
Abstract
Commonsense epidemiology—how lay people think about diseases and their causes and consequences—can influence how people respond. We examined three lay epidemiological beliefs about 20 triggers and 19 symptoms among 349 caregivers of children with asthma. Our findings contradicted the prevalence-seriousness hypothesis (perceived prevalence and seriousness correlate negatively). The data partially supported the prevalence-control hypothesis (perceived prevalence and asthma control correlate negatively). We found weak support for the seriousness-control hypothesis (perceived seriousness and asthma control correlate negatively). These findings suggest boundary conditions on the application of commonsense epidemiological beliefs.
Keywords
Lay people often must function as amateur epidemiologists when they gather and process information about health and disease (Jemmott et al., 1988). Commonsense epidemiology refers to how laypeople think about the symptoms, etiology, management, and prognosis of diseases (Bar-Lev and Beimel, 2020). Understanding laypeople’s subjective beliefs about illness is important because it can inform how they respond to illnesses and health threats (Meyer et al., 1985). In the current study, we examined the occurrence of three common-sense epidemiological beliefs in a sample of caregivers of children with asthma. Although all three beliefs will certainly have exceptions, they nevertheless represent how people may broadly think about diseases in general.
The prevalence-seriousness belief is that rare medical conditions are more serious than are common medical conditions. People perceive the prevalence and seriousness of a disease as covarying, rating more serious diseases as less prevalent than less serious diseases (Jemmott et al., 1988), and rating less prevalent diseases as more serious than more prevalent diseases (Jemmott et al., 1986; see also Weinstein, 1982).
The prevalence-control belief is that greater prevalence of a disease or its symptoms corresponds with less control over the disease. This belief is evident not only at a community level when considering easily transmissible diseases such as viruses, but also at an individual level when considering the presence of symptoms. That is, experiencing more symptoms or experiencing symptoms more frequently suggests that a medical condition is less controlled. In the context of asthma, this belief is consistent with the clinical guidance caregivers receive from providers: more frequent asthma symptoms or reactions to triggers means the child’s asthma is less controlled” (National Asthma Education and Prevention Program, 2020).
The seriousness-control belief is that disease seriousness and controllability covary: generally speaking, the less controlled or controllable a medical condition, the more inclined people are to perceive it as serious. Preliminary evidence comes from research showing a consistent, albeit small correlation (0.17–0.22) between perceived disease severity and perceived disease controllability (Weinstein, 1982, 1989), which likely arises from the perception that diseases are more serious if people cannot take action to avoid or treat them, or to reduce or eliminate the symptoms.
Researchers have examined other commonsense beliefs including the experience-prevalence belief—people who have a history (experience) with a condition estimate that the prevalence is higher than do people with no history with the disease (Jemmott et al., 1988). We focused specifically on the three commonsense beliefs we described because of our larger interest in how caregivers of children with asthma think about specific aspects of asthma triggers and symptoms.
Overview and hypotheses
We tested the boundaries of the layperson epidemiological beliefs by examining whether they extend to caregiver judgments of the prevalence, controllability, and seriousness of asthma triggers and asthma symptoms. We predicted that greater perceived prevalence of asthma triggers and symptoms would correspond with lower perceived seriousness (prevalence-seriousness hypothesis) and asthma control (prevalence-control hypothesis), and that greater perceived asthma control would correspond with lower perceived seriousness of asthma triggers and symptoms (seriousness-control hypothesis). We pre-registered our hypotheses and analyses prior to data collection at the Open Science Framework: https://osf.io/n9pb8/. Although we pre-registered other analyses, we report here only the analyses relevant to the current paper. We report deviations from our pre-registered plan at the OSF link: https://osf.io/pfwqr/.
Method
Participants
In December 2019, we recruited caregivers of children (ages 0–17 years) with asthma through Qualtrics panels (Qualtrics, Provo, UT), which actively manages market research panels. Prior to analysis we excluded responses from 45 participants who failed any of three data quality checks (see Supplement for additional details), resulting in 349 responses. Based on the smallest sample size (n = 143) analyzed in our correlation analyses, we had 80% power to detect a small-to-moderate effect size of r = 0.23 or R2 = 0.05 for individual triggers and symptoms. See Table 1 for demographic information and the supplement at the OSF link (https://osf.io/tsdhx/) for additional recruitment and exclusion information.
Demographic information.
