
Abstract
This study aims to explore the association between parents parenting styles differences and lifetime suicidal ideation (LSI). The sample included 2598 Chinese medical students. Results showed that 10.5% of students reported LSI. Moreover, total differences in parenting styles (OR = 1.04, 95% CI = 1.02, 1.06), parental nurture rejects differences (OR = 1.11, 95% CI = 1.04, 1.18), parental emotional warmth differences (OR = 1.08, 95% CI = 1.03, 1.14), and parental overprotective differences (OR = 1.11, 95% CI = 1.06, 1.16), obtain a scholarship, physical disease and mental health were associated with LSI. The major finding reminds us of the importance of consistent parenting style for suicide prevention.
Introduction
According to the estimation by World Health Organization (WHO), suicide was the second leading cause of death among 15–29 years old (WHO, 2014), and it was also the fifth leading cause of death in China, accounting for about 287,000 deaths a year. In China, suicide was also the leading cause of death among young people aged 15–34 in 1990s, accounting for 18.9% of all deaths (Phillips et al., 2002). Although the overall Chinese suicide rate had shown a downward trend in the recent decades (Zhang et al., 2014), the suicide rates among 15–24 years old were also in high levels (Wang et al., 2014), which implied that young people aged 15–24 suicide was still an important public health problem in China. College students were a special group of 15–24 years old that also reports high levels of suicidal behaviors and psychological problems worldwide (Eskin et al., 2016). For example, studies in the United States (US) found that over 10.0% of college students experienced suicidal ideation (SI; Garlow et al., 2008; Wilcox et al., 2010). Besides, SI is also at a higher level among medical students receiving health training in China and worldwide (Dyrbye et al., 2008; Sun et al., 2017; Tyssen et al., 2001). For example, a study conducted at the medical schools in Sweden found that medical students suffered from high academic pressure and higher rates of depression than the general population (Dahlin et al., 2005). Therefore, suicide problems among medical college students should be paid more attention.
In the recent decades, SI was identified as an important predictor for the following suicidal behaviors (Nock et al., 2008), and the results identified that the risk factors for SI are also complex, which included social, psychological, cultural, and biological factors (Coentre and Góis, 2018; Desalegn et al., 2020; Menezes et al., 2012). Specifically, many factors had been proved as likely contributors to the development of suicide ideation among medical college students, including stressful academic events (Tyssen et al., 2001), depression (Dyrbye et al., 2008), previous diagnosis of a psychiatric disorder (Van Niekerk et al., 2012), feeling neglected by parent, academic achievement, family relationships (Menezes et al., 2012), maternal occupation, and level of education (Sun et al., 2017).
In the process of exploring the factors associated with SI, we had found that family factors played important roles among students. Previous studies mainly analyzed family-related variables as one variable (DeVille et al., 2020; Oppenheimer et al., 2018). In addition, previous studies have provided important information on the links between various parenting styles and students development (Hayek et al., 2021), and have also found a weak link between parenting styles and SI (Prusty and Panda, 2017; Sun et al., 2017). However, they do not address the impact on undergraduate college students when parents adopt different parenting styles. Past research on parental inconsistency has focused on specific parental behaviors (e.g. inconsistent expectations) rather than inconsistent parenting styles. It is true that parenting styles are different between parents, and that this difference can lead to different parenting outcomes for college students (Simons and Conger, 2007).
Relevant theories also remind us that differences in parenting styles may be related to SI, such as strain theory, suicide discordant pressure theory and so on. The strain theory of suicide that explains the deep motive of suicide (Zhang and Lester, 2008), suggests that differences in value may bring inner struggles and pain to medical college students, thus promoting the formation of SI (Lew et al., 2020). Parental parenting styles as one of important factor for the value, which imply us that the association between differences in parental parenting styles and suicidal behavior. In addition, the theory of suicide discordant pressure also remind that differences in parenting styles may be related to suicide, in terms of discordant pressure and psychological pressure caused by contradiction (Zhang, 2005). Other studies have found similar results. For example, overprotective parenting style is found to have negative on the mental health of youth (Kim, 2019). Another study showed that parents’ knowledge about the development of self-esteem in adolescents was significantly positively correlated with parental parenting styles (communication, support, positive reinforcement, etc.) and authoritative parenting styles (Banstola et al., 2020). The research on the relationship between the three dimensions of parental parenting style (parental warmth, behavioral control, and psychological control) and SI of Chinese high school students found that parental warmth had a negative predictive effect, while psychological control had a positive predictive effect on the contrary (Li et al., 2016). A similar study among College students in Taiwan observed a linear positive correlation between increased suicidal tendencies and low emotional, overprotective, and authoritarian controlled parenting styles (Gau et al., 2008).
Previous research has also shown that living in a family with inconsistent parenting styles played an important role in increasing the risk of future intentional deliberate self-harm in children (average age 18), one of the strongest predictors of suicide (Mitrou et al., 2010). However, few studies discuss the effect of differences in parenting styles on SI in Chinese medical college students. These results may not be translated in China because of the specific characteristics of suicide (Qin and Mortensen, 2001). Therefore, it is necessary and urgent to explore the characteristics and factors related to SI.
In this study, we aim to explore the relationship between parents parenting styles differences and SI among medical college students in China. It is helpful for us to understand the association between differences in parenting styles and SI among Chinese medical college students, so as to better provide evidences for suicide prevention and intervention. Based on the above evidences, we proposed two hypotheses of this study. First, it was hypothesized that total differences in parenting styles was association with lifetime suicidal ideation among medical college students. Second, it was hypothesized that each sub-scale of parental nurture rejects differences, parental emotional warmth differences, and parental overprotective differences were also associated with lifetime suicidal ideation among medical college students.
