
Abstract
End-of-life (EOL) medical care in the United States often does not align with patients’ goals and preferences. This study explored EOL hopes and fears among 86 community-dwelling adults and examined medical and psychological predictors of death anxiety. Common EOL hopes included absence of suffering, closure, and personal fulfillment. Common EOL fears included suffering, lack of competence, and specific types of death. Fear of the dying process was greater than fear of death itself. Health predicted death anxiety; age alone, did not. Advance care planning and clinical decision making should include these psychological insights and explicitly address EOL hopes and fears.
Psychologists have examined the universal impact of death and dying for more than a century (Hall, 1915). These efforts include dissecting death’s meaning (Feifel, 1959), identifying coping mechanisms (Pyszczynski et al., 2021), and exploring different time perspectives (Carstensen and Hershfield, 2021). In the United States (US), integrating these psychological insights into clinical decision making is hampered by a medicalized system of clinical training, care, and reimbursement. Physicians themselves have criticized the medicalization of death and dying. Some have lamented the shift away from death as a natural occurrence at home to a perceived technical failure in the hospital (Steinhauser and Tulsky, 2015). Others have identified training gaps that leave physicians ill-prepared to honor dying patients’ personhood and ameliorate psychological suffering (Byock, 1996). These issues clearly manifest in the psychological disconnect between physicians’ preferences for low intensity, comfort-based measures at the end of their own lives, and the costly, invasive, often futile measures they routinely deliver to patients (Pizzo and Walker, 2015). This trend persists across medical specialties (Habib et al., 2019) and settings (Soliman et al., 2018), including hospice and palliative medicine (Gramling et al., 2019; Luck et al., 2017).
To address these challenges, national efforts to optimize end of life (EOL) care have centered on greater clinical attention and adherence to patient and family preferences (Committee on Approaching Death, 2015), elicited via advance care planning (ACP), and legally documented via advance directives (AD). While ACP discussion is associated with clinical quality (Bischoff et al., 2013), and for physicians, is now a reimbursable service, training in ACP communication is still not standard in medical education (Association of American Medical Colleges, 2016). Uncomfortable, unsupported, and untrained, physicians often avoid ACP discussion, or fail to adequately elicit and document patient and family preferences (Heyland et al., 2013). Payment does not substitute for training. Little evidence suggests ACP financial reimbursement enhances discussion frequency (Tsai and Taylor, 2018), Medicare claims data provide no information on ACP content or quality (Belanger et al., 2019), and a national review of AD statutes found language addressing patient quality of life in only three states (Eggenberger et al., 2020).
In addition to these systemic barriers, patient and family-related barriers to ACP have also been identified among healthy (Fulmer et al., 2018) and seriously ill patient populations (You et al., 2015). Chief among these is lack of knowledge about or lack of motivation to engage in ACP (Blackwood et al., 2019). That said, many primary care patients and health care providers report positive views of ACP (Jimenez et al., 2018). Further, most of the general population (80%–90%) is aware of the ACP concept and believes it is important (Grant et al., 2021). Although patients and families are willing to have these conversations; most expect their health care providers to initiate them (Howard et al., 2018). Unfortunately, this does not occur: 92% of primary care patients report never having these conversations with their primary care provider (Howard et al., 2018). Consequently, most individuals have not identified a health care proxy or completed an AD (Grant et al., 2021), leaving patient and family EOL preferences largely unknown.
A psychological approach
Fortunately, psychological approaches are effective when it comes to EOL conversations and care. In response to medicalization, palliative psychology has emerged (Strada, 2017). Palliative psychological interventions are evidence-based (Von Blanckenburg and Leppin, 2018), particularly for EOL anxiety and depression (Fulton et al., 2018). Unfortunately, while some physicians have advocated for psychology integration (Gundersen, 2015) access to psychosocial intervention is still not standard EOL care (Committee on Approaching Death, 2015); however, this may be changing. The Society of Behavioral Medicine formed a palliative care special interest group (Hoerger et al., 2019), the first author (ADF) co-created and co-chairs a similar group within the American Psychological Association (@EOLSIG), and the second author (BB) has directed medical student and resident clinical rotations in geriatrics and palliative care, and recently served on an expert advisory panel addressing behavioral health integration and serious illness care (Cheung et al., 2019).
