
Abstract
The role that the superwoman schema (SWS) plays in U.S. Black women’s perceptions of barriers (biological, psychological, and sociological) to healthy weight management is unknown. This exploratory study examined whether 122 women classified as normal weight, overweight or obese differed in their perceptions of types of barriers and if the SWS predicted perceived barriers to weight management. Women classified as obese reported more barriers than those classified as normal weight. The SWS uniquely positively predicted perceived psychological and sociological barriers. Our findings suggest that the SWS may play a vital role in the self-management of weight in U.S. Black women.
Introduction
Over half of Black women in the United States are obese, and have exceeded all other racial and ethnic groups in the prevalence of obesity for several decades (Chu et al., 2009; Hales et al., 2018, 2020; Ogden et al., 2014, 2017; Rummo et al., 2018). This disparity confers a dramatic increase in risk for acute health complications and death including Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection (Nakeshbandi et al., 2020). Obesity has a longstanding association with chronic diseases, including hypertension, type-2 diabetes, hypercholesterolemia, thyroid disease, sleep apnea, and some cancers (Chaker et al., 2017; Guh et al., 2009; Hall et al., 2015; Kyriacou et al., 2019; Leitner et al., 2017; Lucassen and Cizza, 2012; Seravalle and Grassi, 2017; Wilson et al., 2002; Wirth et al., 2014; Yang et al., 2017). Moreover, obesity also contributes to the experience of weight-related stigma which can impact adherence to health providers’ recommendations (Palad et al., 2019; Snyder et al., 2020 ).
Identifying and addressing barriers to weight self-management has been an ongoing health initiative with important implications for Black women’s health (Agyemang and Powell-Wiley, 2013; Bowie et al., 2018). This knowledge has become even more critical in the face of the current pandemic to reduce Covid-19-related morbidity and mortality.
Barriers to Black women achieving and maintaining a healthy weight include biological (e.g. genetics, hormonal responses, etc.) (Agyemang and Powell-Wiley, 2013; Gore et al., 2003; Headen et al., 2012; Spaeth et al., 2015, psychological (e.g. motivation, underestimation of weight, psychosocial stress, etc.) (Agyemang and Powell-Wiley, 2013; Harris et al., 2016; Hendley et al., 2011; Warren et al., 2016), and sociological factors (e.g. neighborhoods characterized by dense fast-food venues and less physical activity resources, etc.) (Jilcott Pitts et al., 2013; Powell-Wiley et al., 2013). Other social determinants include lower socioeconomic status, which interacts with psychosocial stress, weight stigma, dietary preferences, pressures to conform to food habits, acceptance of larger body size, and hair care practices that limit exercise have also been linked to overweight/obesity (Anekwe et al., 2020; Befort et al., 2008; Bertoni et al., 2011; Hall et al., 2015; Robinson et al., 2012; Thomas et al., 2013; White et al., 2017). Mental illnesses and their treatment may also be a barrier to achieving a healthy weight given their association with dysregulated eating and reduced metabolism (Cortese et al., 2016; Shrivastava and Johnston, 2010; Zimmerman and Wylie-Rosett, 2003). In the current climate of the Covid-19 pandemic, it is more critical than ever to understand Black women’s perceived barriers to managing their weight, given the high prevalence of obesity in these women and recent studies highlighting a disproportionate increase in mortality from Covid-19 infection in those who are Black with obesity (Ferdinand, 2020; Townsend et al., 2020).
The role that Black women’s self-schemas play in perceptions of barriers to weight management is unknown. Self-schemas are internalized generalizations derived from socialization experiences that influence how one thinks, feels and acts in certain settings or situations (Markus, 1977). One such prominent schema among Black women is the Superwoman Schema (SWS) (Woods-Giscombé, 2010), which postulates that the self-schemas of many Black women reflect perceived obligation to (1) present an image of strength, (2) resist displays of vulnerability or dependency, (3) suppress negative emotions, (4) succeed regardless of resources, and (5) help others (Woods-Giscombé, 2010). Such strength-based schemas have been associated with anxiety and depression, sleep disturbance, delays in self-care, reduced help-seeking behavior, and dysregulated eating in Black women (Abrams et al., 2019; Black and Woods-Giscombé, 2012; Harrington et al., 2010; Watson and Hunter, 2015; Woods-Giscombe et al., 2019). The aims of the current exploratory study were to examine whether (1) normal weight, overweight, and obese Black women differed in their perceptions of types of barriers and (2) the SWS predicts perceived barriers to weight self-management.
