
Abstract
Psychometric scales can be used to assess the cognition of and behavior toward tuberculosis (TB) disease and anti-TB medicines in TB patients by applying the Information-Motivation-Behavioral-Skills model. This study validated a psychometric scale from the responses of 115 TB patients using principal component (PCA) and reliability analyses. The Cronbach’s-alpha was 0.864. The PCA identified 21 factors, with eigenvalues greater than one. Six factors, with factor loading >0.5 had more than two items loaded to a factor. Twenty-five items validated from six factors suggest that the scale can be used for cognitive and behavioral assessment and interventions in tuberculosis patients.
Keywords
Tuberculosis (TB) is a communicable disease that is a major global public health problem. It is one of the top 10 leading causes of death worldwide and has been the leading cause of death from a single infectious agent since 2011, ahead of the Human Immunodeficiency Virus (HIV) disease (World Health Organization [WHO], 2018). TB is a chronic infectious disease that affects mainly the most disadvantaged populations who suffer from poverty, economic distress, vulnerability, marginalization, discrimination, and stigma. It involves complex treatment regimens with potentially severe side effects. Tuberculosis can be spread when infected persons expel the bacteria in the air after coughing, sneezing, or talking. Though TB can affect anyone anywhere, the majority of infected persons are male adults (WHO, 2020).
Mycobacterium tuberculosis (M. TB) is the causative agent for TB, infecting about a quarter of the world’s population, and about 10 million people in 2019 (WHO, 2020). M. TB is an intracellular microorganism that replicates very slowly, requiring prolonged multi-drug treatment of 6 months to 1 year which is implemented through the Directly Observed Therapy (Federal Ministry of Health [FMOH], 2015). Although successful treatment is available and achievable, challenges of medication adherence usually arise due to the prolonged, multi-drug treatment regimen.
Adherence is a complex and dynamic behavioral phenomenon that influences treatment outcomes—which are major indicators for evaluating TB treatment programs, classified as successful or unsuccessful (Chisholm-Burns and Spivey, 2008; Ruslami, 2008; WHO, 2018). Adherence is defined as the extent to which the patient’s behavior matches agreed recommendations from the prescriber (Horne et al., 2005). With TB, there has been a global increase in the incidence of multi- and extensive-drug resistance due to non-adherence and treatment failure (Borgdroff et al., 2002). Non-adherence is a complex cognitive and behavioral concern in medication therapy, accounting for about 64% of unsuccessful/poor treatment outcomes (Barber, 2002).
Treatment adherence, also known as pharmacoadherence denotes adherence solely associated with medication-taking behavior, narrowing the focus to a patient’s practice of taking a prescribed medication. Pharmacoadherence is a health behavior that can be affected by beliefs about the origins, transmission, and treatment of TB, often resulting in the stigmatization of those affected (Chisholm-Burns and Spivey, 2008). Health behavior is an activity taken by a person to protect, promote, or maintain his or her health, regardless of his or her perceived health status, and regardless of whether the behavior is effective (Bowling, 2007). The place of health in a person’s value system may be reflected in his/her definitions of health or illness which is often as complex as definitions usually vary according to culture. The interaction of these factors makes adherence to anti-TB medicines not only a priority but a complex and dynamic issue, which relates to consumers, providers, health systems, and broader socio-economic contexts (Munro et al., 2007; WHO, 2020).
Populations with low educational levels have been shown to be more vulnerable to TB infection (Sun et al., 2018). In addition, low health education level has been identified as a limitation in TB management and control (Li et al., 2019). Patient education is “the process of influencing patient behavior and producing the changes in knowledge, attitudes, and skills necessary to maintain or improve health” (American Academy of Family Physicians [AAFP], 2000). It includes informing patients about side-effects, behavioral skills such as self-monitoring, self-rewards, social support, and reminders (telephone follow-up or short message services-SMS). These have been used in combination to yield improvement in treatment outcomes (Liu et al., 2015).
Using Bloom’s taxonomy of learning objectives, patient education can be structured to guide the transfer of knowledge and provide a basis for evaluation, including the extent to which such learning has occurred. In addition, where multiple health workers are involved in the education process, objectives provide continuity of focus. Patient-focused objectives that are directed toward learning valuable information, rather than on volumes of unnecessary information, are most effective as they prioritize the patient and not the health worker or the process (Krau, 2011). Bloom’s taxonomy classifies learning into three: cognitive, affective, and psychomotor.
The cognitive domain evaluates the patient’s level of understanding of their disease and the medicines they are taking. If the patient has a good understanding of the disease process, he/she can apply the knowledge to his/her treatment plan, as well as ask questions that will improve the management of the disease. The patient can also adapt to the new lifestyle and form new ways of living with the disease by creating a plan that would help in achieving his or her goals in regards to living with the disease (Palm, 2013). Patient knowledge (cognition) has been shown to be a major determinant of treatment success (Dim and Dim, 2014; Fatiregun et al., 2009).
