
Abstract
Given that suicidal behaviour is a pressing concern in inflammatory bowel disease populations, this study sought to model the sequence of variables that lead to its development. Participants (n = 282) completed online self-report questionnaires regarding predictors of suicidal behaviour. A cross-sectional model of the progression from symptoms to suicide risk revealed that biomedical variables were significantly associated with psychosocial predictors of suicidal behaviour, which were significantly related to theory-driven predictors of suicidal behaviour, which were ultimately associated with suicide risk. Evidently, interventions need to target distal predictors of suicidal behaviour to mitigate harmful downstream effects.
Annually, approximately 800,000 deaths result from suicide across the world (World Health Organization (WHO), 2018). Precursor behaviours, such as suicidal ideation (thoughts about, considerations of or plans for suicide) and suicide attempts, are even more prevalent (Nock et al., 2008). Given the global impact of suicidal behaviour, there is a need to identify groups most at risk for suicide and their associated risk factors. Individuals with inflammatory bowel disease (IBD; umbrella term for Crohn’s disease and ulcerative colitis) may represent one such group, as rates of suicidal ideation exceed 30 per cent in some IBD samples (Fuller-Thomson and Sulman, 2006; Kim et al., 2017). Although epidemiological data suggest that suicidal ideation is a persistent cause for concern in IBD populations, research on suicidal behaviour in IBD populations is limited and the progression towards suicide risk has not yet been modelled in this population. As such, this study sought to model associations between empirically supported risk factors of suicidal behaviour in an online IBD sample to gain a comprehensive understanding of suicide risk in IBD.
The experience of IBD symptoms themselves may contribute to increased suicide risk. Indeed, high levels of disease activity are associated with increased suicidal behaviour in individuals with various chronic health conditions (Mok et al., 2014). A potential link between disease activity in chronic health conditions and suicidal behaviour may be pain, given that individuals with painful chronic health conditions are at an elevated risk for suicidal behaviours (Racine, 2017). The associations between disease activity, pain and suicidal behaviour are concerning as pain is a common IBD experience (Bielefeldt et al., 2009), and recent research suggests a significant relationship between IBD pain concerns and suicidal ideation (Hashash et al., 2019).
Symptom severity and pain may indirectly increase an individual’s risk of suicide when paired with heightened psychological distress, a common experience for individuals with IBD (Casati et al., 2000; Walker et al., 2008). Feelings of shame associated with physical appearance (e.g. ostomy bags), diet changes, frequency of toilet use, uncontrollable flatulence or fears of incontinence can be particularly distressing (Casati et al., 2000) and are significantly associated with depressive symptoms in IBD populations (Trindade et al., 2017). Given the lifetime prevalence of depression in IBD populations (Walker et al., 2008), and the relationship between depression and suicidal behaviour (Ribeiro et al., 2018), it is not surprising that over 40 per cent of individuals with comorbid IBD and depression considered suicide at some point during their lifetime (Fuller-Thomson and Sulman, 2006). Indeed, Hashash et al. (2019) found that one of the strongest risk factors for suicidal ideation in IBD outpatients was depressive symptom severity. A related variable with a proposed role in predicting suicidal behaviour is hopelessness (Ribeiro et al., 2018), though this has been given less attention in IBD research.
Further still, two theories of suicide that act as immediate precursors to suicidal behaviour remain unexplored in IBD populations. The theory of psychache posits that suicide occurs when an individual deems their psychache (i.e. psychological pain) to be unbearable (Shneidman, 1993). Several studies support the claim that psychache is a core clinical variable for understanding suicide, and that other predictors (e.g. depression) are associated with suicidal behaviour insofar as they predict psychache (Verrocchio et al., 2016). Alternatively, the Interpersonal-Psychological Theory of Suicide (IPTS) suggests two variables that contribute to suicidal ideation: perceived burdensomeness (i.e. the belief that one’s existence is a burden on others) and thwarted belongingness (i.e. the experience that one reports feeling alienated from valued social circles; Van Orden et al., 2010). The addition of a third variable, acquired capability to commit suicide, leads to a suicide attempt (Van Orden et al., 2010). A systematic review of the IPTS revealed that perceived burdensomeness was strongly associated with suicidal ideation, whereas thwarted belongingness was only moderately associated with suicidal ideation, suggesting that thwarted belongingness may be an ancillary predictor of suicidal behaviour (Ma et al., 2016).
