge–methods, relationships, ethical–legal standards–policy, individual–cultural diversity and interdisciplinary systems. These domains of competency prepare professionals for acquiring functional competency. Functional competency focuses on the skills and knowledge, which are vital in performing one’s role as a psychologist. It includes assessment and diagnoses of cases, intervention, consultation, research–evaluation, supervision and teaching, and management and administration. These characterise the everyday function of professional psychologists. The model is useful across the stages of professional development, including doctoral education, postdoctoral training and continuing competency. For the purpose of this study, we focused on the stage of continuing competency since the participants in the study were practicing psychologists who had completed their graduate training. Furthermore, we synthesised ideas from Rodolfa et al. (2005), Fouad et al. (2009) and Pope and Vasquez (2007), and thematised foundational competency under four areas: intellectual, emotional, professional and cultural competencies. Table 1 presents a summary of the two domains as well as the key components assessed in this study.
Key components for continuing competence (based on Rodolfa et al., 2005).
Methods
The study was conducted as part of a 2016 course project in an MPhil Clinical Psychology Ethics class at the University of Ghana. In addition to examining the aims of the study outlined earlier, the overarching objective of this course project was to build students’ capacity in developing, conducting, analysing and reporting on issues pertaining to professional ethics and competence in clinical practice in Ghana.
Research design
The study was conducted using qualitative methodology. Qualitative methodology offers the opportunity for deep and nuanced exploration of issues under investigation, especially when target issues are underexplored (Brannen, 2005; Denzin and Lincoln, 2011).