Patient interventions usually target the patient’s cognition through patient education and adherence counseling, to achieve a positive behavioral change which can vary from lifestyle modifications to adherence to prescribed medications, that can improve treatment success, as modeled by the WHO’s Information-Motivation-Behavioral (IMB) skills model. The IMB model (Figure 1) is an example of a psychological health model used in research to study adherence as a complex behavioral and social phenomenon. It proposes that information is a prerequisite for changing behavior but in itself is not enough to produce this change. Motivation and behavioral skills are major determinants and are independent of behavioral change. Information and motivation work largely on behavioral skills to affect behavior through informed decisions. Therefore, both information and motivation increase the likelihood of adherence because it is the desired behavioral change (WHO, 2003). This is the theory behind the cognitive and behavioral intervention which leads to the behavioral change desired (adherence) in TB treatment that improves treatment outcomes through reinforced medication education and adherence counseling, as proposed in this study.
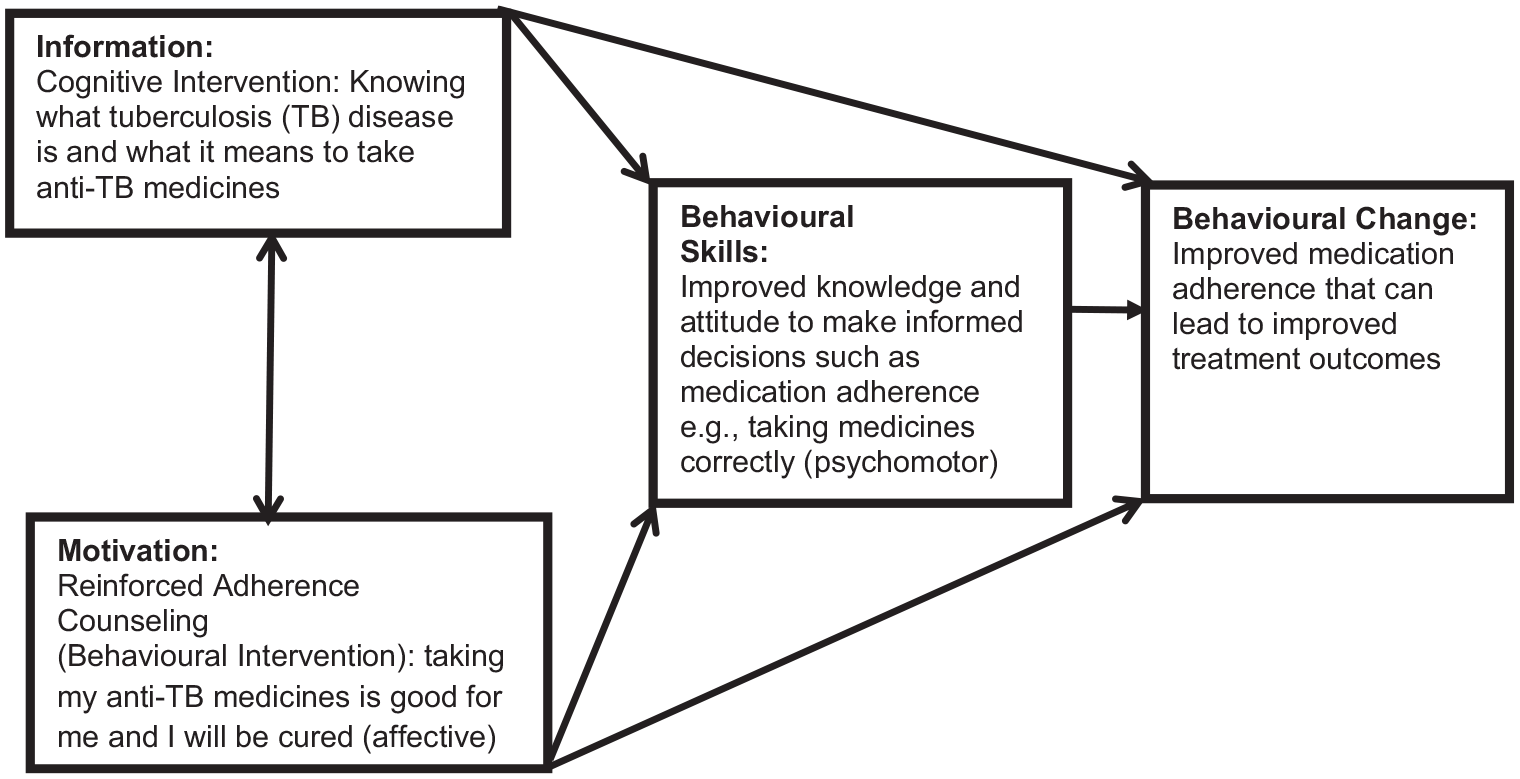
Information-motivation-behavioral skills model (WHO, 2003).