In this study, various theoretically and empirically supported determinants of suicide risk were modelled using the structure of the integrated motivational–volitional (IMV) model of suicidal behaviour, a tripartite model describing the biopsychosocial context in which suicidal behaviour may emerge (pre-motivational phase), the variables that lead to the emergence of suicidal ideation (motivational phase), and the variables that lead the transition from suicidal ideation to suicide attempts/death (volitional phase; O’Connor and Kirtley, 2018). As per the IMV model, pre-motivational variables affect suicide risk through their influence on constructs within the motivational and volitional phases. In this study, IBD symptoms and pain are biological vulnerabilities (pre-motivational phase) that contribute to the experience of psychosocial vulnerabilities (i.e. shame, depressive symptoms and hopelessness begin the motivational phase). In turn, these psychosocial vulnerabilities contribute to the development of immediate predictors of suicide risk (i.e. psychache, perceived burdensomeness and thwarted belongingness conclude the motivational phase). Thus, it was hypothesized that biomedical variables (i.e. IBD symptom severity, average pain) would be related to psychosocial variables (i.e. shame, depressive symptoms and hopelessness), which then would be associated with theory-driven variables (i.e. psychache, perceived burdensomeness and thwarted belongingness), which ultimately would be associated with suicide risk.
Method
Participants
To be eligible to participate in this study, individuals had to be over the age of 18 years, able to read and write in English, and diagnosed with IBD. Individuals suffering from a major psychiatric disorder (e.g. psychosis) or a major medical condition (e.g. severe cardiac, pulmonary, renal or hepatic disease) that would interfere with their study participation were excluded from participation.
Two hundred and eighty two participants (Mage = 40.95 years, range = 18–79 years old) completed at least 80 per cent of each questionnaire and were included in the analysis. Participant information is presented in Table 1. Despite a lack of generalized guidelines and varying heuristics for sample size requirements for structural equation models, the present sample size reflects the state of structural equation modelling in psychology (i.e. median sample size ~200 cases; Kline, 2015).
Participant characteristics of study sample.
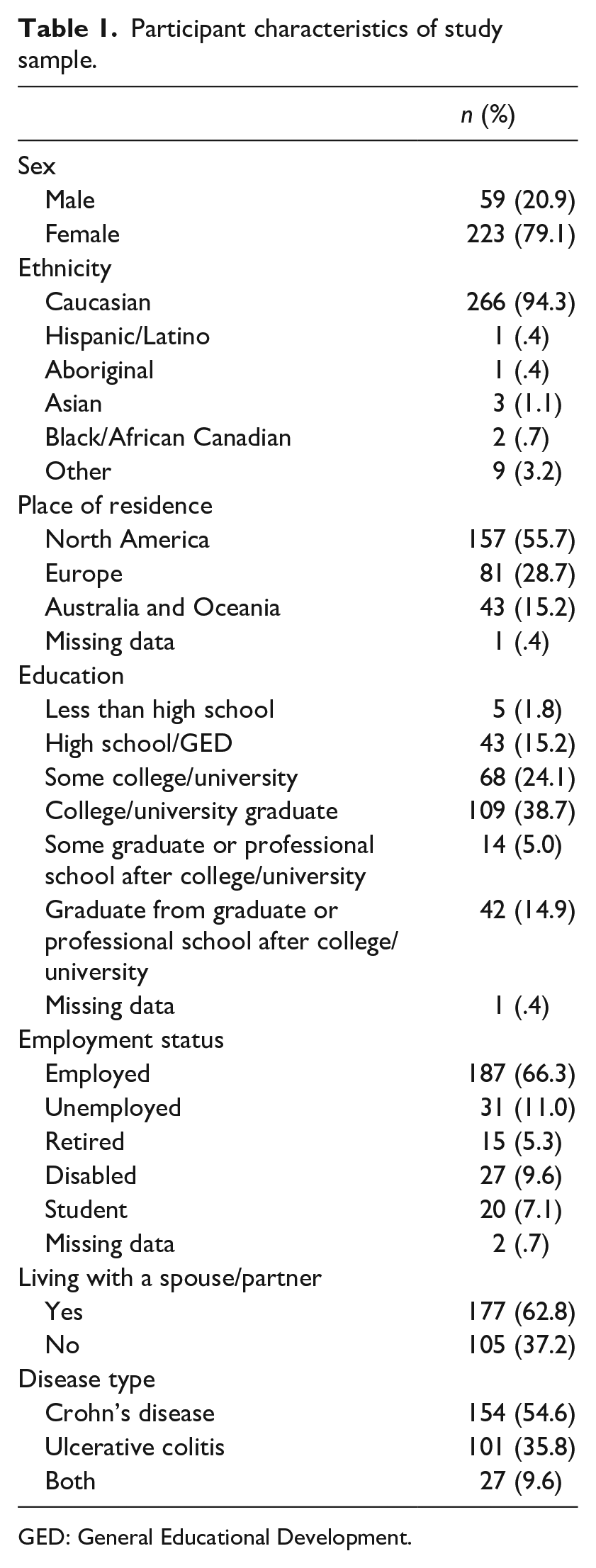
GED: General Educational Development.