Method
Participants and design
A convenience sample of 169 adult Black women aged 18 and older was recruited from university students taking psychology courses at a Predominantly Black Institution in the Southeastern United States as part of a larger study of perception and health. The institution serves an undergraduate population that is 71% women and 64% Black or African American. The student body reflects 82% minority population. Women (N = 122) who had complete data on the primary study variables were retained for the current cross-sectional study.
Procedure
This study was approved by the institution’s IRB. Psychology instructors emailed their students an introduction to the study purpose and an online Qualtrics survey. Students were offered one point of extra credit, the opportunity to be placed in a raffle for a $25 gift card in exchange for participation, or to complete an alternative assignment for extra credit. Students consented to participating in the study by endorsing on the Qualtrics survey that they were at least 18 years old and desired to participate. The students were not required to record any personally identifying information.
Measures
Demographic and anthropometric variables
A demographics questionnaire developed by the study investigators assessed age, gender assignment at birth, height, weight, household income, marital status, and diagnosed medical conditions. Age was measured as a continuous variable. Self-reported height (measured in inches) and weight (measured in pounds) were used to calculate body mass index (BMI) (Weir and Jan, 2020). Household income was assessed using census categories and adjusted for household size using the “equivalence scales” methodology (Johnson et al., 2005). Participants endorsed if they had been diagnosed with and/or took medication for psychological (depression, anxiety disorder, schizophrenia/psychotic disorder, attention deficit hyperactivity disorder) and physical (diabetes, high cholesterol, arthritis, hyperthyroidism, hypothyroidism, hypertension, sleep apnea, heart disease, Cushing’s syndrome, Polycystic Ovarian Syndrome, menopause, Addison’s Disease) health conditions. Each condition was dummy coded (0 = did not have; 1 = did have) and a mean was generated based on the overall number of psychological and physical conditions (see Table 1). These specific psychological variables were selected as controls due to the common prevalence of anxiety and depression in college students (American Psychiatric Association, 2013; Ramón-Arbués et al., 2020) and the clinical associations of all of the conditions with psychiatric-medication induced obesity (Schwartz et al., 2004). Physical conditions were selected as controls due to their long-standing and consistent associations with obesity in the extant literature (e.g. Guh et al., 2009; Hall et al., 2015; Kyriacou et al., 2019; Seravalle and Grassi, 2017). See Table 1 for participant characteristics.