The affective domain focuses on how things are dealt with emotionally. Emotion draws attention and channels strong residual memory, thus affecting cognition (Wilson, 2019). The psychomotor objective is specific to discrete physical functions, reflex actions, and interpretive movements. A physical action supports cognitive growth and enhances recognition skills. In patient therapy, the psychomotor objective involves actions that patients can take to improve their health outcomes such as graded exercise and taking medicines-medication adherence (Palm, 2013).
Patient education builds a sense of autonomy which equips the patient with the necessary knowledge and skill to make informed healthcare decisions. The results of a meta-analysis from a study indicated that combining interventions that included cognitive, behavioral, and affective (emotional) components were most successful in improving pharmacoadherence; a finding that is generally consistent with systematic reviews of pharmacoadherence interventions (Chisholm-Burns and Spivey, 2008; Li et al., 2019). A systematic review of strategies that promoted TB medication adherence in developed countries recommended the need to pilot test in developing countries before full implementation to optimize resource use (Volmink and Garner, 1997). The aim of this study, therefore, was to validate psychometric scales used in developed countries, for cognitive and behavioral interventions in tuberculosis patients in Jos, Plateau State, Nigeria—a developing country.
Methods
Study design, setting, and population
The cross-sectional prospective study analyzed responses from psychometric scales obtained from TB patients who were 15 years and above (Centers for Disease and Control and prevention [CDC], 2013) and diagnosed by positive bacteriological or clinical confirmation from December 2015 to April 2016 in Jos, Plateau State. Located in North-Central Nigeria, Plateau State has a landmass area of 26,899 square kilometers, with a population of 3,206,531 people (National Population Commission [NPC], 2017). The study was carried out in four Directly Observed Therapy (DOT) centers for TB in Jos: Bingham University Teaching Hospital (BUTH), Our Lady of Apostles Hospital (OLAH)—which are faith-based hospitals, Jos University Teaching Hospital (JUTH), and Plateau State Specialist Hospital (PSSH)—which are tertiary health institutions owned by the Federal Government of Nigeria and Plateau State Government respectively. The DOT centers were purposefully selected based on preliminary information that they account for more than 50% of reported and documented TB cases in Plateau State.
Ethics
The Institutional Health Research Ethics Committee of the Jos University Teaching Hospital, Jos, Nigeria, with reference number: JUTH/DCS/ADM/127/XIX/6442 approved the protocol of this study and granted permission to access the data used for this research. Written informed consent was sought and obtained from the respondents before data collection. Participation in the study was voluntary. The respondents were assured that the filling of the questionnaire was not an examination as there was no right or wrong answer, but what mattered was their views about TB illness and the anti-TB medicines they were taking. This was done to encourage honest responses (Horne et al., 1999).
Data collection method and instruments
Patients were recruited as they came in for their medication refill. Interviewers administered a 74-item questionnaire developed by combining items/questions from four standard psychometric scales to measure TB patient’s cognition and behavior toward their illness and treatment. Five of the 120 recruited respondents withdrew from the study, leaving a sample of 115 patients. The psychometric scales used include:
a. The Morisky medication adherence scale-4 (Morisky et al., 1986), which is a structured four-item-self reported adherence instrument that targets the patient’s cognition in relation to medication-taking behavior because non-adherence to taking medications could occur in any or all of several ways: forgetting, carelessness, and stopping the drug when feeling better or worse.
b. The Revised Illness Perception Question-naire (IPQ-R), obtained from Leventhal’s self-regulatory model of illness measures cognitive, emotional, and coping behaviors. It provides a coherent understanding of the illness—a type of meta-cognition reflecting the way a patient evaluates the coherence of his/her illness that is, how the illness makes sense as a whole to the patient. This may play a role in long-term adjustment, response to symptoms of the illness, and medication adherence (Moss-Morris et al., 2002).
c. The Belief about Medicines Ques-tionnaire (BMQ) is a scale of items derived from themes identified in published studies and from interviews with chronically ill patients. It is made up of two sections: BMQ-specific and BMQ-general which measures aspects of both emotion and cognition (Horne et al., 1999).
d. The Perceived Sensitivity to Medicine (PSM) scale explains three aspects of medicine-related behavior: treatment decisions, adherence, and reporting of side effects, since patients are becoming more actively involved in their care (Horne et al., 2013).
Data analysis
Data were collated and cleaned with the aid of SPSS version 24 (IBM, Chicago, IL, USA). The TB patient’s responses to each of the items were scored on a five-point Likert type scale and subjected to principal component analysis for extraction and reduction of the components. Reliability tests, including Cronbach’s-alpha, and inter-item correlation were done.
Factor analysis
Factor analysis is a multivariate statistical procedure that reduces a large number of variables into a smaller set of variables or factors. It isolates items with high loadings scientifically. It provides construct validity and examines the relationship between variables. It searches to find factors that put together, explain the majority of the responses. Principal component analysis (PCA), a type of exploratory factor analysis (EFA) was used in this study to determine the number of factors to extract, reduce the large set of constructs, and understand what constructs underlie the data (Williams et al., 2010).