Consistent with these initiatives, the psychological concept of person-centeredness (Rogers, 1951) is increasingly being applied to medical care (American Geriatrics Society, 2016). Person-centeredness requires accurate empathy and lack of judgment, focuses on physical and emotional well-being, and ensures medical care is consistent with patient goals and preferences. Although an important step, the clinical disconnect between describing and delivering person-centered care persists (Grant et al., 2021). Greater integration of psychological insights and training is necessary to effectively elicit and honor patient goals and preferences throughout the lifespan, and ultimately improve ACP and EOL care. Recent research supports a psychological approach to these conversations. For example, person-centered factors including personal control and dignity were the most influential motivators for ACP among healthy adults and actually predicted AD completion regardless of age (Genewick et al., 2018).
Possible selves
Possible selves, by definition, represent a person-centered construct encapsulating an individual’s most salient future hopes and fears. Possible selves are elements of the self-concept that include what a person expects to become, hopes to become, or is afraid of becoming (Markus and Nurius, 1986). Related research has identified differences in hopes and fears related to age, developmental stage, and cultural context (Frazier and Hooker, 2006). For example, health-related hopes and fears begin to emerge in midlife and persist through older adulthood (Dark-Freudeman and West, 2016; McGinty et al., 2013). Further, older adults often report fears related to losing independence, autonomy, and burdening their family (Frazier et al., 2003). Although common hopes and fears related to aging and specific illnesses have been identified (Cotrell and Hooker, 2005; Kristiansen et al., 2017), possible selves related to dying, death, and loss have been ignored. Thus, the current study sought to fill this gap by identifying common EOL possible selves among community dwelling adults within the US.
Study aims
Aim 1: Explore common themes that emerge among the end-of-life hopes and fears of health adults.
Aim 2: Examine the degree to which adults feel capable of achieving their end-of-life hopes and avoiding their end-of-life fears.
Aim 3: Identify death-related attitudes of adults and explore how death anxiety relates to medical (chronological age and general health) and psychological (depressive symptoms and self-efficacy) factors.
Method
Participants
The sample included 86 healthy adults ages 42–88 (M = 54.74, SD = 9.41) recruited via university students in the southeastern US. Participants were predominately Caucasian (90.7%), female (66.3%), married (76.7%), and Christian (71.8%). Eligible participants were 40 years of age or older, fluent in English, and had computer access with reliable internet. This age range was selected to ensure the sample included both middle-aged and older adults.
Procedure
The study was approved by our Institutional Review Board, IRB protocol #16-0131. Participants were recruited through the university’s research pool from 2016 through 2017. Students were asked to identify one to two family members who could be invited to complete an online survey. Students, with the help of a research assistant, emailed family members a form letter containing detailed directions and a unique survey link. Students received credit toward their introductory psychology course for their own participation in a subsequent survey and an additional credit for sending invitations to family members. This additional credit was not contingent on survey completion.
After opening the email and following the survey link, participants were presented with an online consent form. The survey began with the possible selves questionnaire followed by the remaining items concerning death anxiety, health, depressive symptoms, and demographics.
Measures
Possible Selves Questionnaire (PSQ)
The PSQ is an open-ended questionnaire designed to elicit qualitative data on hopes and fears for the future (Frazier and Hooker, 2006). The current study modified the PSQ to focus on end-of-life (EOL) hopes and fears. Participants were first asked to describe their end-of-life hopes related to death and dying. Participants then identified their most important end-of-life hope. Next participants answered two follow-up questions on a 7-point Likert scale (1 = Not at all, 7 = Very), assessing self-efficacy related to achieving their most important EOL hope: “How capable do you feel of attaining this end-of-life hope?” and “How likely do you think it is that this hope will be attained?” Participants then described their end-of-life fears related to death and dying, identified their most dreaded EOL fear, and answered two follow-up questions assessing self-efficacy for preventing their most dreaded EOL fear. Self-efficacy items were averaged to create a specific measure of self-efficacy related to attaining and avoiding EOL hopes and fears. Possible selves were coded by two independent raters and examined using QSR International’s NVivo 10.