Participant characteristics.
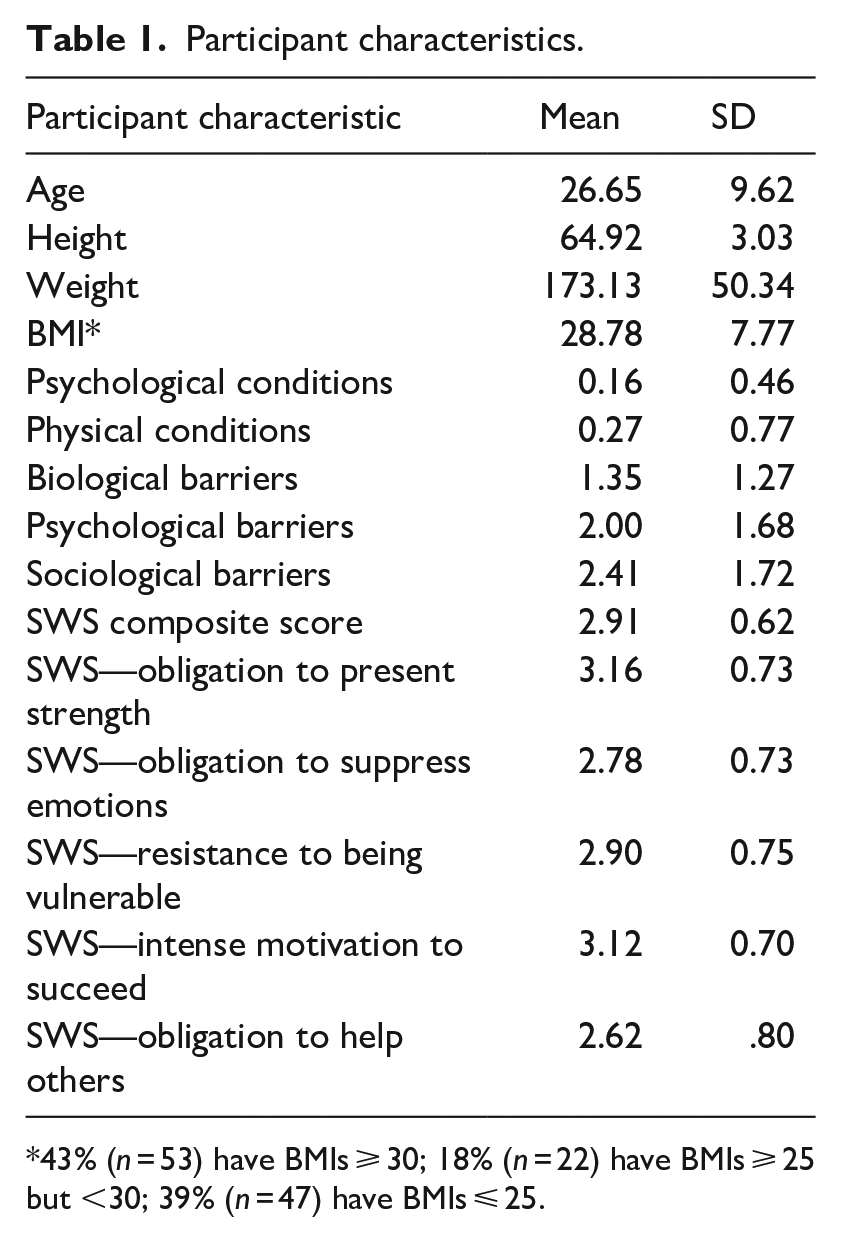
43% (n = 53) have BMIs ⩾ 30; 18% (n = 22) have BMIs ⩾ 25 but <30; 39% (n = 47) have BMIs ⩽ 25.
Superwoman schema
The Giscombe Superwoman Schema questionnaire (Woods-Giscombe et al., 2019) is a 35-item questionnaire that asks women to endorse the frequency (1 = “not true for me”; 4 = “all the time”) with which they held beliefs and engaged in specific behaviors associated with the superwoman role. The survey yields a total scale score (current chronbach’s alpha = 0.96) as well as subscale scores across the five domains that comprise the SWS: obligation to manifest strength, obligation to suppress emotions, resistance to vulnerability/dependency, determination to succeed, and obligation to help others. See Table 1 for descriptive statistics on SWS scores.
Perceived barriers to weight management
Perceived barriers to weight management identified in the extant literature (Jilcott Pitts et al., 2013; Spaeth et al., 2015; Warren et al., 2016) were classified into biological, psychological, and sociological barriers. Participants endorsed the degree to which the barriers interfered with their weight management efforts on a scale of “Not at all” to “Extremely.” Five items reflected biological barriers (pregnancy, menopause, genetics, medical conditions, too tired/lack of energy); eight reflected psychological barriers (lack of motivation, lack of self-discipline, self-conscious about public exercise, frequent stress, binge eating, hair concerns, don’t like to sweat, lack of time); and five reflected sociological barriers (work/employment, no access to a gym, no safe place to exercise, not enough money for healthy food, family food preferences). Although other barriers may exist, these barriers were selected based upon their prominent and consistent associations in the extant literature (e.g. Jilcott Pitts et al., 2013; Spaeth et al., 2015; Warren et al., 2016). See Table 1 for descriptive statistics on perceived barriers to weight management.
Statistical analyses
Data were analyzed using SPSS statistical software for Windows, version 25. Two-tailed tests were used in analyses, with a significance level of p < 0.05. To minimize the impact of missing data, a mean interference score for each barrier was calculated for each participant and the sum of that mean interference score was used in analyses. The mean number of perceived barriers to weight management were as follows: biological (M = 1.35, SD = 1.27), psychological (M = 2.00, SD = 1.68), and sociological barriers (M = 2.41, SD = 1.72). To minimize the impact of missing data, the mean values of the SWS subscales were calculated for participants who completed at least two-thirds of the items and a composite SWS score reflecting the sum of mean scores on the SWS subscales was constructed (M = 2.91, SD = .62 ).
