
Abstract
There is a knowledge gap when treating comorbid chronic pain and posttraumatic stress disorder (PTSD) during the COVID-19 pandemic. Addressing this gap, 169 individuals (57.4% female), aged 39.8 years were recruited based on levels of pain-related disability and PTSD symptoms. Participants were assessed prior to, and during, the COVID-19 pandemic. Improvements in pain-related disability were marginally attenuated for the comorbid group, compared to the chronic pain group. Results show that some condition-specific symptoms may not have been affected by the COVID-19 pandemic. Cautious interpretation is warranted due to only two time points and the lack of a diverse sample.
On March 11, 2020, the World Health Organization (WHO) classified the novel Coronavirus-19 (COVID-19) as a pandemic. Along with the devastating death toll, COVID-19 has upended the way Americans engage with their health providers (Smith et al., 2020), potentially impacting their ability to manage their symptoms. If medical or psychological treatment is not considered urgent, it is possible that treatment was delayed or the modality altered (e.g. from in-person to telehealth; Moring et al., 2020; Piraccini et al., 2020). Delayed or altered treatment could then lead to more severe symptomology. Early research on the pandemic focused on the general population, showing how exposure to the pandemic is associated with more severe symptoms of depression, anxiety, suicidal ideation, and posttraumatic stress disorder (PTSD; Czeisler et al., 2020; Guo et al., 2020; Liu et al., 2020; Tang et al., 2020a, 2020b; Wu et al., 2020). Among those with mental and physical health conditions, the research is less robust, resulting in clinicians having fewer certainties as to the needs of patients during the pandemic. This leads to a clinical treatment gap during the pandemic. A better understanding of how symptoms present among patients with chronic pain and PTSD during the pandemic may help clinicians make important clinical decisions.
Chronic pain, defined as experiencing consistent pain for at least 3 months (Treed et al., 2015), and PTSD are partially characterized by several processes, including avoidance of pain or PTSD-specific stimuli (e.g. thoughts about the trauma), negative affect, and disruption of identity (Ravn et al., 2018; Reed et al., 2021; Sharp and Harvey, 2001). A combination of pharmacological and non-pharmacological treatments is recommended for both disorders when treated separately (American Psychological Association, 2017; Gatchel et al., 2014). The pandemic has the potential to disrupt these services (Boyraz and Legros, 2020; Turolla et al., 2020), which may have an effect on mood, pain-related disability, and PTSD symptoms. Distress specifically related to COVID-19, such as news reports on the pandemic and fears about getting sick from COVID-19 may put people with chronic pain and/or PTSD at risk of more severe pain and/or PTSD symptoms (Clauw et al., 2020).
The combination of chronic pain and PTSD is particularly problematic for multiple reasons. Comorbid chronic pain and PTSD are highly prevalent (Akhtar et al., 2019; Asmundson et al., 2002; Hooten, 2016) and associated with higher pain severity, pain-related disability, medication use, and mental health services use compared to chronic pain only (Akhtar et al., 2019; Lehinger et al., 2020; Outcalt et al., 2014). Among PTSD populations, those with chronic pain are more likely to report higher pain severity and PTSD symptoms (Beckham et al., 1997; Shipherd et al., 2007). As the pandemic continues, those with pre-existing conditions are presented with new forms of physical and mental stressors and may be at a greater risk for mental health problems compared to healthy individuals (Fiorillo and Gorwood, 2020). Moreover, individuals with physical disabilities may be particularly affected by the pandemic’s disruption in their daily activities (Boyraz and Legros, 2020). For individuals with pain and PTSD, their allostatic load, or the combined effect of comorbid illnesses (McEwen, 1998; Sterling and Eyer, 1988), likely decreases their ability to manage novel stressors (Guidi et al., 2021). Pain and PTSD management can be time-consuming, tiring, and stressful, and the addition of pandemic-related stressors may overburden patients, resulting in more severe physical and psychological symptoms (cf. Guidi et al., 2021). Indeed, the addition of depressive symptoms to anxiety, fear-avoidance, and pain catastrophizing is associated with greater pain-related disability (McGeary et al., 2020). Moreover, a recent review highlights how allostatic load is linked to fibromyalgia, physical health (e.g. diabetes and cardiovascular disease), depression, lower mental health, and traumatic experiences (Guidi et al., 2021). In sum, a higher allostatic load is (1) present for those with mental and physical disorders, and (2) linked to more severe symptomology. Therefore, it would be expected that those with comorbid chronic pain and PTSD, compared to individuals with just one of these disorders, would experience more severe symptoms with the addition of the novel stressor of the COVID-19 pandemic. However, to the best of our knowledge, this empirical question has yet to be examined.
The present study
The present study attempts to fill this gap through the implementation of a longitudinal cohort study design, whereby PTSD symptoms, pain-related disability, and mood were assessed prior to the novel coronavirus pandemic (January 14–February 12, 2020) and during its active phase in the United States (May 5–May 13, 2020). We hypothesized that (1: mood) individuals with comorbid chronic pain and PTSD would endorse more negative changes in mood between Time 1 and Time 2 compared to those with chronic pain only, PTSD only, and individuals in the control group; (2: mood) individuals with chronic pain only or PTSD only would endorse more negative changes in mood between Time 1 and Time 2 compared to individuals in the control group; (3: pain-related disability) individuals with comorbid chronic pain and PTSD would endorse a more severe increase in pain-related disability between Time 1 and Time 2 compared to those with chronic pain only; (4: PTSD symptoms) individuals with comorbid chronic pain and PTSD would endorse a more severe increase in PTSD symptoms between Time 1 and Time 2 compared to those with PTSD only.