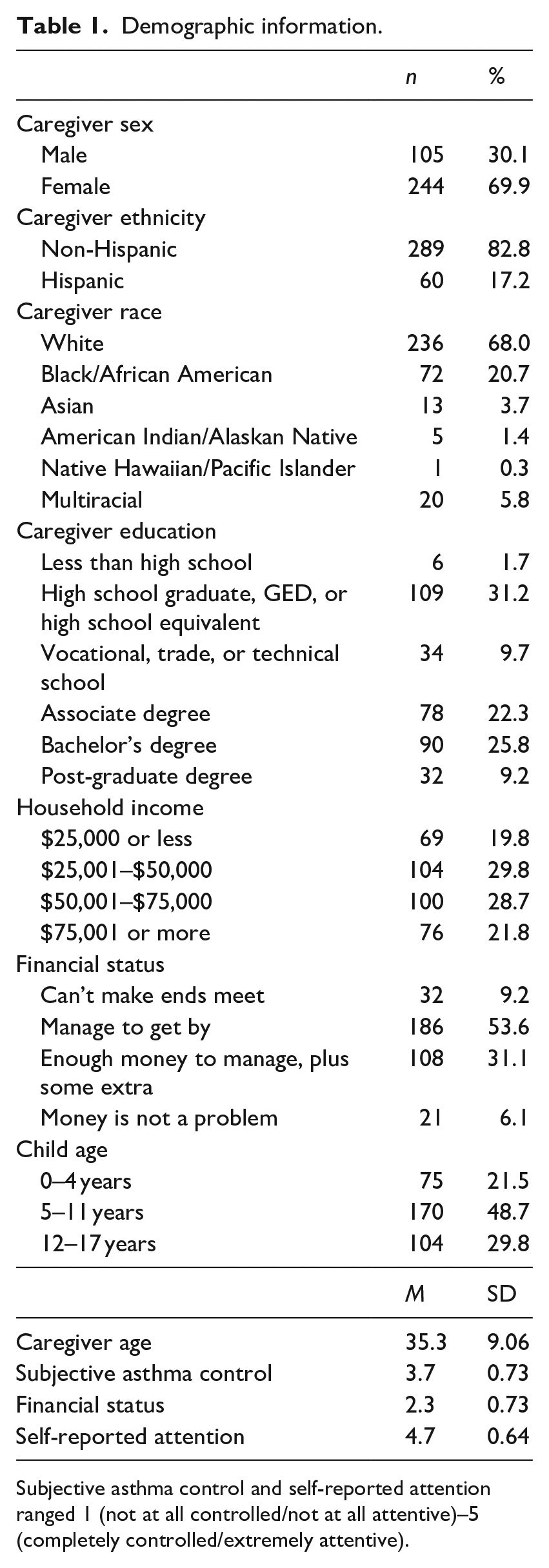
Subjective asthma control and self-reported attention ranged 1 (not at all controlled/not at all attentive)–5 (completely controlled/extremely attentive).
Procedure
To reduce participant burden, after consenting we randomly assigned participants to complete a subset of all items, either asthma triggers or asthma symptoms. We also randomly assigned participants to respond using either 4- or 5-point scales to test hypotheses unrelated to the current investigation. Participants responded to the prevalence items prior to the seriousness items. Additional information about the procedure is available in the pre-registration at the OSF link. The Institutional Review Board at the University of Florida approved all procedures and measures (IRB#201802313).
Materials
Prevalence and seriousness
Caregivers estimated the frequency with which their child encountered 20 asthma triggers that can cause breathing problems (“How often does your child have breathing problems when exposed to _____?”) or experienced 19 asthma symptoms (“How often has your child experienced the following because of asthma?”) in the last year. The response scale for both questions was 1 = never, 4/5 = all the time. Caregivers also estimated the seriousness of the 20 triggers (“How bad would it be for your child’s breathing if he or she was exposed to _____?”) or the 19 symptoms (“How bad would it be for your child’s breathing if he or she had the following symptom?”). The response scale for both questions was 1 = not at all bad, 4/5 = extremely bad. We identified the triggers and symptoms from the literature and from interviews with caregivers. We included triggers that may lack support in the biomedical model of asthma to obtain a more complete picture of caregivers’ beliefs (see Tables 2 and 3 for the list of triggers and symptoms, and the pre-registration at the OSF link for a more detailed description). We standardized responses the 4- and 5-point scales and then combined them to report a single set of analyses and retain the statistical power of the full sample.
Descriptive statistics for asthma triggers.