We used individual semi-structured interviews, as we were interested in individual professional experiences. The interview format facilitates one-on-one interaction and the nuanced examination of subjective issues. This approach therefore allowed participants the opportunity to present and explain their professional experience and management of competent practice at length, in their own way and in private.
The interview guide
The semi-structured interview guide was informed by Rodolfa et al.’s (2005) model, as described in the previous section and summarised in Table 1.
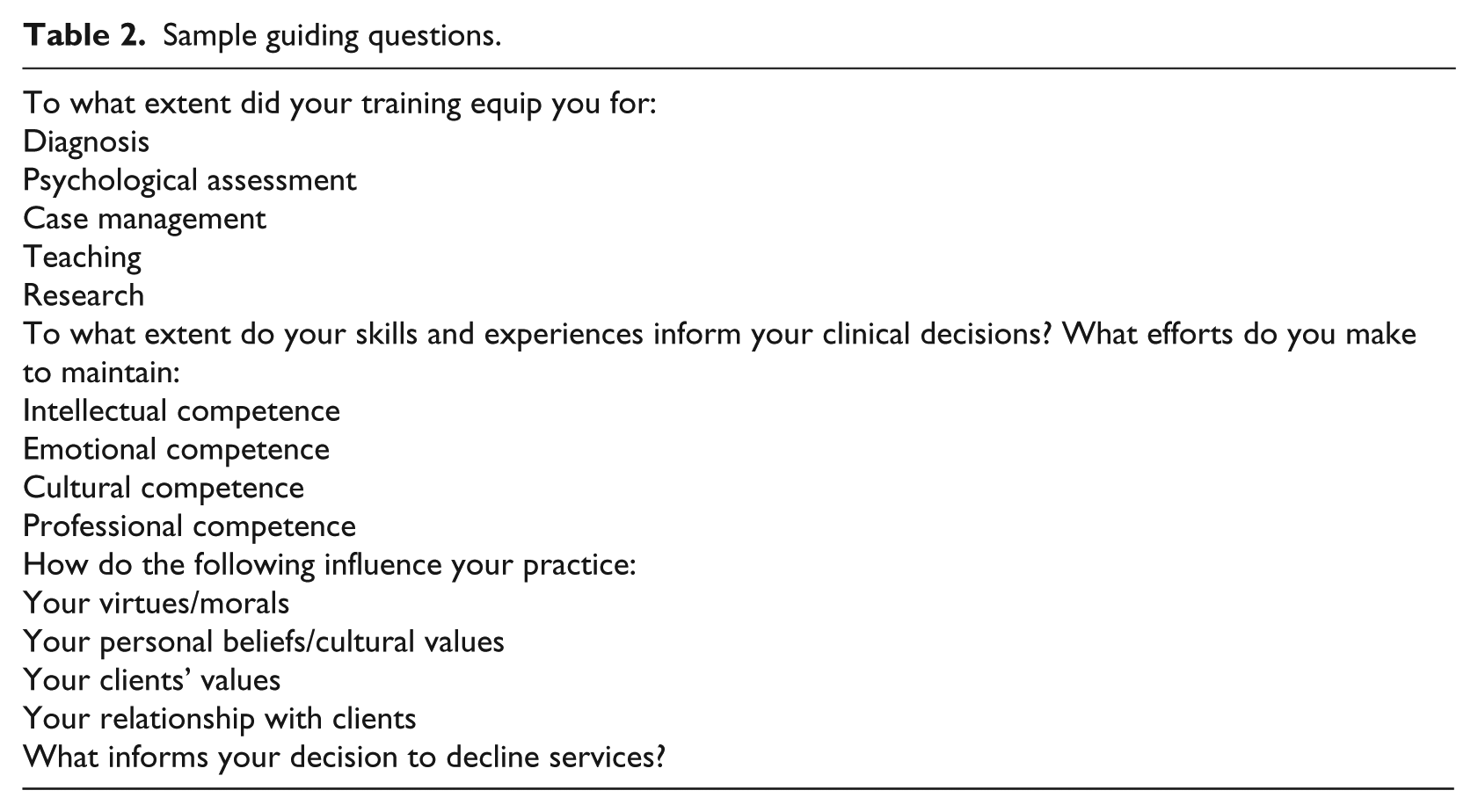
The guide covered three main domains: (1) stages of professional development, (2) foundational competency and (3) functional competency. The professional development domain focused on continuing competency of the practicing psychologists after graduate training. The foundational competency domain focused on the two key areas outlined in Table 1: reflective practice and individual–cultural diversity awareness and sensitivity. Here we explored four competencies – intellectual, emotional, professional and cultural. The functional competency domain assessed issues relating to assessment, diagnosis, intervention, consultations and managing clinical practice. Table 2 contains sample questions covered in the interview guide.
Sample guiding questions.
Participants
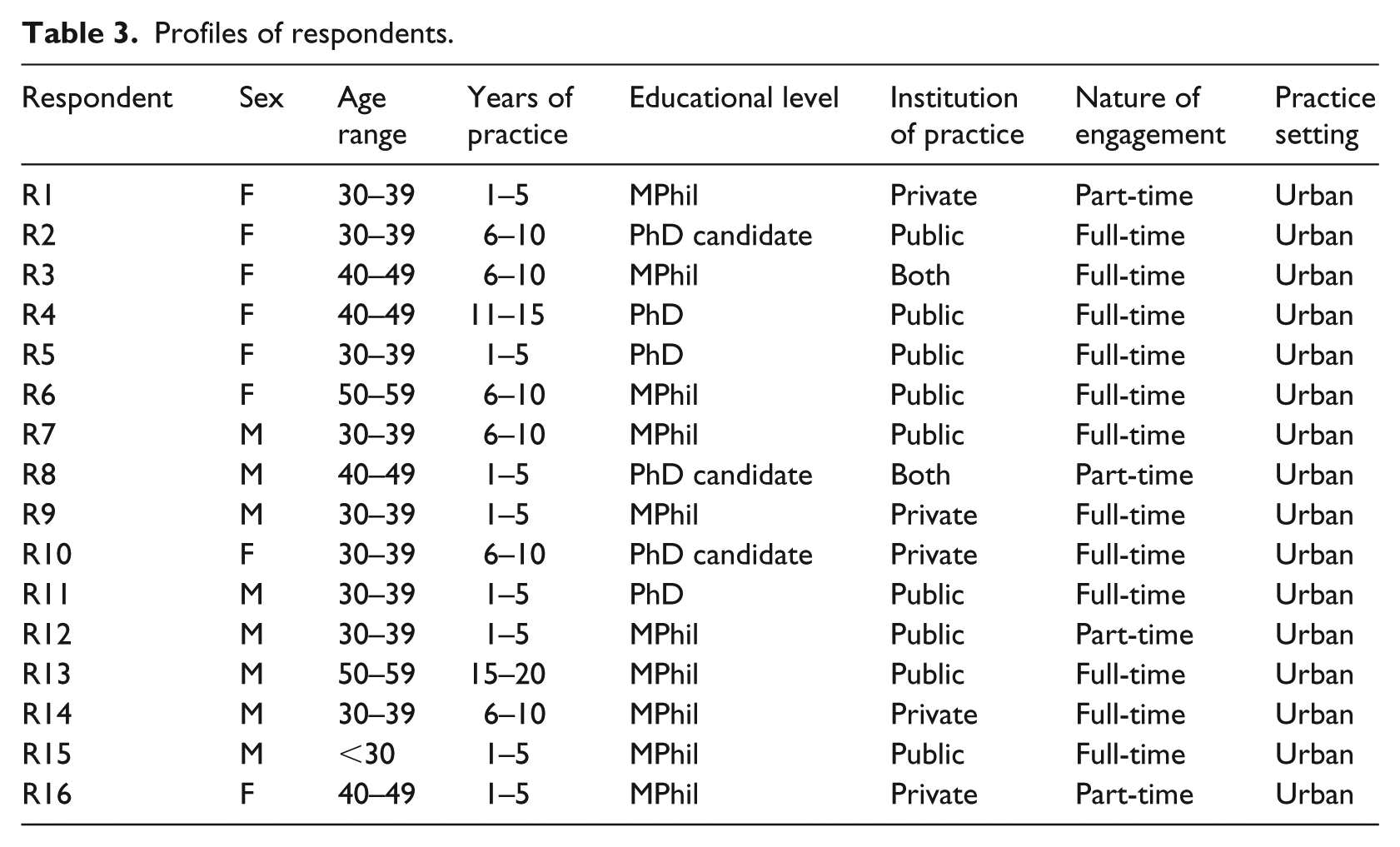
Participants were practicing psychologists who provide psychotherapy services in health settings in Ghana. They had been in active clinical practice for at least one year in Ghana. Sixteen practitioners were conveniently selected and interviewed. Table 2 shows the socio-demographic characteristics of the practitioners who took part in the study. There