Method
Procedure
All participants were recruited through CloudResearch (Litman et al., 2017), an online platform able to obtain high-quality data for patient populations challenging to reach. A total of 897 individuals were screened for eligibility and categorized into one of four groups: control group (scored in the lower quartile of the sample of both the Oswestry Disability Index (ODI; 8%) and Posttraumatic Stress Disorder checklist-5 (PCL-5; total score 15 or lower)), chronic pain only (endorsed 21% or more on ODI, which is indicative of at least moderate pain-related disability (Breitenseher et al., 1996; Michigan State University, 2021) and in the lower quartile of the PCL-5), PTSD only (total score 37 or above on the PCL-5, which is indicative of a potential PTSD diagnosis (Blevins et al., 2015), and in the lower quartile of the ODI), and comorbid chronic pain and PTSD (scored 21% or greater on the ODI and 37 or above on the PCL-5). Participants were paid $0.30 to complete the screening. Quartiles were chosen in order to clearly delineate those who did and did not endorse chronic pain and/or pain-related disability, and based on prior published methodology (Vail et al., 2019, 2020). Participants were excluded if they were not located in the U.S., and participants were not excluded based on other diagnostic criteria (e.g. other mental health disorders). These criteria resulted in 587 individuals being offered the opportunity to participate in the study. Pre-pandemic data collection took place on January 14–February 12, 2020, and follow-up data was collected on May 5–May 13, 2020. Participants were paid $2.00 to complete the assessments pre-COVID-19 pandemic (Time 1) and $3.00 to complete the assessment during the COVID-19 pandemic (Time 2). A total of 169 individuals completed Time 1, and a total of 110 individuals completed both Time 1 and Time 2. All 169 individuals were included in the analysis (29% of the 587 initially invited to participate; see data analysis strategy for missing data handling). For more detailed information related to data collection procedures and original study design, see https://osf.io/hsyxv. The consort and pre-registered hypotheses for the present study may be accessed at https://osf.io/a35m4/ and https://osf.io/7hjdb, respectively. Study methods were approved by the appropriate Institutional Review Board and informed consent waived.
Participants
A total of 169 individuals (57.40% female) aged 39.76 years (SD = 13.10; range: 21–82) were enrolled in the initial study. Most participants were White (83.43%); endorsed a heterosexual sexual orientation (86.39%); and many endorsed either some college (23.67%) or having completed a 4-year degree (32.54%). Please see Table 1 for demographic information.
Sample characteristics.
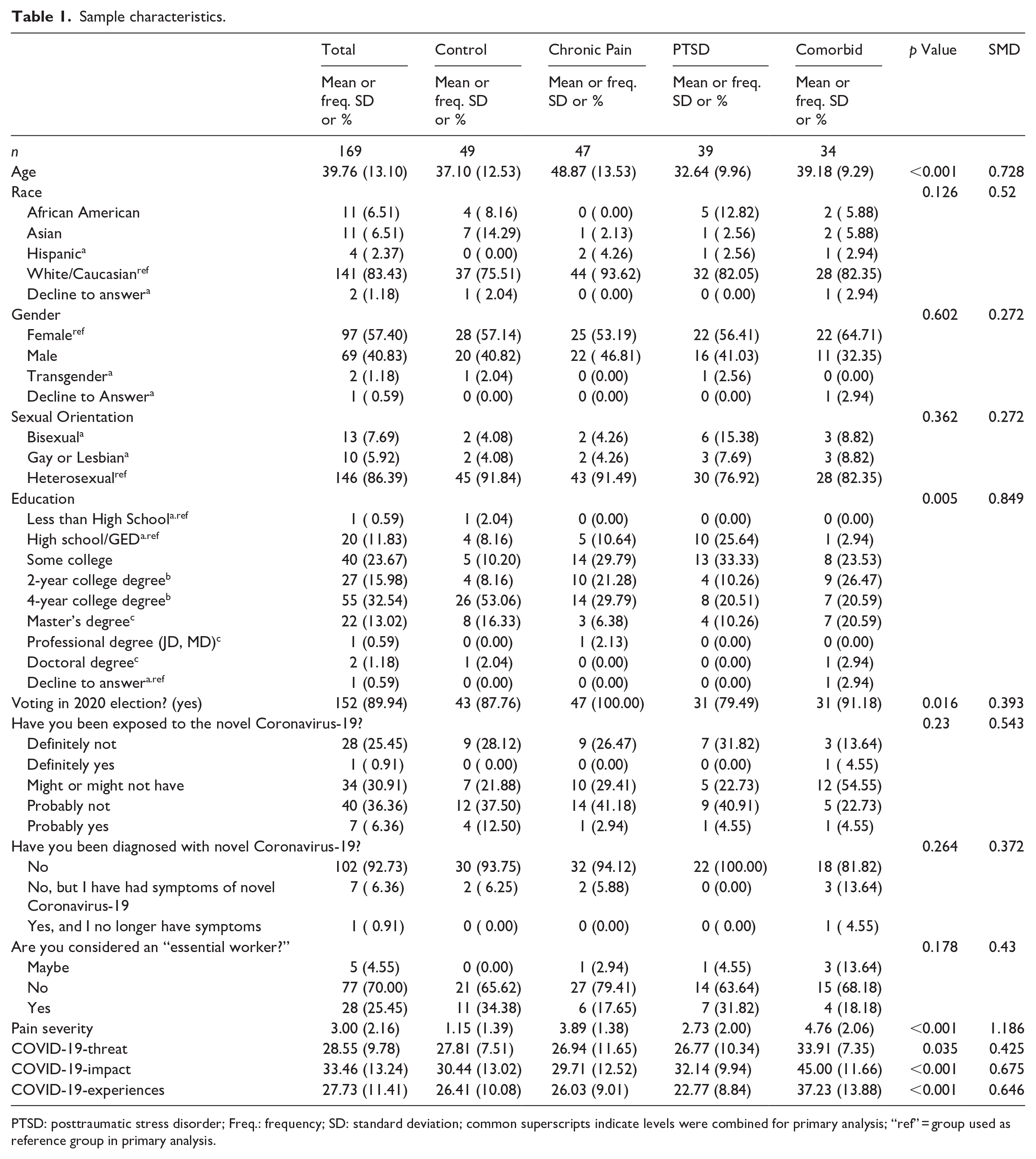
PTSD: posttraumatic stress disorder; Freq.: frequency; SD: standard deviation; common superscripts indicate levels were combined for primary analysis; “ref” = group used as reference group in primary analysis.
Measures
Demographics
Participants provided information on age, race, gender, sexual orientation, and education.