Method
Participants and survey procedure
All of the respondents were medical college undergraduate students, and a cross-sectional design was used in the current study. In the study, two medical schools in Shandong province were selected as research samples by using multi-stage cluster sampling technique. The study covered all 12 medical majors from the 2 medical schools, including clinical medicine, preventive medicine, pharmacy, stomatology, nursing, and rehabilitation medicine. For each major, we selected all the grades from the first grade to the fourth or fifth grade. In each grade, a complete class will be selected to participate in our survey. A total of 2598 respondents answered the questionnaire, including 1162 boys (44.7%) and 1436 girls (55.3%), with an average age of 20.42 years. In this study, students were not compensated with credits or in any other way. Data from medical undergraduates was collected in their classrooms of the respective schools. Prior to the onset of the study, each researcher underwent a strict training process in order to ensure consistency across the sample. Firstly, one of the trained researchers visited the medical students in the classrooms, explained the study, obtained a consent form with the student’s signature and all of the students were informed about the confidentiality of personal information. Secondly, under the guidance of the researchers, the students were asked to fill out questionnaires and then turn in the completed questionnaires. Social-demographic characteristics, parental characteristics, mental health, parenting styles, and lifetime suicidal ideation were included in the questionnaire.
Instrument and measures
Lifetime suicidal ideation
For the lifetime suicidal ideation (LSI), we asked the respondents that “Have you ever seriously considered killing yourself?” We classified the affirmative respondents as having SI (Kessler et al., 1999). The question about LSI was from the National Comorbidity Survey (NCS), which has been widely used to assess SI in many previous studies (Sun et al., 2017; Zhao et al., 2020).
Differences in parenting styles
In this study, Short Egna Minnen Barndoms Uppfostran Chinese Version (S-EMBU-C) was used to estimate the parenting styles and parenting styles differences. The Chinese Version (S-EMBU-C) consisted of 21 items that measured parental parenting styles about three scales (Rejection, Emotional Warmth, and Overprotection) with respectively six, seven, and eight items, and the score for each item ranged from 1 to 4 and the total score for the three scales (Rejection, Emotional Warmth, and Overprotection) ranged from respectively 6–24, 7–28, and 8–32. The Chinese version of this scale (S-EMBU-C) was also used in the previous studies about parenting style (Xu et al., 2017) and the 21-item S-EMBU is also recommended as a reliable functional equivalent to the 81-item early EMBU (Arrindell et al., 1999). The paternal and maternal total scores of the three scales were calculated respectively, among which the rejection inclusion items were 1, 4, 7, 12, 14, and 19, the emotional warmth inclusion items were 2, 6, 9, 11, 13, 17, and 21, and the overprotection inclusion items were 3, 5, 8, 10, 15, 16, 18, and 20. For each of the 21 items, the answer was: “No, never” = 1, “Yes, but rarely” = 2, “Yes, often” = 3, and “most of the time” = 4. Please observe that item No. 15 should be recoded as follows: 0 = 3, 1 = 2, 2 = 1, 3 = 0.
The differences in parenting styles F was calculated by the following formula.




Where
The absolute value of the 21 items, which was taken subtracting maternal score from paternal score on the same item, were added in the 3 scales respectively to obtain the total scores of rejection, emotional warmth, and overprotection, which represented the differences in parental parenting styles. The scores for each item ranged from 0 to 3 and the score for the three scales (Rejection, Emotional Warmth, and Overprotection) ranged from respectively 0 to 18, 0 to 21, and 0 to 24. An overall score by adding up these three areas indicates differences in parenting style. The higher the score, the greater the difference in parenting style. The Cronbach’s α of the scale in this sample was 0.860.
Parental characteristics
Family composition types are defined as normal families, restructured families, single-parent families, and others. In order to better compare the differences in parenting styles between parents, a sample of 125 single-parent families was removed and family composition was classified as regular and others. Where: “regular families” = regular, the other two categories are others. The answers of “How are your parental relationship?” could be chosen from “very good,” “good,” “common,” “bad,” or “very bad.” Further classified as the answer was: “very good” and “good” = good, and the other three types are classified as “not good.” Father or mother’s education level was measured by “illiteracy or semiliterate,” “primary school,” “junior high school,” “technical secondary school,” “junior college,” “senior high school,” “undergraduate,” and “master degree or above.” We recoded them into “junior high school or below,” “junior college or senior high school,” and “bachelor degree or above.” Father or mother’s vocations were estimated by farmers, workers, individual business, cadre, teacher, and others. As there were few individual business, cadre, teacher, and others, we combine them and recoded them into others.
Mental health
The Kessler Psychological Distress Scale (K10), an extensively used 10-question examination to detect possible anxiety, depressive, or mental distress-based disorders (Baillie, 2005), assessed individual mental health levels. Each question requires individuals to assess how often they experience mental distress on a 5-Point Likert scale that ranges from 1 (i.e. none of the time) to 5 (i.e. all of the time) and mainly focused on depression and anxiety during the past 4 weeks (Easton et al., 2017). The higher the K10 score, the higher the psychological stress. This questionnaire was used in the previous studies examined the clinical utility of the Kessler K10 mental health score as an indicator of SI (Chamberlain et al., 2009). Moreover, the K10 was also used in health risk appraisal surveys and primary care screening, and its good precision has proved to be very useful as a broad screening scale for mental illness (Kessler et al., 2002). The Chinese version of K10 has previously shown good reliability and validity in Chinese populations (Zhou et al., 2008) and also used in the US National Comorbidity Survey (NCS; Kessler et al., 2005). The Cronbach’s α of the scale in this sample was 0.918.
Social-demographic characteristics
The questionnaire for medical undergraduates consisted of socio-demographic information (age, sex, obtain a scholarship, etc.), and physical disease. The answers of “Have you ever obtain a scholarship?” could be chosen from “yes” or “no,” and the question of “Do you have any physical disease?” also chosen from “yes” or “no.”
Father’s higher level in parenting styles
The following formula was used to calculate the score to express the higher father’s parenting styles than mother.




