
Abstract
This study identifies mediators and moderators of changes in physical activity (PA) following a school-based pilot intervention. Students from two Lebanese schools were randomly allocated into intervention (n = 191) and control (n = 183) groups. The multiple-mediation analysis revealed that active self-identity and perceived barriers mediated the intervention’s effect on PA changes. Baseline intention, attitude, PBC, and age moderated PA changes at post-intervention. The youngest participants and those reporting the lowest PA scores at baseline benefited most from the intervention. Future interventions with students should target these mediators and moderators to promote positive change in PA behavior.
Keywords
Regular physical activity (PA) is a cornerstone modifiable factor in reducing the risk of childhood obesity and associated diseases (Booth et al., 2012). Nonetheless, a marked decrease in PA level is reported in children during the transition from childhood into adolescence (Bacil et al., 2015). According to a recent pooled analysis, only 21.8% of schoolchildren in Western countries (Guthold et al., 2020) and 17.9% of Lebanese schoolchildren are sufficiently active (Guthold et al., 2020). These figures highlight the necessity to devote more attention to factors explaining why some children are active while others remain sedentary.
Schools have been identified as key environment in which PA information and promotion efforts can be delivered to a large number of children (Metcalf et al., 2012). Nonetheless, a poor understanding of which mechanisms work best for whom has hindered the development of effective school-based interventions for this population (Bauman et al., 2002; Brown et al., 2013; Lubans et al., 2008; Sheeran et al., 2017; van Stralen et al., 2011). According to previous researchers, it is imperative that a full understanding be gained of the factors that influence the strength of change in PA behavior (moderators) and the mechanisms by which such change occurs (mediators) (Brown et al., 2013; Lubans et al., 2008; Sheeran et al., 2017) by using a theory of change behavior, such as the theory of planned behavior (TPB). Exploring mediators, or the variables that affect the causal relationship with PA practices, can help to determine the causal pathway of the intervention effect (which changes to variables are targeted by the intervention; e.g. the participants’ intention to engage in PA) that influenced outcome variables (Brown et al., 2013; Sheeran et al., 2017). Examining moderators, or the variables (e.g. age, attitude) that affect the direction of the relationships between the independent variables (intervention) and the outcome variables (PA changes), can help to identify who will most likely benefit from programs. In turn, this can inform intervention design (Lewis et al., 2002; Sheeran et al., 2017).
The TPB is one of the most prominent theories in examining the determinants of PA behavior. A previous meta-analysis (Steinmetz et al., 2016) reported that the TPB appears to perform well in explaining the variance of 35.5% in PA behavior. The TPB posits that individuals’ behavior is directly influenced by their intention (motivation), which is determined by three main factors and their associated beliefs: the individual’s attitude (behavioral beliefs: positive or negative feeling about performing PA), the subjective norm and the subjective norm (normative beliefs: perceived pressure from important referent individuals or groups to perform PA), and the perceived behavioral control, or PBC (control beliefs: the degree to which an individual perceives him- or herself as having the skills, resources, and opportunities to perform PA). PBC can also directly affect behavior when actual control declines (Ajzen, 1991). The beliefs listed above can be influenced by the external variables such as age, gender, and other factors.
Numerous reviews have revealed that of these variables, the evidence for PBC is strongest when it comes to mediating PA changes in youth (Baranowski and Jago, 2005; Brown et al., 2013; Demetriou and Höner, 2012; Lewis et al., 2002; Lubans et al., 2008), with mixed or limited evidence for the other TPB variables, such as the intention to be physically active, subjective norms, perceived social support for PA, and attitude toward PA (Brown et al., 2013; Demetriou and Höner, 2012; Kelly et al., 2017; Lewis et al., 2002; Lubans et al., 2008).
Findings are not entirely consistent regarding the moderators of PA changes. Baseline characteristics such as demographics (e.g. sex, age, mother’s and father’s education level) (Barbosa Filho et al., 2017; Bergh et al., 2012; Cook et al., 2014), psychosocial factors (e.g. intention, attitude, PBC) (Cook et al., 2014), and obesity-related variables (e.g. BMI status, waist circumference and screen time) (Bergh et al., 2012) have been found to be moderators of PA change behavior in youth. A previous meta-analysis supported the addition of “active self-identity” (meaning the person identifies him- or herself with the PA behavior as part of his or her personality) (Tajfel, 1981) in that it may increase the TPB’s utility with regard to PA changes in youth, specifically during the transition into early adolescence (Rhodes et al., 2016). Furthermore, the authors of this meta-analysis recommended extending the TPB with the notion of active self-identity in regard to youth (Rhodes et al., 2016).
It is important to note that these mediators and moderators were identified by studies with a diverse range of youth samples (preschool children, young children, preteen children, and tweens) and results did not make a distinction between the interventions with preschool children, young children and tweens versus preteen children in transition to puberty, around the age of 11. The mechanisms by which PA behavior change occurs may differ across these samples, potentially explaining some of the inconsistent findings (Brown et al., 2013; Lewis et al., 2002; Lubans et al., 2008). A one-size-fits-all intervention strategy may not cover the diverse needs of various subgroups (van Sluijs et al., 2007). Therefore, interventions tailored to specific groups have been suggested (van Sluijs et al., 2007). Thus, we must ask whether the mechanisms of intervention affecting PA changes during the period of transition to puberty themselves change through this complex and dynamic time period in which PA levels begin to decline in Lebanon (World Health Organization, 2014) and in most industrial countries (Bacil et al., 2015). Very few studies targeting children in this transition period have tested mediating and moderating mechanisms using a formal statistical test as recommended (Baron and Kenny, 1986; Hayes, 2017) and with sufficient resources to determine the a sample size (Bergh et al., 2012; Robbins et al., 2019; Salmon et al., 2008). This information is considered essential for providing convincing evidence of the causal chain between intervention, theory, and behavior change. Previous reviews on the mediation of PA changes (Brown et al., 2013; Demetriou and Höner, 2012; Lewis et al., 2002; Yildirim et al., 2011) have concluded that there is still a scarcity of knowledge concerning which interventions work for whom and under what circumstances among children, specifically during the transition to puberty. Furthermore, reviews have highlighted that existing results come from Europe and the United States (Baranowski and Jago, 2005; Brown et al., 2013; Demetriou and Höner, 2012; Kremers et al., 2007; Lewis et al., 2002; Lubans et al., 2008), while there is an absence of robust proven or promising interventions from Lebanon or Arabic countries. To the best of the authors’ knowledge, the question of whether factors moderate and mediate the effect of theory-based PA interventions among Arabic schoolchildren has not been studied.