Study measures
All measures used in this study are valid and reliable, as described in the measures’ original papers. The Cronbach’s alpha (α) and McDonald’s omega (ω) for each questionnaire in the current sample are reported below.
IBD symptoms were measured with the IBD Symptom Inventory Short Form (IBDSI-SF; α = .92, ω = .93; Sexton et al., 2019), a 26-item questionnaire assessing a broad range of patient-reported IBD symptoms (bowel symptoms, abdominal and bodily discomfort and fatigue; e.g. ‘I had abdominal pain’ rated none to prolonged/severe). A total score was calculated by summing all items. Higher scores indicate elevated symptom severity.
Pain experience and intensity was assessed using the pain body diagram from the McGill Pain Questionnaire (Melzack, 1975), which was divided using a grid system that identifies 45 different areas of the body (Margolis et al., 1986). Participants marked locations where they experience pain and rated the intensity of their pain in that region on a scale from 1 (mild pain) to 10 (extreme pain). An average pain 1 score was calculated by summing the pain intensity ratings and dividing this value by the number of pain regions the participant selected. Higher scores indicate greater average pain.
Shame was measured using the Chronic Illness-Related Shame Scale (CISS; α = .91, ω = .94; Trindade et al., 2017), which assessed the level of shame related to a chronic disease and/or its symptomatology. Participants indicated the degree to which they experience the thoughts/feelings described in seven statements (e.g. ‘I feel that my illness is embarrassing’) using a rating scale from 0 (never true) to 4 (always true). A total score was not calculated as shame was a latent construct (see section ‘Statistical analysis’).
Depressive symptoms were measured using the Patient Health Questionnaire-9 (PHQ-9; α = .88, ω = .90; Kroenke et al., 2001), which assessed depressive symptoms within the past 2 weeks. Participants reported their level of agreement to nine statements (e.g. ‘Little interest or pleasure in doing things’), based on clinically diagnostic criteria of depression, using a rating scale from 0 (not at all) to 3 (nearly every day). A total score was calculated using the sum of these nine items. Higher scores indicate greater severity of depressive symptoms.
Hopelessness was measured using the State Hopelessness Scale (SHS; α = .93, ω = .95; Dunn et al., 2014), which assessed negative outlook and helplessness towards the future over the past week. Participants indicated their level of agreement to 10 statements (e.g. ‘I see my future as gloomy’) using a rating scale from 1 (strongly disagree) to 4 (strongly agree). A total score was not calculated as hopelessness was a latent construct (see section ‘Statistical analysis’).
Psychache was measured using the Psychache Scale (α = .96, ω = .97; Holden et al., 2001), a 13-item questionnaire assessing the degree to which participants experience psychache (i.e. general psychological pain). Participants rated the frequency with which items 1–9 (e.g. ‘Psychologically, I feel terrible’) occur using a rating scale from 1 (never) to 5 (always), and their level of agreement to items 10–13 (e.g. ‘My pain is making me fall apart’) using a rating scale from 1 (strongly disagree) to 5 (strongly agree). A total score was calculated using the sum of these 13 items. Higher scores indicate greater psychache.