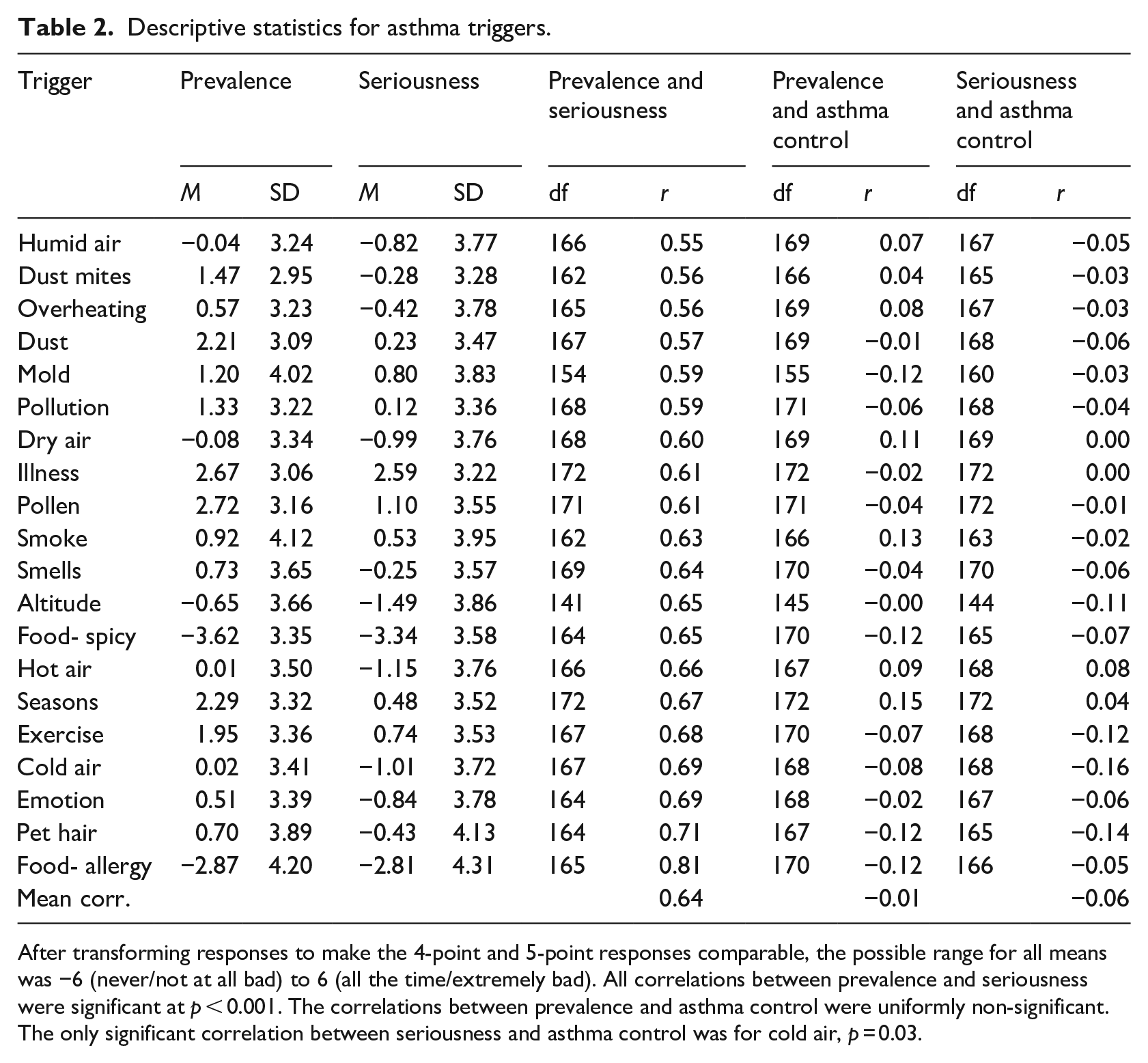
After transforming responses to make the 4-point and 5-point responses comparable, the possible range for all means was −6 (never/not at all bad) to 6 (all the time/extremely bad). All correlations between prevalence and seriousness were significant at p < 0.001. The correlations between prevalence and asthma control were uniformly non-significant. The only significant correlation between seriousness and asthma control was for cold air, p = 0.03.
Descriptive statistics for asthma symptoms.