The IMove30+ program, a theory-based PA promotion pilot program in Lebanese schools, is the lone effective school-based program designed to determine the effects of 14 weeks of moderate-to-vigorous PA among children, and for which results have been published (Santina et al., 2021). It was previously reported that, relative to controls, children assigned to the intervention experienced significant decreases in their BMI status and waist circumference, as well as increases in their total moderate-to-vigorous PA levels (Santina et al., 2021). Therefore, the present study is a secondary analysis of the IMove30+ program data using the analytic techniques described by Hayes (2017) to examine the potential mediators and moderators, using an extended TPB, associated with the change in PA that occurred among 10–12-year-olds.
Based on the TPB, the following hypotheses were tested:
The change in psychosocial variables (active self-identity, intention, attitude, subjective norms, PBC, behavioral beliefs, normative beliefs, perceived barriers, and facilitating factors) between pre- and post-measurements mediates the change in PA at post-intervention.
The baseline value of these psychosocial variables moderates the PA changes.
The baseline obesity-related variables (BMI status, waist circumference, screen time) moderate the PA changes.
The baseline demographic variables (sex, age, grade, parent education level) moderate the PA changes.
Variables tested as mediators and moderators were derived from the original conceptual model (Supplemental File 1) that guided the design of the IMove30+ program, which was based on the literature and previous work in this community (Santina et al., 2017).
Methods
Study design and sample
A quasi-experimental design for reducing the prevalence of children’s adiposity and increasing their PA level is described elsewhere (Santina et al., 2021). In short, two private schools in southern Lebanon—selected from the 11 regional schools based on similarities in the number of students, educational level offered, school fees and urban school environment—were randomly assigned to the intervention (one school receiving the IMove30+ program and the standard school curriculum) or to the control group (one school receiving the standard school curriculum only). All the sixth- and seventh-graders in both schools (n = 392) were invited to participate (Supplemental File 2). The outcomes were measured twice in both groups: prior to, and at the end of the IMove30+ program (after 14 weeks), during the 2015–16 academic year.
A priori power analysis was informed by the Fritz and Mackinnon (2007) bias-corrected bootstrap program for mediation analysis: a sample size of 99 participants in each group was assumed with a significance level of 0.05 (power of 80, two-tailed t-test) to detect a medium effect size (Cohen’s d = 0.39) for both a and b pathways with a 2.8% loss rate. This estimate of a 2.8% dropout rate was based on previous similar trials (Habib-Mourad et al., 2014) and on the expected results of close collaboration with school teachers and principals. Since including interaction terms in a regression may reduce the power, specifically regarding moderator effect, the sample size was increased and the p-values (as indicators of significance) of the interaction terms were set at 0.05 (Yildirim et al., 2011). The final sample consisted of 374 children (191 in the intervention and 183 in the control) who filled out pre- and post-intervention measurements and were included in the analyses (response rate = 95.4%). The children’s participation was authorized by a parent or guardian signing an informed consent form, and the children gave their own signed assent. This study was approved by the university’s Institutional Review Board (number 2014–274, Phase IV) and registered in the International Standard Randomized Controlled Trial Number Registry (registration number ISRCTN19405802).
Intervention description
The IMove30+ program was a pilot multi-component PA intervention primarily aiming to promote 30 minutes of school-based moderate-to-vigorous PA per day in order to reduce obesity among 10–12-year-old children (Santina et al., 2021). The intervention mapping protocol (Bartholomew et al., 2016) and the TPB (Ajzen, 1991) were applied in order to design the intervention in a logical, step-wise fashion to ensure that the final materials and activities had clearly specified objectives grounded in empirical evidence and theory (Santina et al., 2020). The intervention development protocol and design of the IMove30+ program can be found elsewhere (Santina et al., 2020), and are briefly described below. The development of the intervention components was based on the TPB (Ajzen, 1991) integrated with extensive formative research, including focus groups (Santina et al., 2017) with local leaders in school health, school staff, and children age 10– 12 years old (Santina et al., 2020). These focus groups aimed to identify population-specific beliefs relevant to physical activity, including active self-identity, intentions, attitudes, subjective norms, and PBC (Santina et al., 2017). Additionally, a pilot survey was used to determine the factors influencing school-based PA and general PA for 10–12-year-olds (Santina et al., 2017). The IMove30+ program is a multicomponent intervention, including:
Calendars offering regular breaks for PA, relaxation and posture exercises during regular lessons;
Parent information services including information and sport activities for parents;
Changes to the school’s structural environment, an updated procedure for using sports equipment, and redesigned physical classroom and playground infrastructure;
A pupil follow-up system and a PA monitoring system;
PA events at school, a monthly social PA event in or outside of the school (e.g. biking), school sport activities, daily structured PA in the classroom and easily accessible unstructured PA during recess; and
Educational activities using personal workbooks for children and their parents with assignments to perform in class and at home and an instruction book for the school staff.