Perceived burdensomeness and thwarted belongingness were measured using the Interpersonal Needs Questionnaire-15 (INQ-15; α = .94, ω = .96; Van Orden et al., 2012), a 15-item questionnaire assessing one’s perceived social fit (e.g. ‘These days I think I am a burden on society’). Participants indicated the degree to which each item is true, using a rating scale from 1 (not at all true for me) to 7 (always true for me). The perceived burdensomeness score was calculated using the sum of items 1–6 (α = .94, ω = .97), and the thwarted belongingness score was calculated using the sum of items 7–15 (α = .91, ω = .95). Higher scores indicate greater perceived burdensomeness and thwarted belongingness, respectively.
Suicide risk was measured with the Suicide Behaviours Questionnaire Revised (SBQ-R; α = .81, ω = .84; Osman et al., 2001), a four-item questionnaire assessing lifetime suicidal thoughts and actions, suicidal ideation in the past year, lifetime suicide plans and self-reported future risk of suicide (e.g. ‘How often have you thought about killing yourself in the past year?’). A total score was calculated by summing the four items. Scores ⩾7 indicate clinically significant suicide risk compared with an adult general population, and scores ⩾8 indicate clinically significant suicide risk compared with an adult psychiatric inpatient population.
Procedure
This study was advertised online through emails to English-speaking IBD patient support groups, advertisements on the Crohn’s and Colitis Canada website and Facebook advertisements targeted to individuals with IBD-related ‘likes’. Interested participants clicked on the study link to access the letter of information and consent form. Eligible participants checked off a box to indicate their consent to participate, after which questionnaires were administered. Completion of the questionnaires took approximately 1 hour. Participants had the option of declining any questions they felt uncomfortable answering. Although the questions in this survey were of a sensitive nature, participation in online research assessing suicidal behaviour generally does not cause harmful distress to research participants (Gibson et al., 2014). Regardless of their stopping point in the survey, all participants received a debriefing form listing online resources for dealing with feelings of distress. Participants did not receive compensation for their participation. This study was approved by the Queen’s University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board.
Statistical analysis
Partially latent structural regression models were used to examine how various biopsychosocial variables contribute to predicting suicide risk in individuals with IBD. Given that the IBDSI-SF, PHQ-9 and SBQ-R are emergent variable systems, IBD symptoms, depressive symptoms and suicide risk, respectively, are measured variables. As well, average pain is a measured variable because it is a single mean score. In addition, psychache is a measured variable because the Psychache Scale was developed using principle components analysis, which is fundamentally different from factor analysis. Consequently, to fairly compare psychache with the IPTS, perceived burdensomeness and thwarted belongingness are measured variables, leaving shame and hopelessness as the latent variables in the structural models. Models were refined until acceptable fit and parsimony (i.e. exclusion of non-significant paths) were achieved. All data analyses were conducted in R (R Core Team, 2017) using the Lavaan (Rosseel, 2012) and Psych (Revelle, 2018) packages. All regression coefficients presented in this study are unstandardized, and error variances on all models were free to vary. A comprehensive figure including indicators and non-significant paths can be found in Supplementary Materials.
Results
Of the total sample, 40.78 per cent of participants scored ⩾7 on the SBQ-R, indicating clinically significant suicide risk compared with an adult general population, and 30.85 per cent of participants scored ⩾8, indicating clinically significant suicide risk compared with an adult psychiatric inpatient population.
Maximum likelihood estimations were used to test multiple cross-sectional models representing the possible relationships between IBD symptoms, average body pain, illness-related shame, depressive symptoms, hopelessness, psychache, perceived burdensomeness, thwarted belongingness and suicide risk. Although the hypothesized model achieved acceptable fit on all fit indices (Table 2), one path was not significant; thwarted belongingness was not significantly associated with suicide risk, b = .023, SE = .014, p = .093. As such, a more parsimonious refined model that did not include thwarted belongingness (Figure 1) was tested. The refined model achieved acceptable fit on all fit indices (Table 2), and all paths were significant.
Fit indices for partially latent structural regression models.
