
Abstract
Utilizing data from the nationally representative China Health and Retirement Longitudinal Study, this study analyzed the effect of intensity and duration of adverse childhood experiences on depression in middle aged and older aged adults in China. The mediating effect of cumulative health risk and personal factors were validated through the Karlson–Holm–Breen method. The results showed a significant dose-response relationship between adverse childhood experiences and adult depression. The elevated health risks of chronic diseases, disabilities, and physical pain, as well as the disadvantages in education, employment, and economic status caused by the adverse childhood experiences indirectly worsen adult depression.
Keywords
Introduction
Depression is one of the most common mental illnesses among the middle and old aged, and a large contributor to morbidity and mortality. Although the cause of depression has not yet been fully clarified, psychological research has confirmed that adverse childhood experiences (ACE) not only negatively impacts individuals’ mental health in adolescence, but can persist into adulthood (Collishaw et al., 2007; McLaughlin et al., 2012). The life span of the individual is intimately interwoven with macro-historical events and the micro-family incidents. The middle aged and old aged in China are no strangers to the ACE compared to those in Western countries. Individuals in China aged over 40 years old lived through periods of disadvantage during their childhood when their material standard of living hovered at a low level for a long time, punctuated by intensive periods of extreme hardship due to famine, war, and political revolution. Also, traditional Chinese culture and beliefs in many families encouraged harsh parenting behaviors, including corporal punishment, as a common feature of normal discipline (Chao, 1994; Simons et al., 2000).
The 1995–1997 CDC-Kaiser Permanente Adverse Childhood Experiences Study was one the largest investigations of childhood insults and later-life health and well-being (Felitti et al., 1998). Research has confirmed that ACE, such as physical abuse, sexual abuse, emotional, or psychological abuse and neglect, can have a profound negative impact on mental disorders (Edwards et al., 2003; Gilbert et al., 2009; Merrick et al., 2017; Mwachofi et al., 2020), and are the common origin of various mental illnesses (Kessler, 1997). As one of the most common psychiatric disorders, the relationship between depression and ACE has been the focus of recent research. Partial studies explored the impact of ACE on adult depression from a single dimension, such as childhood maltreatment (Hou et al., 2020) and early parental loss (Høeg et al., 2017). However, multiple ACE often occurred simultaneously (Edwards et al., 2003; Finkelhor et al., 2007), and analyses of single ACE may overestimate their impact. In response, a growing body of studies has shifted from single forms of ACE to cumulative exposure to ACE, indicating that there is a dose-response effect of ACE, or the greater the number of ACE, the more likely it is to increase the risk of depression in adulthood (Afifi et al., 2008; Chapman et al., 2004; Trauelsen et al., 2015).
While there is considerable evidence of a relationship between ACE and depression in adulthood, what remains less clear are the moderators and mediating mechanisms underlying the ACE—depression association (McLaughlin, 2016). Relational resilience (Howell et al., 2020), and emotion regulation (John et al., 2017) were perceived to mediate the effects of ACE on depression, through the individual’s ability to cope with subsequent stressful events and to handle their emotions. In addition, studies have explored possible mediating mechanisms from a biological perspective (Heim et al., 2008; Lupien et al., 2009). The results suggested that ACE resulting in chronic exposure to stress lead to changes in stress response, and that this sustained stress response altered the hypothalamic-pituitary-adrenal axis, culminating in the production of glucocorticoids, which leads to an impact on brain structures involved in mental health (Heim et al., 2008; Lupien et al., 2009).
Second, while associations between ACE and depression in adulthood are well documented in the literature, these studies have been conducted cover a relatively short life course, mostly focusing on the adolescent or mid-life years. Few ACE—depression studies have addressed the long-term effects of ACE on geriatric depression (Ege et al., 2015), where the duration of exposure to ACE may lead to a gradient of subsequent adverse effects (George, 2014). Much attention has been paid to the cumulative types of ACE, but much less attention has been directed to the cumulative persistence of ACE in the time dimension.
Finally, previous studies have tended to focus on outcome variables. The absence of pathways analysis leaves a critical piece of the puzzle missing in the understanding of the long arm effect of ACE. Although some studies have tentatively proposed possible pathways from a theoretical perspective (Liu, 2017), whether these pathways hold true, and the corresponding magnitudes of influence, remain ambiguous, awaiting plausible explanations, and empirical validation.
Considering the prevalence of ACE and their possible impact on depression in middle and old age, we ask the following questions: for Chinese middle aged and older adults, does the cumulative exposure, or intensity, and the duration of exposure to ACE increase the likelihood of depression?; if so, is there cohort heterogeneity due to age of respondents in the above effects?; and what are the possible pathway or mediation factors between ACE and depression in adulthood? Our research makes the following contributions to the literature. First, we extended the influence of adverse childhood experiences on depression to the older aged. Second, we not only focus on the intensity, or cumulative exposure of childhood adversities, but also incorporate their duration, covering the persistence of exposure to childhood adversities. Third, we validated some of the possible pathway and their corresponding magnitudes of ACE on depression in adulthood.
Theoretical analysis and research hypotheses
The formulation of life course theory provides a direct theoretical basis for understanding the long-term effects of ACE (Elder, 1998; O’Rand, 1996). ACE are a series of cumulative deleterious stressors developed during childhood that over a person’s life course evidences risk factors threatening a person’s mental health (Nurius et al., 2015). The elevated cumulative exposure, or intensity, of ACE and duration of ACE, measured by the duration of childhood starvation, reflect the initial adversities stress potential, and the higher and longer the initial stress potential, the more likely it is to lead to depression in adulthood, thus creating a “dose-response” effect. We hypothesize:
Hypothesis 1a: The higher the intensity of ACE, the higher the likelihood of depression in adulthood, which confirms the “dose-response” effect of the cumulative exposure to ACE on depression.
Hypothesis 1b: The longer the duration of the childhood starvation, the higher the likelihood of adult depression, which confirms the “dose-response” effect of the duration of ACE on depression.
In terms of general health risks (Ferraro et al., 2016; Hughes et al., 2017; Nurius et al., 2019), studies have demonstrated the cumulative impact of ACE increase the individual’s risk of suffering from later life chronic diseases (Chanlongbutra et al., 2018; Espeleta et al., 2020). For example, an adverse childhood experience gradient has been shown with regard to lung cancer (Brown et al., 2009), heart attack (O’Rand and Hamil-Luker, 2005), chronic obstructive pulmonary disease (Anda et al., 2008), chronic pain (Goosby, 2013), and premature death during adulthood (Brown et al., 2009). With regard to personal development, a small but burgeoning number of studies link ACE to educational attainment, employment, and income. For example, children exposed to ACE are at increased risk of lower educational attainment (Blodgett and Lanigan, 2018; Crouch et al., 2019) and ACE, such as abuse, neglect, and violence, can negatively affect adult employment status (McDonough et al., 2015; Sansone et al., 2012). This empirical evidence suggests that ACE reinforce the accumulation of later life adversities, such as health risks and developmental disruptions, magnifying the negative consequences of ACE. Therefore, we formulate the following hypotheses:
Hypothesis 2a: The greater the intensity of ACE, the greater the impact on the accumulation of health risks and personal development, which confirms the cumulative disadvantage effect of exposure to ACE.