were equal numbers of male and female respondents. The respondents were aged between 29 and 69 years, with the majority within the 30- to 39-year age range. Years of practice ranged between 1 and 20 years: almost half of the respondents had been practicing between 1 and 5 years, six respondents had practised between 6 and 10 years. Majority of the respondents (11) had master’s degrees. Two participants had a doctorate degree and three others were pursuing their doctoral studies at the time of the study.
Almost half (n = 7) of the practitioners practised in only public institutions, three practised in only private institutions and six practised in both public and private institutions. All the practitioners practised in urban areas. Majority of the practitioners (n = 12) were practicing full-time and four practised on part-time basis. All the 16 participants were clinical psychologists but some indicating additional training in other sub-fields of psychology such as counselling (1), neuropsychology (1), sports psychology (1) and psychometrics (1). In terms of theoretical orientation, majority of the practitioners (n = 12) stated that they used cognitive-behavioural therapy (CBT), one practitioner described himself as a ‘learning theorist’ and the remaining three drew on eclectic approaches.
Process and ethical consideration
All the interviews were conducted at a location of choosing by the practitioners and interviews lasted between 30 and 60 minutes. Interviews were conducted in the English Language and were audiotaped with respondents’ permission. Ethical approval of the study was obtained from the ethical review board of the College of Humanities, University of Ghana, under an existing project by the second author. The study aims were explained to respondents before written consent was obtained. Interviews were recorded with respondents’ permission.