Of the 122 women in the sample, 43% had BMIs ⩾ 30 (classified in obese range) (N = 53), 18% had BMIs above 25 but less than 30 (classified in the overweight range) (N = 22), and 39% had BMIs less than or equal to 24 (classified in the normal weight range) (N = 47). These classifications are based on the National Institutes of Health, National Heart, Lung, and Blood Institute’s BMI classification taxonomy (NHLBI Obesity Education Initiative, 2000). See Table 1 for descriptive statistics. Three One-Way ANOVAs were conducted with biological, psychological, and sociological barriers as dependent variables and BMI category as the independent variable to examine differences among women with obesity, overweight, and normal weight. Tukey HSD Post-hoc tests were utilized to identify the source of statistically significant differences. There was a significant difference in biological (F (2, 119) = 5.60, p = 0.01), psychological (F (2, 119) = 10.04, p < 0.01), and sociological (F (2, 119) = 3.97, p = 0.02) barriers among women of different weight classifications. Women with BMIs in the obese classification range reported more biological barriers (M = 0.62, SD = 0.52) compared to women whose BMIs were classified in the normal weight range (M = 0.28, SD = .41). They also reported more psychological barriers (M = 0.96, SD = 0.60) compared to women with BMIs in the normal weight classification (M = 0.43, SD = 0.55) and more sociological barriers (M = 0.75, SD = 0.68) compared to women in the normal weight classification (M = 0.41, SD = 0.56). There were no significant differences in perception of barriers found between women with BMIs in the overweight and obese classifications or between women with BMIs in the overweight and normal weight classifications.
Correlations were used to examine associations between demographic variables and endorsed physical and psychological conditions with the primary study variables. Age, BMI, total number of physical, and total number of psychological conditions had significant correlations with the primary study variables and were entered as predictors at the first step and the SWS score was entered as a predictor at the second step in hierarchical regression models. Table 2 depicts the regression analyses testing whether SWS predicted the three types of perceived barriers to weight management. When predicting the biological barriers, the full model accounted for 19% of the variance (F (5, 116) = 5.51, p < 0.01), and psychological conditions and BMI were significant positive predictors. When predicting psychological barriers, the full model accounted for 24% of the variance (F (5, 116) = 7.35, p < 0.01) and psychological conditions, BMI, and the SWS were significant positive predictors. When predicting sociological barriers, the full model accounted for 18% of the variance (F (5, 116) = 4.94, p < 0.01), and physical conditions, BMI, and the SWS were significant positive predictors.
Predicting barriers from control variables and superwoman schemas.
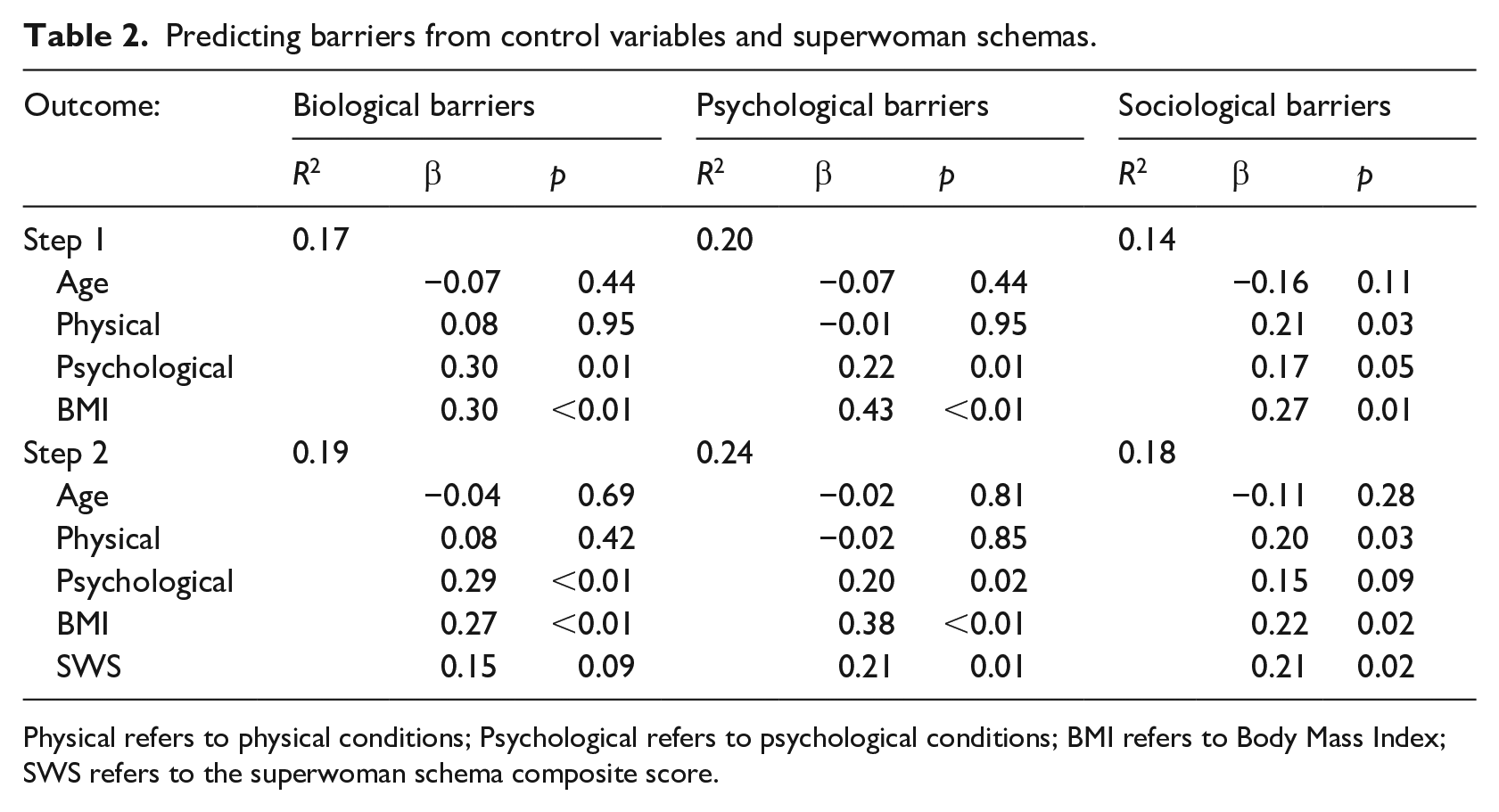
Physical refers to physical conditions; Psychological refers to psychological conditions; BMI refers to Body Mass Index; SWS refers to the superwoman schema composite score.
Results