Hypothesis 2b: The longer the duration of the childhood starvation, the greater the impact on the accumulation of health risk and personal development, which confirms the cumulative disadvantage effect of the duration of ACE.
Previous research documents that the early life exposure to ACE leads to negative impacts on future life development through what is often referenced as pathway dependence, in which ACE indirectly affect mental health through the intervening health and socioeconomic conditions they engender (Goosby, 2013; Hayward and Gorman, 2004; Walsemann et al., 2008). Health risk factors, such as chronic disease, physical disability, and chronic pain, have been generally recognized as contributing factors to depression. These chronic disease-associated stressors threaten patients’ ability to maintain emotional balance, thus eliciting a higher risk for depression (Bisschop et al., 2004; Huang et al., 2010). Analogously, physical disability was found to be a risk factor for depression (da Silva et al., 2011; Lenze et al., 2001) and a growing clinical and gerontological literature argues that depression is strongly associate with chronic pain (Bierman, 2011; Gureje et al., 2008).
ACE impact personal development through socioeconomic factors, such as education, employment, and material well-being in adulthood, which, in turn, is significantly associated with an increased risk of mental disorders (Kivimäki et al., 2020; Lorant et al., 2003). Education is perceived as central to the process of cumulative disadvantage because it is a determinant of subsequent outcomes throughout an individual’s life course (Pallas, 2003). There is a clear inverse association between educational attainment and depression (Ladin, 2008). Further, employment status can predict depressive symptoms (Dooley et al., 2000; Mossakowski, 2009) and, at the individual level, fewer material assets were associated with increased odds of depression (Rai et al., 2013). Based on the cumulative disadvantage hypothesis and existing research, it can be assumed that the mechanisms by which ACE influence depression in adulthood throughout the life course may be mediated through both health risks and personal development. The following hypotheses follow:
Hypothesis 3a: Compared to those without ACE, those with ACE suffered from higher cumulative health risks (chronic diseases, disability, and physical pain), and these differences partly explain the difference in depressive status.
Hypothesis 3b: Compared to those without ACE, those with ACE suffered from higher risks of personal development disruptions (educational attainment, non-farm employment, family asset status), and these differences partly explain the difference in depressive status.
Data and methodology
Data
We utilize data from the China Health and Retirement Longitudinal Study (CHARLS) of 2014 and 2015, which was conducted by the Institute of Social Science Survey, Peking University. The data contain basic information about individuals and family members, including health status, employment, income, consumption, and assets. CHARLS2014, the life course survey of middle aged and old aged people in China, systematically reviewed respondents’ life span information, including data on demographic background, family information, education history, and health history. We matched CHARLS2015 with CHARLS2014 to obtain information on the ACE of respondents. The data filters excluded cases older than 80 and younger than 40 and missing values on dependent variables and independent variables, yielding a sample of 11,639 observations.
Variables
Dependent variable
The dependent variable was depression, assessed by the Short Form of the Center for Epidemiologic Studies Depression Scale (CES-D 10-SF). The CES-D 10-SF, a simplified version of the CES-D scale for measuring and rating depressive symptoms, is based on asking the respondents 10 relevant questions. Each question provides four options: rarely or none of the time (<1 day), some or a little of the time (1–2 days), occasionally or a moderate amount of the time (3–4 days), most or all of the time (5–7 days). For negative questions, such as “I felt depressed,” the four options are assigned a score of 0, 1, 2, and 3. For positive questions, such as “I was happy,” then the four options are assigned a reverse order score. The score of CES-D 10-SF has a range of values from 0 to 30. A score equal to or greater than 10 on the CES-D-SF scale is defined as the presence of depressive symptoms, while a score less than 10 indicates the absence of depression (Andresen et al., 1994). The Cronbach’s alpha for the CES-D 10-SF items was 0.795, with a relatively high internal consistency.
Independent variable
ACE are a series of potentially traumatic, out of the child’s control exposures that occur during childhood, including starvation, abuse, neglect, and household dysfunction (Felitti et al., 1998). We focus on the intensity of ACE and duration of childhood starvation on adult depression. Intensity refers to the cumulative effects of ACE, and duration is the length of exposure to ACE, which negatively affects an individual’s mental health, according to a dose-response relationship (Costello, 2016). We assess the long-term effects of traumatic stress during childhood, measured by the ACE intensity score and duration of childhood starvation score, on later life depression. Consistent with existing studies of childhood misadventures (Felitti et al., 1998) and specific to the behavior in Chinese families, we selected eight different types of ACE: starvation; relative poverty; premature death of parents; parents who were bedridden, severely disabled, or mentally disordered; parents who quarreled frequently; parents who divorced; and often scolded by parents or bullied by neighborhood children. The values were set to 1 when an ACE was present and 0 otherwise, with the aggregate ACE intensity score ranging between 0 and 8. Considering that the proportion of experiencing five or more ACE was very small (only 1.17%), with references to Felitti et al. (1998) and Sonu et al. (2019), we assign four or more ACE as the highest ACE intensity.
CHARLS2014 did not ask about the duration of each ACE. Referring to Shi and Wu (2018), we choose the duration of childhood starvation as a proxy variable for the ACE exposure duration. We imputed duration by using the multiple-choice questions on the 0–5 years old, 6–12 years old, and 13–17 years old age ranges during which childhood starvation might be experienced. To measure starvation duration, we set the starvation value to 1 for each age period during which starvation was experienced, ranging from 0 (no starvation) to 3 (starvation during all three age ranges).
Control variables
To capture the net effect of ACE on adult depression, we collected basic personal data, including demographic characteristics and socioeconomic and family characteristics as control variables. Demographic variables included age (continuous variable), sex (male = 1, female = 0), and marital status (married and living with spouse = 1, otherwise = 0). Socioeconomic and family variables included the father’s education (father not formally educated = 1, otherwise = 0), the mother’s education (mother not formally educated = 1, otherwise = 0), father’s occupation at age 17 (non-agricultural = 1, otherwise = 0), the number of siblings (continuous variable), residence environment (very clean/relatively clean = 1, otherwise = 0).
Mediator variables
We examined health risks and personal development as mediator variables. Health risks were the total number of chronic diseases, disabilities (physical disabilities, brain damage, mental retardation, vision problem, hearing problem, and speech impediment = 1, otherwise = 0), and physical pain (often troubled by body pains = 1, otherwise = 0). Personal development was measured by years of school attainment (illiteracy = 0, primary school = 6, middle school = 9, high school = 12, technical secondary school = 11, junior college student = 14, undergraduate = 16, master = 19, doctor = 22), nonfarm employment (longest working job was nonfarm = 1, otherwise = 0), and household asset status (proxied by owned a car or air conditioner = 1, otherwise = 0).