Principal component and reliability analyses
The suitability of the sample size was checked using the minimum Kaiser-Meyer-Olkin (KMO) values requirement of ⩾0.50 (Jimam et al., 2019; Wolf et al., 2013). The PCA was used to reduce the large number of items into smaller and meaningful categories through the “Kaiser’s eigenvalue-greater-than-one rule” (Maloney et al., 2011; Müller et al., 2015). Cattell’s criteria of visually selecting components above the cut-off from the scree plot were used (Field, 2009). The variables attributable to a factor were examined and named. The varimax method of orthogonal rotation was used to restrict the factors from correlating with one another in order to get the appropriate number of factors that could be clearly interpreted based on the types and numbers of items loaded on them (Suhr, 2006). Items with minimum factor loadings less than 0.5 were considered weak or having no relationship with the factor, so they were excluded (Moss-Morris et al., 2002), after which the analysis was re-run.
Data sharing statement
De-identified participant data for all variables reported in this study, including participant responses to the 74-item questionnaire on the Likert scale are shared on FigShare.
Results
Demographic characteristics of the respondents
A total of 115 completely filled questionnaires from 120 administered gave a response rate of 95.8%. The percentage of male respondents was 66 (57.4%). The majority 7 (60.8%) of the respondents were in the productive age group of 21–40 years, had secondary education (55.7%), and were married (60%), as shown in Table 1.
Demographic characteristics of respondents (N = 115).
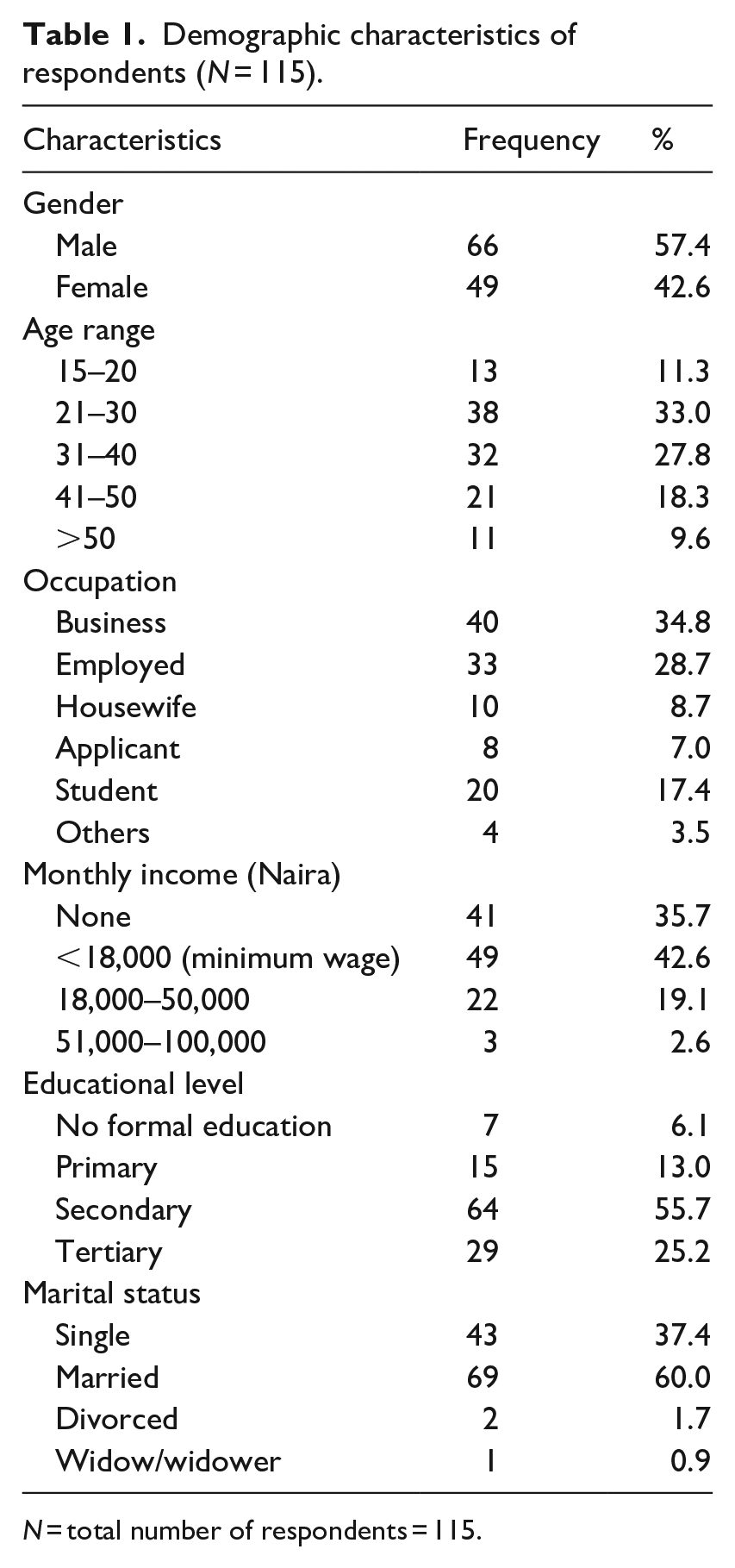
N = total number of respondents = 115.