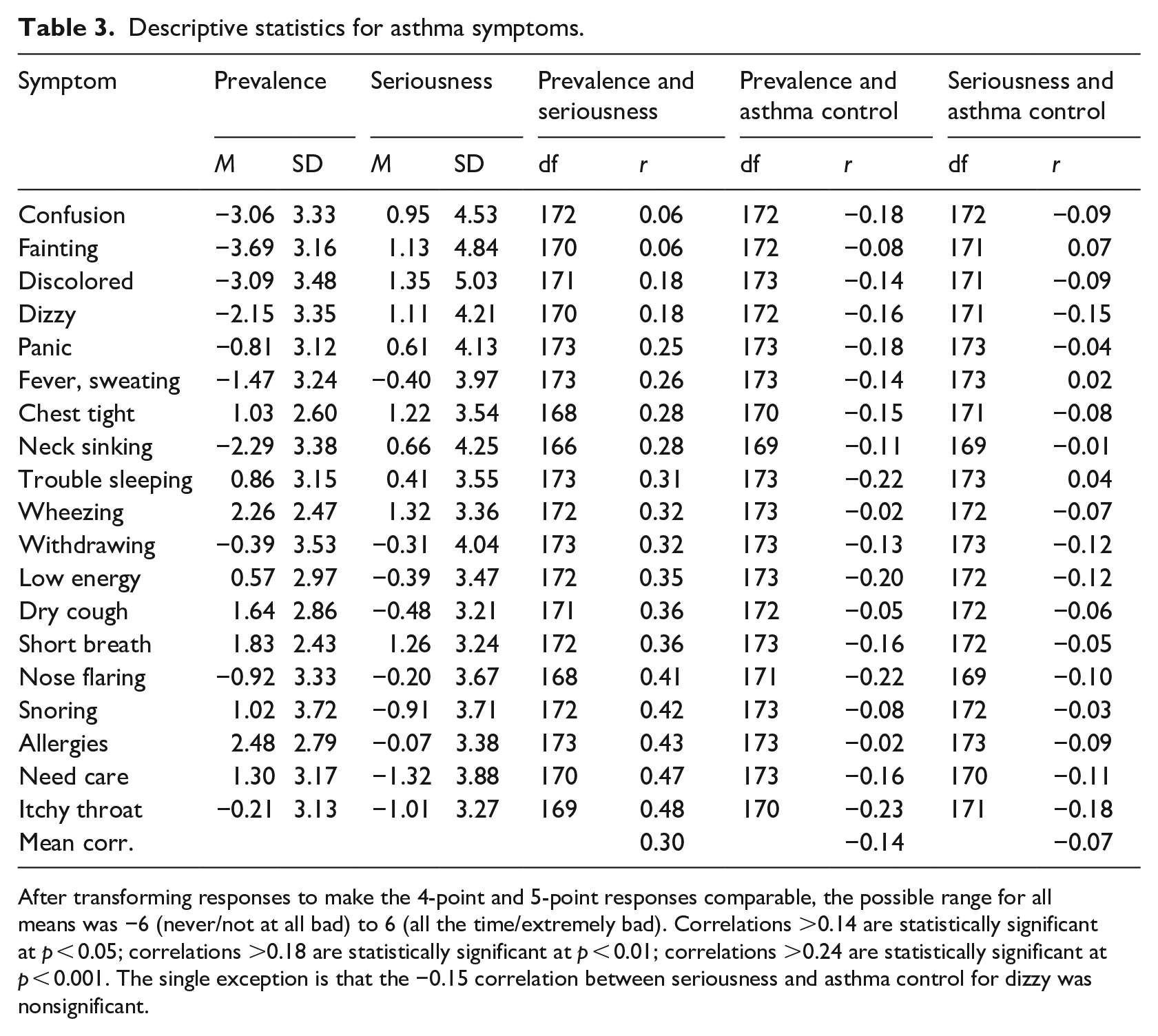
After transforming responses to make the 4-point and 5-point responses comparable, the possible range for all means was −6 (never/not at all bad) to 6 (all the time/extremely bad). Correlations >0.14 are statistically significant at p < 0.05; correlations >0.18 are statistically significant at p < 0.01; correlations >0.24 are statistically significant at p < 0.001. The single exception is that the −0.15 correlation between seriousness and asthma control for dizzy was nonsignificant.
Asthma control
We measured caregivers’ estimates of their child’s subjective asthma control in the past 2 months with a single item we derived from the Parent-Proxy Asthma Control Test (PP-ACT, DuRivage et al., 2017): “How would you rate your child’s asthma control in the past 2 months? (1 = not at all controlled, 2 = poorly controlled, 3 = somewhat controlled, 4 = well controlled, 5 = completely controlled).”