Where
After subtracting the mother’s score from the father’s score, the 21 questions were added directly to the 3 scales, getting fathers higher scores than mothers on 3 parenting styles: rejection, emotional warmth, and overprotection. Add up the scores from these three scales to get an overall score indicating father’s higher level in parenting styles. Similarly, The higher the score, the higher the level of parenting style of fathers than mothers. The scores for each item ranged from −3 to 3 and the score for the three scales (Rejection, Emotional Warmth, and Overprotection) ranged from respectively −18 to 18, −21 to 21, −24 to 24.
Statistical analysis
IBM SPSS Statistics 24.0 (web version) was used for data analysis. First, we used frequency and percentage to describe the demographic characteristics of the respondents. Second, Chi-square test was used to compare difference for categorical variables and t-tests was performed to compare the continuous variables across groups. Third, logistic regression analyses were performed to observe the association between SI and parenting styles differences among the medical undergraduates. All of the factors were chosen as the independent variables. Finally, the R language was used for box plot to graphically express the relationship between differences in parenting styles and LSI. To determine statistical significance, 95% confidence intervals (CIs) and p-values at a significance level <0.05 were used.
Result
Demographic and parental characteristics
The prevalence of lifetime suicide ideation was 10.5% (9.5% for girls and 11.9% for boys). The mean age of the college students was 20.42 years, the proportion of girls was higher than boys, that is, 55.3% and 44.7% respectively. Results from the Chi square and t-tests show that age (t = −2.59, p = 0.010), gender (χ2 = 3.94, p = 0.047), family composition (χ2 = 7.65, p = 0.006), obtain a scholarship (χ2 = 17.82, p < 0.001), parental relationship (χ2 = 16.41, p < 0.001), physical disease (χ2 = 30.19, p < p < 0.001), mental health (t = −22.39, p < 0.001), father’s education level (χ2 = 9.27, p = 0.010), parental nurture rejects differences (t = −6.44, p < 0.001), parental emotional warmth differences (t = −5.75, p < 0.001), parental overprotective differences (t = −5.98, p < 0.001), and total differences in parenting styles (t = −6.84, p < 0.001) were significantly associated with suicide ideation. The detailed information can be seen in Table 1.
Descriptive analysis of lifetime suicidal ideation in Chinese medical college students (N = 2598).
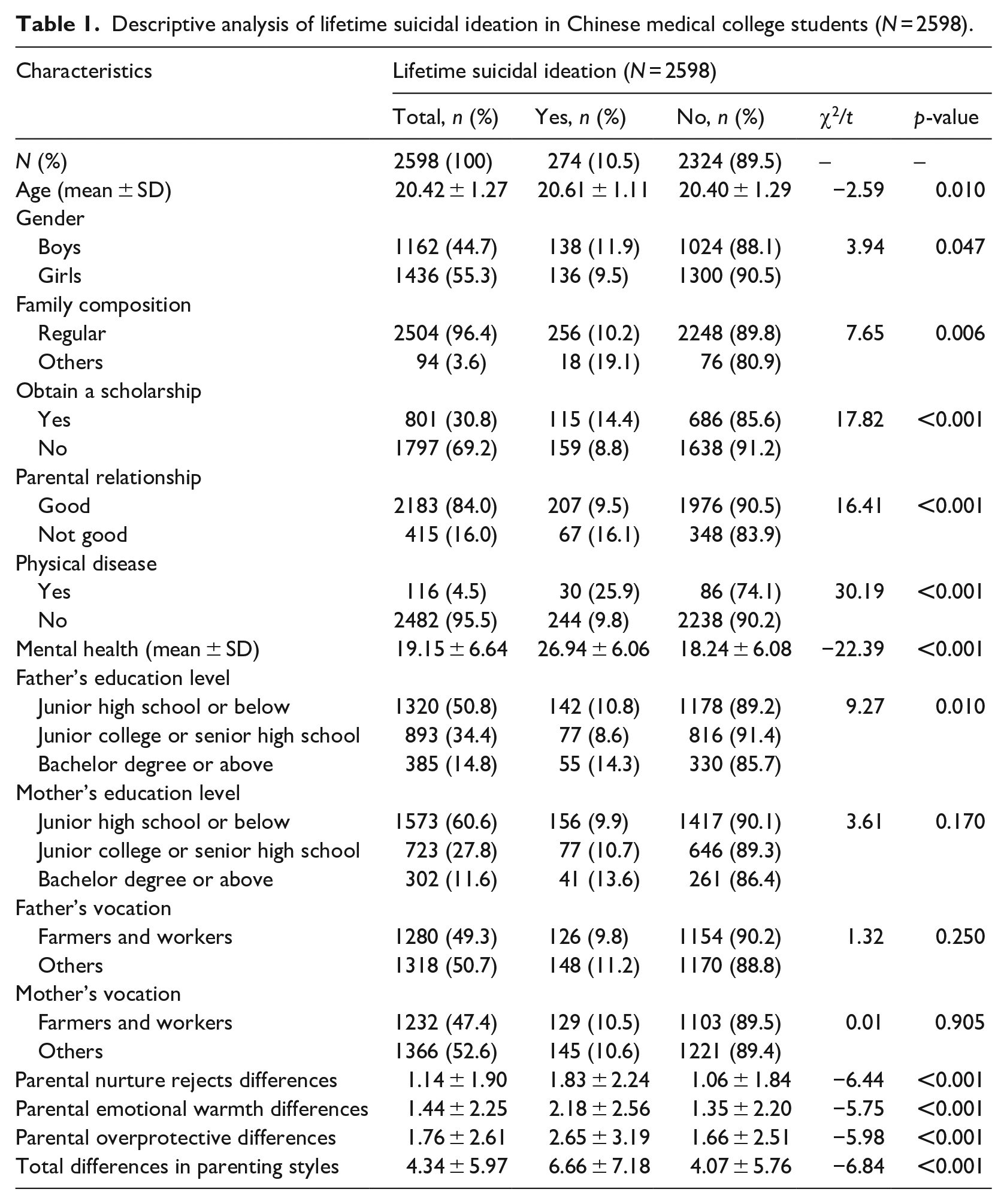
The average score for the total difference in parental parenting patterns was 4.34. Specifically, the average scores for parental parenting style differences in rejection, emotional warmth, and overprotection were 1.14, 1.44, and 1.76, respectively. Figure 1 display the relationship between differences in parenting styles and LSI. Figure 1a indicated that the total differences in parental parenting styles of medical undergraduates with LSI were significantly higher than those without SI (6.66 vs 4.07 scores). Similarly, the differences in parental nurture rejects (1.83 vs 1.06 scores) in Figure 1b, parental emotional warmth (2.18 vs 1.35 scores) in Figure 1c, and parental overprotective (2.65 vs 1.66 scores) in Figure 1d remained among medical students.