The duration of the intervention was 14 consecutive weeks (one semester), and the program was designed to be repeated as desired. The components were designed to address the factors (active self-identity, intention, PBC, perceived barriers, and gender) influencing 10–12-year-old children to engage in moderate-to-vigorous PA (Santina et al., 2021). Protocol details for the IMove30+ program is provided in Supplemental File 3. The applied strategies included interactive exercises, contests with prizes, rewards, coping plans, brainstorming, games, role-playing, role-model stories, discussions, keeping a daily record of school PA (intensity, frequency, and duration), videos, and take-home assignments. The program was implemented by trained teachers and school nurses using standardized manuals. It was delivered during the school day in addition to the regular school curriculum (which featured one 50-minute session of physical education per week). The control school was asked to maintain its regular curriculum (e.g. only one 50-minute physical education class per week). Fidelity to program delivery was ensured through intervention manuals, training and direct observation by a research team member.
Measures
An Arabic-language self-reported questionnaire including three sections was completed by children within a 20-minute timeframe in the presence of their class teacher and a research team member in a quiet classroom setting. First, the Physical Activity Questionnaire for Older Children (PAQ-C) was used to measure children’s general moderate-to-vigorous PA levels (Kowalski et al., 2004). It contains nine items measured on a 5-point scale measuring general PA levels over 7 days, including sports, games, PA during recess, and leisure activities. Girls and boys with minimum mean scores of 2.96 and 3.44, respectively, are considered physically active (Kowalski et al., 2004). The Arabic version of the PAQ-C demonstrated adequate psychometric properties for the study population (Cronbach’s alpha [α] = 0.89, intraclass correlation coefficient = 0.74) (Santina et al., 2017). Second, the psychosocial variables included active self-identity (Tajfel, 1981) and the eight psychosocial variables of the TPB (intention, attitude, subjective norm, PBC, behavioral beliefs, normative beliefs, perceived barriers, and facilitating factors). Its measures use a 4-point Likert scale ranging from 1 for “not at all” to 4 for “yes, for sure.” More detailed information on the construction and content of the psychosocial questionnaire is provided in Supplemental File 4. Third, the variable addressing screen time during leisure time was measured with four items (α = 0.79, intraclass correlation coefficient = 0.75) by asking participants about the time they spent watching TV and playing computer or video games over the last 24 hours as follows: “Yesterday, did you watch TV?” The psychometric properties for all the above variables were measured among the study population in the initial development phase of the current program (Santina et al., 2017). Following the questionnaire’s completion, anthropometric measures (weight and height for BMI calculation, waist circumference) were collected by registered nutritionists using standardized protocols (Cornier et al., 2011) in the presence of school nurses.
Weight was measured to the nearest 0.1 kg using a digital scale (Seca 803, Germany), height was measured to the nearest 0.1 cm using a stadiometer (Seca 213), and waist circumference was measured with a measuring tape to the nearest 0.5 cm (Seca 201). The children were categorized as normal/underweight, overweight, or obese based on the BMI (kg/m2) classification of the World Health Organization (de Onis et al., 2007). Since the BMI has limitations in detecting fat distribution and differentiating between fat and muscle deposition, particularly in growing subjects such as children, it was completed with the measure of waist circumference as recommended by the Centers for Disease Control and Prevention (2011) guidelines. Information on each child’s age, sex, grade level, and highest parent educational level were provided by the school administrations.
Statistical analyses
Descriptive analyses
Descriptive statistics (mean, standard deviations (SD), and proportions) were computed to present baseline characteristics in each group. Chi-square and students’ t-tests were performed to verify group equivalence at baseline.
Changes in PA and intervention effects analyses
The change in PA was computed as the between-group mean difference for change in PAQ-C scores from baseline to post-intervention, using the generalized estimating equation. The change in PA was entered as the dependent variable, and the effects of the group, time and group-by-time interactions were entered as independent variables. To aid interpretation of the change in PA, the PAQ-C scores were dichotomized according to guidelines (Kowalski et al., 2004) into physically active children (girls and boys with PAQ-C scores of ⩾2.96 and ⩾3.44, respectively) or non-active children (boys, <3.44; girls, <2.96). The Cohen’s d was calculated to determine the magnitude of effect for changes in PA using guidelines for practice-based research syntheses and interpreted using Cohen’s guidelines that d = 0.20 is a small effect size, d = 0.50 is medium, and d = 0.80 is large (Cohen, 1998).
Mediation model analysis
To test Hypothesis 1, Hayes (2017) procedures for simple and multiple mediation models were used. Simple mediation model analysis means that the indirect effect of the intervention (independent variable, X) on the PA changes (dependent variable, Y) is due to the change of one psychosocial variable targeted in the intervention (mediator, M), whereas the multiple mediation model analysis includes all the potential mediators (Hayes, 2017). Mediation analysis involves four steps: (1) assessing the effect of the group (intervention vs control) on the mediators (path a); (2) examining the direct effect of the proposed mediators on the PA changes (path b), and determining the direct effect of the group (not transmitted through mediators) on the PA changes’ (path c’); (3) measuring the total effect of the group on PA changes (path c = ab + c’); and (4) calculating the indirect effect of the group on changes in the PA levels through the proposed mediators (path ab = c−c’) by bootstrapping the sampling (1000 resamples), with 95% bias-corrected bootstrap confidence intervals (CIs) (Hayes, 2017). All models were controlled for the covariates (baseline PAQ-C scores and psychosocial variables). The investigated mediators included the post-intervention change on psychosocial variables (active self-identity, intention, attitude, subjective norms, PBC, behavioral beliefs, normative beliefs, perceived barriers, and facilitating factors). For a variable to satisfy the criteria for mediation, the 95% bias-corrected bootstrap CI for the product of coefficients (path ab) must not contain zero (Hayes, 2017).