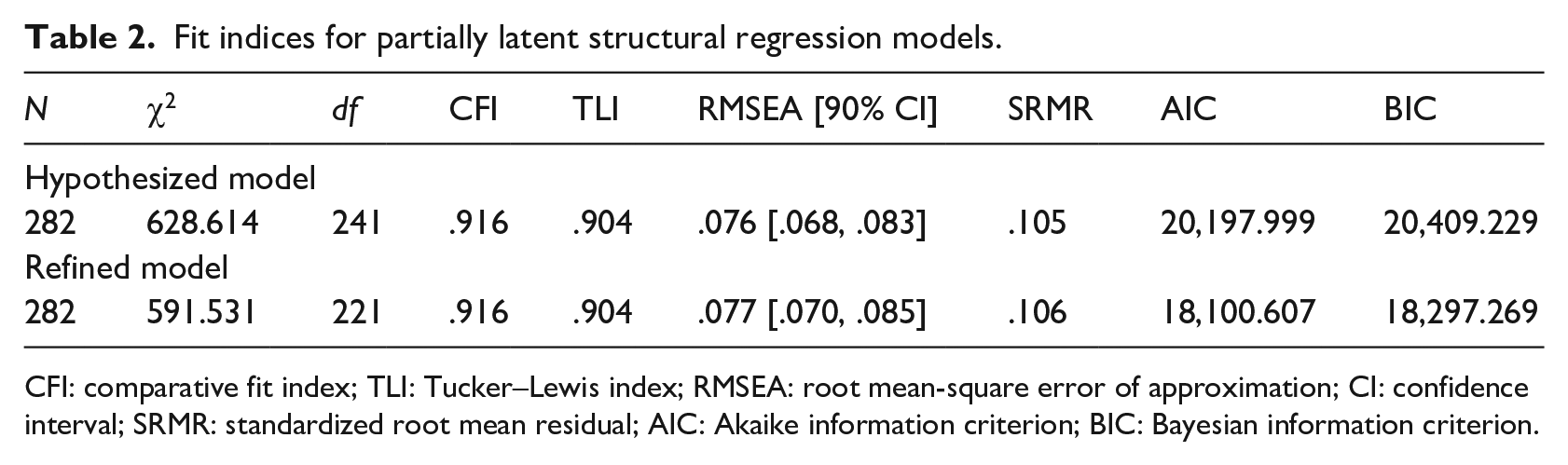
CFI: comparative fit index; TLI: Tucker–Lewis index; RMSEA: root mean-square error of approximation; CI: confidence interval; SRMR: standardized root mean residual; AIC: Akaike information criterion; BIC: Bayesian information criterion.
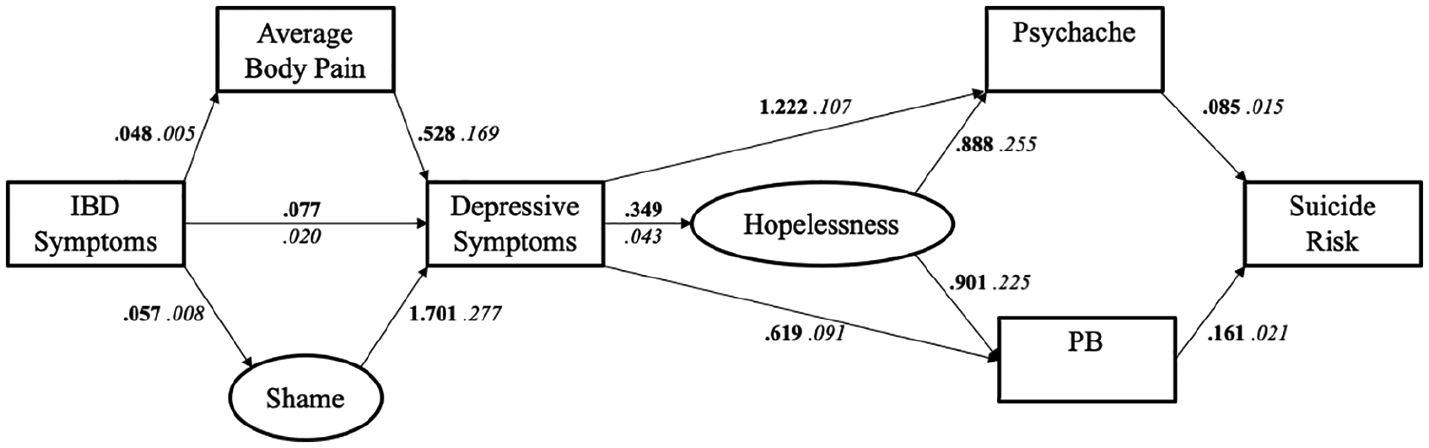
Refined model of the cross-sectional progression of IBD symptoms to suicide risk.