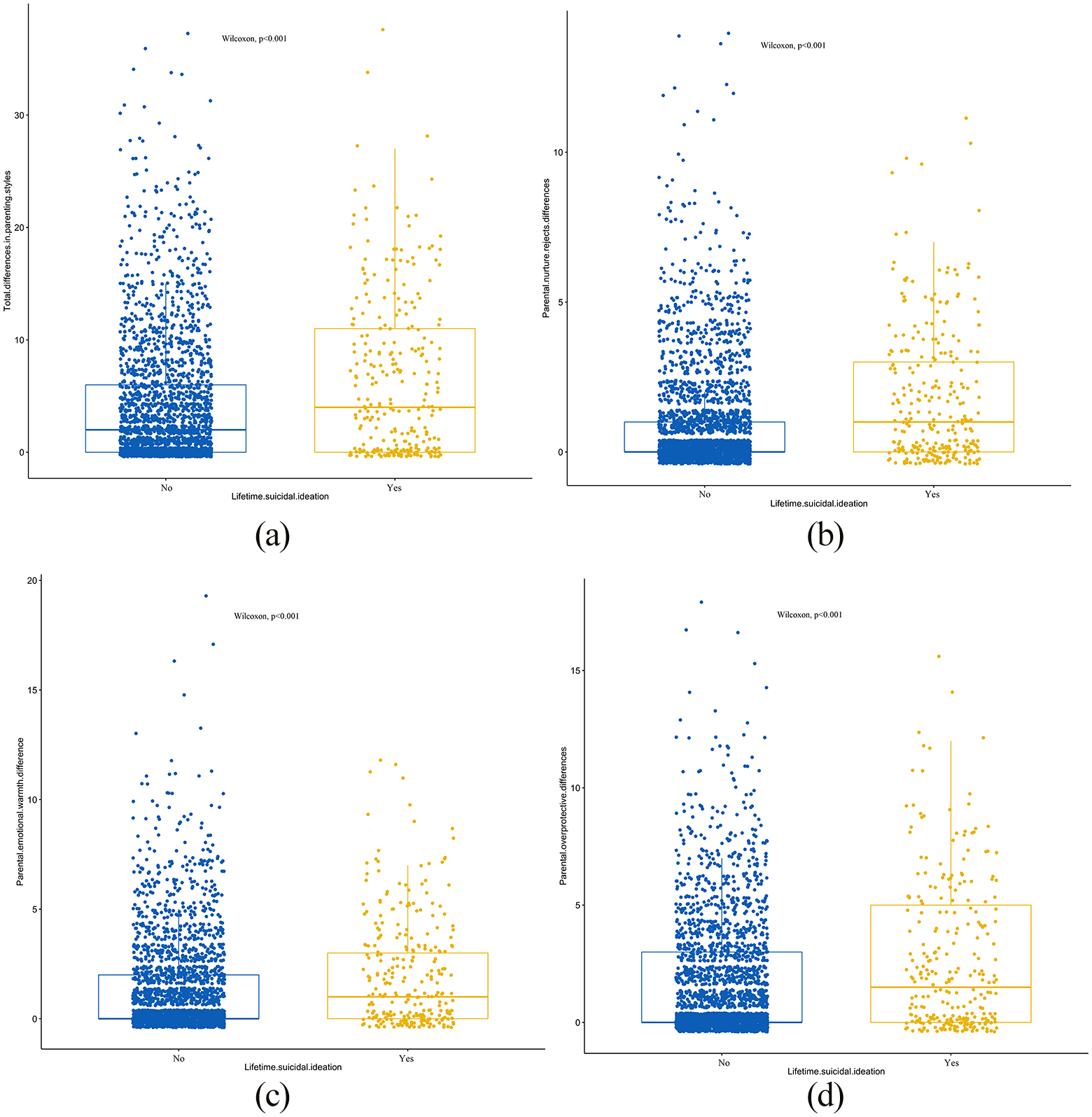
Differences in parenting styles and lifetime suicidal ideation box plot: (a) total differences in parenting styles and lifetime suicidal, (b) parental nurture rejects differences and lifetime suicidal ideation, (c) parental emotional warmth difference and lifetime suicidal ideation, and (d) parental overprotective differences and lifetime suicidal ideation.