Moderators’ analysis
To test Hypotheses 2, 3, and 4, Hayes (2017) analysis was used to assess the effect of moderator variables on PA changes. Variables associated with PA changes in previous studies—such as sex, age, grade, mother’s and father’s education level, weight classification, screen time, (Bergh et al., 2012) and psychosocial variables (Cook et al., 2014)—were tested. For each variable, a three-step procedure was performed. First, the groups (intervention and control) were regressed on the PAQ-C score at post-intervention. Second, the moderators (e.g. sex) were added. Third, the interaction term (group × moderators) was entered. A moderator effect was detected if the explained variance (R2) from steps 2 to 3 was increased (p < 0.01). If a moderator effect was detected, a simple slope for each level of the moderators was generated (at mean −1 SD, mean, and mean +1 SD).
In the mediating and moderating analyses, the term “change” on the behavioral or psychosocial variables was used to refer to the post-intervention variables controlled for the baseline values of the change variable (including variables that differed at baseline between intervention and control groups) in the regression models and not to a change the score per se. Thus, the individual differences in functioning at the previous time point did not confound the results. All data analyses were performed using SAS software (version 9.2; SAS Institute, Cary, NC, USA).
Results
Descriptive statistics
At baseline, the mean age of the participants was 10.64 (SD = 0.57) years, 54.3% were boys, 49.5% were in grade 5, and 50.0% were overweight or obese. In both groups, the mean PA score (measured using PAQ-C) was low (2.77, SD = 0.61), indicating the participants were not sufficiently active (Supplemental File 5). The participants reported high positive mean scores on all psychosocial variables related to their engagement in ⩾30 minutes a day of school-based moderate-to-vigorous PA, ranging from 3.23 to 3.78 on a 4-point scale, except for perceived barriers (2.72, SD = 0.79). A comparison of the baseline characteristics revealed a marginal difference between the intervention and control groups concerning the children’s sexes, mother’s and father’s education levels, weight classifications, PAQ-C scores, active self-identity, normative beliefs, and perceived barriers.
Changes in PA and intervention effect
Scores on the change in PA significantly increased for all the children in the intervention group at post-intervention as compared with baseline (β = 0.991, p < 0.001). The differences between groups were statistically significant as compared with baseline (regression coefficient, β = 0.5254, p < 0.001). Contrast analyses revealed that the mean change in PA was significantly higher in the intervention group than in the control group (Table 1). Cohen’s d for the change in PA revealed a large effect size (d = 0.87). Thereafter, the scores on the change in PA were dichotomized into children who were either physically active or non-active. The children in the intervention group were more than twice as physically active than those in the control group (ratio = 2.27, p < 0.01). Two-thirds of the children (girls, 75.8%; boys, 76.1%) were physically active in the intervention group after the intervention.
Pre- and post-intervention change in PA within groups.
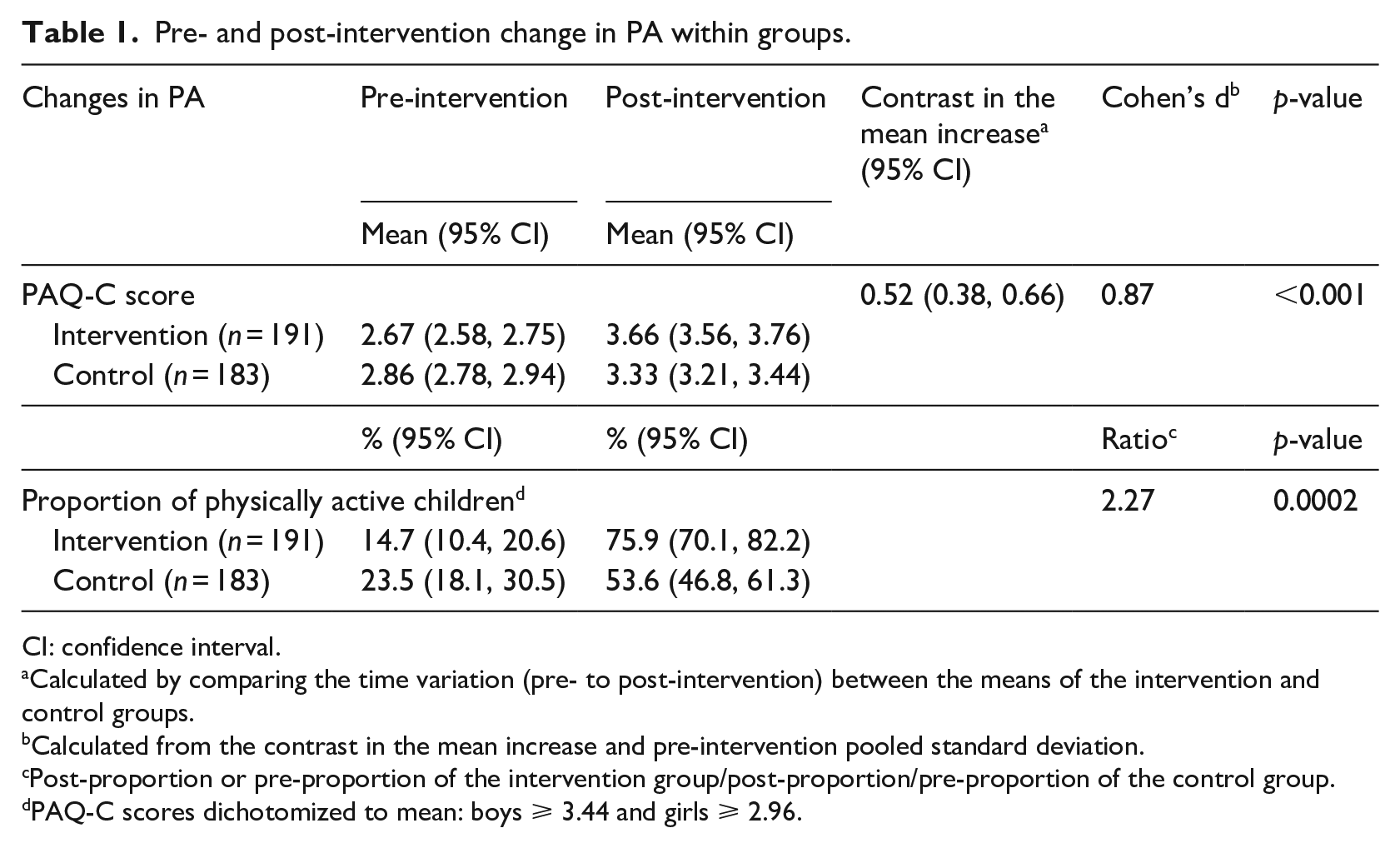
CI: confidence interval.