Results
To facilitate reporting the means and SDs across the 4- and 5-point scale conditions, we recoded the four-point scale responses as: 1 = −6, 2 = −2, 3 = 2, 4 = 6. We recoded the 5-point scale responses as: 1 = −6, 2 = −3, 3 = 0, 4 = 3, 5 = 6. Although the transformations introduced negative values, the scales remained unipolar.
We tested the prevalence-seriousness hypothesis by correlating the frequency and seriousness ratings for the 19 triggers before computing the average correlation among the triggers. We repeated this process for the 20 symptoms. Contrary to prediction, we observed uniformly positive correlations between prevalence and seriousness for both asthma triggers (Table 2; weighted mean correlation or rwm = 0.64, 95% CI [0.62, 0.66]) and symptoms (Table 3; rwm = 0.31 [0.28, 0.34]), with stronger correlations for the triggers than the symptoms.
We tested the prevalence-control hypothesis by computing the correlations between the ratings of trigger (and symptom) prevalence and caregivers’ subjective rating of their child’s asthma control in the past 2 months. The non-significant correlations for triggers were inconsistent with prediction (rwm = −0.01 [−0.05, 0.03]). Consistent with prediction, however, the correlations for symptoms were uniformly negative, and although they varied in magnitude, their weighted mean was significant (rwm = −0.14 [−0.17, −0.11]).
We tested the seriousness-control hypothesis by computing the correlations between the ratings of trigger (and symptom) seriousness and caregivers’ subjective rating of their child’s asthma control in the past 2 months. Consistent with prediction, weighted mean correlations were small but significantly negative for both triggers (rwm = −0.06 [−0.10, −0.02]) and symptoms (rwm = −0.07 [−0.10, −0.03]). Examining the individual correlations in Tables 2 and 3, almost none are statistically significant. However, examining the weighted mean correlations, we observe small but significant negative correlations.
Sensitivity analyses that included the 45 participants we had excluded due to data quality concerns revealed negligible change in the mean correlations for triggers and symptoms. See the Supplemental Material (https://osf.io/tsdhx/) for the results and a discussion of the exclusion decisions.
Discussion
Our findings contradicted the prevalence-seriousness hypothesis—that greater perceived prevalence of asthma triggers and symptoms would correspond with greater perceived seriousness. The most likely explanation comes from a difference in how we assessed prevalence. Whereas prior research assessed prevalence in terms of how many people have the disease, we assessed prevalence in terms of how often a trigger elicits asthma symptoms or how frequently the child experiences asthma symptoms. Caregivers appear to infer, understandably, that a trigger is serious—one that should be avoided and viewed as dangerous—if it frequently initiates breathing problems. With symptoms, greater prevalence means that the caregiver must respond to it more frequently; that it requires greater effort and attention. Much like use of the availability heuristic (Tversky and Kahneman, 1973), whereby people base judgments of likelihood on the ease with which something comes to mind, caregivers may infer that symptoms that require more effort and attention are more serious. Importantly, some asthma symptoms (dizziness and discoloration) are more serious than other symptoms (wheezing) (Children’s Hospital St. Louis, 2020), but our sample appeared not to recognize this fact.
We found partial support for the prevalence-control hypothesis, but only for asthma symptoms and not for asthma triggers. The effect for symptoms is consistent with clinical guidance that experiencing more frequent symptoms is evidence of lower asthma control (National Asthma Education and Prevention Program, 2020). The null effect we observed for triggers may reflect the complexity of asthma, where triggers and the resulting symptoms can vary across people. Moreover, it can be difficult to identify specific triggers of an asthma exacerbation. As a consequence, caregivers may not perceive a link between trigger prevalence and their child’s level of asthma control.
We found small but significant support for the seriousness-control hypothesis for both asthma triggers and symptoms. On average, caregivers viewed lower asthma control as corresponding with greater perceived seriousness of asthma triggers and symptoms. The weakness of the correlations may reflect the fact that even children with well-controlled asthma occasionally experience asthma exacerbations (i.e. infrequent but serious symptoms that may or may not be reactions to strong triggers). Caregivers may perceive only a weak link between their child’s asthma control and the seriousness of asthma triggers and symptoms.