Binary logistic regression analysis for parents parenting styles differences and lifetime suicidal ideation
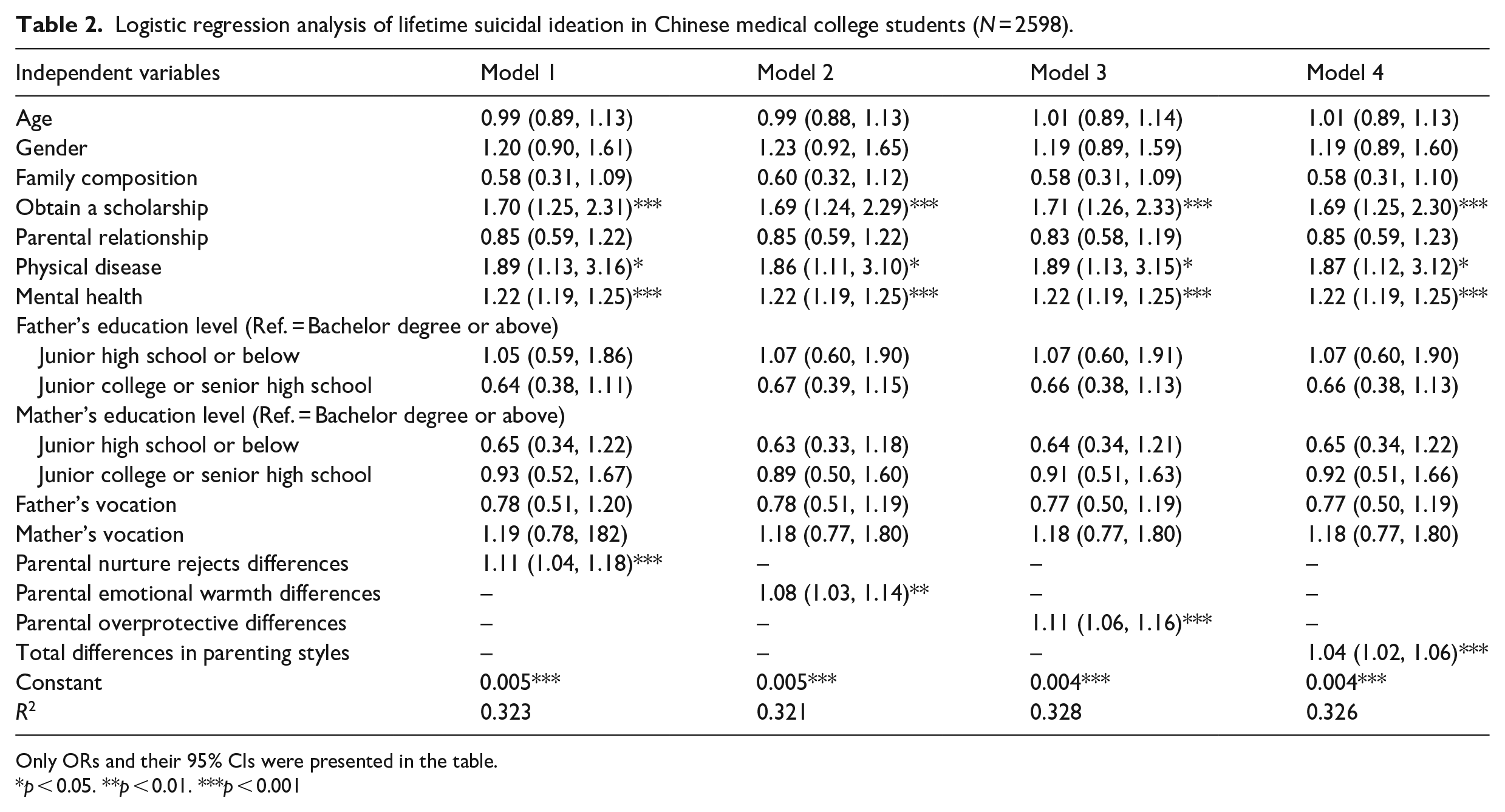
In Table 2, we conducted four models to establish the association between parental parenting style differences and LSI in medical college students. The results of multiple logistic regression showed that LSI was associated with parental parenting style differences (OR = 1.04, 95% CI = 1.02, 1.06). Specifically, the LSI was associated with parental nurture rejects differences (OR = 1.11, 95% CI = 1.04, 1.18), parental emotional warmth differences (OR = 1.08, 95% CI = 1.03, 1.14), and parental overprotective differences (OR = 1.11, 95% CI = 1.06, 1.16), respectively.
Logistic regression analysis of lifetime suicidal ideation in Chinese medical college students (N = 2598).
Only ORs and their 95% CIs were presented in the table.
p < 0.05. **p < 0.01. ***p < 0.001
Binary logistic regression analysis for higher father’s parenting styles and lifetime suicidal ideation
In Table 3, we conducted five models to establish the association between higher father’s parenting styles and LSI in medical college students. The unadjusted model1 shows that higher father’s parenting styles was not significantly associated with lifetime suicide ideation (OR = 0.98, 95% CI = 0.95, 1.01). Specifically, higher father’s nurture rejects (OR = 0.95, 95% CI = 0.89, 1.02), higher father’s emotional warmth (OR = 1.01, 95% CI = 0.94, 1.07), and higher father’s overprotective (OR = 0.96, 95% CI = 0.91, 1.01) were all not significantly associated with lifetime suicide ideation. The results of multiple logistic regression showed that LSI was still not significantly associated with higher father’s parenting styles (OR = 0.99, 95% CI = 0.95, 1.02). Specifically, the LSI was not associated with higher father’s nurture rejects (OR = 0.98, 95% CI = 0.90, 1.05), higher father’s emotional warmth (OR = 1.02, 95% CI = 0.96, 1.09), and higher father’s overprotective (OR = 0.95, 95% CI = 0.89, 1.01), respectively.
Logistic regression analysis of father’s high level in parenting styles in Chinese medical college students (N = 2598).
