
Abstract
Theories of allostatic load suggest that recurrent adaptive adjustments in contexts of adversity may have a negative impact on physical well-being. To test this hypothesis, this study evaluated 6-year-old children’s ego-resilience and physical abuse experiences on behavior problems and physical illness at the age of 8 years. A significant interaction between ego-resilience and physical abuse exposure indicated that, although ego-resilience buffered physically abused children from internalizing problems, it also predicted more physical illness in that group. Findings contribute to the growing body of evidence suggesting that efforts to mobilize an adaptive response in contexts of adversity may exact a cost on physical well-being.
Given that an estimated 64 percent of adults report exposure to at least one clear and pronounced adverse experience (e.g. physical abuse and poverty) prior to the age of 18 years (Anda et al., 2006), efforts to identify processes that promote positive adaptation in contexts of adversity (i.e. resilience) are a prominent focus of developmental science and practice (Curtis and Cicchetti, 2003; Luthar, 2015). Originally conceptualized as extraordinary expressions of invulnerability (Anthony and Cohler, 1987), pioneering research has revealed the Ordinary Magic of resilience (Masten, 2001). In this view, core developmental systems, such as self-regulation and attachment, operate normally despite adverse circumstance to support developmentally and culturally expected adaptation. In recent years, however, a small but growing number of studies have illuminated the ephemeral (and perhaps costly) expression of resilience over time, as well as across contexts. For example, results from a study of children reared in impoverished families revealed that high self-control was associated with psychosocial resilience (i.e. lower depressive symptoms and substance use), but accelerated cellular aging (Miller et al., 2015). Thus far, studies probing the potential costs of resilience have focused on specific indicators of competence (e.g. academic achievement) in contexts of chronic adversity (e.g. poverty) among primarily African American samples (Brody et al., 2013, 2016). This study expanded this literature by evaluating individual and interactive associations of children’s global capacity to navigate contextual demands (i.e. ego-resilience) and their exposure to a specific childhood adversity (i.e. physical abuse) with their socioemotional and physical adjustments in a diverse, primarily Latinx sample.
A multidimensional model of resilience
Research has shown that resilience expressed in one domain (e.g. school adjustment) may be related to (and potentially exacerbate) vulnerability in another domain (e.g. heightened internalizing problems; Luthar, 1991). Furthermore, longitudinal studies suggest that resilience at one point in time (e.g. childhood) may be associated with vulnerability at a later point in time (e.g. adulthood; Chen et al., 2015). For example, in Werner and Smith’s (1992) groundbreaking study of risk and resilience among a cohort of children born in Kauai, participants who evidenced competent adaptation (e.g. fewer depressive symptoms and behavior problems) in childhood reported higher rates of mental and physical health problems in adulthood as compared to participants with similar levels of adversity exposure who exhibited lower levels of competence during childhood. Likewise, studies by Brody and colleagues suggest that socioemotional resilience in contexts of adversity may exact a physical health cost vis-a-vis increased levels of physiological dysregulation (e.g. allostatic load) and accelerated aging among African American participants (Brody et al., 2013; Chen et al., 2015; Miller et al., 2015). For example, African American adolescents from economically disadvantaged families who evidenced a striving behavioral style, which is characterized by high aspirations, unwavering persistence, and investment in education and success (Brody et al., 2016: 2), had fewer depressive symptoms, but higher rates of type 2 diabetes at the age of 29 years as compared to low-striving adolescents from similar economic backgrounds. Although a number of explanatory processes may underlie these relations, extant research has favored allostatic models wherein the cumulative physiological dysregulation required to adapt to recurrent stressors (i.e. allostatic load) is thought to eventuate in physical wear and tear on the body (McEwen, 1998).
Despite recent advances in our understanding of the long-term strain placed on physical systems due to increased adaptive demands in high-stress contexts (McEwen, 1998), a number of gaps remain in our understanding of these relations. First, few studies have evaluated the potential for associations between socioemotional resilience and physical illness within childhood. Theories of allostatic load suggest that these processes accrue over time, which may have prompted an emphasis on studies of adolescents and adults using retrospective reports of adversity exposure. Notwithstanding the importance of these long-term associations, ignoring these processes within childhood may hinder our efforts to understand (and support) children’s adaptive organization in the context of adverse experiences. Second, prior studies of resilience and health have focused on systemic adversities, primarily poverty (Brody et al., 2013; Luthar, 1991), with less consideration accorded to specific adverse life events, such as child abuse. Third, a large subset of prior work has examined behavior-specific expressions of resilience (e.g. academic achievement; Brody et al., 2016), rather than more global and stable indicators, such as children’s capacity to negotiate challenges in a way that is flexible, resourceful, and adaptive (i.e. ego-resilience; Block and Block, 1980). Finally, previous studies have primarily focused on African American communities because they are disproportionately affected by chronic adversities, such as poverty and systemic racism. Thus, it is unclear whether or not putative competence costs generalize to other groups. This study sought to extend prior research by evaluating individual and interactive relations of 6 year olds’ ego-resilience and physical abuse exposure with their internalizing and externalizing behavior problems and physical illness at the age of 8 years in a diverse, predominantly Latinx sample.
An interactive model of competence and adversity
As a global capacity to negotiate challenges in a way that is flexible, resourceful, and responsive to contextual demands (Block and Block, 1980; Funder and Block, 1989), ego-resilience is a core component of childhood competence (Swanson et al., 2011). Consistent with this assertion, research shows that ego-resilience predicts positive socioemotional outcomes across diverse samples of children (Swanson et al., 2011), including those who have been exposed to adverse life events (Bolger and Patterson, 2003; Flores et al., 2005; Masten et al., 1999). However, despite the positive implications of ego-resilience for supporting psychosocial adaptation, theories of allostatic load suggest that recurrent efforts to mobilize an adaptive response in contexts of adversity may entail physiological demands that eventuate in heightened risks and rates of physical illness across development (McEwen, 1998).