Voting
We asked participants whether they planned on voting in the 2020 Presidential election in the event that this decision was associated with variables relevant to one’s self-identity. Self-identity was the focus of the pre-pandemic original study design. Participants could respond “Yes” or “No.”
Pain severity
The Modified Brief Pain Inventory Short Form (mBPI-SF; Cleeland, 1991; α = 0.92 at Time 1) assessed pain at its worst, least, average, and current pain (0–10 scale). Items were averaged for analyses, with higher scores indicating worse pain severity.
Pain-related disability
A modified version of the Oswestry Disability Index (ODI; Fairbank et al., 1980; Fritz and Irrgang, 2001; 10 items on a 0–5 scale) measured perception of disability due to pain using 10 life domains (α = 0.94, Time 1; α = 0.93, Time 2). The modified version asks about social life, instead of sex life (Item 8). Results are converted into a percentage of disability. Moderate disability is indicated by 21% to 40%; severe disability is indicated by 41% to 60%; and more severe disability over 60% (Michigan State University, 2021).
PTSD
The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5) assessed posttraumatic stress disorder symptoms across the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (5th Edition)’s criteria (American Psychiatric Association, 2013; Weathers et al., 2013); 20 items, 0–4 scale; α = 0.98, Time 1; α = 0.96, Time 2. A score of 31–33 on the PCL-5 is indicative of a provisional PTSD diagnosis (Blevins et al., 2015; U.S. Department of Veterans Affairs, 2020).
Mood
The Mental Health Inventory-5 (MHI-5) uses five items (6-point scale); α = 0.90, Time 1; α = 0.92, Time 2; (Berwick et al., 1991; California Mental Health Services Authority, 2016) to describe one’s overall mood relevant to anxiety and depression. Higher scores indicate more positive mood. We chose this measure because it captures overall mood and is not specific to a DSM-5 diagnosis of anxiety or depression. The MHI-5 has previously been used in pain (Zhang et al., 2021) and PTSD (Nishimi et al., 2021) samples.
COVID-19 information
Items included information on participants’ and others’ exposure to COVID-19 and whether they had been diagnosed with the virus. Items also included the extent to which the pandemic had interfered with treatment and/or medication. See Tables 1 and 2 for more item information.
Frequencies of COVID-19 interference.
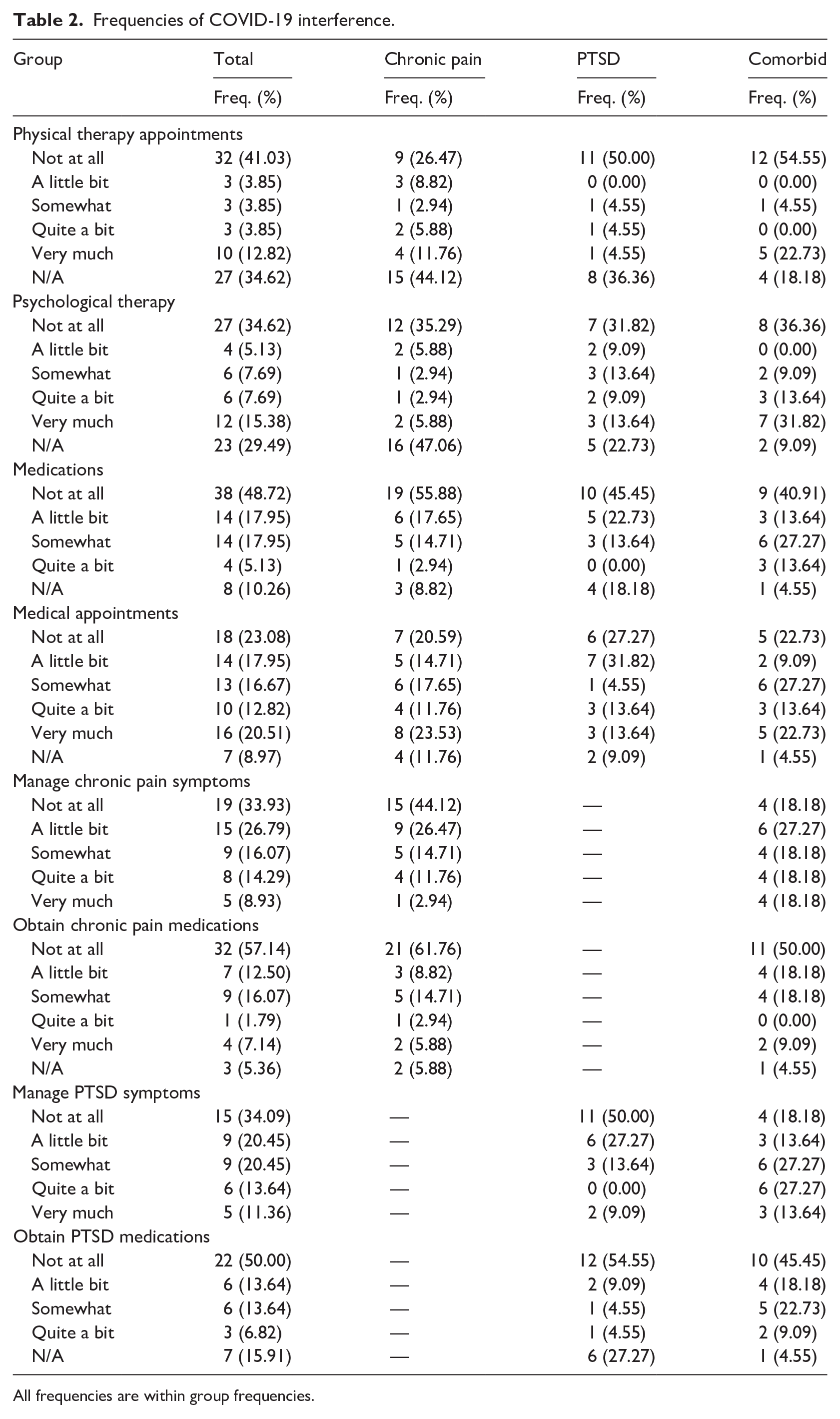
All frequencies are within group frequencies.
COVID-19 threat
Thoughts and feelings about getting sick and feeling threatened by COVID-19 were assessed (six items; α = 0.90; e.g. “I am afraid of the coronavirus.”; Conway et al., 2020).