In the refined model, greater IBD symptom activity and severity was significantly associated with greater average body pain, b = .048, SE = .005, p < .001, and illness-related shame, b = .057, SE = .008, p < .001. Moreover, more IBD symptom activity and severity, average body pain, and illness-related shame were each significantly and independently associated with greater depressive symptoms, b = .077, SE = .020, p < .001; b = .528, SE = .169, p = .002; b = 1.701, SE = .277, p < .001, respectively. Greater depressive symptoms then were significantly associated with greater hopelessness, b = .349, SE = .043, p < .001, psychache, b = 1.222, SE = .107, p < .001, and perceived burdensomeness, b = .619, SE = .091, p < .001. Greater hopelessness was similarly significantly associated with greater psychache, b = .888, SE = .255, p < .001, and perceived burdensomeness, b = .901, SE = .225, p < .001. Finally, greater psychache and perceived burdensomeness were significantly associated with higher suicide risk, b = .085, SE = .015, p < .001; b = .161, SE = .021, p < .001, respectively.
The hypothesized and refined models were compared to determine which model is a better fit to the data. A chi-square difference test revealed that the models were significantly different, χ2 = 37.083, p = .011, indicating that the more complex hypothesized model would be preferred. However, the hypothesized model had higher Akaike information criterion and Bayesian information criterion than did the refined model indicating that the refined model had better predictive accuracy (McElreath, 2016). Consequently, the refined model was selected as the final model of the cross-sectional progression of IBD symptoms to suicide risk. The refined model accounted for 42.6 per cent of the variance in suicide risk.
Discussion
The present examination of suicide risk in an online IBD sample indicates a concerning global rate of suicide risk in IBD populations; over 40 per cent of individuals in the present sample were clinically at-risk for suicide compared with the general adult population.
To understand the emergence of suicide risk in IBD populations, this study situated the progression of IBD symptoms to suicide risk within a theoretical framework. The IMV model of suicidal behaviour (O’Connor and Kirtley, 2018) was applied in the present sample to evaluate an empirically supported risk factor’s relative place within the process leading from symptoms to suicide risk. As hypothesized, biomedical variables (i.e. IBD symptoms, average pain) were associated with psychosocial variables (i.e. shame, depressive symptoms, hopelessness), which were related to theory-driven variables (i.e. psychache, perceived burdensomeness), which were then associated with greater suicide risk. However, contrary to the expectation that both perceived burdensomeness and thwarted belongingness would be associated with higher suicide risk, thwarted belongingness was not significantly related to suicide risk. One possible explanation for this non-significant relationship is that individuals with chronic diseases, such as IBD, are particularly attuned to the potential difficulty their disease places on their support systems (Wilson et al., 2005). Indeed, individuals with IBD have reported feeling like a burden to others (Casati et al., 2000). Moreover, the predictive ability of perceived burdensomeness over thwarted belongingness for suicide risk in the present sample is consistent with reviews of the IPTS (Ma et al., 2016), providing further support that thwarted belongingness may be an ancillary predictor of suicide risk in general.
The results of this study relate to one of the main treatment goals outlined in the World Gastroenterology Organization practice guidelines for treating and managing IBD: improve and maintain the general well-being of patients to optimize their quality of life (Bernstein et al., 2016). With this treatment goal and the present findings in mind, health care professionals working with IBD patients should not shy away from inquiring about suicidal behaviour in a patient – asking about suicidal thoughts does not provoke suicidal acts (Dazzi et al., 2014). For health care professionals, a first step towards having open conversations about psychological distress may be screening for suicide risk and associated predictors using validated screening tools (e.g. PHQ-9 and SBQ-R), as these tools can assess the severity of depressive symptoms, indicate suicidal ideation and monitor patients’ psychological well-being in subsequent visits (Hashash et al., 2019).