Child physical abuse is a powerful contributor to adjustment difficulties for many, but not all children (Norman et al., 2012; Springer et al., 2007). Operationally defined as excessive physical punishment or cruel acts that result in physical injury to the child (e.g. bruises, cuts, and broken bones), child physical abuse has been linked to increased internalizing and externalizing symptomatology (Moylan et al., 2010), physiological dysregulation evidenced by blunted cortisol reactivity (Carpenter et al., 2011), and elevated risk of adult obesity (Richardson et al., 2014). In a rare test of interactive relations of social competence and childhood physical abuse with later behavior problems, Lansford et al. (2006) found that social competence and child physical abuse were associated with lower and higher rates of behavior problems, respectively, but there was not a significant interaction between competence and child physical abuse suggesting no heightened vulnerability to behavior problems for children who evidenced resilience. However, given the limited research in this area, it is not yet clear if and how children’s overarching ego-resilience (vs domain-specific social or academic competence) in the wake of physical abuse experiences may confer an elevated risk of physical (vs socioemotional) problems.
Study overview
This study sought to fill gaps in the extant literature examining the potential physical health costs of resilience by employing an ethnically and racially diverse sample followed over time within childhood. Furthermore, we evaluated the specific and interactive influences of a global indicator of competence, namely ego-resilience, and a discrete adverse life experience, namely, child physical abuse, on children’s socioemotional health (i.e. internalizing and externalizing problems) and physical health outcomes (i.e. rates of physical illness) to test if and how the adaptive implications of prior expressions of resilience would vary across domains.
Following documented relations between ego-resilience and a range of positive socioemotional outcomes in prior studies (Flores et al., 2005), we hypothesized that examiners’ ratings of children’s ego-resilience would be negatively associated with both internalizing and externalizing problems. However, given the dearth of research on ego-resilience and physical health, main effect predictions to rates of children’s physical illness were exploratory in nature. Consistent with prior studies suggesting both socioemotional and physiological problems in the wake of child physical abuse (Moylan et al., 2010; Richardson et al., 2014), we hypothesized that child physical abuse would be associated with higher rates of behavior problems and physical illness.
Importantly, our central hypothesis was that the relation between children’s ego-resilience (i.e. their overarching adaptive capacity) and later adjustment outcomes would be moderated by child physical abuse exposure. In line with past work testing relations of resilience with later socioemotional and physical health outcomes (Brody et al., 2013), we predicted that ego-resilience would be associated with fewer behavior problems, but higher rates of physical illness among children who had experienced child physical abuse, whereas, ego-resilience would be positively related to both socioemotional and physical health indicators among children without a history of child physical abuse. Furthermore, we expected that these associations, which have been observed in primarily African American samples, would be significant in this ethnically and racially diverse sample given that presumed processes of allostatic wear and tear are likely to be universal, rather than restricted to any single ethnic/racial group. This sample was comprised of children from diverse ethnic/racial groups, with the largest portion of children being of Latinx descent. Latinx individuals, much like African American youth, experience high rates of discrimination and social stressors that are both pervasive (e.g. racism) and varying in intensity across structural contexts (e.g. anti-immigrant legislation). Thus, many scholars have suggested youth in these communities are at increased risk of experiencing physical strain when evidencing resilience (Pascoe and Smart Richman, 2009). Therefore, this study evaluated the generalizability of these patterns across diverse ethnic/racial groups. All analyses accounted for covariates of child intelligence quotient (IQ) and family socioeconomic status (SES) because they are known contributors to children’s behavior problems and physical health, respectively (Gallo and Matthews, 2003).
Methods
Participants
Participants were drawn from an ongoing study of child development among 250 child–caregiver dyads. Dyads (n = 230) were included in these analyses if the family completed at least one laboratory assessments at the ages of 6 years (n = 215; Mage = 6 years and 1 month, SD = 2.51 months) and 8 years (n = 214; Mage = 8 years and 1 month, SD = 3.21 months). Nearly half (49.3%) the children in these analyses were female. Caregivers described their child’s ethnicity/race as Latinx (43.9%), Black (18.7%), Multiracial-ethnic (25.3%), and White (12.1%). All caregivers were female (91.9% biological mothers, 5.0% grandmothers or other female kin caregivers, and 3.0% foster/adoptive mothers). The majority of caregivers were married (61.6%) or in a committed relationship (18.8%), and just over half were employed (55.6%). Education levels were variable (e.g. 12.2% of caregivers had not completed high school and 12.4% of caregivers had earned a 4-year degree). The average family SES score using the Hollingshead (1975) Four-Factor Index of Social Status was 33.29 (SD = 11.86), which corresponds to semi-skilled employment (e.g. sales clerk). The ethnic/racial, educational, and socioeconomic demographics of this sample were representative of the southern California community from which the participants were recruited (US Census Bureau, 2011). A non-parametric Mann–Whitney test revealed no significant differences between children who completed both assessments (n = 199) and those who completed one assessment (n = 31) across study variables, including child sex (p = 0.687), child ethnicity/race (p = 0.239), SES (p = 0.463), ego-resilience (p = 0.563), child physical abuse (p = 0.213), internalizing (p = 0.391), externalizing (p = 0.763), or physical illness reports (p = 0.569).