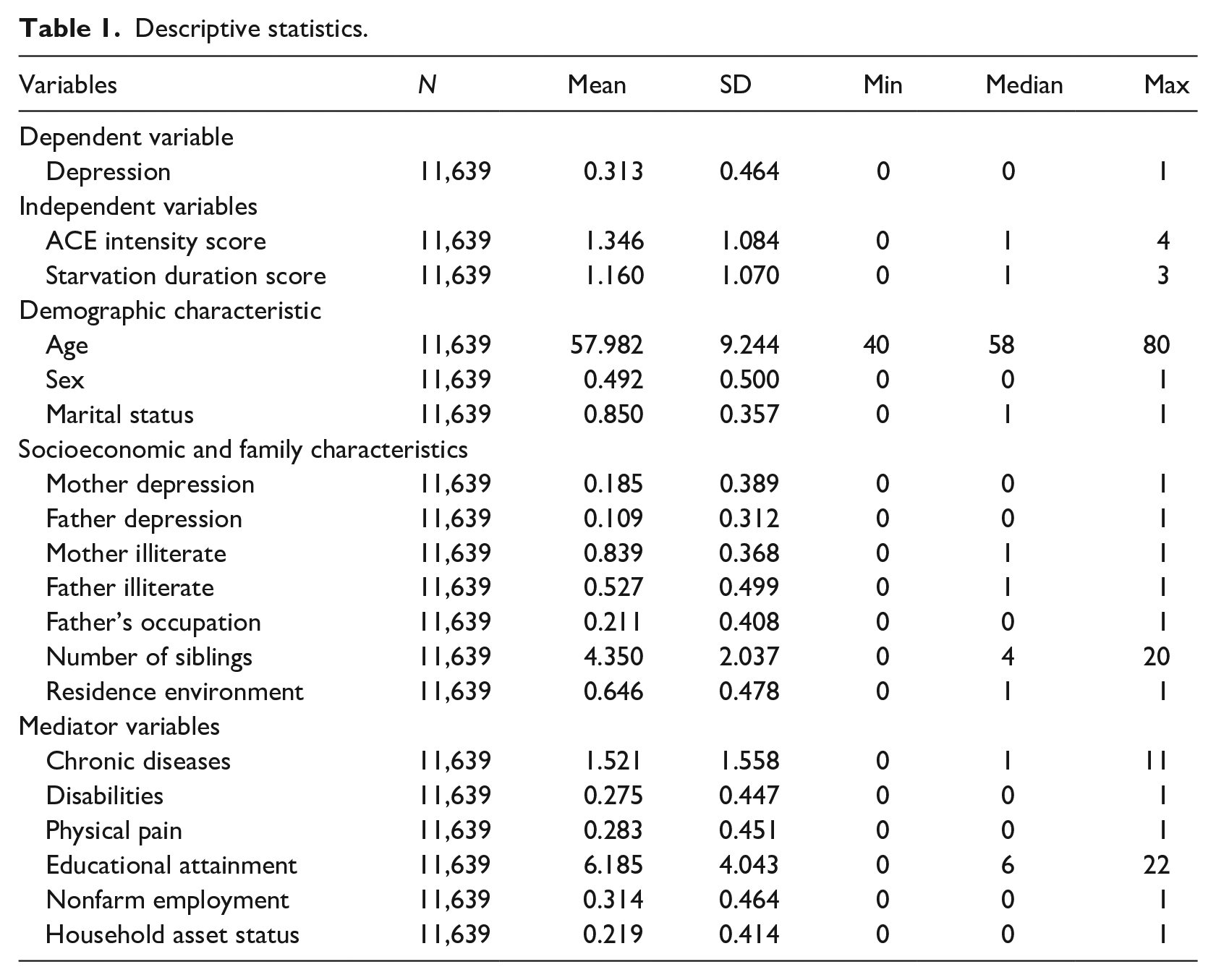
Table 1 displays the descriptive statistics for all variables. About one-third (31.3%) of the respondents suffered from depression (SD = 0.464). Respondents experienced an average of 1.346 ACE (SD = 1.084, range 1–4) and 1.160 of the three age groups of childhood starvation (SD = 1.070, range 1–3). In terms of control variables, the mean age of the respondent was 58 years old (SD = 9.244, range 40–80); 49.2% of the respondent were male; and the proportion of respondents married was 85% (SD = 0.357). With respect to socioeconomic and family characteristics, the percentage of respondents’ mothers who exhibited depression or sadness was 18.5% (SD = 0.389), higher than the percentage of respondents’ fathers (10.9%; SD = 0.312). The proportion of fathers with no formal education (52.7%; SD = 0.499) was significantly lower than the proportion of mothers with no formal education (83.9%; SD = 0.368). The proportion of respondents whose fathers were engaged in non-agriculture work was 21.1% (SD = 0.408); respondents had 4.35 sibling on average (SD = 2.037, range 0–20); and 64.6% (SD = 0.478) of the respondents lived in a very/relatively clean place during their childhood. In terms of mediation variables, the mean number of chronic diseases was 1.521 (SD = 1.558, range 1–11); the percentage of those suffering from physical disability was 27.5% (SD = 0.447); and 28.3% (SD = 0.451) suffered physical pain. The average years of education of the respondents was 6.185 (SD = 4.043, range 0–22); the proportion of respondents in nonfarm employment was 31.4% (SD = 0.464); and 21.9% of respondents owned a car or air-conditioned their house (SD = 0.414).
Descriptive statistics.
Empirical method
Since depression was a bicategorical discrete variable, a logit model was specified:

where ACE is the ACE score or duration of childhood starvation,
We estimated our nonlinear mediation effects model by utilizing the Karlson–Holm–Breen (KHB) method that decomposed the “confounding” and “rescaling” effects (Breen et al., 2013). The confounding effect represents the change in coefficients due to the change in total variance with the addition of a control variable, and the rescaling effect represents the effect of the addition of the mediating variables on the independent variable. This method not only decomposes the nonlinear probability model, but also allows multiple mediating variables to be introduced into the model simultaneously.
Statistical analysis was performed using STATA15.0. All the de-identified individual participant data in this study can be freely accessed for study. All individual participant data collected during the course of the study, after de-identification, can be shared immediately after publication, with no end date. Study Protocols, Statistical Analysis Plans, and Analytic Code are also available to anyone who wishes to access the data for study. These data are available at http://charls.pku.edu.cn/.
Results
Bivariate relationship among key variables
Table 2 displays the bivariate correlation analyses between predictor, mediators, and outcome variables, with Pearson and Spearman correlation coefficients similar. We take the results of Pearson correlation coefficient in Table 2 as an example. First, the ACE score (
Bivariate correlations among variables.