It is important to note that the present approach to modelling the progression of IBD symptoms to suicide risk was primarily psychologically based. Variables such as shame and depressive symptoms were represented as secondary reactions to IBD symptom activity in a cross-sectional model. However, it is not known definitively whether biomedical variables precede psychosocial variables. Indeed, IBD activity and mood have a bidirectional relationship (Gracie et al., 2018). For example, Crohn’s disease patients with active disease are particularly susceptible to comorbid depressive symptoms, suggesting disease activity is a risk factor for depression (Geiss et al., 2018). However, another study found that IBD patients who were depressed at baseline were at a significantly greater risk for more aggressive disease, and developed more aggressive disease significantly sooner, than did patients who were not depressed (Kochar et al., 2018). Irrespective of the sequence of risk factors, IBD management should move towards an approach that integrates managing disease activity and psychological well-being concurrently. Clinical interventions in IBD patients with high risk of suicide should target psychosocial predictors of suicidal behaviour (i.e. shame, depressive symptoms, hopelessness) to mitigate their downstream effects. Psychological interventions, such as cognitive-behavioural therapy and mindfulness-based interventions, are effective treatments for reducing psychological distress in individuals with IBD (Gracie et al., 2017; Neilson et al., 2015).
Limitations and future directions
This study has several limitations. First, homogeneity of the current sample makes it difficult to generalize the findings to other ethnic and cultural groups. A related limitation affecting generalizability is self-selection bias associated with membership in support groups and participation in online studies (Keiding and Louis, 2018). Membership in support groups can be a powerful resource for individuals living with chronic health conditions (Davison et al., 2000). Indeed, one of the key reasons why IBD patients choose to participate in support groups, both in-person and online, is to connect with others who are in a similar situation, to have an opportunity to share illness experiences, and to learn from how others have coped (Coulson, 2013). Therefore, the current sample may have self-selected for individuals who are generally more distressed and seeking support, given that members of support groups for other chronic illnesses report these reasons (Voerman et al., 2007). However, this study did not collect information about participants’ physiological or psychological comorbidities or whether participants were receiving any treatment (IBD-related and/or other). Thus, reasons for seeking support may not be due to IBD-specific distress and the influence of other variables on suicide risk cannot be excluded in the present sample. Finally, given that this study is cross sectional, temporal associations between the variables in the present model cannot be established.
However, this novel study can encourage future research that further explores the predictive ability of the present model in larger, more diverse samples and at multiple timepoints, as risk factors of suicide may not be static constructs that easily can be captured with a single assessment. Measurements taken at varying lengths (e.g. 1 week, 6 months, 1 year) may be important avenues of potential research. To address the potential influence of physiological and psychological comorbidities, future research should examine other predictors of suicidal behaviour not included in this study. For example, adverse childhood experiences (e.g. physical, sexual, and emotional abuse, as well as neglect) consistently are associated with suicidal behaviour, and may prove to be unique in their prediction of suicide risk among individuals with IBD (Zatti et al., 2017).
Moreover, IBD can be a context used to model suicide risk in other chronic illnesses, including other gastrointestinal conditions (e.g. irritable bowel syndrome, gastroesophageal reflux disease, Celiac disease) that may be accompanied by abdominal pain. The present model and findings may be able to generalize to other chronic illnesses as experiences of psychosocial variables (e.g. shame, depression, hopelessness) in this study are not limited to individuals with IBD. Although the actual symptoms that initiate the development of suicide risk may be different for different illnesses, the general model may hold.
In conclusion, this study revealed alarming rates of suicide risk, indicating a concerning general trend in IBD populations worldwide. The present model of the progression of IBD symptoms to suicide risk highlights the importance for routine screening of suicide risk and associated predictors in IBD patients, as well as the need for early intervention in patients at-risk for suicide. Overall, the results of this study introduce variables such as psychache and perceptions of being a burden into the IBD literature and provide new IBD management targets for suicidal behaviour.
Supplemental Material
Supplemental_Figure_A – Supplemental material for Modelling symptoms to suicide risk in individuals with inflammatory bowel disease
Supplemental material, Supplemental_Figure_A for Modelling symptoms to suicide risk in individuals with inflammatory bowel disease by Valentina Mihajlovic, Dean A Tripp and Jill A Jacobson in Journal of Health Psychology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.