Calculated by comparing the time variation (pre- to post-intervention) between the means of the intervention and control groups.
Calculated from the contrast in the mean increase and pre-intervention pooled standard deviation.
Post-proportion or pre-proportion of the intervention group/post-proportion/pre-proportion of the control group.
PAQ-C scores dichotomized to mean: boys ⩾ 3.44 and girls ⩾ 2.96.
Mediators of intervention effects
In the simple-mediation analysis, bootstrapping analysis revealed an indirect effect (path ab = c−c’) for changes in intention, active self-identity, normative beliefs, perceived facilitating factors and PBC following the intervention on the change in PA (PAQ-C scores) at post-intervention. Figure 1 illustrates the effect of the group on intention, active self-identity, normative beliefs, perceived facilitating factors, and PBC (path a); the effect of these psychosocial variables on changes in PAQ-C scores at post-intervention (path b); the direct effect of the group (intervention vs control) on changes in PAQ-C scores without the influence of the mediators (path c); and the total effect of the group controlling for the mediator variables (path c’ = ab + c). The indirect effect of the group on post-intervention PA changes through moderators (e.g. intention) are estimated as path ab.
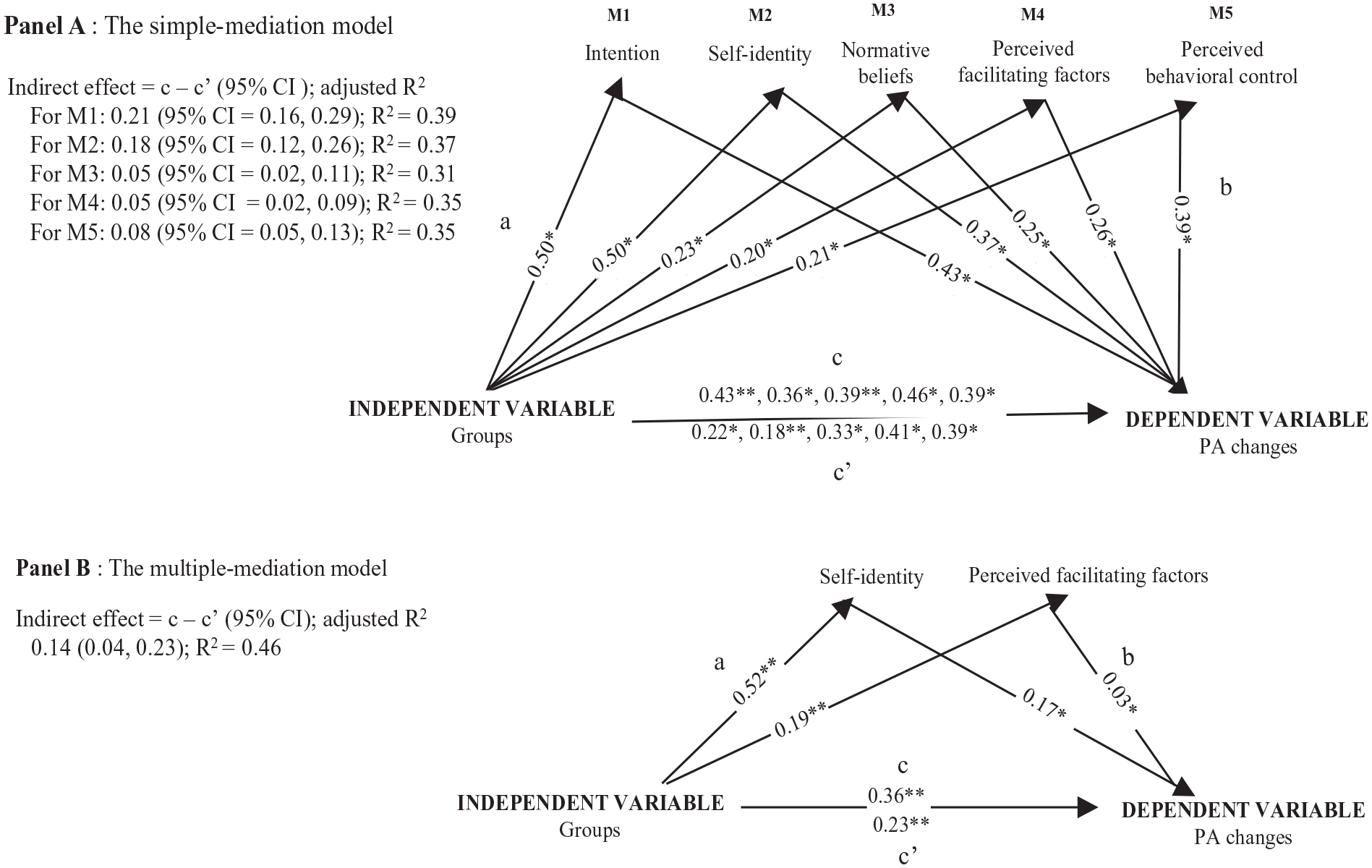
Mediators of the intervention effects on the change in PA level at post-intervention.