Data analysis
The interviews were audiotaped and transcribed verbatim, and then the data were analysed using thematic analysis (Attride-Stirling, 2001; Braun and Clarke, 2006). Coding and analysis were done manually and involved reading and initial coding of the 16 transcripts; grouping codes to minor themes and then major themes; grouping into emergent themes.
Coding was done deductively and inductively. Deductive codes were derived from key elements of the three-dimensional cube model of competence (Table 1) and insights from existing Ghanaian studies (Oppong, 2014; Owusu-Ansah and Donnir, 2016). For example, existing Ghanaian studies highlighted the following challenges to professional competence: lack of in-depth knowledge, clinical skills, continuous training and culturally specific instruments and code of ethics for Ghanaian psychologists.
Inductive codes were identified after an exhaustive list of deductive codes had been identified: these referred to new ideas and narratives on competence emerging from the specific contexts of the study interviews. For example, struggles with faith and professional expectations. The coding frame was developed through an iterative process of individual and sub-group coding and multiple team discussions.
The second stage of analysis was interpretive and involved developing a synthesis between codes, themes, appropriate quotes, existing empirical data, study objectives and the conceptual framework. At this stage, areas of consensus, conflict or absence across respondent narratives were identified.
The analysis was conducted by all researchers. Coding was done by a group of 10 MPhil students and 2 PhD students, under the supervision of the first and second authors. A five-stage iterative analysis process developed for this study is presented in Appendix 1. This context-specific approach was developed to train the MPhil students who were new to qualitative research and analysis.
Findings
The results section provides a description of the practitioners’ perspectives regarding their training and practice on the functional competency and foundational competency, and under each theme, supporting quotes are presented. Respondents are identified by respondents’ numbers (R1–R16), as shown in Table 3.
Profiles of respondents.
Functional competency
Functional competency focused on training adequacy in diagnosis, assessment, clinical decision making, case management, research and teaching.
Evaluation of training adequacy for diagnosis
The practitioners’ assessment of their competence for diagnosis was mixed: while a little over half (n = 9) indicated that the training was adequate, others (n = 7) said that their training was not adequate. The latter group judged that their training only partially equipped them for competent diagnosis.
… the training in terms of diagnosis was very extensive. It has equipped me very well to be able to do some diagnosis. [R1] As for the training, I will say not really because when you start practice, you find that you struggle with diagnosis in the early stages. It is after you have practice for a while that you become good at it. [R13] I will say my training gave me the skills [that] are needed to start but I will say uhm ah I don’t know whether to say not enough. [R12]
Evaluation of training adequacy for assessment
Some of the practitioners (n = 6) stated that the training equipped them for assessment. In the illustrative quote below, respondents stated that training was enough. One respondent expressed similar views on diagnosis and assessment.
For diagnosing mental disorders I think to a large extent, I mean the training is good or has been very good. [R5] Well, yes I will say it was enough because you have to eh engage in your practicum for virtually one year covering about 600 credit hours, supervised, aha, so … that will make you competent enough to be able to handle patients even on your own. [R7]
However, more than half of the practitioners (n = 9) evaluated their competency for assessment as ‘limited’ [R9].
Assessment was most limited; there are a lot of assessments tools that we never saw. We only heard about them. [R9] I think it’s ok but it depends on you personally because I learnt some of the assessment during the course of practices and not during training because the training was more of academic focus so in terms of training in assessment more has to do with the practice. [R15]
Evaluation of skills adequacy for clinical decisions
Five respondents indicated that the skills acquired during training informed their clinical decisions.
… the skills you acquire from training is a lot for you to be able to understand patients well, be able to diagnose, formulate your treatment approach and be able to effectively treat patients. [R7] Yea, mostly I fall on my skills what I have leant over the years and how I handled issues over the years I fall on that in most of the cases is only a few situation that maybe some of the cases are spontaneous but to the large extend. [R15]
Ten respondents indicated that their clinical decision making depended on their skills as well as other evolving factors, including client and situational dynamics.