Procedures
Flyers inviting participation in a “study of children’s learning and development” were distributed to local child care centers. Caregivers completed a brief intake screening by phone before scheduling a 3-hour laboratory assessment. Exclusionary criteria included children with diagnosed developmental disabilities and delays (e.g. autism spectrum disorder and intellectual disabilities; n = 3), children who were not able to understand English (n = 4), and children outside the target age range of 45–54 months (not tracked). Dyads completed 3-hour laboratory assessments at each time point, which consisted of measures with the child, the caregiver, and the caregiver and child interacting. Caregivers were compensated with US$25 per hour for their participation, and children received a small gift. Participants in this investigation attended either the age 6, age 8, or both the age 6 and age 8 assessments. Written informed consent was obtained from the child’s legal guardian at the beginning of each laboratory visit, and verbal informed assent was obtained from child participants beginning at the age of 8 years as suggested by prior research (Hurley and Underwood, 2002). All procedures were approved by the University’s Human Research Review Board.
Measures
Child IQ was assessed at the age of 6 years using the Vocabulary and Block Design subtests of the Wechsler (2002) Preschool and Primary Scale of Intelligence–III. Verbal IQ was measured using the vocabulary test in which the child verbally explained what orally presented words meant. Performance IQ was assessed using the Block Design subtest in which the child was asked to assemble red and white blocks to match models. Estimated verbal and performance IQs were averaged to yield a prorated measure of Full Scale IQ (Sattler, 1988).
Ego-resilience was assessed by trained independent examiners following the completion of the age 6 assessment using the California Child Q-Sort (CCQ; Block and Block, 1980) with common language updates provided by Caspi et al. (1992). Children were rated on 100 personality descriptors (e.g. when dealing with uncertainty tends to yield or give in, recovers quickly from a setback, and seems comfortable with self) using a 9-point scale from 1 (extremely uncharacteristic) to 9 (extremely characteristic) in a forced distribution using the computerized Riverside Accuracy Project (2010) Q-Sorter Program. Ratings of each child across the 100 items were correlated with Block’s (1991) ego-resilient prototype to yield a single concordance score with positive values reflecting higher ego-resilience (i.e. the global capacity to negotiate challenges in a way that is flexible, resourceful, and responsive to contextual demands) and lower scores reflecting less concordance with the prototype, or ego-brittleness (i.e. a global inability or difficulty adapting to changes in environment and/or navigating stressful contexts and emotions; see Block, 2008; Block and Block, 1980). Prior research has demonstrated the construct and structural validity of the CCQ ego-resilience profile in diverse samples with regard to ethnicity/race and SES (Arend et al., 1979; Block, 2008; Farkas and Orosz, 2015; Flores et al., 2005). Although not available from the single-rater data in this study, prior research also supports the reliability of this Q-sort methodology in varied samples (Nave et al., 2008).
Child Physical Abuse was assessed at the age of 6 years based on caregiver reports on the Early Trauma Inventory (ETI; Bremner et al., 2000) and the Parent-Child Conflict Tactics Scales–Short-form (CTS-PC-SF; Straus et al., 1995; Straus and Mattingly, 2007). The ETI includes a series of behaviorally specific questions regarding the child’s exposure to physical abuse (e.g. has someone ever punished your child resulting in physical injury) with prompts provided to assess ages of onset and offset, perpetrator identity and age, specific behaviors present during each incident, resulting injuries or interventions (e.g. legal and medical), and the chronicity or duration of abuse. Two independent coders rated the severity of child physical abuse as reported on the ETI using criteria set forth by McGee and colleagues (1995) on a 4-point scale, including no abuse (0), mild abuse (1), moderate abuse (2), and severe abuse (3). Severity ratings were established based on both the intensity and frequency of abuse. Mild intensity was reserved for corporal punishment experiences (i.e. physical contact in the context of caregiver discipline with minimal harm to the child), and was not included in final calculations of child physical abuse. Moderate intensity was indicated by contacts that caused marks or injuries, and went beyond accepted norms for disciplinary method or force (e.g. punching, kicking, and hitting with a hard object). High intensity captured experiences that had the potential for severe injury (e.g. beating, burning, and use of weapons). Intraclass correlations (ICCs) were calculated across all cases to assess reliability (ICC = 0.812). Severity ratings of 2 or higher were characterized as physical abuse exposure for this study. The CTS-PC-SF asks caregivers to rate the frequency with which they engaged in each of four physically abusive caregiving behaviors (e.g. hit child in face or head and hit on a part of body besides the bottom with a hard object) on a 6-point scale ranging from never (0) to more than 20 times in the past year (5). Endorsement of 2 or more physically abuse events in the past year was characterized as physical exposure for this study. Child physical abuse ratings from the ETI and the CTS-PC-SF were evaluated to yield a dichotomous rating of child physical abuse exposure such that a characterization of abuse on either scale would be considered as experiencing physical abuse (20.21%). Although children in the non-abused group may have received physical punishment (e.g. spanking on the bottom and one instance of a slap on the hand), these experiences did not rise to the definition of physical abuse (McGee et al., 1995). These criteria have been widely used and are considered the gold standard coding scheme for characterizing both participant and county-recorded child abuse reports (Dube et al., 2004; Shaffer et al., 2008; Wekerle et al., 2001).
Child Physical Illness was assessed at the age of 8 years using caregiver reports on the Child Health and Illness Profile–Child Edition (CHIP-CE; Rebok et al., 2001). The CHIP-CE includes seven items that assess the frequency of the child’s experiences of both general physical illness in the past 6 months (e.g. How often was your child sick?) and specific illnesses (e.g. How often has your child had a cold? . . . strep throat? . . . a skin infection?). All items were scored on a 5-point scale from never (0), to almost never (1), to sometimes (2), to almost always (3), and to always (4). The CHIP-CE evidenced moderate reliability (α = 0.617) in this study, which is expected given that individual forms of physical illness are not necessarily expected to correlate (e.g. a cold and a skin infection). The CHIP-CE evidences high criterion validity (e.g. strong correlations between each criterion and its related subdomain divided by types of illness) across diverse samples with regard to ethnicity/race and SES (Riley et al., 2004).