The results of the multiple-mediation analysis revealed that only the post-intervention changes in active self-identity and perceived barriers mediated changes in PAQ-C scores at post-intervention (path ab). It is worth mentioning that perceived barriers were close but non-significant in the simple-mediation analysis. This model explained 46% of the variance in PA changes (Figure 1).
Moderators of intervention effects
With post-intervention changes in the PAQ-C scores as the dependent variable, interaction effects were found between the group and baseline age, intention, attitude, and PBC. Subgroup analyses (Figure 2) revealed that, compared with the control group, the intervention was more effective at increasing PA levels at post-intervention among younger children (aged 10 years old) than among older children (aged 11–12 years old) (β = 0.44, 95% CI 0.17, 0.70; p < 0.001), as well as among children with high baseline intention (β = 0.31, 95% CI 0.07, 0.54; p = 0.01), attitude (β = 0.52, 95% CI 0.17, 0.87; p = 0.003) and PBC levels (β = 0.32, 95% CI 0.05, 0.58; p = 0.020). No other moderating effects were found on baseline measures relating to obesity (e.g. BMI), sociodemographic (e.g. sex) or psychosocial variables.
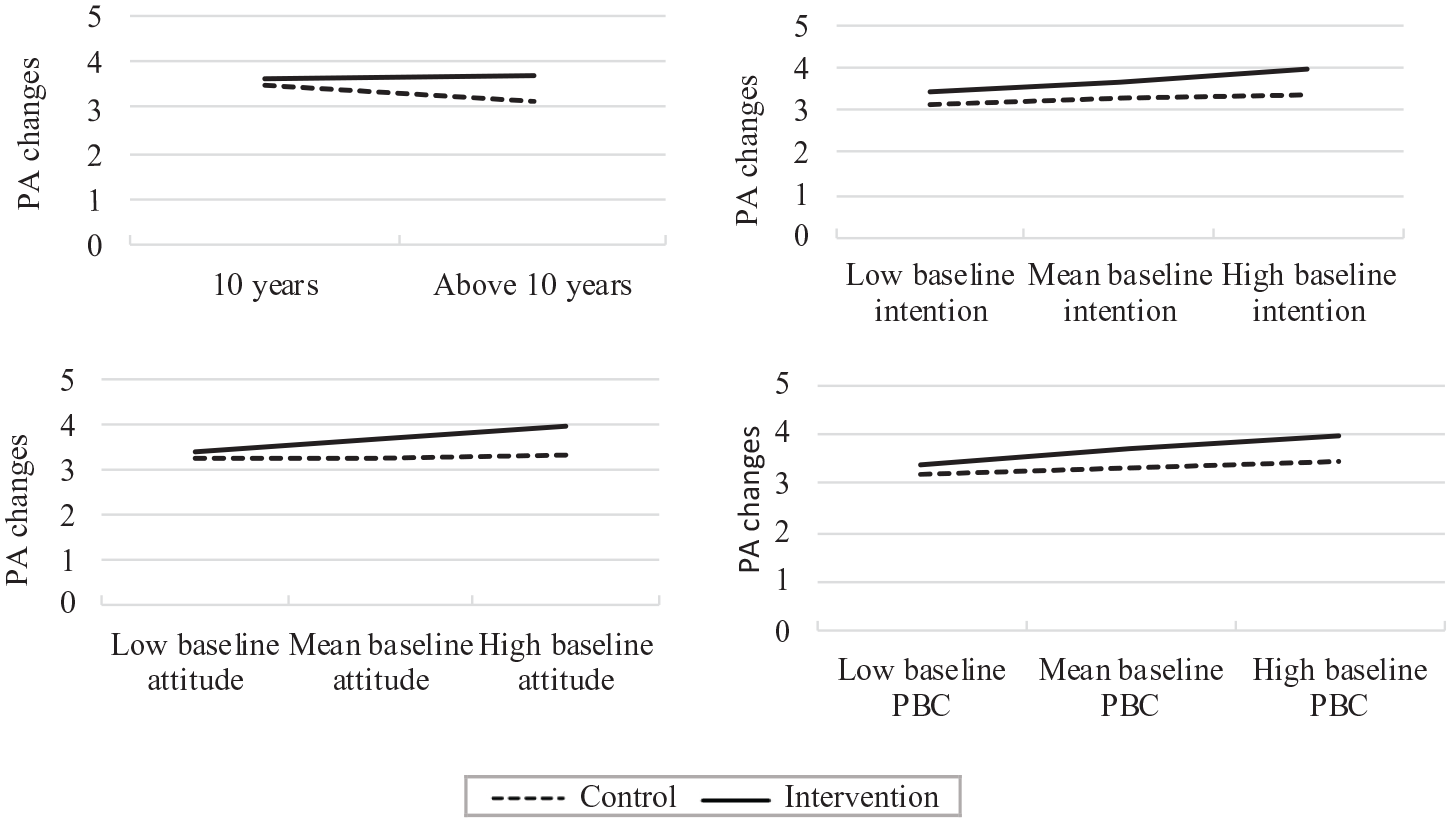
Variables moderating the change on PA (measuring using PAQ-C scores) at post-intervention by groups (N = 374: intervention = 191, control = 183).