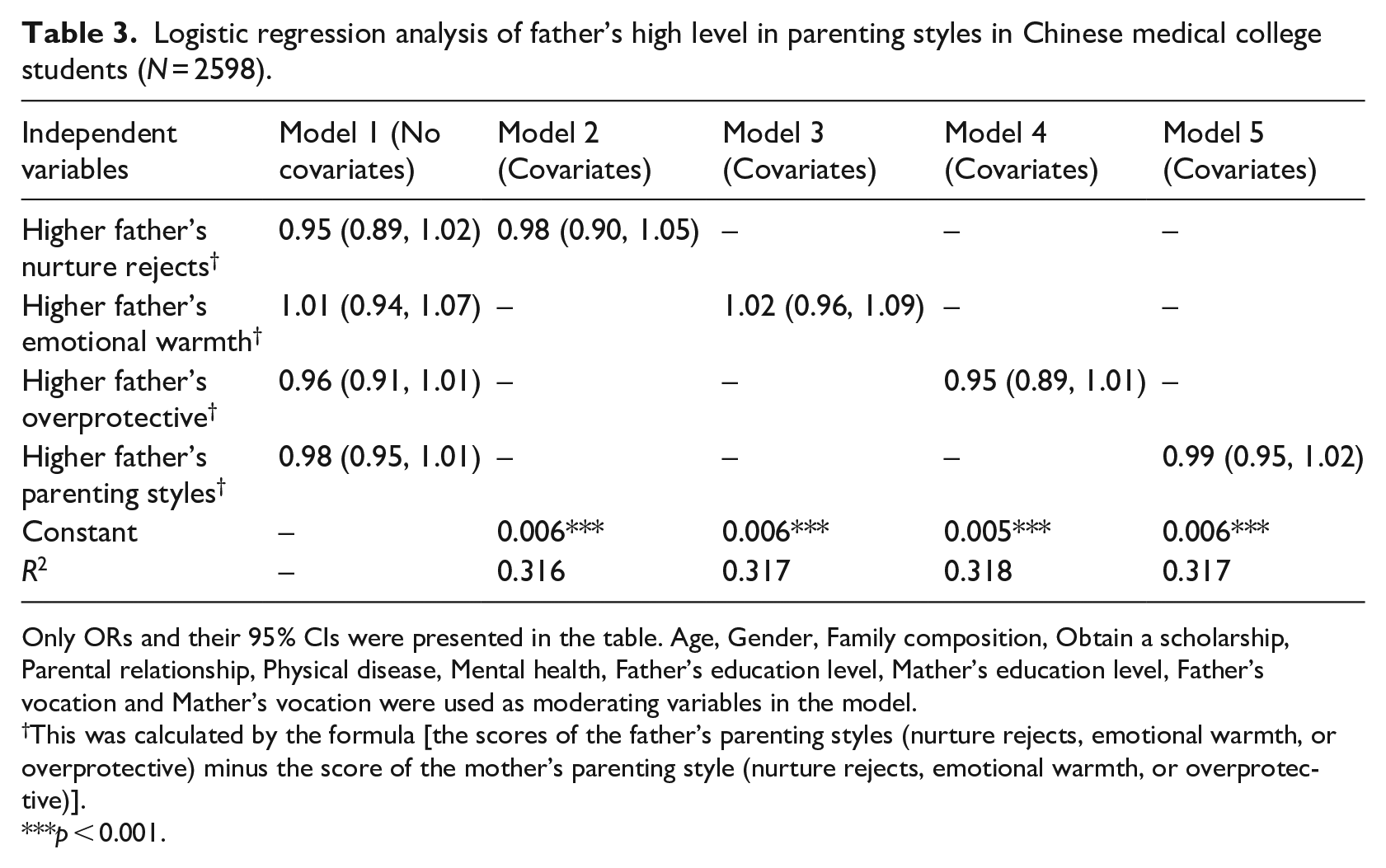
Only ORs and their 95% CIs were presented in the table. Age, Gender, Family composition, Obtain a scholarship, Parental relationship, Physical disease, Mental health, Father’s education level, Mather’s education level, Father’s vocation and Mather’s vocation were used as moderating variables in the model.
This was calculated by the formula [the scores of the father’s parenting styles (nurture rejects, emotional warmth, or overprotective) minus the score of the mother’s parenting style (nurture rejects, emotional warmth, or overprotective)].
***p < 0.001.
Discussion
In this study, we found that the prevalence of suicidal ideation was 10.5%. Moreover, total differences in parenting styles, parental nurture rejects differences, parental emotional warmth differences, and parental overprotective differences, obtain a scholarship, physical disease and mental health were significant associated with LSI among medical college students. However, it was interesting that all the same kinds of higher father’s parenting styles (express the higher father’s parenting styles than mother) were not associated with SI.
The prevalence of LSI among Chinese medical college students of this study was close to another survey conducted in Germany medical college students (7.4%; Wege et al., 2016). However, it was much lower than that Chinese medical students (17.9%; Sun et al., 2017) and American medical students (29.9%; MacLean et al., 2016). Because of the different levels of research backgrounds and the time point of definition, the previous research has shown a very high prevalence of LSI in medical students, ranging from 2.9% to 53.6% (Coentre and Góis, 2018).
The main topic of this study was to analyze the relationship between parenting styles differences and LSI among medical college students in China. The study showed that the differences in parenting styles were related to LSI among medical college students. A previous research has indicated that living in a family with inconsistent parenting styles played an important role on the increasing risk of future hospitalisation with deliberate self-harm in children (Mitrou et al., 2010) and the study assessed parenting styles only by asking a simple parenting style question, with answers that could be chosen from encouraging, coercive, neutral, or inconsistent. In contrast, the 21-item S-EMBU-C scale was used in our study to score the parenting styles of medical students’ father and mother in detail in three aspects: rejection, emotional warmth, and overprotection, so as to obtain the differences in parental parenting styles.