It still depends on other factors, for instance the client or the condition. Even sometimes it depends on you the practitioner. So the skills alone mostly are not enough. You have to take other factors into consideration. [R11] Hmm … sometimes, for example you are given a case that has to do with a couple and you can clearly tell that one person is wrong but it becomes very difficult for you to decide how best to handle it. So sometimes even your skills are not able to help [R3]
Evaluation of training adequacy for case management
The majority of respondents (n = 13) evaluated their training for case management positively.
I think that the practicum really helped in the case management because when you have sessions with your clinical supervisor we have case presentations how you go about cases I think it helps. It prepares you to handle or manage cases that can even be weird. [R13] Yeah … I will say the training helps you to manage cases very effectively. [R5]
However, three respondents believed that their training did not equip them adequately when it comes to case management.
It was also not adequate because there are times that we needed questions to what you are looking at but we don’t get it immediately it will take you days and sometimes weeks to get someone to help you understand and manage a case. [R9] … so for the training, well, I will say that it did equip us to some degree because it gave us the basis but there are still more to be added so we can manage cases well. [R12]
Evaluation of training adequacy for research
The majority of respondents (n = 14) stated that they received adequate training for research.
Yes, the research was also an integral part of my training [ok] in which you have to pass eheheh research thesis [yes] aha before you will be able to graduate, apart from that you have several assignments based on research which you have to complete. [R7] Yes, when it comes to research, I think I got above average skills to do research. [R9]
Evaluation of training adequacy for teaching
For more than half of the practitioners (n = 10), their training equipped them for teaching.
In fact the training has broadened my knowledge in the subject area, so I can confidently teach the subject even at the university level. [R11] I will say to some extent because since the model that we use is a scientist practitioner model so it helps you to practice, teach and research. [R15]
However, four practitioners stated that their teaching skills were not developed during their clinical training but rather from non-clinical activities, such as being a graduate assistant.
… not specifically but we helped to teach, those of us who have had the opportunity to be taken on as eh graduate assistants, we had the opportunity to teach students several subjects. [R7]
Foundational competency
Four areas of foundational competency were explored: intellectual, emotional, cultural and professional. We also explored challenges faced by the practitioners.
Intellectual competence
Respondents indicated that they maintained competence mainly through attendance of conferences and seminars (n = 13), consultation (n = 11), reading articles and journals (n = 11), short courses (n = 9) and further advanced education (n = 4).
Anytime I get to know that there is a conference or a seminar on psychology I try to attend to update my knowledge. [R7] I also consult experienced and senior psychologists, both in Ghana and abroad for guidance and advice. [R11] I read a lot of articles on specific things so for instance if I have a case of premature ejaculation I try to use an article that was or maybe a case study that was used to treat it. [R9] … currently I am even upgrading myself, so I am doing my doctorate degree in the field. [R12]
Emotional competence
Practitioners used emotional detachment (n = 9), humour (n = 8), consultation (n = 8) and self-understanding (n = 6) to maintain emotional competence in their practice.
… it’s my job why should I be affected by it, I have gone past that, sometimes its touching, imagine if you are crying and they are also crying it doesn’t make sense. [R5] … I also have people who are in the field who I talk to so I find a way to also … you know … an outlet sort of to … sometimes let out some of my own challenges. I’ve made the effort to speak to another person who can help me deal with my issues before I try to get in there. [R1] I also make sure that or try to understand myself as a person as a human being … in yes understanding my emotions so that they don’t impair or get in the way in my treatment of clients. [R7] Well, for myself I am a person an individual who sees humour in a lot of things, I don’t take life too seriously. [R4]
Professional competence
This was maintained through professional membership (n = 14); engaging in ethical practice (n = 5) and consultation (n = 5).
I join professional bodies like the Ghana Psychological Association to ensure I always have information concerning practice in Ghana. [R10] There are ethical standards that guide our practice so I work according to those standards because for me, that is what makes you credible. [R1] As I said earlier that when I need help, I fall on them. If I think it is within my colleagues capacity, I just call on them. I call anybody at all. [R3]
Cultural competence
Practitioners mainly mentioned having cultural knowledge (n = 14) on family and social life and understanding differences in religious values.