Discussion
This present study examined the possible moderators and mediators underlying PA changes among children aged 10–12 years old following a 14-week school-based PA intervention program. Guided by the TPB, this study tested four hypotheses. As expected in the first hypothesis, changes in intention, active self-identity, PBC, normative beliefs, and perceived facilitating factors mediated the changes in PAQ-C scores at post-intervention in the simple-mediation analysis. These results indicate that the IMove30+ program targeted the important psychosocial determinants of moderate-to-vigorous PA at schools which were explored in our previous research (Santina et al., 2021), and as such the results confirm the appropriateness of the approach undertaken. However, multiple-mediation analysis revealed that changes in active self-identity and perceived barriers were the only remaining mediators of PA changes. This suggests that significant suppression effects occurred for intention, PBC, normative beliefs and perceived facilitators with regard to PA changes, after controlling for all the intervention variables at baseline (Lubans et al., 2008). These results highlight the importance for children age 10–12 years old regarding perceiving themselves as physically active and being able to overcome the barriers they encounter to increasing PA. The contribution of active self-identity supports its inclusion in prediction and intervention studies (Hagger and Chatzisarantis, 2006). This finding is in line with several studies that observed the distinctive role of active self-identity, in comparison with intention, in the childhood decision-making process (Hagger and Chatzisarantis, 2006), and its contribution in improving PA behavior prediction (Rise et al., 2010) and promoting its adoption or change (Santina et al., 2021; Strachan et al., 2015). Regarding the role of perceived barriers to PA changes, it should be noted that the scale used to measure these barriers was derived from the measure of self-efficacy recommended in Bandura’s (1986) approach, and was adapted to suit the cognitive stage of development of 10–12-year-old children (Piaget, 1948). Self-efficacy reflects the individual’s perceived ability to perform a behavior, whereas PBC refers to the person’s perceived capacity and control over performing the target behavior (Ajzen, 1991). These findings reinforce those of many previous studies on the mediating role of self-efficacy in PA interventions (Baranowski and Jago, 2005; Brown et al., 2013; Demetriou and Höner, 2012; Kelly et al., 2017; Lewis et al., 2002; Lubans et al., 2008) and emphasize its specific contribution to PBC.
The roles of active self-identity and perceived barriers as the main mediators of PA changes in a multiple-regression model among adolescents were also reported in a previous review (Kelly et al., 2017). In practical terms, these results highlight the urgent need to explore which behavior change techniques (Bartholomew et al., 2016), identified as the most effective to change these variables in particular (e.g. PBC and active self-identity), should be integrated into future interventions to enable more significant changes in these variables and to tailor PA interventions to the most relevant targets for each child (Kelly et al., 2017).
Consistent with the second hypothesis on moderation effects, the baseline psychosocial factors from the TPB (intention, attitude, and PBC) moderated PA changes at post-intervention. Similarly, a previous intervention reported that higher baseline intention moderated PA changes among adolescents (Cook et al., 2014). These results provide useful information to guide the promotion of childhood PA. Indeed, since interventions appeared to work best among children with high baseline intention, attitude, and PBC levels, intervention developers should pay particular attention in ensuring that interventions primarily support children with the lowest scores on these variables.
Regarding the third and fourth hypotheses, age was the sole moderator for which the oldest participants displayed a lower increase in PA. This result could be explained by the transition period from childhood to adolescence, with an increasing search for autonomy from parents and adults accompanied by the growing influence of friends on behaviors and beliefs (Cook et al., 2014). This also corresponds with the dramatic decline of PA during the transition to adolescence consistently reported in the existing literature on this subject (Kemp et al., 2019), making the promotion of childhood PA during this period a public health priority (Sirard and Barr-Anderson, 2008). Therefore, different efforts are needed in order to strengthen the interest of older children (Kemp et al., 2019) relating to PA engagement.
Attention should also be paid to the variables that did not display moderating effects, such as sex and baseline BMI, even if, at baseline, girls were less active than boys and 50% of children were obese or overweight. These findings can be attributed to the intervention designers of the present program striving to provide many PA options appealing to both girls and boys, regardless of their BMI status, and including changes to the school environment planned and approved by children themselves. These results also confirm the findings of earlier intervention that combined school environment changes and child-led play and reported no moderating effects of sex or baseline BMI status on PA changes in preteen children (Simon et al., 2008).
Strengths and limitations
This study has several strengths. First, to our knowledge, this is one of the few school-based PA interventions assessing theoretical underpinnings in children during the transition to puberty only and conducting mediation analyses (Bergh et al., 2012; Robbins et al., 2019) and moderation analyses (Bergh et al., 2012; Cook et al., 2014; Salmon et al., 2008). Second, this study stands out because it was conducted in an Arabic country, where no study of this nature has been published. This work, therefore, significantly contributes to culture-based contextualization of intervention developments (Bernal, 2006). Third, the preliminary identification of factors influencing school-based PA (Santina et al., 2017), the rigorous intervention development procedure (Santina et al., 2020), and the inclusion of a control group may contribute to its success in increasing PA levels (Santina et al., 2021) and offer confidence in the interpretation of its results. Finally, all hypothesized mediators were included in a multiple-mediation model instead of a simple model only. This approach facilitated the identification of the most important variables that should be targeted in school-based PA interventions, providing orientations for more effective future intervention development (Sheeran et al., 2017).