Our findings revealed that in comparison to Black women with BMIs less than 25, those with BMIs greater than or equal to 30 reported significantly more biological, psychological, and sociological barriers to weight management. There were no significant differences found in perception of barriers between women with BMIs above 25 but less than 30 and those with BMIs that were 30 or higher. Similarly, no differences were found between women with BMIs ranging above 25 but less than 30 and those with lower BMIs in perception of barriers. For Black women participating in our study, psychological conditions and BMI were predictors of biological barriers. Psychological conditions, BMI, and the SWS were predictors of psychological barriers. Physical conditions, BMI, and the SWS were predictors of sociological barriers.
Discussion
In this study, nearly a fourth of the variance in perceived interference of psychological barriers and almost a fifth of the variance in sociological barriers was explained by older age, having psychological conditions, higher BMI and endorsement of the SWS, with the SWS uniquely contributing to this variance. Hence in this exploratory study, the plausible significance of SWS in understanding weight management is established.
Such findings suggest that individual SWS domains or the interactions between them may explain perceived barriers to self-regulation of weight. Although Black women’s strength is adaptive and has been documented as a buffer against stigma, racism and discrimination (Allen et al., 2019; Watson and Hunter, 2015) an untoward finding is the adverse associations of strength with self-care. After controlling for age, self-reported psychological and physical conditions and BMI, women higher in the SWS in this study were more likely to perceive that psychological and sociological factors negatively interfere with their ability to achieve and maintain a healthy weight.
The extant research suggests that in the Black community, superwomen are socialized through cultural experiences. Compared to White and Latina mothers, Black mothers are more likely to view strength, self-reliance, and independence as desirable and necessary for their girls’ development to ensure their success within the larger society (Oshin and Milan, 2019). It is likely that women high in the SWS have been exposed to models of independence and strength from a young age and heavily encouraged to value achievement while minimizing negative affect and vulnerability (Oshin and Milan, 2019). This value of fortitude is embedded within the collectivistic orientation of the culture (Coon and Kemmelmeier, 2001) and could explain the prioritization of the needs of their families and communities over their own while minimizing help seeking behavior. Unfortunately, the inhibition of emotional expression which is also characteristic of the SWS has a long-standing association with negative psychological and physical outcomes (Chapman et al., 2013; Gross and John, 2003; John and Gross, 2004,), including unhealthy coping through emotional eating (Ferrer et al., 2017; Harrington et al., 2010). Self-awareness of the stress associated with being strong and successful while attempting to care for others and contribute to their community likely influences their perceptions of psychological barriers. This is consistent with our finding that women who endorsed psychological conditions (e.g. anxiety, depression) were also more likely to endorse other psychological barriers beyond psychological conditions.