The present study found that differences in parenting styles in rejection, emotional warmth, and overprotection, as well as total differences in parenting styles combined with the three, increased the risk of LSI among medically students. When there are differences in parental parenting styles, there may be more psychological and emotional contradictions for medical students, which makes them suffer more psychological pain and pressure. Combined with Zhang proposed the strain theory of suicide to explain the deep motivation of suicide (Zhang and Lester, 2008). The theoretical hypothesis that individual experienced a special psychological pressure before suicide, which was formed by contradictory and competitive pressures, and the theory gradually gained recognition in the academic circle (Lew et al., 2020; Zhang et al., 2017). In combination with this study, when there are differences in parental parenting styles, non-contradictory, and reconcilable pressure (i.e. torque) will be caused to students, which will lead to inner struggles and pains of students and further promote the formation of SI. In addition, the interpersonal psychological theory of suicide (IPTS) also suggests that differences in parenting styles may be related to suicide, as studies have shown that IPTS is able to account for the inconsistent effects of parental parenting styles on senior students suicide-related behaviors and suggest that parental parenting styles are associated with reduced senior students suicide attempts (Cero and Sifers, 2013). Other studies have discussed how different parenting styles may be associated with suicide in terms of negative urgency and emotion dysregulation (Anestis and Joiner, 2011).
In addition, we also analyzed the relationship between the higher score of father’s parenting style than mother’s and LSI. The results showed that higher father’s parenting styles were always not significantly associated with lifetime suicide ideation either before or after the addition of adjustment variables. Combined with the above findings of this study, the differences in parental parenting styles were related to LSI among Chinese medical college students. Further, it was differences in parenting styles between parents rather than unilateral higher father’s parenting styles than mother that increased the risk of LSI among medical students, which further proves the findings that differences in parenting styles increase the risk of LSI. This is also a reminder to us that parents should strengthen communication with each other in the process of raising their children and try to maintain the same parenting style or reduce the differences in parenting style so as to reduce the SI of their children.
Many previous studies have reported the effect of mental health on suicide ideation. For example, a study of 16- to 19-year-olds in Malaysia found that psychological factors such as depression, anxiety, and stress were significantly associated with SI, and depression could be a predictor of SI (Ibrahim et al., 2014). The results also show that the prevalence of depression, anxiety, and stress was 11.1%, 10.0%, and 9.5%, respectively. Another study in college students also showed that stress were significantly related to SI, and stressful life events can significantly predicted SI (Wilburn and Smith, 2005). These are consistent with the findings of this study that mental health is significantly associated with suicidal ideation among medical students. Compared with students of other majors, Chinese medical college students have higher academic pressure and higher depression rates than the general population (Dahlin et al., 2005), which may be one of the reasons why they have higher rates of SI.
We also found that physical disease, mental health and obtain a scholarship were associated with LSI. The findings are consistent with previous studies have reported that physical disease and mental health were associated with higher levels of SI (Kavalidou et al., 2017). Previous studies have shown that physical diseases increased the risk of mental disorders (Henriksson et al., 1995; Qin et al., 2014) and varied as a function of the presence of subsequent mental disorder. Moreover, the physical diseases like cancer, asthma, musculoskeletal, and cardiovascular disease may play a role in the development of suicidal behaviors (Bolton et al., 2015; Webb, 2012). Further, numerous studies have found depression to be the most common psychiatric diagnosis among chronic physically ill patients, being associated with a higher suicide risk (Anguiano et al., 2012; Pompili et al., 2014). We also found a strong association between obtain a scholarship and LSI, and the association was statistically significant. Although some previous studies showed that poor academic performance is a risk factor for SI (Kim et al., 2015; Ulusoy and Demir, 2005), but most of their research has focused on teenagers aged 16 and under who don’t have much academic pressure. Obtaining a scholarship means better academic performance and more academic stress for college medical students who may have a higher risk of suicide. Specifically, students may experience an increased suicide risk when their actual performance in the examination falls short of their expected performance, even if their actual test scores are high compared to other students’, which is consistent with our study. For example, students whose national ranks in the high-stakes college entrance examination fell short of their expected national ranks exhibit a higher likelihood of having SI than those whose performance was better than expected (Wang, 2016).
There are also several limitations that should be addressed when we interpreting these results. First, as a cross-sectional study, causal inferences are difficult to justify. Second, the data was collected from two medical colleges in Shandong Province, China, and the generalization of the findings has to be done cautiously. Third, all the data were collected from the students, and thus the information about their parents and families may have some biases. Last, the way in which having a physical diseased is asked is relatively simple and cannot distinguish severe physical diseases.
Conclusions
Despite these limitations, the study can still contribute to our understanding about the effect of parental parenting styles differences on LSI among medical college students in China. The major finding that the differences in parental parenting styles were associated with LSI is critical, reminding us of the importance of consistent parenting style for suicide prevention, which can be translated into practical measures for suicide prevention in China as well as elsewhere in the world.