However, some limitations should be addressed. First, the study participants were from two schools (in keeping with the pilot) drawn from a limited geographic region within southern Lebanon, which may limit the generalizability of the results to other populations and could lead to inflated type I error rates. Future research within larger groups of Arabic schoolchildren could provide valuable information for designing targeted school-based PA interventions. Second, the PA measure was self-reported, which has potential limitations, such as inaccurate recall of the intensity and duration of activities (recall bias), inaccurate comprehension of questions, and social desirability bias (Sallis and Saelens, 2000). Future research should incorporate objective measures (e.g. accelerometers) to provide a more accurate assessment of PA levels (Brown et al., 2013). Third, the use of BMI measurement to identify children with excess adiposity during pubertal development, such in the current study, may overestimate adiposity in children. Therefore, an erroneous classification could occur—some participants may be considered to have excess adiposity when they do not (Rodríguez et al., 2004), which may explain the lack of moderation effect for BMI on intervention effect in this and a previous systematic review (Yildirim et al., 2011). Future research should incorporate objective measures to provide a more accurate assessment of obesity levels. The fourth limitation concerns the short-term effects of measuring 1 week after the end of the intervention, despite research indicating that PA maintenance could be a greater challenge than PA adoption (Sallis and Saelens, 2000). A post-intervention follow-up of PA at 6 months, for example, would have been optimal.
Conclusion
Multiple-mediation analysis highlighted the importance of active self-identity and perceived barriers as mediators of PA changes among children. These findings confirm the roles of these variables in promoting PA, as well as the relevance of using strategies that have the potential to influence these variables. Through moderation analysis, this study also clarified the characteristics of children who might benefit less from school-based interventions, and who should be more intensively targeted by school-based interventions seeking to improve PA levels. The absence of moderating effects on the part of sex and BMI status indicates that the IMove30+ program was effective in enhancing PA without perpetuating childhood health inequality in these variables. Overall, by improving understanding of the mediators and moderators of a PA intervention, this study helps address current gaps in the literature on studies targeting schoolchildren and provides guidance for upcoming research regarding the impact of specific intervention targets.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053211061407 – Supplemental material for Mediators and moderators of physical activity changes in a school-based intervention targeting childhood obesity
Supplemental material, sj-docx-1-hpq-10.1177_13591053211061407 for Mediators and moderators of physical activity changes in a school-based intervention targeting childhood obesity by Tania Santina, Dominique Beaulieu, Camille Gagné and Laurence Guillaumie in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053211061407 – Supplemental material for Mediators and moderators of physical activity changes in a school-based intervention targeting childhood obesity
Supplemental material, sj-docx-2-hpq-10.1177_13591053211061407 for Mediators and moderators of physical activity changes in a school-based intervention targeting childhood obesity by Tania Santina, Dominique Beaulieu, Camille Gagné and Laurence Guillaumie in Journal of Health Psychology
Supplemental Material
sj-docx-3-hpq-10.1177_13591053211061407 – Supplemental material for Mediators and moderators of physical activity changes in a school-based intervention targeting childhood obesity
Supplemental material, sj-docx-3-hpq-10.1177_13591053211061407 for Mediators and moderators of physical activity changes in a school-based intervention targeting childhood obesity by Tania Santina, Dominique Beaulieu, Camille Gagné and Laurence Guillaumie in Journal of Health Psychology
Supplemental Material
sj-pdf-1-hpq-10.1177_13591053211061407 – Supplemental material for Mediators and moderators of physical activity changes in a school-based intervention targeting childhood obesity
Supplemental material, sj-pdf-1-hpq-10.1177_13591053211061407 for Mediators and moderators of physical activity changes in a school-based intervention targeting childhood obesity by Tania Santina, Dominique Beaulieu, Camille Gagné and Laurence Guillaumie in Journal of Health Psychology
Supplemental Material
sj-pdf-2-hpq-10.1177_13591053211061407 – Supplemental material for Mediators and moderators of physical activity changes in a school-based intervention targeting childhood obesity
Supplemental material, sj-pdf-2-hpq-10.1177_13591053211061407 for Mediators and moderators of physical activity changes in a school-based intervention targeting childhood obesity by Tania Santina, Dominique Beaulieu, Camille Gagné and Laurence Guillaumie in Journal of Health Psychology
Supplemental Material
sj-pptx-1-hpq-10.1177_13591053211061407 – Supplemental material for Mediators and moderators of physical activity changes in a school-based intervention targeting childhood obesity
Supplemental material, sj-pptx-1-hpq-10.1177_13591053211061407 for Mediators and moderators of physical activity changes in a school-based intervention targeting childhood obesity by Tania Santina, Dominique Beaulieu, Camille Gagné and Laurence Guillaumie in Journal of Health Psychology
Supplemental Material
sj-pptx-2-hpq-10.1177_13591053211061407 – Supplemental material for Mediators and moderators of physical activity changes in a school-based intervention targeting childhood obesity
Supplemental material, sj-pptx-2-hpq-10.1177_13591053211061407 for Mediators and moderators of physical activity changes in a school-based intervention targeting childhood obesity by Tania Santina, Dominique Beaulieu, Camille Gagné and Laurence Guillaumie in Journal of Health Psychology
Footnotes
Author note
Camille Gagné and Laurence Guillaumie are now affiliated to Lebanese University, Lebanon.
Data sharing statement
The current article includes the complete raw dataset collected in the study including the participants’ dataset, syntax file and log files for analysis. These files are all available in the Figshare repository and as Supplemental Material via the SAGE Journals platform.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors desclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author received financial support for the research from the Faculty of Nursing, Université Laval, Canada.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.