According to the ego-depletion framework, people have a limited amount of self-control resources and the depletion of such resources can diminish successful self-regulation (Baumeister, 2002). Specifically, self-control has been found to become depleted in a variety of contexts that quite naturally underscore aspects of the SWS, such as suppression of emotions, relationship maintenance, and even ineffective eating behaviors have been linked to ego-depletion (Mead et al., 2010). Thus, internalization of the SWS may serve to directly undermine self-control resources which may compound perceptions of barriers to weight management or even direct beliefs/behaviors that govern healthy weight management.
The obligation to prioritize caregiving of others may also influence perception of barriers given that caregiving creates a competing role demand that requires a commitment of time as well as psychological resources (Mead et al., 2010). What remains unclear from our study is whether overweight and obese women compared to normal weight women indeed have greater caregiving responsibilities compared to their normal weight counterparts. Given the association of higher BMI with perceived barriers in our study, future research is needed to determine whether perceived obligations for caregiving is more prominent than other components of the SWS for overweight/obese women. This may have implications for these women’s perceptions of psychological barriers.
Perceived sociological barriers such as family food preferences and a lack of financial resources to purchase healthy foods for oneself when the family prefers different foods may also reflect the tendency to prioritize others needs over one’s own. This may be particularly important for the college women in this study whose mean adjusted income was less than $20,000. Budgetary decisions to support one’s health may not take precedence over those to support their families. A limitation of this study is that we did not objectively assess the caregiving, including financial responsibilities of women in this study.
The heterogeneity of Black women likely extends to differences in how the different domains that comprise the SWS are manifested and differentially affect health behaviors. This should be a focus of future research. An interesting finding in this study is that women with BMIs classified in the obese range, but not women with BMIs classified as overweight, differed from women whose BMIs were classified in the normal weight range in their perceptions of barriers. In past research overweight black women were more likely to perceive their weight classification as normal weight (Harris et al., 2016). These differences in subjective perceptions of BMI are also evident among adolescent Black girls (Martin et al., 2010). Over 50% of women classified as overweight in the current study perceived themselves at most as normal weight. Previous research indicates that self-reported weight in Black young adults is highly correlated with objective measures of weight (Olfert et al., 2018). Therefore, it is probable that women in this study accurately reported their weight and height for calculation of BMI. This notwithstanding, consistent with previous research (Harris et al., 2016), women with BMIs ranged above 25 but less than 30 in this study were more likely to describe their weight category as “normal weight” despite having BMIs that fall into the NIH classification of “overweight.” Consequently, they may have similarly perceived their barriers the same as women with lower BMIs. This can be problematic given that women with BMIs above 25 but less than 30 share similar risks to women with higher BMIs. Overweight women who misperceive their weight do not meet the recommendations for physical activity compared to other ethnic groups, conferring greater risk for adverse health effects such as cardiovascular disease (Chomistek et al., 2013; Duncan et al., 2011). This suggests the importance of developing interventions that target misperceptions of weight, particularly those high in the SWS, to prevent further escalation of BMI-related risk factors. Finally, it is critical that weight management interventions with Black women address the distinct cultural aspects of identity associated with the SWS to influence perceptions of barriers and find ways to improve self-efficacy to overcome them. In line with emerging research, weight management interventions should be attuned to culturally relevant contexts (Bowie et al., 2018; Di Noia et al., 2013) to enhance their efficacy. Kong et al. (2014) noted several interventions that are culturally sensitive approaches such as training church members as health educators, using cookbooks in dietary interventions that are relative to specific regions, and addressing barriers to behavior change that are unique to black women. Being that Black women are less likely to maintain weight loss (Murphy and Williams, 2013) developing culturally relevant interventions is essential for addressing the myriad of unique factors that Black women face that serve to limit the utility of conventional interventions. The current findings suggest that consideration of SWS may further enhance the effectiveness of those interventions and their efficacy may be facilitated by considering the SWS.