I am always conscious of the cultural differences, people’s perspective of things so I do not judge them wrongly when they are undertaking or they are behaving in specific ways because of their culture. [R7] I know Ghana that some places that they practice polygamy so I will want to be sure whether he is practicing polygamy so that I will know the line to tow if am in session instead of condemning. [R9] … religion is one area that you are expected not to be brought into therapy. So I never initiate religion or initiate a religious discourse. [R4]
Challenges
Respondents indicated several challenges they faced in their practice, including conflicting religious values (between clients and psychologists), interference from religious authorities, financial and emotional stress, lack of clarity regarding the role(s) of psychologists and limited facilities and resources like consulting rooms and assessment tools. The practitioners explained that these challenges affected their practice in diverse ways. For instance, conflicting religious values affected judgement and professional decisions in ways that did not address clients’ needs.
I know for a fact that being a Christian affects some of the judgments I do. So it might affect me and I am aware, so I try to take myself away from it. [R12] Then we have interferences and influences from religious, a person’s own personal beliefs and stuff like that … And I have had instances where I think people from other domains try to sabotage. [R5] When you take for instance gayism, me, I am a Christian [yes] and I don’t believe in that you see. So when somebody comes to me and says he is a gay, I know that is abnormal so we have to treat that before we can treat any other problem the person is having. If the person is not willing to deal with his gayism, then he is not ready for help. [R6] … in some instances personal values comes into play for instance if somebody comes to tell you he is cheating on his wife that if he go out to cheat on the wife he doesn’t get erection he gets premature ejaculation but for his wife it is ok, you can’t treat such a person because you know morally it’s not good so you decline. [R15]
Discussion
We used the three-dimensional cube model of core competencies developed by Rodolfa et al. (2005) as a framework to explore competencies of professional psychologists in active practice in Ghana. The results suggested mixed experiences on functional competency relating to diagnosis, assessment, clinical decision making, case management, research and teaching. Training equipped the practitioners for research; moderately for teaching; and less so for clinical practice. Participants reported feeling prepared for case management but less so for clinical decision making. They did not feel their graduate training equipped them for diagnosis and assessment. This finding is similar to Oppong’s (2014) study in which participants expressed concerns about the lack of depth of knowledge and skills in handling selected clinical cases. In order to maintain functional competencies, practitioners drew on self-taught strategies which lay outside formal structures of training and support.
Foundational competency was weak. The majority of practitioners had limited knowledge of the four key areas we examined. To maintain intellectual competence, the practitioners relied mainly on conference attendance; some consulted local experts and journals and a minority pursued short courses and higher degrees. Emotional competence was underdeveloped. Pope and Vasquez (2007) define emotional competence as knowing oneself and include self-knowledge, self-acceptance and self-monitoring as part of the process. Few practitioners engaged in self-exploration and the majority used emotional detachment as a professional technique.
Practitioners also had a limited view of cultural competence; defining it as remaining knowledgeable of the cultural influences in the practice context. Cultural competence involves having awareness of and sensitivity towards people from diverse cultural backgrounds (Rodolfa et al., 2005). Participants’ definition focused on being knowledgeable of cultural influences in the practice context. Yet, they appeared particularly insensitive to the complex dynamics of religious faith and sexual orientation. One participant stated that religion was not to be brought to therapy; another was unwilling to provide therapy to gay clients if they were not willing to ‘treat’ issues with their sexual orientation. Broader material and structural challenges compounded the limitations in foundational competency. These multi-level challenges are issues of continuous focus in western psychological practice but have been downplayed in African settings (e.g. Daniel et al., 2004).