Sampling adequacy for factor analysis
The Kaiser-Meyer-Olkin measure of sampling adequacy for the exploratory factor analysis was 0.595 and 0.759 before and after deletion of misfit items; indicating the adequacy of the sample population. Bartlett’s test of sphericity further confirmed a strong correlation (p < 0.001) between the items on the scale as seen in Table 2.
Kaiser-Meyer-Olkin (KMO) and Bartlett’s Test of Sphericity.
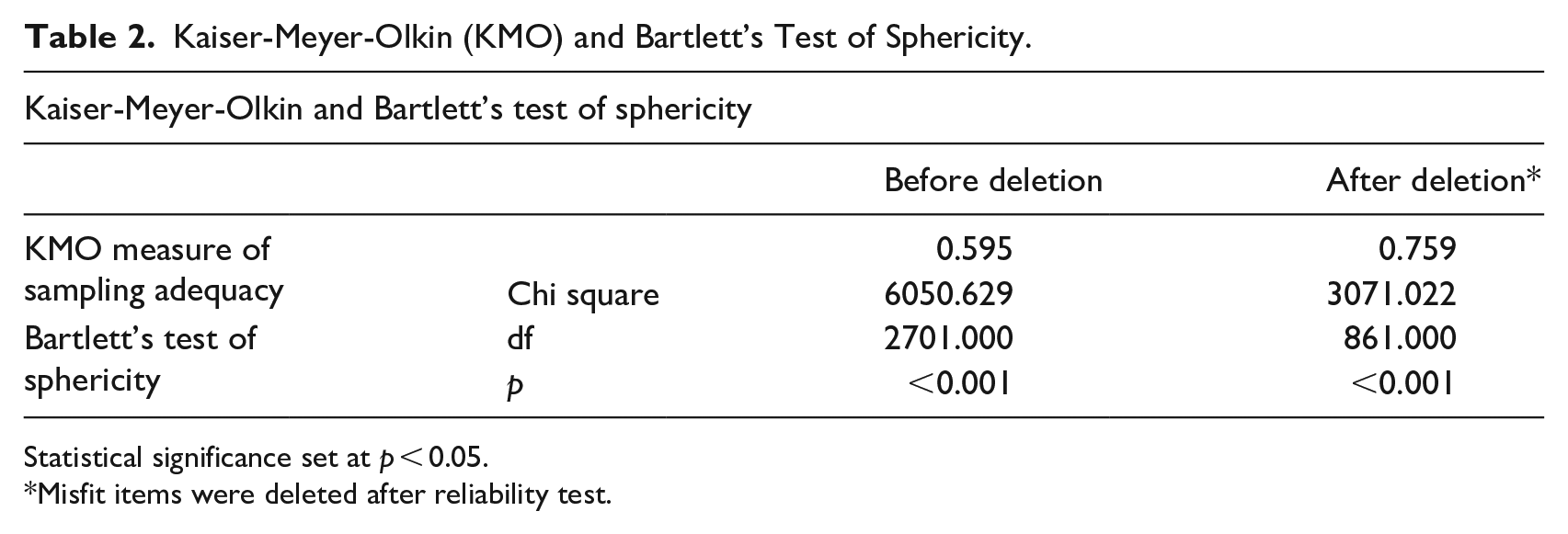
Statistical significance set at p < 0.05.
Misfit items were deleted after reliability test.
Item reliability (Cronbach’s alpha)
The overall Cronbach’s alpha for the 74 items was 0.864. The Cronbach’s alpha “if item is deleted” for the individual items of the 74-item draft instrument before deletion of misfit items ranged between 0.852 (item 61) and 0.866 (item 45), while the values ranged between 0.807 (item 65) and 0.831 (item 32) for the 42-item scale after deletion. The Cronbach’s alpha value for the 42-item scale after deletion of 32 misfit items was 0.805. The “corrected item-total correlations” (item discrimination index) for the draft scale ranged between −0.093 (item 1) and 0.669 (item 65), while the values for the 42 items after deletion were in the range of −0.079 (item 38) and 0.702 (item 65), which indicated the item discrimination levels. Items with “corrected item-total correlation” values of ⩾0.30 were considered satisfactory, while those with values of ⩾0.2 but ⩽0.29 were considered as being fairly good items, but those whose index values were ⩽0.19 were considered as poor items (DeVon et al., 2007). At this stage of analysis, there might be a possibility of the software treating all the respective items as single dimension instruments rather than considering them as multi-dimensional during the computation (Kline, 2015). Therefore, to avoid the possibility of eliminating potentially important items, all the items for the instruments were retained for exploratory factor analysis (EFA).