Strengths and limitations
The primary strength of this study includes the exploration of a culturally-relevant framework (the SWS) for examining health disparities in perceived barriers to weight loss among Black women. A prospective limitation is that the sample participants were relatively young and college educated, which potentially introduces a sampling bias as the findings may not generalize to other populations of Black women. This notwithstanding, the mean age of the women in this study was 27 years old, thus these findings may be generalizable to a broader group of women than traditional undergraduate students. The findings may be even more robust among older individuals who may find more barriers encompass their everyday experiences. Another limitation is that the data acquired was via self-report, which may be prone to social desirability bias. While past research shows a consistently significant and high correlation between self-report and actual weight (r’s 0.87–0.92) (Olfert et al., 2018), BMI calculated from self-reported height and weight in this study can still pose a potential limitation. Lastly, the selected physical and psychological conditions controlled in the study as well as the barriers appraised in this study are not exhaustive.
Conclusion
The current study builds upon emerging work involving the SWS and health risk among Black women. It uniquely contributes to the research on barriers to weight loss in Black women by exploring the role of culturally-relevant strength-based schemas in U.S. Black women’s perceptions of barriers to weight loss efforts. Based on general findings documenting the SWS globally predicts differences in perceptions of barriers to weight management, future research might want to examine the contributions of the individual dimensions of SWS to better understand how this construct relates to health outcomes.
Supplemental Material
sj-docx-4-hpq-10.1177_13591053211068974 – Supplemental material for Superwoman’s kryptonite: The superwoman schema and perceived barriers to weight management among U.S. Black women
Supplemental material, sj-docx-4-hpq-10.1177_13591053211068974 for Superwoman’s kryptonite: The superwoman schema and perceived barriers to weight management among U.S. Black women by Charlie L Harris, Brian M Goldman, Pinar Gurkas, Crystal Butler and Priscilla Bookman in Journal of Health Psychology
Supplemental Material
sj-docx-5-hpq-10.1177_13591053211068974 – Supplemental material for Superwoman’s kryptonite: The superwoman schema and perceived barriers to weight management among U.S. Black women
Supplemental material, sj-docx-5-hpq-10.1177_13591053211068974 for Superwoman’s kryptonite: The superwoman schema and perceived barriers to weight management among U.S. Black women by Charlie L Harris, Brian M Goldman, Pinar Gurkas, Crystal Butler and Priscilla Bookman in Journal of Health Psychology
Research Data
sj-sav-1-hpq-10.1177_13591053211068974 – for Superwoman’s kryptonite: The superwoman schema and perceived barriers to weight management among U.S. Black women
sj-sav-1-hpq-10.1177_13591053211068974 for Superwoman’s kryptonite: The superwoman schema and perceived barriers to weight management among U.S. Black women by Charlie L Harris, Brian M Goldman, Pinar Gurkas, Crystal Butler and Priscilla Bookman in Journal of Health Psychology
Supplemental Material
sj-sps-2-hpq-10.1177_13591053211068974 – Supplemental material for Superwoman’s kryptonite: The superwoman schema and perceived barriers to weight management among U.S. Black women
Supplemental material, sj-sps-2-hpq-10.1177_13591053211068974 for Superwoman’s kryptonite: The superwoman schema and perceived barriers to weight management among U.S. Black women by Charlie L Harris, Brian M Goldman, Pinar Gurkas, Crystal Butler and Priscilla Bookman in Journal of Health Psychology
Supplemental Material
sj-spv-3-hpq-10.1177_13591053211068974 – Supplemental material for Superwoman’s kryptonite: The superwoman schema and perceived barriers to weight management among U.S. Black women
Supplemental material, sj-spv-3-hpq-10.1177_13591053211068974 for Superwoman’s kryptonite: The superwoman schema and perceived barriers to weight management among U.S. Black women by Charlie L Harris, Brian M Goldman, Pinar Gurkas, Crystal Butler and Priscilla Bookman in Journal of Health Psychology
Footnotes
Data sharing statement
The current article includes the complete raw dataset collected in the study including the participants’ data set, syntax file and log files for analysis. These files are available in the Figshare repository and as Supplemental Material via the SAGE Journals platform.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.