COVID-19 impact
Measure used nine items to assess how COVID-19 has affected individuals’ income, resources, and emotional/cognitive health (α = 0.85; e.g. “The Coronavirus (COVID-19) has NOT affected my ability to get needed resources.”; Conway et al., 2020).
COVID-19 experiences
Items assess the extent to which people have been diagnosed/known someone who has been diagnosed with COVID-19/felt symptomatic of COVID-19 and been sick with something other than COVID-19. The measure also assesses one’s engagement with COVID-19 news (α = 0.76; e.g. “I have been in close proximity with someone who has been diagnosed with coronavirus (COVID-19).”; Conway et al., 2020).
Data analytic strategy
Random intercept ANOVAs (Raudenbush and Bryk, 2002) were implemented for all hypotheses testing. Pain severity at Time 1 was included as a covariate for all analyses. We also included race, gender, sexual orientation, and education as covariates. Categories of covariates were combined to assist in model estimation (See Table 1). Full information maximum likelihood accounted for missing data. Age and whether or not one was planning on voting in the 2020 presidential election predicted missingness; therefore, both variables were included in the models to assist in attenuating bias (Enders, 2010). We deviated from our preregistered data analysis plan due to estimation problems; however, our conceptual hypotheses remained the same. Our data analysis plan also deviated in the following ways: we decided to use full information maximum likelihood to account for missing data, as opposed to multiple imputation; pain severity was included in all analyses, as opposed to only in sensitivity analyses. Finally, because we assessed three outcomes, we chose p < 0.0166 (α = 0.05/3 outcomes = .0166) as the inference criteria for regression models (as opposed to p < 0.025, α = 0.05/2 = 0.025). Pearson correlations were used to examine correlations between COVID-19 variables and outcome variables.
Results
Sample characteristics
The control group included 49 individuals who endorsed low baseline levels of pain-related disability (M = 1.96%; SD = 2.78%) and PTSD symptoms (M = 4.35, SD = 4.54). In the chronic pain only group (n = 47), participants averaged 38.60% (SD = 14.52%) pain-related disability, which is considered moderately disabled (Michigan State University, 2021), and 6.66 (SD = 5.16) on the PCL-5. In the PTSD only group (n = 39), pain-related disability averaged 2.46% (SD = 3.06%), and scores were high on the PCL-5 (M = 52.18; SD = 11.53). Those in the comorbid group (n = 34) endorsed high pain-related disability (M = 35.35%; SD = 12.66%) and high PTSD symptoms (M = 53.97; SD = 10.40). Mood scores at baseline were the following for each group: control group, M = 23.31 (SD = 4.53); chronic pain only group, M = 23.62 (SD = 4.88); PTSD only group, M = 16.05 (SD = 5.14); and comorbid group, M = 16.41 (SD = 4.77). See Table 1 for baseline characteristics. At Time 2, the chronic pain (M = 29.24%; SD = 18.08%) and comorbid group (M = 33.18; SD = 19.29) continued to endorse moderate pain-related disability. At Time 2, the comorbid group also endorsed high PTSD symptoms (M = 38.23; SD = 17.65). However, the PTSD only group endorsed PTSD symptoms approaching, but lower, than the recommended cutoff scores for a provisional diagnosis (M = 30.09; SD = 17.20).
Treatment and medication interruptions
A substantial number of participants in the three groups (i.e. chronic pain, PTSD, or comorbid group) reported they were not engaged (i.e. reported not applicable) in physical therapy appointments (35%) or psychological therapy (29%). For PTSD patients, 18% indicated they did not use general medications (i.e. reported not applicable), and 27% indicated they did not use PTSD-specific medications (i.e. reported not applicable). Although 44% of participants indicated the pandemic interfered with managing their chronic pain symptoms “Not at All” in the chronic pain group, only 18% indicated this in the comorbid group. Similarly, while 50% of participants indicated the pandemic interfered with managing their PTSD symptoms “Not at All” in the PTSD group, only 18% indicated this in the comorbid group. See Table 2 for all descriptive statistics for these variables.
COVID-19, pain-related disability, and PTSD symptoms
Correlations between COVID-19 variables and outcome variables indicate that more COVID-19 Threat was significantly related to lower mood at Time 2. Being impacted more by COVID-19 was related to worse outcomes (mood, pain-related disability, and PTSD symptoms) at Time 2. Having more COVID-19 experiences was related to worse pain-related disability and PTSD sy,ptoms at Time 2. See Table 3 for all correlations and relevant variable descriptive statistics.
Correlations, standard deviations, and means of COVID-19 and outcome variables.