In sum, we found mixed support for the three beliefs we examined, with the strongest supportive evidence appearing for the prevalence-control belief, but only in beliefs about symptoms and not in beliefs about triggers. We found small but significant support for the seriousness-control hypothesis and found evidence that contradicted the prevalence-seriousness hypotheses. These findings suggest that caregivers of children with asthma may hold common-sense epidemiological beliefs idiosyncratically. Of course, our findings are limited by the way we operationalized prevalence, seriousness, and asthma control, and different operations may have yielded different results. Yet that limitation speaks to our broader point: people appear to apply common-sense epidemiological beliefs judiciously.
Research Data
sj-csv-7-hpq-10.1177_13591053211064986 – for Examining commonsense epidemiology: The case of asthma
sj-csv-7-hpq-10.1177_13591053211064986 for Examining commonsense epidemiology: The case of asthma by Gabrielle Pogge, Erika A Waters, Gregory D Webster, David Fedele, Sreekala Prabhakaran and James A Shepperd in Journal of Health Psychology
Supplemental Material
sj-docx-5-hpq-10.1177_13591053211064986 – Supplemental material for Examining commonsense epidemiology: The case of asthma
Supplemental material, sj-docx-5-hpq-10.1177_13591053211064986 for Examining commonsense epidemiology: The case of asthma by Gabrielle Pogge, Erika A Waters, Gregory D Webster, David Fedele, Sreekala Prabhakaran and James A Shepperd in Journal of Health Psychology
Research Data
sj-docx-8-hpq-10.1177_13591053211064986 – for Examining commonsense epidemiology: The case of asthma
sj-docx-8-hpq-10.1177_13591053211064986 for Examining commonsense epidemiology: The case of asthma by Gabrielle Pogge, Erika A Waters, Gregory D Webster, David Fedele, Sreekala Prabhakaran and James A Shepperd in Journal of Health Psychology
Research Data
sj-R-6-hpq-10.1177_13591053211064986 – for Examining commonsense epidemiology: The case of asthma
sj-R-6-hpq-10.1177_13591053211064986 for Examining commonsense epidemiology: The case of asthma by Gabrielle Pogge, Erika A Waters, Gregory D Webster, David Fedele, Sreekala Prabhakaran and James A Shepperd in Journal of Health Psychology
Research Data
sj-rtf-1-hpq-10.1177_13591053211064986 – for Examining commonsense epidemiology: The case of asthma
sj-rtf-1-hpq-10.1177_13591053211064986 for Examining commonsense epidemiology: The case of asthma by Gabrielle Pogge, Erika A Waters, Gregory D Webster, David Fedele, Sreekala Prabhakaran and James A Shepperd in Journal of Health Psychology
Research Data
sj-xlsx-2-hpq-10.1177_13591053211064986 – for Examining commonsense epidemiology: The case of asthma
sj-xlsx-2-hpq-10.1177_13591053211064986 for Examining commonsense epidemiology: The case of asthma by Gabrielle Pogge, Erika A Waters, Gregory D Webster, David Fedele, Sreekala Prabhakaran and James A Shepperd in Journal of Health Psychology
Research Data
sj-xlsx-3-hpq-10.1177_13591053211064986 – for Examining commonsense epidemiology: The case of asthma
sj-xlsx-3-hpq-10.1177_13591053211064986 for Examining commonsense epidemiology: The case of asthma by Gabrielle Pogge, Erika A Waters, Gregory D Webster, David Fedele, Sreekala Prabhakaran and James A Shepperd in Journal of Health Psychology
Research Data
sj-xlsx-4-hpq-10.1177_13591053211064986 – for Examining commonsense epidemiology: The case of asthma
sj-xlsx-4-hpq-10.1177_13591053211064986 for Examining commonsense epidemiology: The case of asthma by Gabrielle Pogge, Erika A Waters, Gregory D Webster, David Fedele, Sreekala Prabhakaran and James A Shepperd in Journal of Health Psychology
Footnotes
Author Contributions
Gabrielle Pogge and James A. Shepperd drafted the manuscript and contributed to the conceptualization. Erika Waters contributed to the writing and to the conceptualization. Sreekala Prabakaran and David Fedele provided technical expertise on asthma. Gregory D. Webster contributed to the analysis.
Data sharing statement
All of the de-identified individual participant data collected during the study that are relevant to this paper (trigger and symptom frequency and seriousness ratings, asthma control ratings, and demographics), the codebook, protocol, informed consent, statistical analysis plan, and analysis script are available in the Figshare repository and as Supplemental Material via the SAGE Journals platform.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health [grant number R01HL137680; MPI: James A Shepperd and Erika A. Waters].
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.