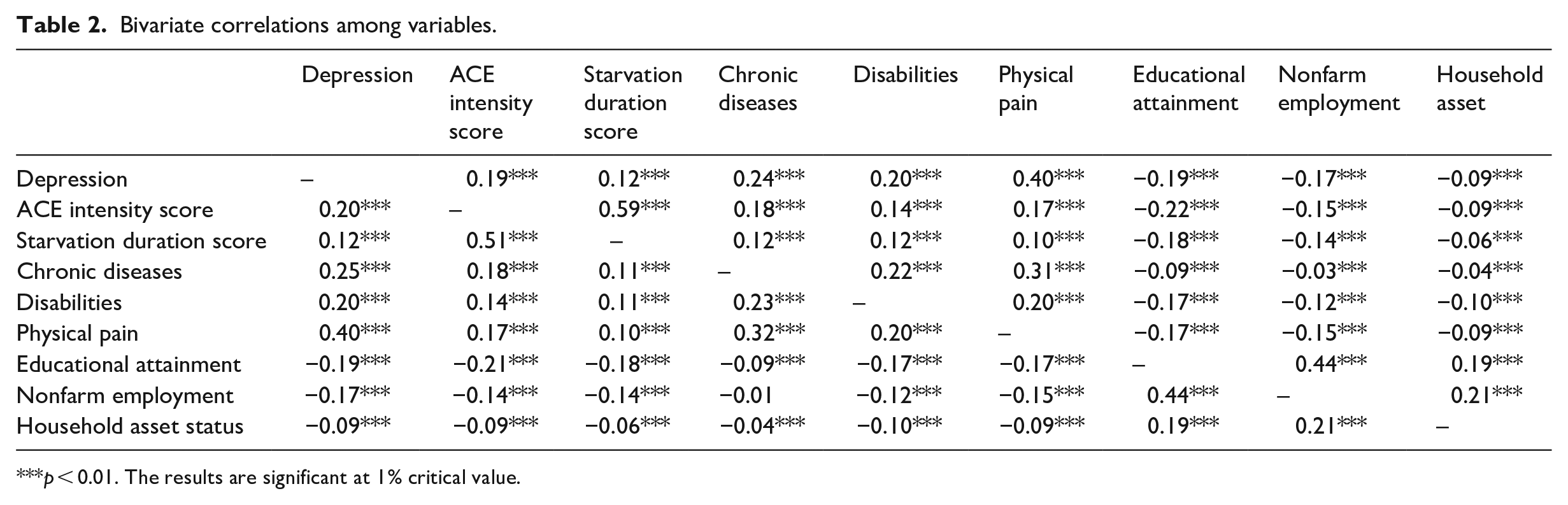
p < 0.01. The results are significant at 1% critical value.
The impact of adverse childhood experiences on depression
Treating ACE as a continuous variable, Model 1 ACE intensity score and Model 3 starvation duration score in Table 3 show that after controlling for socioeconomic, family, and demographic characteristics, ACE had a significant positive effect on depression in adulthood. The models show that ACE intensity (the more adversities experienced in early life), or the longer the duration of starvation, the higher the probability of depression in adulthood. The odds ratio indicate that for each increase in the ACE score, the odds ratio of depression in adulthood increased by 32.8% on average and for each increase in the duration of childhood starvation, the odds ratio of depression in adulthood increased by 18.5% on average.
The effect of ACE on depression in adulthood.
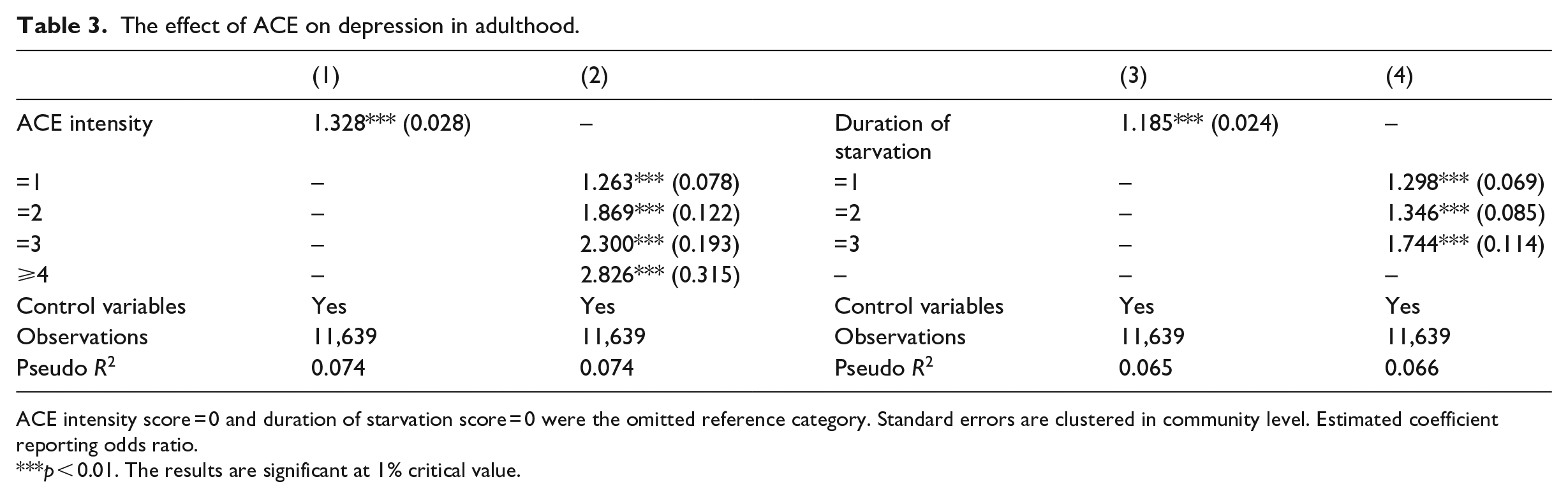
ACE intensity score = 0 and duration of starvation score = 0 were the omitted reference category. Standard errors are clustered in community level. Estimated coefficient reporting odds ratio.
p < 0.01. The results are significant at 1% critical value.
Models 2 and 4 in Table 3 regarded the ACE intensity score and the duration of starvation score as categorical variables. As the ACE intensity score and starvation duration score increased, the results showed a gradient increase in the effect of the ACE and starvation duration on depression. Experiencing one ACE increased the odds ratio of depression in adulthood by 26.3%, two ACE by 86.9%, three ACE by 130.0%, and four or more ACE by 182.6%. Experiencing childhood starvation in one age group increased the odds of depression in adulthood by 29.8%, by 34.6% when suffering childhood starvation in two age groups and by 74.4% when suffering starvation in all three age groups compared to individuals who did not experience childhood starvation.
Regardless of whether the ACE intensity and the duration of starvation are considered as continuous or categorical variables, the above results indicate that as ACE intensity and the duration of starvation increased, a stressful accumulation of adversities occurred, exhibiting a significant graded dose-response relationship. Hypothesis 1a and Hypothesis 1b are supported.
The mediation effect of ACE on depression
Did early life adversities work with later life factors to cumulatively and interactively influence respondents’ depression status? We verified the existence and extent of mediation effects in two steps. First, we estimated the effect of the intensity of ACE and duration of starvation on the mediator variables to test whether ACE had a cumulative adverse effect on the mediator variables. Second, we employed the KHB method to estimate the mediator variables decomposition effects of ACE on depression and to test whether ACE contributed to new disadvantages that indirectly affect depression in adulthood.