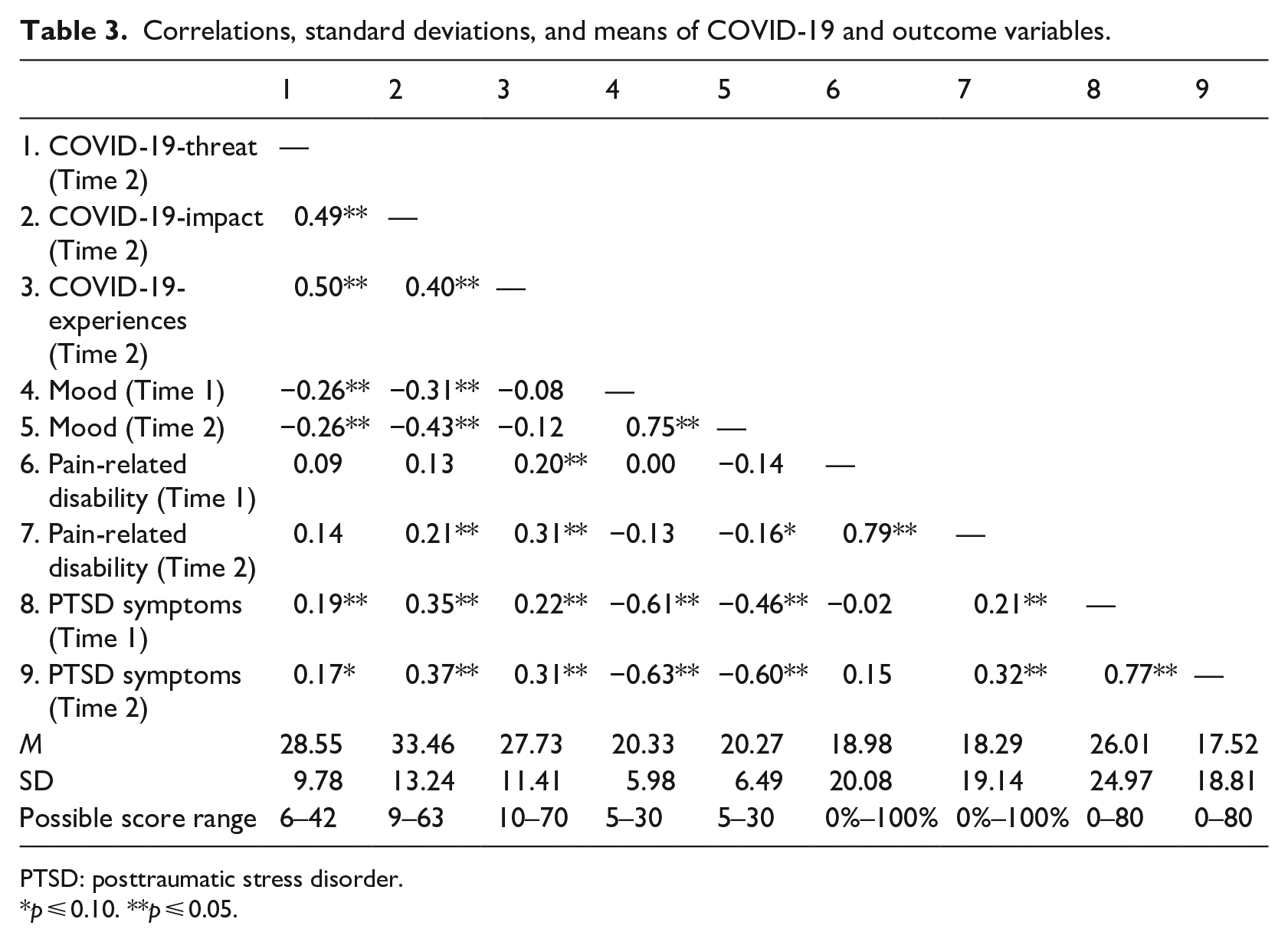
PTSD: posttraumatic stress disorder.
p ⩽ 0.10. **p ⩽ 0.05.
Mood
Hypothesis 1 was not supported, as changes in mood over time in the comorbid group did not differ from changes in mood over time in the control group (b = −0.51, SE = 1.14, p = 0.657, 95% CI: −2.72, 1.94) or chronic pain only group, (b = 0.24, SE = 1.13, p = 0.836, 95% CI: −1.82, 2.44), and was marginally different from the PTSD only group (b = 2.26, SE = 1.24, p = 0.071, 95% CI: 0.02, 4.77). Hypothesis 2 was not supported, as changes in mood over time for the chronic pain only group did not differ from changes in mood for the control group (b = 0.75, SE = 1.02, p = 0.467, 95% CI: −1.29, 2.91). Moreover, although changes in mood over time for the PTSD only group significantly differed from changes in mood over time for the control group (b = 2.77, SE = 1.14, p = 0.017, 95% CI: 0.67, 5.01), a simple slopes analysis showed that this interaction represented the difference between a non-significant decrease in mood in the control group (−1.13, SE = 0.73, p = 0.125) and a marginal increase (improvement) in mood in the PTSD group (1.64, SE = 0.88, p = 0.064). Tukey post hoc contrasts are located in Table 4. Regression coefficients are located in Table 5.
Estimated marginal means.
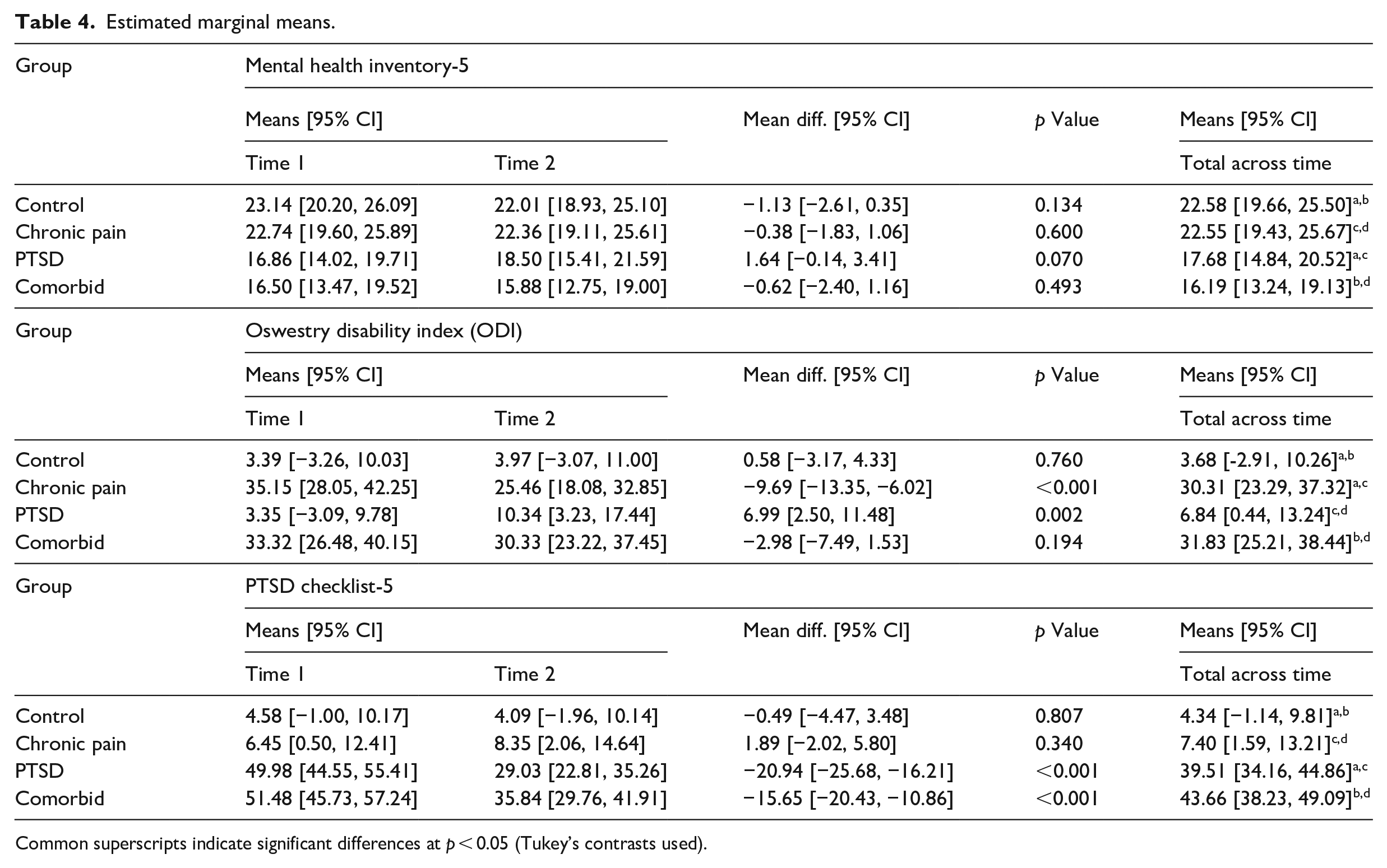
Common superscripts indicate significant differences at p < 0.05 (Tukey’s contrasts used).