Professional psychology training and research
The findings highlight the need for professional psychology training in Ghana to start focusing on practitioners’ personal growth. The limited knowledge on emotional and cultural competencies calls for new structures in clinical training and supervision that can lay the foundation for reflective practice. The professional psychologists in this study worked from a model reminiscent of the traditional doctor–patient relationship. Important contemporary issues such as religion and sexual orientation were a source of professional discomfort for some and therefore do not welcome in therapy. However, contemporary contexts in Ghana and other African countries create dynamic sociocultural environments for subjective, inter-subjective and group experience (Adams and Dzokoto, 2003; de-Graft Aikins, 2012, 2018). These complexities must be examined in psychological practice in Ghana. It is, therefore, important that psychologists are trained to incorporate the complex social constructions of clients’ problems into clinical concepts and interventions (Hoshmand, 2003; Pillay et al., 2013).
The findings strongly suggest the need to examine the ideologies as well as the models which inform professional psychology training in Ghana. Such an examination will reveal the importance of expanding the scope of training to encompass a psychology that looks at psychological practice both as a science and a cultural practice (Campbell and Murray, 2004; Hilton and Johnston, 2017; Hoshmand, 1996, 2003; Marks, 1996). This requires that training helps prospective psychologists to be reflective about how evolving local knowledge and situations might be important in their professional practice. One way to do this is to introduce cultural studies and critical psychology into training that allows students to evaluate psychology practice beyond mainstream scientific criteria (Adams and Dzokoto, 2003; de-Graft Aikins, 2018; de-Graft Aikins and Marks, 2007; Grobler et al., 2006; Hoshmand, 2003). The curriculum can be broadened to include contemporary studies in the social sciences and humanities in Ghana, as well as creative methodologies and students should be mentored to cultivate and nurture a culture of reflective practice. Another is to broaden the scope of psychology by engaging in research that is culturally and socially meaningful, embedded in historical understanding – for instance, exploring the socio-ecological roots of the psychological needs and problems of Ghanaians and developing context-specific interventions. Failure to reorient training and practice to the social realities of clients will restrict the services psychologists offer, leading to the provision of unsophisticated and even unethical practice.
Preventing a crisis of competence
Continuing competence is an ethical and professional obligation (Hilton and Johnston, 2017; Pope and Vasquez, 2007). The social and psychological challenges identified by respondents – for example, tensions between religious faith and demands of professional practice, emotional management, stresses of handling unusual cases without evolving guidelines – could inform material for continuous education. Presently, continuing competence is not officially monitored or regulated. As a result, practicing psychologists in Ghana do not receive context-specific continuous training that addresses their current needs as well as keep them ethically competent for practice. If the current trend in training and practice continues, we anticipate there will be a crisis of competence. Psychologists will not be able to meet the contemporary needs of Ghanaians. The social realities that Ghanaians face are complex and multifaceted and include poverty, family disintegration, physical and mental health disorders associated with modernity and ageing and conflicts of faith. The complex roots of these problems require open-minded and nuanced professional diagnosis, assessment and care. To be relevant in a changing world, professional psychology practice in Ghana should embed scientific psychological knowledge within evolving local knowledge and sociocultural contexts.
The study had two limitations. First, we explored the views of only 16 practitioners based in Accra. Second, we relied on retrospective responses to assess training. Currently, there are almost 300 psychologists registered with the Ghana Psychology Council, who work across the country. The majority (255) are clinical and counselling psychologists. We reached meaning saturation on themes reported in previous studies (e.g. the lack of formal support for continuous training). However, we did not reach meaning saturation on emerging themes relating to foundational competence: the lack of reflective practice, poor understanding of culture and diversity and tensions between personal faith and the demands of professional practice. Future studies can explore these issues with a larger cohort of participants, segmented across the country. Furthermore, it will be important to conduct assessment of training during and immediately after training, to set the benchmarks for continuous assessment over the careers of practitioners.
Conclusion
The study shows that professional psycho-logy training in Ghana does not fully equip psychologists with basic competencies needed for ethical practice. Even though the field is still young in Ghana, relative to other countries, issues relating to maintaining emotional, intellectual and professional competencies are central, and non-negotiable, aspects of professional practice. This study contributes to existing research on continuous competence in professional psychology in Ghana and to the global discourse on continuous competence in psychology.
Footnotes
Appendix 1
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.