Exploratory factor analysis
The principal component analysis identified 21 components/factors, with eigenvalues greater than one (Figure 2). Out of the 21 components, 11 components had items with factor loading greater than 0.5. Components or factors with more than two items were chosen and this reduced the components to six. Each factor made up of three or more items was further subjected to reliability (Cronbach’s-α) test to select only items that improved the reliability of the factor that is, any item when deleted would increase the Cronbach’s α of the factor. The item-total correlation in each component was greater than 0.30. A total of 25 items grouped under six components were identified for the intervention as shown in Table 3. Four knowledge items were added from previous studies (Sariem et al., 2013, 2015), to make a total of six knowledge items used in the study.
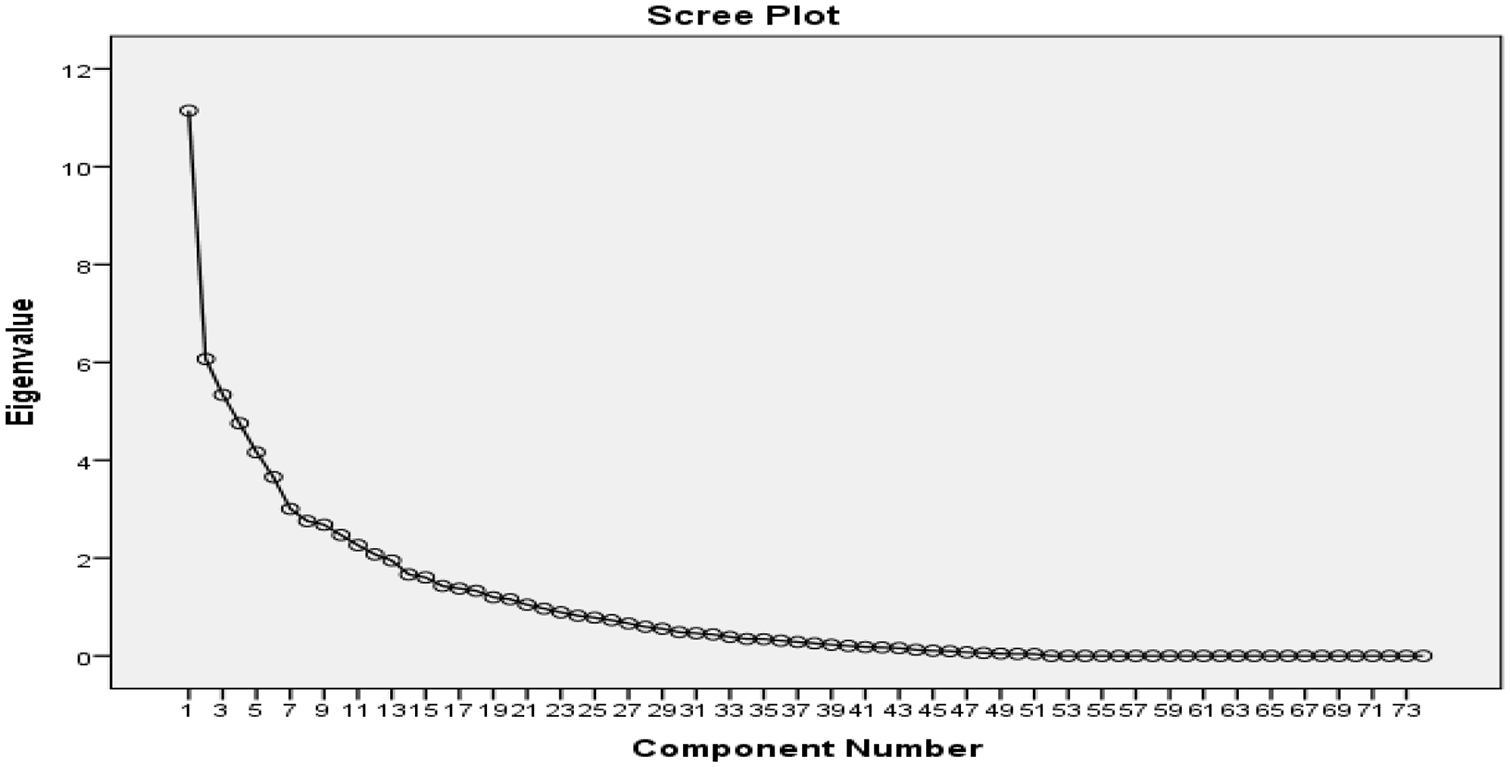
Scree plot of factors for cognitive and behavioral intervention scale.
Principal component analysis and reliability of cognitive and behavioral intervention scale (N = 115).