Model coefficients.
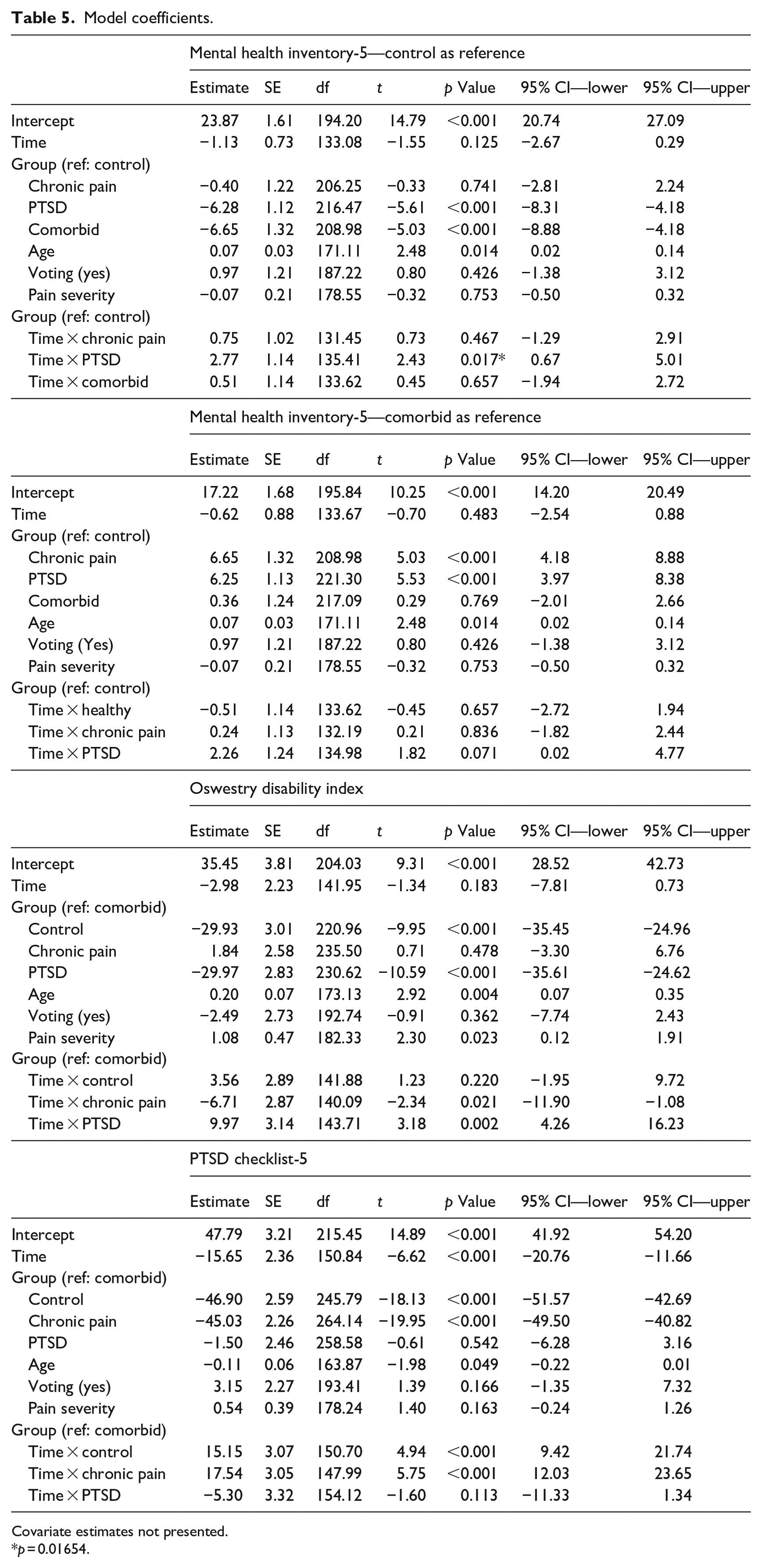
Covariate estimates not presented.
p = 0.01654.
Pain-related disability
We hypothesized that those in the comorbid group would show a more severe increase in disability over time compared to the chronic pain group (Hypothesis 3). This hypothesis was not supported, as a simple slopes analysis showed that the chronic pain only group endorsed improvements in pain-related disability over time (b = −9.69, SE = 1.81, p < 0.001) and the comorbid group remained stable (−2.98, SE = 2.23, p = 0.183). The difference between these two groups’ slopes (b = −6.71, SE = 2.87, p = 0.021, 95% CI: −11.90, −1.08) was significant at p < 0.05, but marginally significant with our pre-planned alpha correction. Tukey post-hoc contrasts can be found in Table 4. Regression coefficients can be found in Table 5.