Child Behavior Problems were reported by the caregiver at the age of 8 years using the Child Behavior Checklist (CBCL) of the Achenbach test battery (McConaughy and Achenbach, 2004). The CBCL assessed child behavior problems across 113 items (e.g. obeys rules and adjusts well to changes in family plans) during the preceding 2 months using a 3-point scale from not true (0), to sometimes true (1), to very true or very often true (2). The CBCL broadband psychopathology scales for internalizing (e.g. withdrawn/depressed; α = 0.817) and externalizing problems (e.g. oppositional; α = 0.736) were used in these analyses, and evidence strong criterion validity (e.g. the degree of association between the current measure and external characteristics of the construct it is intended to assess) in samples of clinically referred and non-referred children from diverse groups (Achenbach and Rescorla, 2001).
Data preparation
All analyses were performed in SPSS version 24. Data were examined for non-normality to render parametric statistics valid (Afifi et al., 2007). Follow-up data were missing for caregiver reports of children’s behavior problems (n = 17; 7.9%) and physical illness (n = 20; 9.3%) at age 8. Missing data were imputed using the expectation–maximization (EM) algorithm as supported by Little’s Missing Completely at Random (MCAR) test: χ2 = 14.563, DF = 16, p = 0.557. Multiple imputation using the EM algorithm is superior to prior approaches, such as listwise deletion, mean substitution, and imputation with a limited number of iterations, because it estimates expected values from observed values through multiple iterations (up to 100) until the values stabilize to yield the best and most likely pooled estimate (Musil et al., 2002).
A multivariate analysis of variance (MANOVA) evaluated group differences across study variables as a function of the child’s sex, ethnicity/race, and their interaction. Correlation analyses assessed bivariate relations among study variables. Hayes’ (2013) PROCESS routine evaluated individual and interactive relations between ego-resilience and child physical abuse exposure as related to children’s later behavior problems and physical illness. This method represents an advance over traditional regression techniques because it employs a bootstrapping method to yield 95 percent confidence intervals for conditional effects while correcting for the non-normality of predictors (Hayes, 2012). This correction is particularly important to account for non-ignorable skew and kurtosis in the interaction terms. Three regression models evaluated the effects of ego-resilience and child physical abuse on children’s internalizing behavior problems, externalizing behavior problems, and physical illness problems. Significant interactions were then further probed using simple slopes, and all models were evaluated for three-way interactions by ethnicity/race (e.g. Latinx vs non-Latinx).
Results
Descriptive and bivariate analyses
A MANOVA revealed no significant differences among study variables by child sex (Wilks’ λ = 0.965, p = 0.458), ethnicity/race (Wilks’ λ = 0.911, p = 0.656), or their interaction (Wilks’ λ = 0.849, p = 0.089). As shown in Table 1, child IQ was positively related to family SES and ego-resilience. Family SES was also positively correlated with ego-resilience. Ego-resilience was negatively associated with externalizing problems, but it was not significantly associated with either internalizing problems or physical illness reports. Child physical abuse was positively associated with internalizing behavior problems, but was not significantly associated with externalizing behavior problems or physical illness. Internalizing behavior problems were negatively associated with physical illness, but were not significantly associated with externalizing behavior problems.
Bivariate correlations among study variables.
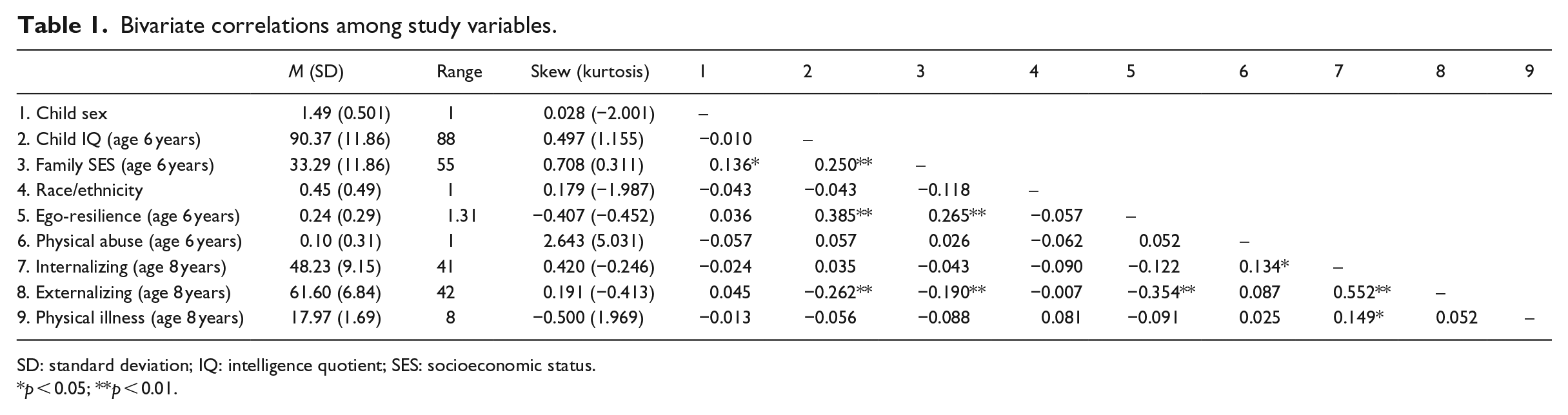
SD: standard deviation; IQ: intelligence quotient; SES: socioeconomic status.
p < 0.05; **p < 0.01.