Panel A in Table 4 indicates the effects of ACE intensity scores on the mediator variables and Panel B the effects of the duration of starvation on the mediator variables. The results revealed that both the ACE intensity score and the duration of childhood starvation significantly increased the likelihood of chronic disease, physical disability, and physical pain in adulthood, while significantly reducing years of school attainment and family asset status and weakening the probability of nonfarm employment. Further, the greater the ACE intensity and the longer the duration of starvation, the greater the effect on the above mediator variables. These results demonstrated that ACE worsen physical health in adulthood and inhibited personal socioeconomic advancement, resulting in a cumulative disadvantage, supporting Hypothesis 2a and Hypothesis 2b.
The effect of ACE intensity and starvation duration on mediator variables.
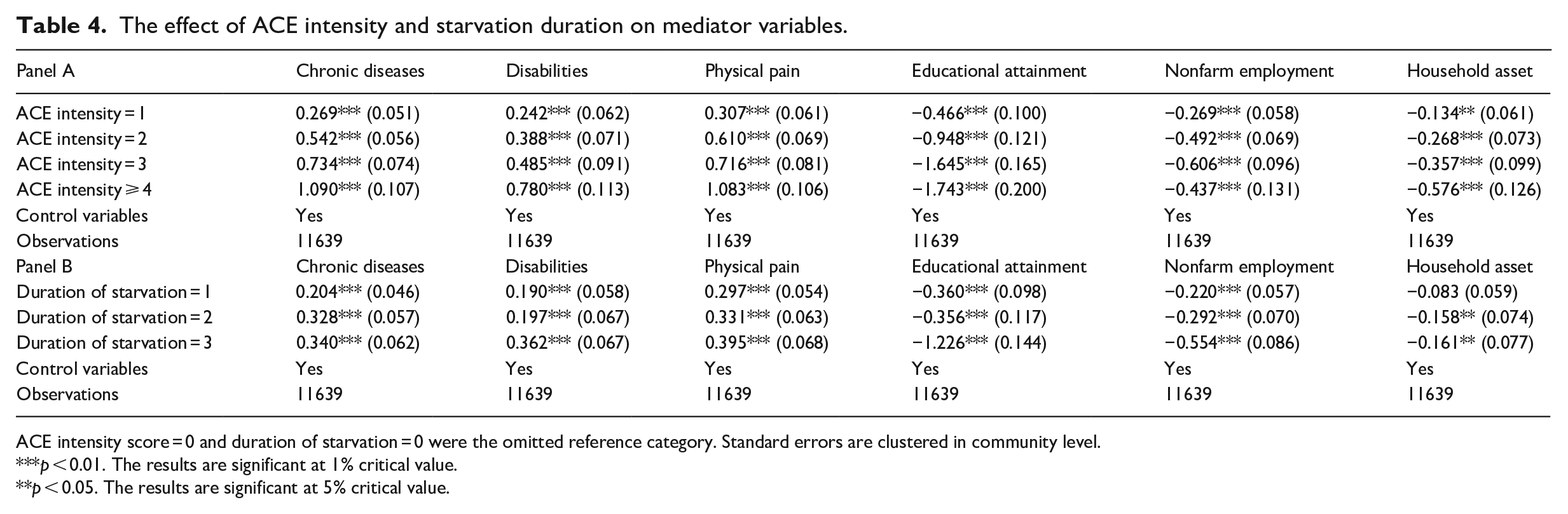
ACE intensity score = 0 and duration of starvation = 0 were the omitted reference category. Standard errors are clustered in community level.
p < 0.01. The results are significant at 1% critical value.
p < 0.05. The results are significant at 5% critical value.
The impact of ACE on depression is partly caused by the cumulative disadvantage of the stress transmission processes. Based on the evidence of the cumulative effect of ACE, we utilized the KHB method to analyze the channel effects of six mediating variables. Table 5 shows that the channel effect of ACE intensity on depression was 47.1%, while the channel effect of the duration of childhood starvation on depression was 42.2%. Each of the mediator variables was statistically significant, suggesting that all of these mediator variables were significant pathways for ACE to influence depression in adulthood. Specifically, the number of chronic diseases explained 19.2% of the intensity effect of ACE and 13.5% of the duration of childhood starvation effect on depression in adulthood. The explanatory power of physical disability explained 9.0% of the ACE intensity effect and 9.3% on the duration effect; physical pain was 27.5% and 21.7%; years of school attainment was 8.9% and 11.2%; non-farm employment was 5.9% and 10.1%; and family asset situation was 2.7% of the intensity effect of ACE and 2.2% of the duration effect. Supporting hypothesis 3a and 3b, these results show that ACE leads to health deterioration and disruptions in personal development in later life, contributing to an increased likelihood of depression in adulthood. The pathway is shown in Figures 1 and 2.
Decomposition of channel effects of ACE on depression.
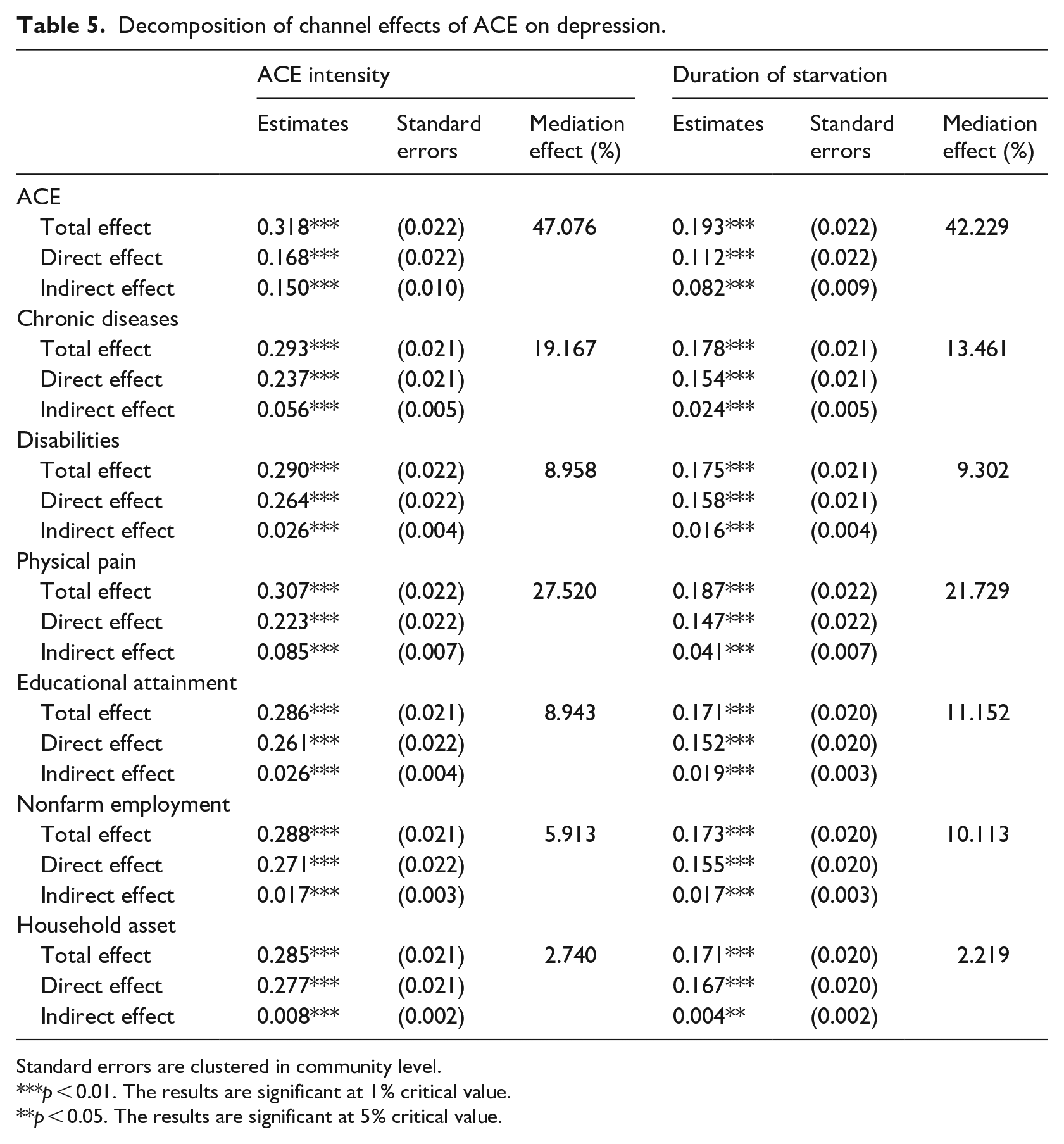
Standard errors are clustered in community level.