PTSD symptoms
We hypothesized that those in the comorbid group would endorse a more severe increase in PTSD symptoms between Time 1 and Time 2 compared to those with PTSD only (Hypothesis 4). This hypothesis was not supported, because a simple slopes analysis showed that both the comorbid group (−15.65, SE = 2.36, p < 0.001) and PTSD only group (−20.94, SE = 2.34, p < 0.001) endorsed significant decreases in PTSD symptoms between Time 1 and Time 2. Moreover, the between-group difference in changes over time (i.e. their slopes) was non-significant (b = −5.30, SE = 3.32, p = 0.113, 95% CI: −11.33, 1.34). Tukey post hoc contrasts are located in Table 4. Regression coefficients are in Table 5.
Discussion
Our initial hypotheses were predicated on research that implicates the compounding effect of the chronic pain and PTSD comorbidity on mood, disability, and PTSD symptoms (Beckham et al., 1997; Benedict et al., 2020). Our hypotheses related to mood were not supported, suggesting that the pandemic has not significantly altered the mood of some individuals. Although unexpected, there are several possibilities for these results. For one, we utilized an online sample who may have been already accustomed to being at home, even prior to the pandemic. These individuals may not experience the effects of social distancing to the same degree as those who normally spend more time outside of their homes. Although the pandemic may be a source of anxiety and stress (Conway et al., 2020; Guo et al., 2020; Liu et al., 2020), the present results suggest that individuals may have adapted to their current circumstances. Time 2 data collection took place in late May, about 2 months after the pandemic began, which may have allowed for a “new normal,” or a time where individuals have successfully navigated COVID-19 stressors. If these same individuals were assessed at the beginning of the pandemic or at a later time point during an increase in COVID-19 cases, we may have noticed a decrease in mood. Indeed, a recent longitudinal analysis, wherein all assessments were taken after the pandemic had begun, showed that although depression increased, anxiety remained stable (González-Sanguino et al., 2020).
Consistent with recent research related to age and COVID-19 (Terry et al., 2020; Wilson et al., 2021), older age was associated with better mood, suggesting that older individuals may have greater abilities to handle the psychological effects of the pandemic. Finally, research indicates that non-White individuals and those who have a lower socioeconomic status are disproportionately affected by the pandemic (Czeisler et al., 2020). The present study included mostly White and educated individuals, which may have biased the sample toward those who may have been less impacted by the pandemic.
We hypothesized that pain-related disability and PTSD symptoms would worsen during the pandemic. However, pain-related disability improved among those in the chronic pain only group, and PTSD symptoms improved among those in the PTSD only group and comorbid group. Several potential explanations are applicable. Regarding chronic pain patients, societal restrictions meant to keep people safe (e.g., stay at home orders and social distancing) may be restricting the range of possible activity levels. In turn, this may prevent participants from experiencing their degree of disability. Social events, walking, traveling, and work have qualitatively changed during the pandemic, allowing individuals to alter their surroundings in a way they may find more suitable and more conducive to their personal desires, as opposed to societal desires (e.g., not needing to physically visit friends and using video conferencing to engage socially). For individuals with chronic pain or PTSD, leaving the comforts of one’s home brings about natural stressors, which may exacerbate chronic pain or PTSD symptoms. For individuals with PTSD, attention directed toward the pandemic may serve as a potent distraction from trauma reminders, providing temporary relief of PTSD symptoms via avoidance.
Avoidance of trauma stimuli is a defining component of PTSD (American Psychiatric Association, 2013). Some patients may not be significantly impacted by limited social engagement because they already avoided social settings prior to social distancing guidelines (Banducci and Weiss, 2020). Therefore, societal restrictions may not have added an additional stressor for individuals to manage. Indeed, individuals with PTSD may experience temporary symptom relief through these societal restrictions, because they facilitate avoidance of feared situations or trauma reminders. Overall symptom improvement in the present study is not inconsistent with recent anecdotal evidence noting initial patient improvement after the pandemic began (Venkateswaran and Hauser, 2020). Results are also consistent with González-Sanguino et al. (2020), showing PTSD symptoms decreasing over time during the pandemic.
Our hypotheses were partially predicated on concerns related to treatment disruption due to the pandemic. However, healthcare provided via telephone and/or videoconferencing is a valid and effective way to manage chronic pain and PTSD (Eccleston et al., 2020; Moring et al., 2020). Treatment for patients in our sample may not have been significantly affected by the COVID-19 pandemic. Indeed, many individuals in the present study reported little to no interference with chronic pain and/or PTSD treatment.
Importantly, pain-related disability did not improve to the same degree in the comorbid condition compared to the chronic pain only condition, although this relationship was marginal. Allostatic load may have played a role, wherein any actual or perceived improvements may have been dampened by the physical and psychological stress of managing both chronic pain and PTSD. These results are consistent with the current study’s descriptive statistics regarding COVID-19 pandemic interruptions. Individuals in the comorbid group endorsed more issues related to managing their chronic pain symptoms compared to the chronic pain group. In addition, we found overall differences in mood between the chronic pain and comorbid groups, but not between the PTSD and comorbid groups. This is consistent with recent research showing how depression symptoms are higher among individuals with comorbid chronic pain and PTSD, compared to those with chronic pain only (Day et al., 2021). Among individuals with comorbid chronic pain and PTSD, depressive symptoms may play a mechanistic role in preventing individuals from reaching their full functional potential (e.g. improvements in mobility).
Clinical implications
From a clinical perspective, it is imperative to note that the current study’s pain-related disability and PTSD symptom improvements may not indicate recovery from an underlying disorder. Indeed, results may show that the significant changes in daily life due to the pandemic are masking pain-related disability and PTSD symptoms. Understanding patients’ chronic pain and PTSD levels pre-pandemic may be an important component of the decision-making process as clinicians navigate decisions around triage of new patients and treatment continuation (or discontinuation). For incoming patients, the symptom patterns may be less severe when compared to pre-pandemic levels. Therefore, symptom monitoring becomes even more important. As societal restrictions are relaxed and “normalcy” returns, pain and PTSD symptoms may also return. Stressors related to the pandemic may be replaced with everyday stressors that have long been associated with pain and PTSD in a patient’s mind (e.g. trauma reminders when going to a restaurant). These associations may re-emerge and appear stronger than ever. Patients may need to re-learn coping strategies to handle these re-emerging stressors, and new coping strategies may be indicated. With the emergence of telehealth as a viable option for treatment (Eccleston et al., 2020; Moring et al., 2020), providers have the ability to remotely guide patients through this process and continue to monitor these symptoms.