Regression analyses
Regression analyses evaluated whether relations between ego-resilience and children’s socioemotional problems and physical illness varied as a function of child physical abuse exposure. There were no significant main effects of either ego-resilience or child physical abuse exposure for internalizing, externalizing, or physical illness problems in the full model. However, the relation between ego-resilience and later internalizing, but not externalizing, problems was moderated by child physical abuse exposure (see Table 2). As shown in Figure 1, among abused children, ego-resilience was negatively related to later internalizing problems (b = −2.318, p = 0.021), but this relation was not significant among children who had not been physically abused (b = −0.307, p = 0.711). The relation between ego-resilience and later physical illness problems was also moderated by child physical abuse exposure (see Table 2). As shown in Figure 2, among abused children, ego-resilience was positively related to physical illness problems (b = 1.904, p = 0.048), but this relation was not significant among children who had not been physically abused (b = −1.121, p = 0.121). Follow-up moderation analyses revealed no significant differences in the obtained relations by ethnicity/race (i.e. ego-resilience, child physical abuse, and Latinx/non-Latinx ethnicity).
Children’s adaptation at the age of 8 years on children’s ego-resilience and physical abuse exposure at the age of 6 years.
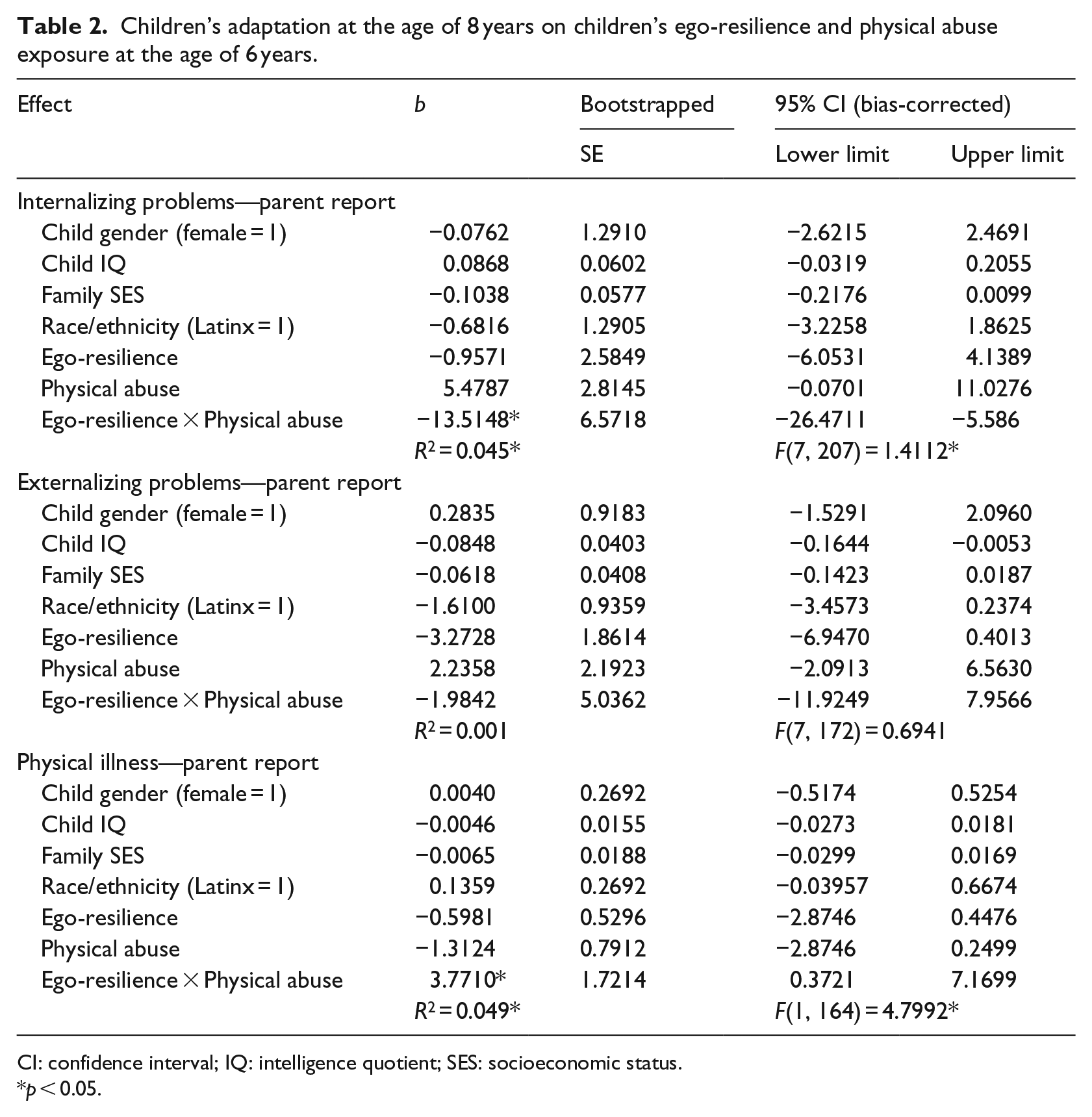
CI: confidence interval; IQ: intelligence quotient; SES: socioeconomic status.
p < 0.05.