p < 0.01. The results are significant at 1% critical value.
p < 0.05. The results are significant at 5% critical value.
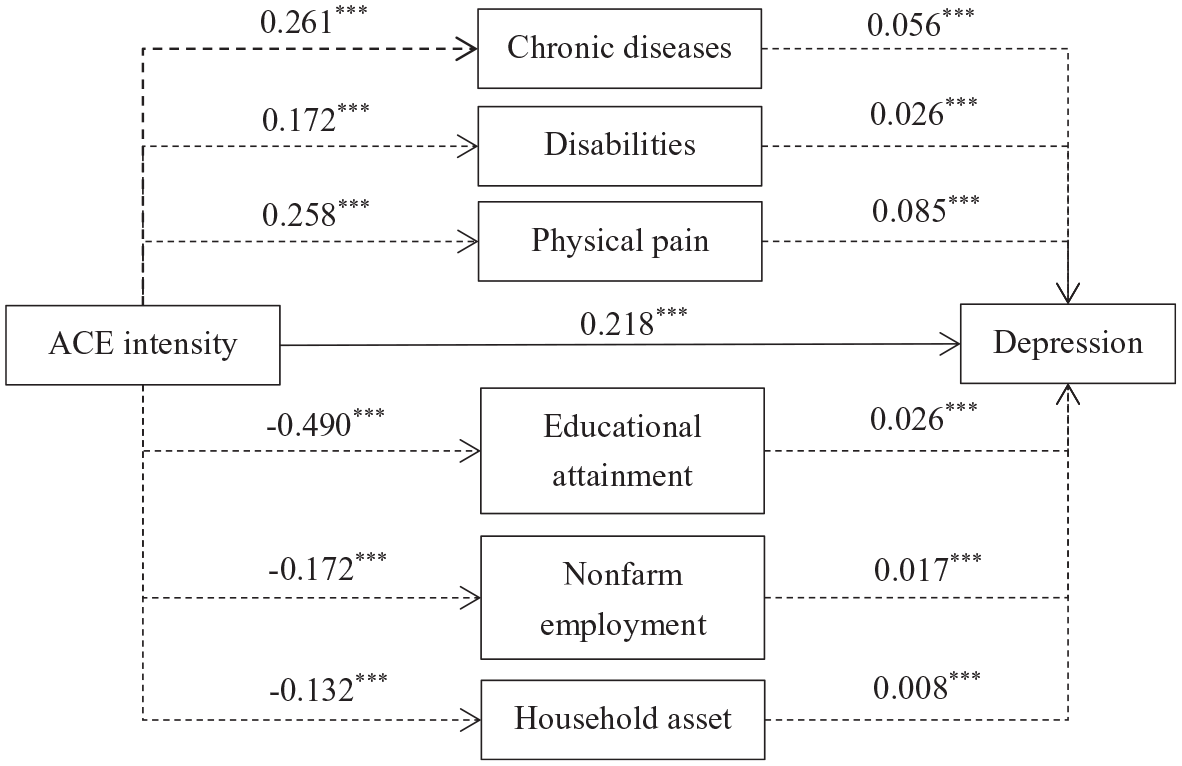
The influence mechanism of the ACE intensity core on depression.
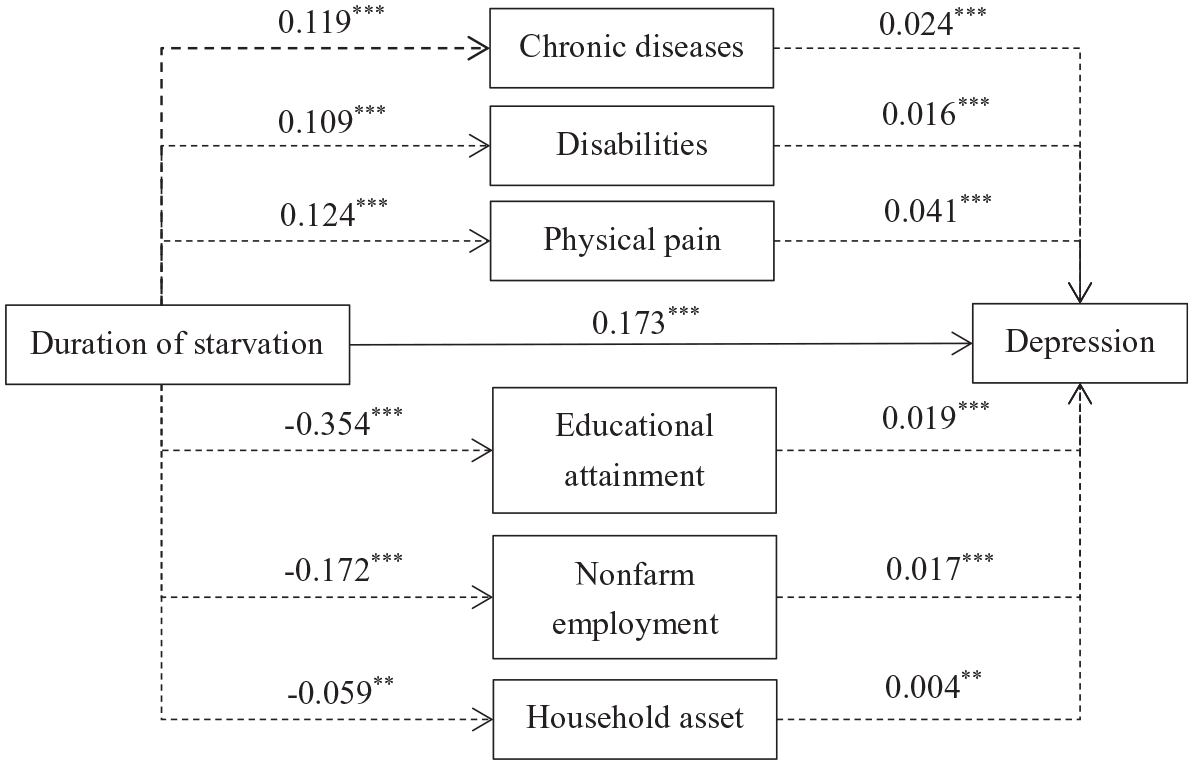
The influence mechanism of the duration of starvation on depression.