Limitations and future directions
Because our sample was mostly White and endorsed significant levels of education, their experience of the pandemic may be very different from the experiences of marginalized people of color, non-citizens, and/or people in low socio-economic households, where they are more likely to experience negative impacts of the pandemic (Czeisler et al., 2020). More research is needed to better understand these populations. Many participants noted that the pandemic had not affected their physical therapy appointments, psychological appointments, or their ability to obtain pain or PTSD medications, which may be indicative of sampling bias resulting from the online recruitment methods of the study. Moreover, many participants indicated they did not engage in physical or psychological therapy. Only two time points were assessed. Therefore, improvements in pain-related disability and PTSD symptoms may be due to regression to the mean. Future studies should use semi-structured interviews to assess for both pain-related disability and PTSD. Null results in changes in mood over time may be due to the small sample sizes in each group. We did not include information relevant to changes in employment due to COVID-19, or baseline information on physical or mental health comorbidities, duration of pain or PTSD symptoms, psychological treatment for pain and/or PTSD, or type of trauma. Future studies should determine how these factors may play a role in symptom change. Moreover, future studies should examine pre-pandemic activity levels as predictors of symptom and mood change. After screening, only 28.79% of respondents participated in Time 1, which may have biased the sample. Finally, we retained 65.09% our sample between time points. Although missing data analysis showed that mood, pain-related disability, and PTSD symptoms were not predictive of missingness, it is possible that attrition biased the results.
Conclusion
The present quasi-experimental study examined four groups (control, chronic pain only, PTSD only, and comorbid chronic pain and PTSD) across two time points: prior to and during the COVID-19 pandemic. Mood remained stable across time, although there were marginal increases in mood in the PTSD group. Pain-related disability and PTSD symptoms improved over time for individuals endorsing those disorders. Results also showed that improvements in pain-related disability were marginally attenuated for those with comorbid chronic pain and PTSD symptoms, compared to those with chronic pain only. Improvements may be the result of circumstances unique to the pandemic, as opposed to improvements in the underlying disorder. The present results provided evidence that for some individuals, the COVID-19 pandemic may not have detrimentally affected mood, pain-related disability, or PTSD symptoms, but cautious interpretation is warranted due to only two time points and the lack of a diverse sample.
Research Data
sj-csv-1-hpq-10.1177_13591053211051821 – for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic
sj-csv-1-hpq-10.1177_13591053211051821 for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic by David E Reed, Briana Cobos, Elizabeth A Lehinger, Paul S Nabity, Kenneth E Vail and Donald D McGeary in Journal of Health Psychology
Research Data
sj-docx-5-hpq-10.1177_13591053211051821 – for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic
sj-docx-5-hpq-10.1177_13591053211051821 for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic by David E Reed, Briana Cobos, Elizabeth A Lehinger, Paul S Nabity, Kenneth E Vail and Donald D McGeary in Journal of Health Psychology
Research Data
sj-pdf-4-hpq-10.1177_13591053211051821 – for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic
sj-pdf-4-hpq-10.1177_13591053211051821 for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic by David E Reed, Briana Cobos, Elizabeth A Lehinger, Paul S Nabity, Kenneth E Vail and Donald D McGeary in Journal of Health Psychology
Research Data
sj-pdf-6-hpq-10.1177_13591053211051821 – for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic
sj-pdf-6-hpq-10.1177_13591053211051821 for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic by David E Reed, Briana Cobos, Elizabeth A Lehinger, Paul S Nabity, Kenneth E Vail and Donald D McGeary in Journal of Health Psychology
Research Data
sj-pdf-7-hpq-10.1177_13591053211051821 – for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic
sj-pdf-7-hpq-10.1177_13591053211051821 for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic by David E Reed, Briana Cobos, Elizabeth A Lehinger, Paul S Nabity, Kenneth E Vail and Donald D McGeary in Journal of Health Psychology
Research Data
sj-pdf-8-hpq-10.1177_13591053211051821 – for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic
sj-pdf-8-hpq-10.1177_13591053211051821 for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic by David E Reed, Briana Cobos, Elizabeth A Lehinger, Paul S Nabity, Kenneth E Vail and Donald D McGeary in Journal of Health Psychology
Research Data
sj-pdf-9-hpq-10.1177_13591053211051821 – for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic
sj-pdf-9-hpq-10.1177_13591053211051821 for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic by David E Reed, Briana Cobos, Elizabeth A Lehinger, Paul S Nabity, Kenneth E Vail and Donald D McGeary in Journal of Health Psychology
Research Data
sj-txt-3-hpq-10.1177_13591053211051821 – for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic
sj-txt-3-hpq-10.1177_13591053211051821 for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic by David E Reed, Briana Cobos, Elizabeth A Lehinger, Paul S Nabity, Kenneth E Vail and Donald D McGeary in Journal of Health Psychology
Research Data
sj-xlsx-2-hpq-10.1177_13591053211051821 – for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic
sj-xlsx-2-hpq-10.1177_13591053211051821 for Pain-related disability, PTSD symptoms, and mood among a comorbid chronic pain and PTSD sample prior to and during the COVID-19 pandemic by David E Reed, Briana Cobos, Elizabeth A Lehinger, Paul S Nabity, Kenneth E Vail and Donald D McGeary in Journal of Health Psychology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data sharing statement
We provided the dataset used in analyses and an R Markdown file that that contains syntax and output for variables used in reported data analyses, in addition to variables used in robustness analyses. It also contains coding keys designed to guide reviewers as to what each variable represents. We attached the dataset, but it can also be found here: ![]() .
.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.