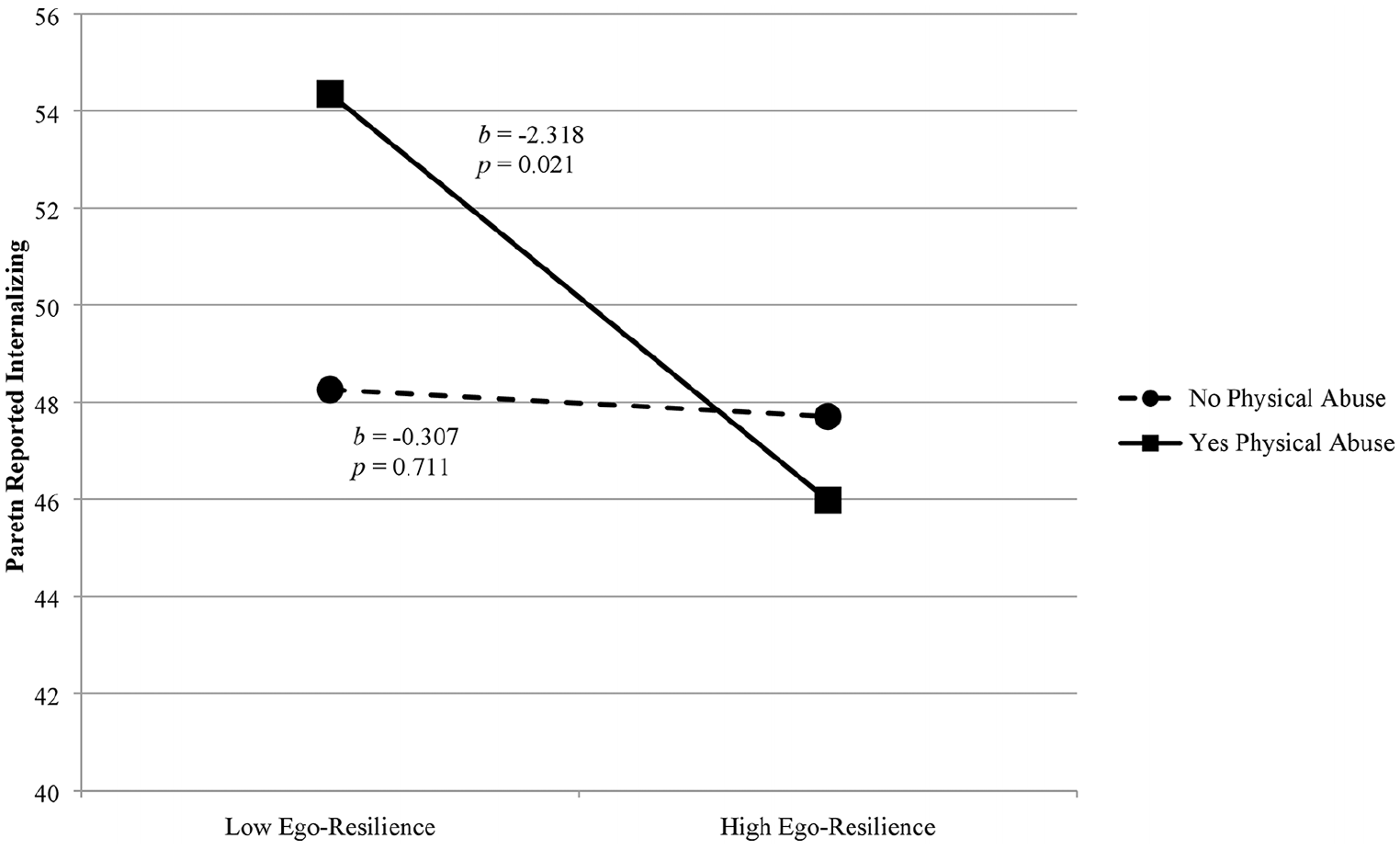
The relation between ego-resilience at the age of 6 years and physical abuse exposure at the age of 6 years as related to children’s internalizing behavior problems at the age of 8 years.
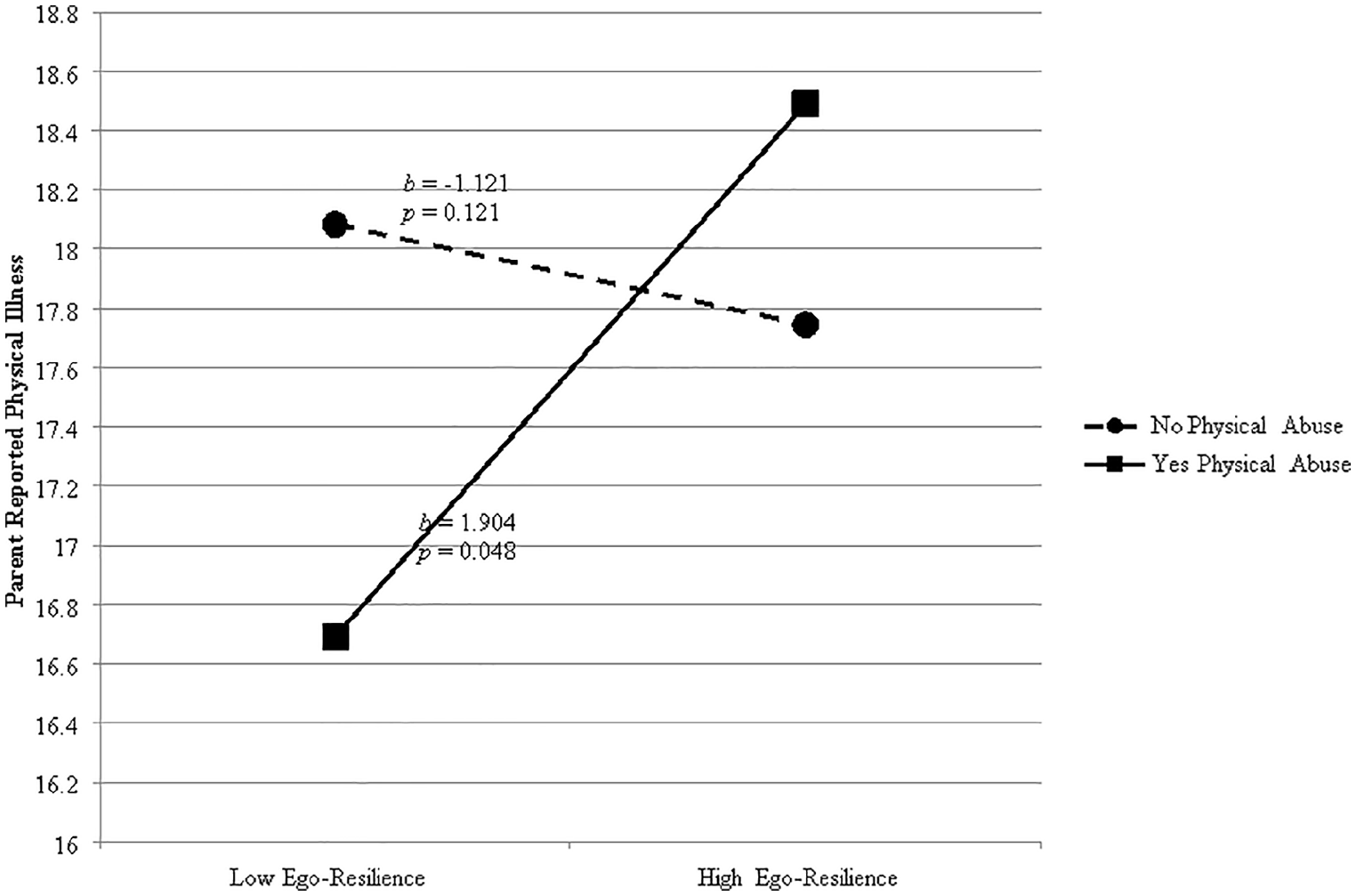
The relation between ego-resilience at the age of 6 years and physical abuse exposure at the age of 6 years as related to children’s physical illness occurrence at the age of 8 years.