Heterogeneity analysis: Age effects
To consider cohort differences, we divided the sample into middle age and old age groups to observe any age-group differences in the effects of ACE on depression. The existence of differences across groups depends on the magnitude and level of significance of the coefficient estimated. However, a straightforward comparison of the coefficient estimated is not an accurate way to assess whether the above differences are significant or not, because the confidence intervals may overlap due to the existence of coefficient interval estimates. Referring to Cleary (1999), we use simulation evidence to calculate empirical p-values and thus determining the significance of observed differences in coefficient estimates.
Table 6 reports the cohort effects and the significance of the differences. Subgroup regression results continued to show a significant gradient effect of ACE on depression in both the middle aged and the old aged. The empirical p-values were obtained by bootstrapping 1000 times. Coefficient of difference tests showed that for the ACE intensity scores less than or equal to 3, the estimated coefficients were significantly higher for the old age group than for the middle age group. However, when the number of ACE intensity score was 4 or more, the effect of ACE on depression in adulthood was not significantly different between the middle age and the old age groups. The effect of duration of childhood starvation did not demonstrate significant differences between the middle age group and the old age group.
Difference between middle-aged and elderly in the effect of ACE on depression.
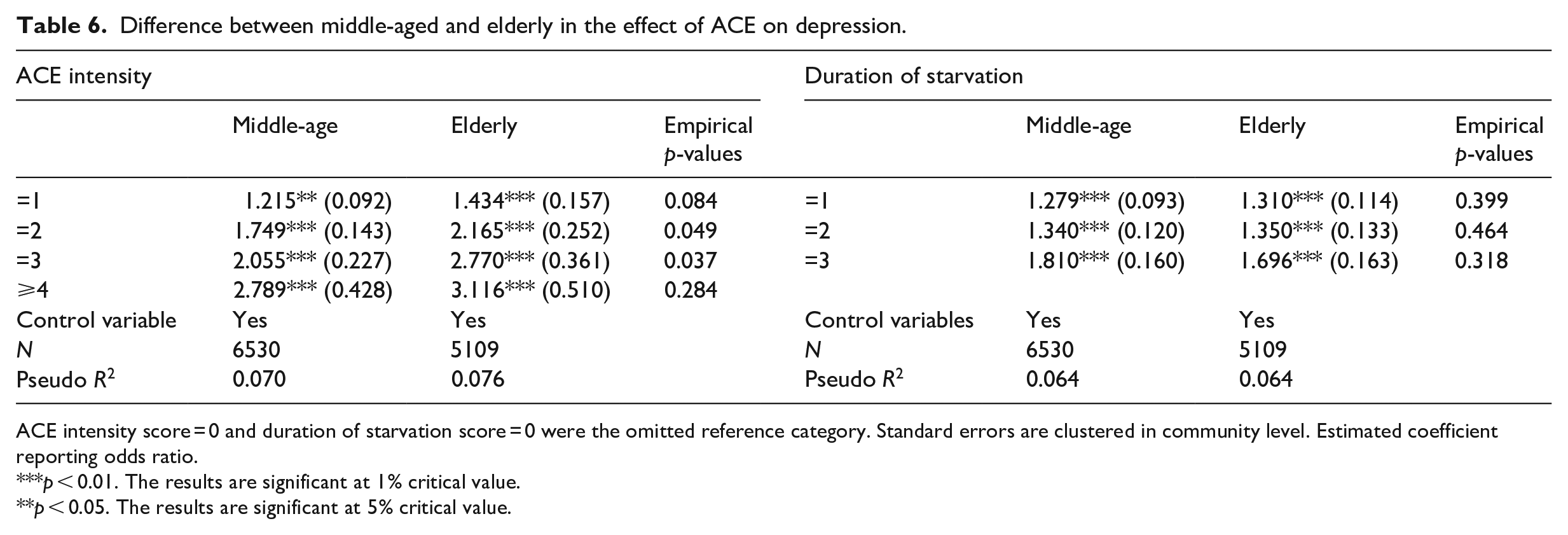
ACE intensity score = 0 and duration of starvation score = 0 were the omitted reference category. Standard errors are clustered in community level. Estimated coefficient reporting odds ratio.
p < 0.01. The results are significant at 1% critical value.
p < 0.05. The results are significant at 5% critical value.
Discussion
ACE are traumatic and stressful events in an individual’s early life course. We utilized nationally representative data to assess the impact of ACE on adult depression. Considering that ACE often occur in conjunction with each other, it is necessary to examine adversities from the perspective of ACE’s cumulative exposure, or intensity, and duration in order to understand their long-term effects on adult mental health. The intensity of ACE was measured by the accumulated value of the ACE and the duration of ACE was measured by the duration of childhood starvation to provide both an ACE quantitative dimension and temporal dimension. Limited by the routine collection of secondary data, previous studies have been generally unable to assess the impact of the intensity and duration of ACE on adult mental health. The results in Table 3 indicated that as the intensity of ACE increased, the odds ratio of suffering from depression in adulthood also increased. Compared to individuals with no ACE, individuals experiencing one ACE increased the odds of depression in adulthood 1.263 times; two ACE increased the odds 1.869 times; three ACE increased the odds 2.3 times; and more than three ACE increased the odds 2.826 times. These findings are consistent with a pronounced dose-response association between ACE intensity and adult depression (Afifi et al., 2008; Anda et al., 2002; Chapman et al., 2004; Trauelsen et al., 2015).
It is important to note that some of the middle age and older respondents in the sample may have experienced the 1959–1961 Chinese Great Famine. Although differential effects of exposure to the Chinese Great Famine at different early-life stage on depressive symptoms in late adulthood have been documented (Li et al., 2018), long-term extreme food shortages, like the Chinese Great Famine, may overestimate the impact of starvation on depression in late life. Rather than focusing only on extreme starvation experiences, such as the Great Famine, we extended the study of the effects of childhood starvation on adult depression by including relatively milder experiences of starvation over each respondent’s early life-time. Experiencing starvation during one age category, increased the odds of depression 1.298 times; during two age categories by 1.346 times and during all three age categories by 1.744 times compared to individuals who did not experience childhood starvation. Our results confirmed George (2014) duration of exposure hypothesis, which proposed that the longer an individual experiences adversity, the more likely it is to result in an adverse outcome.