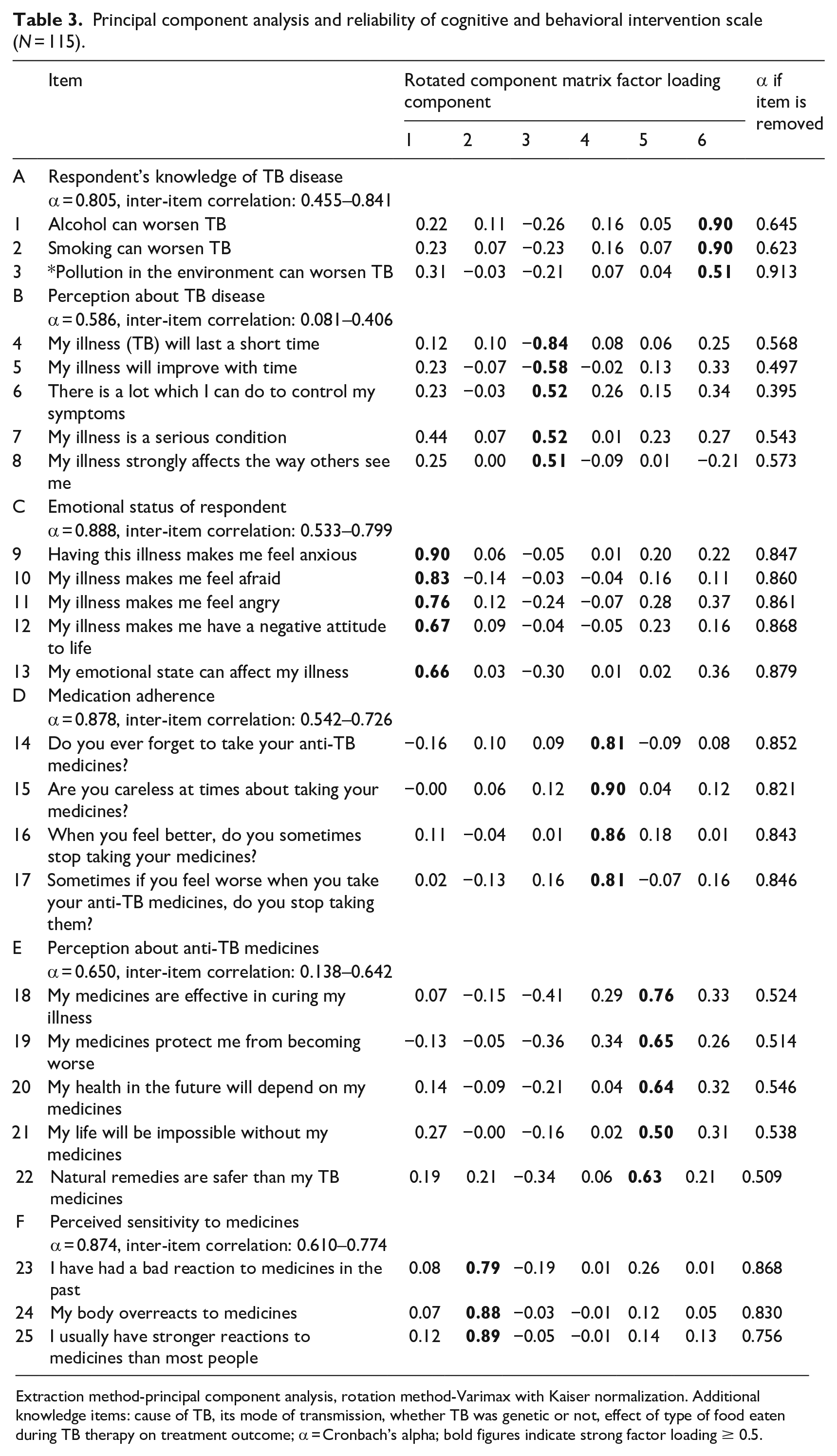
Extraction method-principal component analysis, rotation method-Varimax with Kaiser normalization. Additional knowledge items: cause of TB, its mode of transmission, whether TB was genetic or not, effect of type of food eaten during TB therapy on treatment outcome; α = Cronbach’s alpha; bold figures indicate strong factor loading ≥ 0.5.
Discussion
Tuberculosis is among the top ten causes of mortality globally and the leading cause of death from a single infectious disease (WHO, 2020). Low health education level has been identified as a limitation in its management and control (Li et al., 2019). The factor analysis done in this study extracted and grouped the psychometric scales into six factors namely: TB patient’s knowledge of TB disease, perception about TB disease, emotional status, medication adherence, perception about anti-TB medicines, and perceived sensitivity to anti-TB medicines. With a theoretical framework, the items from the factors identified and validated can be used in designing cognitive and behavioral interventions for tuberculosis management.
The Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy and Bartlett’s test of sphericity assessed the suitability of data for factor analysis and examined the strength of relationship among the items (Munro, 2005). The KMO measure of sampling adequacy of 0.595 and 0.759 implied that the sample size was adequate for factor analysis, with an accepted minimum p-value of 0.5 (Hutcheson and Sofroniou, 1999). The strong correlation (internal consistency) between the items could be due to the fact that the items were from standardized psychometric scales (Boateng, 2018).