Discussion
This study evaluated prospective associations of children’s ego-resilience and child physical abuse with later internalizing behavior problems, externalizing behavior problems, and physical illness to test the hypothesis that expressions of socioemotional competence in contexts of adversity (i.e. resilience) may be associated with increased risk of physical illness in later development. Our findings suggest that, even within a 2-year span of childhood, ego-resilience, as an indicator of childhood competence, was associated with fewer internalizing, but not externalizing, problems among children with a history of physical abuse (i.e. children who evidenced resilient adaptation). However, ego-resilience was also associated with more physical illness problems (i.e. a potential cost of resilient adaptation) in the wake of child physical abuse. Interestingly, these relations were not significant among children who were not physically abused, nor were there significant main effect contributions of either ego-resilience or child physical abuse to the outcomes examined here.
Our findings are consistent with past work showing that, in the context of adversity, competence can be protective in some domains, but exert costs in others (Brody et al., 2013; Brody and Ge, 2001; Chen et al., 2015; Miller et al., 2015). Building upon and extending prior research with older adolescents and adults (Brody et al., 2013; Chen et al., 2015), this study documented these associations within childhood to demonstrate that the potential for physical costs associated with efforts to mobilize competent adaptation in contexts of adversity (i.e. resilience) may be evident earlier in development than extant evidence would suggest. Moreover, in contrast to prior studies with predominantly African American samples, the notable ethnic/racial diversity of the current sample, particularly with regard to the high proportion of Latinx children (43.9%), demonstrated that these processes are operative in diverse ethnic/racial groups.
The obtained interactive findings are consistent with prior studies of African American adolescents and adults, which found that physical illness problems, such as type 2 diabetes and physiological dysregulation, were elevated among individuals who evidenced greater childhood competence (i.e. high teacher-reported self-control as well as academic and social competence) in the context of prior adversity, namely socioeconomic disadvantage (Brody et al., 2013, 2016). Furthermore, although emotion regulation difficulties that often accompany abuse exposure have documented links with internalizing behaviors (Moylan et al., 2010), we found that ego-resilience acted as a buffer between child physical abuse and internalizing, but not externalizing, problems. Importantly, this finding mirrors prior research suggesting that expressions of competence (e.g. self-regulation) may protect against internalizing, but not necessarily externalizing, problems in contexts of adversity (Brody et al., 2016). These findings are also consistent with the only prior study to have assessed the interactive influence of competence and child physical abuse, which yielded non-significant results in the prediction to children’s externalizing problems (Lansford et al., 2006).
Interestingly, there were no significant main effects of ego-resilience or child physical abuse exposure on either socioemotional or physical illness problems. Bivariate correlations revealed a significant negative correlation between ego-resilience and externalizing problems, as well as a significant positive correlation between child physical abuse and internalizing problems. However, the non-significant relations of ego-resilience and child physical abuse with children’s adjustment in the full regression models highlight robust interindividual variability in how experiences of competence and adversity influence development individually and interactively. Specifically, the absence of significant main effects suggests that the combination of competence (i.e. ego-resilience) and adversity (i.e. child physical abuse) may be more informative for understanding children’s adjustment (i.e. internalizing and physical illness problems) than either construct alone. Of note, these patterns may have been particularly pronounced in this non-clinical community sample, which may have featured greater variation in levels of competence and adversity, as compared to clinical samples with more restricted ranges on these variables.
These findings supported our hypothesis that children’s competent adaptation (i.e. high ego-resilience) in contexts of adversity (i.e. child physical abuse exposure) may support positive socioemotional outcomes (i.e. fewer internalizing problems) while compromising their physical well-being (i.e. more physical illness). Ego-resilience encompasses broadband adaptive processes, such as self-regulation and the capacity to navigate challenges, that support global competence (Block, 1993). In turn, these capacities may help to mitigate negative socioemotional outcomes in the wake of childhood adversity (Milioni et al., 2015). However, as demonstrated in this study, and as has been suggested by theories of allostatic load (McEwen, 1998), mobilizing adaptive regulation in contexts of adversity may require more frequent (or more extreme) physiological adjustments that eventuate in physical wear and tear, decreased immune health, and increased physical illness.