Most ACE studies have concentrated on the effects of ACE on adolescents or middle age adults. We extended the long arm of childhood ACE to the old aged. The estimation results for the old aged subsample indicated a significant association between ACE and depression in older adults, which aligns with previous research that identified ACE as risk factors for geriatric depression (Ege et al., 2015; Roh et al., 2015). Although the elderly were a high prevalence depression group, we found that in some cases there was no significant difference between the middle aged and old aged. Compared to individuals without ACE, the odds ratio for the effect of ACE on depression in the old aged was significantly higher when the intensity of ACE was less than four. However, this significant difference vanished when ACE intensity was greater than or equal to four. This suggests that exposure to severe ACE channeled deeply into individuals’ life course, with individuals remaining under the influence of misadventure for a sustained period of time. When it comes to childhood starvation, there was no significant difference in its effect on depression between middle age and the old age.
An important contribution of the paper, but also a challenging one, was to understand and validate the pathway underlying the association between ACE and depression in adulthood. Our results supported our hypotheses that ACE exerted a long-term effect on adult depression through the spread of cumulative disadvantage in adulthood. ACE are a collection of toxic stressors early in life that may act as catalysts for subsequent chain reactions of stress exposure and disparities in depressive outcomes (Nurius et al., 2015). This means that early life adversity sets the stage for subsequent stressor exposure, which leads to stress proliferation. Constructs of stress proliferation serve to join with ACE in a series of forms that influence adult depression independently and interactively (Alexopoulos, 2005), thus providing a foundation for a mechanism of the life course processes in which disadvantage accumulation occurs over time. Based on life course theory and the disadvantage accumulation hypothesis, our study is one of the few to directly validate the multiple pathways underlying the impact of ACE on adult depression. We found that cumulative disadvantage supported a pronounced cascade effect of ACE intensity and the duration of starvation on health risk accumulation and personal development. The greater the ACE intensity or duration of starvation the more likely a poorer health status, including number of chronic diseases, physical disability, and physical pain. The accumulation of disadvantages was also reflected in lower socioeconomic status, including less educational achievement, agricultural employment, and poorer household asset status, each of which collectively increased the risk of adult depression. We further verified whether the above mediator variables hold using the KHB method of mediating effect decomposition. We found that health status and socioeconomic and family variables in adulthood mediated the long-term effects of ACE on depression, which suggests a potential causal relationship between risk factors early in the life course and depression in adulthood based on the process of disadvantage accumulation.
We believe our study has important policy implications. Much of the research on adult depression has emphasized recent risk factors, but stressors early in the life can cast a long shadow over the onset of adult depression. Our findings highlight the necessity of focusing on and attenuating adult depression at its childhood origin. ACE reflect dysfunctions and insults during the early stages in the individual’s development. From a family policy perspective, effective family policies not only reduce the incidence of child maltreatment, but also help families develop positive and healthy child-rearing behaviors. However, current family support policies in China are weak and fragmented, mostly directed to emergency deficit repair, with little focus on the prevention of childhood insults and the development of a healthy upbringing (Peng and Hu, 2015). Future Chinese family policies should support the full development of family functions, not only focusing on vulnerable families and poverty reduction policies to avoid being trapped in a vicious cycle of poverty, but also by playing a preventive and developmental role, including increasing investments in family education and improving human and social capital to build safe, stable, and nurturing relationships. The government should strive to establish augmented health protection in the early period of the life cycle. For health intervention and protection early in the life course, the government should ensure registration with a family doctor, regular medical check-ups, targeted maternal and child protection programs, child nutrition programs, and disease prevention and control programs. Importantly, the government should establish additional mechanisms to detect, intervene and counsel abuse and bullying in childhood.
The paper has a number of limitations. The ACE score is a relatively crude measure of cumulative childhood stress exposure (Anda et al., 2020). The same is true for the duration of childhood starvation. Further, the values were based on self-reported retrospective survey data, which contain ACE derived from respondents’ recollections that may introduce recall bias. Future research should consider alternative measures of ACE. Some CHARLS data, such as economic status, was inadequate, which led to two durable goods measures, cars and air conditioners, as proxy variables. Finally, we validated possible mediating mechanisms and the extent of their magnitude on middle and old age depression, but other pathways of intervention between ACE and depression in adulthood should be clarified and validated in subsequent in-depth studies.
Conclusion
This study investigated the impact of the profound effects of adverse childhood experiences on depression in adulthood and verified the potential pathway based on life course theory and the accumulation of disadvantage hypothesis. The results showed that as the intensity of ACE increased, and the duration of childhood starvation extended, the odds ratio of developing depression in adulthood increased, showing a significant dose-response relationship. Heterogeneity analysis revealed no significant difference in the effect of ACE on depression in mid-life and older adults when individuals faced severe cumulative exposure or childhood starvation, but differences at lower ACE intensity scores. Mediating effects demonstrated that cumulative health risks and personal development factors mediated the long-term effects of ACE on adult depression. Our findings strongly suggest the need to prevent adult depression from early in the life course.
Research Data
sj-do-1-hpq-10.1177_13591053211037727 – Research Data for The long arm of childhood: The prolonged influence of adverse childhood experiences on depression during middle and old age in China
Research Data, sj-do-1-hpq-10.1177_13591053211037727 for The long arm of childhood: The prolonged influence of adverse childhood experiences on depression during middle and old age in China by Hao Chen, Qiuyan Fan, Stephen Nicholas and Elizabeth Maitland in Journal of Health Psychology
Research Data
sj-dta-2-hpq-10.1177_13591053211037727 – Research Data for The long arm of childhood: The prolonged influence of adverse childhood experiences on depression during middle and old age in China
Research Data, sj-dta-2-hpq-10.1177_13591053211037727 for The long arm of childhood: The prolonged influence of adverse childhood experiences on depression during middle and old age in China by Hao Chen, Qiuyan Fan, Stephen Nicholas and Elizabeth Maitland in Journal of Health Psychology
Research Data
sj-log-3-hpq-10.1177_13591053211037727 – Research Data for The long arm of childhood: The prolonged influence of adverse childhood experiences on depression during middle and old age in China
Research Data, sj-log-3-hpq-10.1177_13591053211037727 for The long arm of childhood: The prolonged influence of adverse childhood experiences on depression during middle and old age in China by Hao Chen, Qiuyan Fan, Stephen Nicholas and Elizabeth Maitland in Journal of Health Psychology
Research Data
sj-pdf-4-hpq-10.1177_13591053211037727 – Research Data for The long arm of childhood: The prolonged influence of adverse childhood experiences on depression during middle and old age in China
Research Data, sj-pdf-4-hpq-10.1177_13591053211037727 for The long arm of childhood: The prolonged influence of adverse childhood experiences on depression during middle and old age in China by Hao Chen, Qiuyan Fan, Stephen Nicholas and Elizabeth Maitland in Journal of Health Psychology
Research Data
sj-pdf-5-hpq-10.1177_13591053211037727 – Research Data for The long arm of childhood: The prolonged influence of adverse childhood experiences on depression during middle and old age in China
Research Data, sj-pdf-5-hpq-10.1177_13591053211037727 for The long arm of childhood: The prolonged influence of adverse childhood experiences on depression during middle and old age in China by Hao Chen, Qiuyan Fan, Stephen Nicholas and Elizabeth Maitland in Journal of Health Psychology
Footnotes
Data sharing statement
The complete raw data-set, including the syntax file, and log files for analysis, are available in the Figshare repository and as Supplemental Material via the SAGE Journals platform.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.