Research Data
sj-sav-1-hpq-10.1177_13591053211044532 – Supplemental material for Parents parenting styles differences were associated with lifetime suicidal ideation: Evidences from the Chinese medical college students
Supplemental material, sj-sav-1-hpq-10.1177_13591053211044532 for Parents parenting styles differences were associated with lifetime suicidal ideation: Evidences from the Chinese medical college students by Zhen Gui, Xuehan Ren, Xiao Li, Chengchao Zhou and Long Sun in Journal of Health Psychology
Footnotes
Appendix
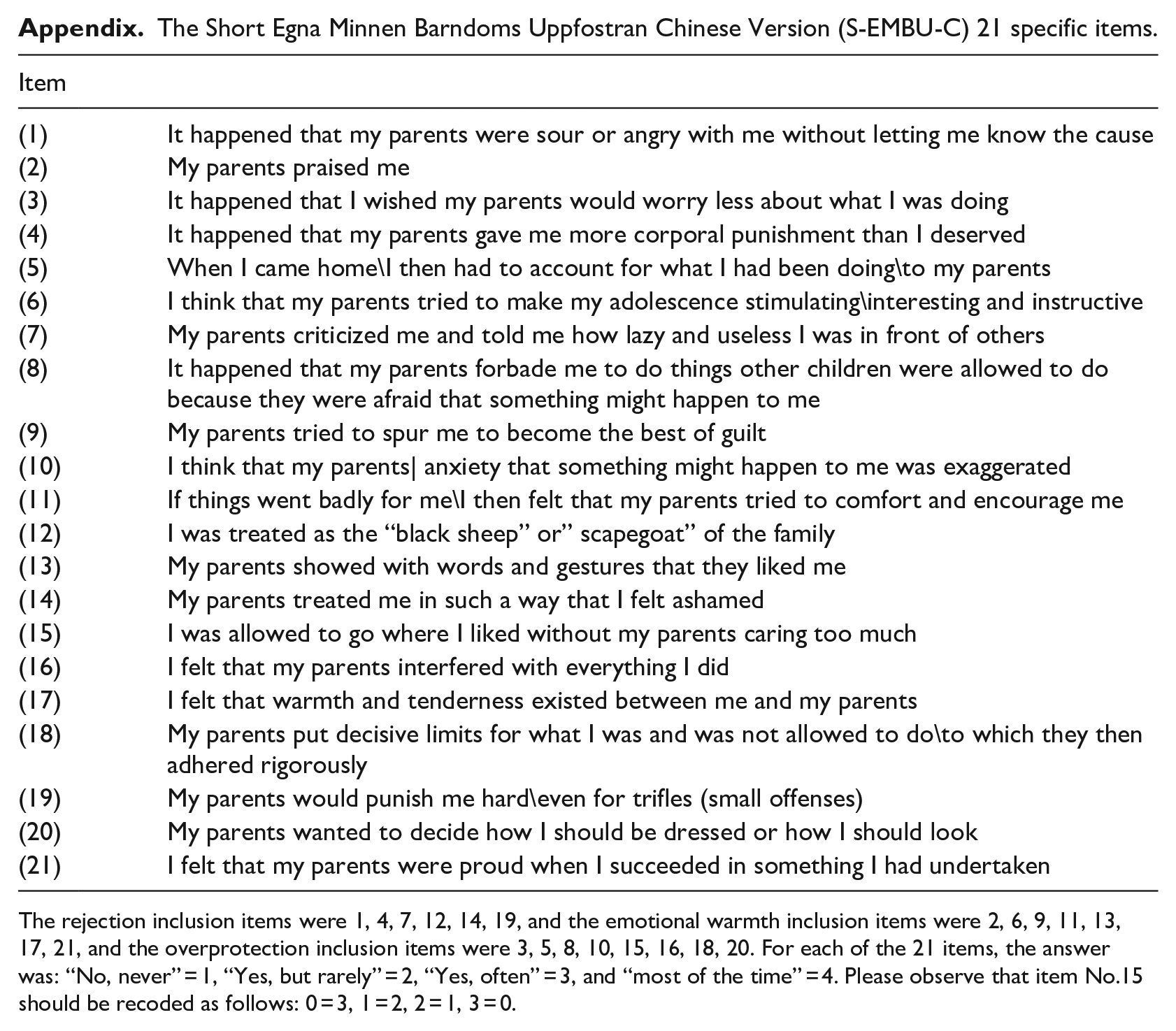
The Short Egna Minnen Barndoms Uppfostran Chinese Version (S-EMBU-C) 21 specific items.
| Item | |
|---|---|
| (1) | It happened that my parents were sour or angry with me without letting me know the cause |
| (2) | My parents praised me |
| (3) | It happened that I wished my parents would worry less about what I was doing |
| (4) | It happened that my parents gave me more corporal punishment than I deserved |
| (5) | When I came home\I then had to account for what I had been doing\to my parents |
| (6) | I think that my parents tried to make my adolescence stimulating\interesting and instructive |
| (7) | My parents criticized me and told me how lazy and useless I was in front of others |
| (8) | It happened that my parents forbade me to do things other children were allowed to do because they were afraid that something might happen to me |
| (9) | My parents tried to spur me to become the best of guilt |
| (10) | I think that my parents| anxiety that something might happen to me was exaggerated |
| (11) | If things went badly for me\I then felt that my parents tried to comfort and encourage me |
| (12) | I was treated as the “black sheep” or” scapegoat” of the family |
| (13) | My parents showed with words and gestures that they liked me |
| (14) | My parents treated me in such a way that I felt ashamed |
| (15) | I was allowed to go where I liked without my parents caring too much |
| (16) | I felt that my parents interfered with everything I did |
| (17) | I felt that warmth and tenderness existed between me and my parents |
| (18) | My parents put decisive limits for what I was and was not allowed to do\to which they then adhered rigorously |
| (19) | My parents would punish me hard\even for trifles (small offenses) |
| (20) | My parents wanted to decide how I should be dressed or how I should look |
| (21) | I felt that my parents were proud when I succeeded in something I had undertaken |
The rejection inclusion items were 1, 4, 7, 12, 14, 19, and the emotional warmth inclusion items were 2, 6, 9, 11, 13, 17, 21, and the overprotection inclusion items were 3, 5, 8, 10, 15, 16, 18, 20. For each of the 21 items, the answer was: “No, never” = 1, “Yes, but rarely” = 2, “Yes, often” = 3, and “most of the time” = 4. Please observe that item No.15 should be recoded as follows: 0 = 3, 1 = 2, 2 = 1, 3 = 0.
Acknowledgements
We would like to thank all participants and staff for their cooperation at the study site. We also thank for the research team from Shandong University for their field work in the data collection.
Authors’ contributions
All authors read and approved the final manuscript. ZG analyzed the data and wrote the manuscript, XL and HX participated in the process of the data analysis, LS collected the data, CZ and LS designed the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (71603149 and 71974114); the Shandong Provincial Natural Science Foundation (ZR2016HQ01); and Shandong University (IFYT18033).
Data sharing statement
The current article includes the complete raw data-set collected in the study including the participants’ data set, syntax file, and log files for analysis. Pending acceptance for publication, all of the data files will be automatically uploaded to the Figshare repository.
Research ethics and patient consent
The Institutional Review Board of Shandong University School of Public Health approved the study protocol before data collection (ref.:20181220). Written informed consent was obtained from all of the participants.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.