Despite these suggestive findings, this study design did not support the evaluation of specific mechanisms that may account for the obtained findings. Certainly, allostatic load theory offers one important pathway by which ego-resilience may exact a physical health cost. Competence in the face of adversity can demand allostasis (i.e. adaptation in the face of potential challenge; McEwen, 1998) and increased level of allostatic load (i.e. increased “wear and tear” on the body from frequent adaptations; McEwen, 1998), and prior studies have demonstrated associations between allostatic load and morbidity and mortality (e.g. Seeman et al., 1997). However, additional mechanisms warrant consideration in future research. For example, it is possible that a subset of children simply manifest the negative effects of child physical abuse on a more physiological level (i.e. although they do not experience the socioemotional effects of adversity to the same degree as others, these children do suffer the physiological effects of these stressful experiences). In this view, apparent health “costs” associated with resilient adaptation may simply reflect an alternate, yet equally problematic, developmental pathway in the wake of adverse experience (i.e. multifinality; Cicchetti and Rogosch, 1996). Similarly, biological sensitivity to context theories suggests that certain subsets of children may be differentially susceptible to their environmental inputs (Boyce and Ellis, 2005). This theory posits that heightened stress reactivity (e.g. heightened cortisol response) may reflect an increased biological sensitivity to context, such that the individual experiences increased potential for negative health effects under conditions of adversity and positive effects under conditions of support and protection. Furthermore, rather than a cost of coping, these effects could reflect how different coping strategies, such as distraction and avoidance, could help children achieve positive socioemotional outcomes, but also engender poor health behaviors that lead to increased physical illness (e.g. poor diet, poor sleep, and ignoring bodily signals).
Strengths and limitations
This study provides evidence for the importance of examining multiple domains of adjustment within childhood, in addition to adolescent or adult examinations with retrospective abuse accounts, to understand the development of both resilience and maladaptation in contexts of adversity. Our findings fill important gaps in this literature by providing evidence that these processes can manifest within childhood, and in diverse ethnic/racial groups in and beyond the African American community. Furthermore, we found that these processes held even when we considered a global, rather than behavioral, measure of competence, in the wake of relational, rather than strictly economic, adversity exposure. Indeed, these findings held even when family SES was controlled. Unfortunately, a number of limitations in this study constrained our ability to fully evaluate competing explanations of our observed findings.
First, although we utilized well-validated measures of both ego-resilience and child physical abuse, our single-informant design precluded assessments of reliability within our study. Second, because we were not able to control for prior levels of children’s socioemotional and physical illness problems, we were unable to draw directional conclusions about relative changes in symptomatology across time points. Third, our use of parent reports of childhood physical abuse exposure likely underestimated the true occurrence of physical abuse in our sample due to social desirability. However, studies comparing the accuracy of self-report maltreatment coding with other types of measurement typically find that parent reports of maltreatment are still useful for studies examining child psychopathology (Bennett et al., 2006). Fourth, although we evaluated child physical abuse because previous literature suggests it is an adverse relational experience (Norman et al., 2012), some children may also have experiences other adversities in addition to physical abuse which could confound these effects. Fifth, although we justified our consideration of physical illness outcomes using allostatic load theory, the absence of biological health measures (e.g. blood pressure, and cortisol; McEwen, 1998) precluded our ability to directly test allostatic load as a mechanism of health problems in the context of resilience to childhood physical abuse. Finally, although our diverse community sample supported our generalization beyond the African American samples of prior studies, we were not able to probe these relations within specific ethnic/racial groups.
Implications and future directions
These findings highlight the multifaceted nature of resilience, such that resilience documented in one domain (i.e. absence of behavior problems), does not equal unilateral resilience (i.e. increased rates of physical illness). Importantly, these findings highlight the need to include physical health adjustment indicators in future studies of risk and resilience. Although future research is needed to clarify competing interpretations of these health effects as a cost of resilience versus a heretofore underappreciated cost of adversity, providing physical health resources (e.g. access to care, better nutrition, and biofeedback; Levin and Brouwer, 2014) to children experiencing abusive caregiving may reduce their physical strain, and be especially effective for children who exhibit high competence or ego-resilience despite exposure to adversity (i.e. resilience).
As noted earlier, future studies should evaluate the generalizability of these processes to other ethnic/racial groups, particularly individuals of Latinx descent. Latinx individuals, much like African American youth, experience high rates of discrimination and social stressors that are both pervasive (e.g. racism) and vary in intensity with structural inputs (e.g. anti-immigrant legislation) and may put these populations at increased risk of physical strain while evidencing resilience (Pascoe and Smart Richman, 2009). Ongoing research efforts are needed to clarify whether or not these effects are unique to the ethnic/racial minority group experience as a function of encountering such chronic stress, or if such associations are present in groups who are protected against adversities outside those being explored (i.e. those drawn from majority ethnic/racial and high SES backgrounds). By conducting future examinations with large, diverse samples distributed across ethnic/racial and economic groups, we will be able to elucidate culturally specific risk and protective factors (e.g. familism and acculturative stress) to further understand the relations between resilience and physical health, as well as to target prevention and intervention efforts.
Similarly, research efforts should expand this study to document relations from the age of 8 years across childhood into later ages. Middle school is known as a time in which children are particularly vulnerable to internalizing problems and increased reports of symptomatology (Kuperminc et al., 2001). This effort to document these associations prior to onset of middle school vulnerability is important, however, examining patterns across this entire developmental period would better aid in understanding pathways to maladaptation.
Finally, future research should seek to elucidate the contexts within which competence may be associated with the greatest health problems (e.g. when encountering specific abuse types and without certain complementary support structures), and clarify the timing and magnitude of these effects with respect to both early versus later risk exposure and early versus later competence. Exploring how specific facets of both competence (e.g. ego-resilience vs academic achievement) and adversity (e.g. environmental vs relational) are uniquely related to children’s socioemotional and physical health outcomes remains an open question. Future research in this area should examine how combinations of experiences influence the expression of resilience versus maladaptation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Science Foundation DLS-0951775.