The Cronbach’s alpha (α) value for internal consistency of the 74-item scale was 0.864, above the minimum acceptable value of 0.7 (Tan et al., 2014). This implies that the items were reliable to measure TB patient’s cognition and behavior toward TB disease and anti-TB medications. A similar study done by Fan et al. (2018) developed a psychometric scale to measure the knowledge, attitude, and practice of student TB patients in china had good internal consistency reliability of 0.817. The Cronbach’s-α value for most of the factors identified in another study was between 0.73 and 0.89, indicating good reliability (Gliem and Gliem, 2003). Values from 0.59 to 0.65 were said to be of acceptable reliability for exploratory investigations (Maloney et al., 2011; Taber, 2018). Cronbach’s-α reliability coefficient normally ranges between 0 and 1.0. However, there is no lower limit to the coefficient. The closer the Cronbach’s-α coefficient is to 1.0, the greater the internal consistency of the items in the scale. In addition, as the number of items increases, Cronbach-α rises toward 1.0, therefore, it is heavily dependent on the number of items composing the scale (Cronbach, 1951). The Cronbach’s-α test to select only items that improved the reliability of the factor that is, any item when deleted would increase the Cronbach’s-α of the factor, led to the deletion of item 3 from Table 3 (pollution in the environment can worsen TB). This increased the reliability of the knowledge factor scale from 0.805 to 0.913.
The inter-item correlation of most of the components was around the accepted value of 0.3 and above, indicating that the individual items sufficiently correlated with each other for factor analysis to be appropriate (Pallant, 2007). It has also been reported that values of <0.30 but ⩾0.20 could be acceptable in explorative analysis (Cristobal et al., 2007). To determine the number of components to extract, Cattell’s criteria of visually selecting components above the cut-off from the scree plot was used. The scree plot (Figure 1) provided a graphical representation of eigenvalues plotted on the Y-axis against the corresponding components on the X-axis. The higher the eigenvalue, the higher the extent of the resolution of the factors (Moss-Morris et al., 2002; Müller et al., 2015).
The 25 items identified from this study can be used to measure and assess TB patient’s cognition and behavior toward TB disease and their anti-TB medicines by applying the Information-Motivation-Behavioral skills model as the theoretical framework, with the aim of improving TB outcomes. Successful management of TB will require that each patient knows and understands TB disease and the rationale behind its management to enhance adherence. These skills can be acquired by motivating the patient through health education, which can be influenced by the individual’s health literacy level—a “reflection of a person’s social and cognitive skills, which in some ways determine whether an individual has the ability to understand, apply, analyze, and disseminate health information or health services and whether an individual can maintain and promote health through these skills” (Li et al., 2019). Health education empowers patients with appropriate and correct information, encourages a positive attitude toward TB and its cure, and encourages their contribution toward TB control especially when they adhere to taking their anti-TB medicines. Researchers, health workers, and policy workers are increasingly recognizing that encouraging patients to play more active roles in their health care improves the quality and efficiency of health care and health outcomes (Kigozi et al., 2017). The psychometric scale developed can be used to design cognitive and behavioral interventions to assess TB patient’s treatment outcomes, enable standard psychometric scales to quantitatively measure, and assess medication-taking behaviors (pharmacoadherence).
This study was limited by the use of only the subjective self-report method to measure adherence. An objective method such as the use of Medication event monitoring systems can be used in addition, even though high reliability and inter-item correlation scores were obtained for the Morisky medication adherence scale-4 used in this study.
Conclusion
Using the Information-Motivation-Behavioral skills model as the theoretical framework, the principal component analysis and reliability test done in this study scientifically reduced and validated 74-items from four psychometric scales to a scale of six factors, with 25-items that can be used to design cognitive and behavioral interventions, whose impact can be assessed on tuberculosis treatment outcomes. The psychometric scale developed from this study can also be tested and used to design and assess the impact of interventions on treatment outcomes of other chronic ailments.
Research Data
sj-sav-1-hpq-10.1177_13591053211039003 – Supplemental material for Application of the information-motivation-behavioral-skills model to validate a cognitive and behavioral intervention scale for tuberculosis patients in Jos, Nigeria
Supplemental material, sj-sav-1-hpq-10.1177_13591053211039003 for Application of the information-motivation-behavioral-skills model to validate a cognitive and behavioral intervention scale for tuberculosis patients in Jos, Nigeria by Comfort Nanbam Sariem, Maxwell Patrick Dapar, Nanloh Samuel Jimam and John Chinyere Aguiyi in Journal of Health Psychology
Footnotes
Acknowledgements
The authors are grateful to the following pharmacists: Joshua Dung, Samson Chuwang, and Joel Bulus, for their support in data collection.
Author contributions
CNS conceptualized the research idea, designed the study, and collected data. MPD and NSJ analyzed and interpreted the data. JCA and NSJ read and revised the manuscript. CNS prepared and wrote the first draft of the manuscript, and all authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Africa Center of Phytomedicine Research and Development, University of Jos (grant number 126974).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.