Death Attitude Profile-Revised (DAP-R): The DAP-R is a 32-item scale assessing attitudes toward death on five subscales: fear of death, death avoidance, neutral acceptance, approach acceptance, and escape acceptance (Wong et al., 1994). The current study focused on two of the subscales, fear of death and death avoidance. Participants responded on a 7-point Likert scale (1 = Strongly disagree, 7 = Strongly agree) to statements such as: “I am disturbed by the finality of death,” and “I avoid thinking about death altogether.” The DAPR had acceptable reliability (32 items; α = 0.78).
Revised Collett-Lester Fear of Death and Dying Scale (RCL): The RCL (Collett and Lester, 1969; Lester, 1990) is a 32-item scale assessing fear of death and dying on four subscales: the fear of one’s own death, the fear of one’s own dying process, the fear of the death of others, and the fear of the dying process of others. Participants were asked “How disturbed or made anxious are you by the following aspects of death and dying?” and responded on a 5-point Likert scale (1 = Not at all, 5 = Very) to statements such as “The pain involved in dying.” The RCL was highly reliable (32 items; α = 0.94).
General Health: The SF36 General Health subscale is 5-item scale assessing general health perceptions (Ware and Sherbourne, 1992). Participants responded on a 5-point scale (1 = Definitely false, 5 = Definitely true) to statements such as “I am as healthy as anybody I know.” Internal consistency is high for the SF-36 subscales, generally exceeding 0.80 (Ware & Sherbourne, 1992).
The Center for Epidemiological Studies Depression Scale (CES-D): The CES-D is a 20-item scale assessing depressive symptoms experienced within the past week (Radloff, 1977). Participants responded on a 4-point scale: (0 = Less than 1 day, to 3 = 5–7 days), to statements such as “I was bothered by things that usually don’t bother me.” The CES-D was highly reliable (20 items; α = 0.93).
Demographic Questionnaire: The demographic questionnaire requested basic demographic information including age, gender, race, and religion.
Data analyses
The current study used a mixed methods approach (Levitt et al., 2018). This approach included eliciting both open-ended qualitative data on EOL possible selves as well as quantitative data examining death anxiety, health, self-efficacy, and depressive symptoms. Analyses are described below.
Qualitative analyses
Thematic analysis was used to explore the content of the open-ended EOL possible selves data using the small q approach (Braun & Clark, 2012) for Aim 1. According to a systematic review by Vasileiou et al. (2018) sample size estimates for qualitative analyses range from 12 to 50 participants. Our sample (n = 86) is therefore adequate. First, to establish data familiarization (Clark and Braun, 2016) the first author reviewed all of the possible selves data and took notes of recurring themes. The first author then examined the notes looking for potential redundancy or overlap among the data. For example, rather than have separate codes for every possible type of death mentioned by our participants (cancer, stroke, accident), the first author created a broader code, type of death, to capture these EOL hopes and fears. Eleven unique themes were subsequently identified from the qualitative data. Using the final 11 themes, the first author developed a coding guide. The coding guide provided a clear and concrete definition for each theme as well as its corresponding numerical code.
Next the coding guide was applied to the dataset. Using the coding guide, all EOL hopes and fears were coded by two independent raters. Interrater reliability was then calculated for hopes (Kappa = 0.82) and fears (Kappa = 0.80) indicating almost perfect agreement (Landis and Koch, 1977).
Quantitative analyses
For Aim 2, one-sample t-tests were used to examine self-efficacy for attaining EOL hopes and avoiding EOL fears. For Aim 3, we examined descriptive statistics of death anxiety on the DAPR and RCL. In addition to these basic observations, two hierarchical regressions were used to analyze medical (chronological age and general health) and psychological predictors (self-efficacy and depressive symptoms) of our outcome variable, death anxiety. Fear of death on the DAPR was entered as the outcome variable for the first hierarchical regression. Death anxiety on the RCL (RCL Total) was entered as the outcome variable for the second hierarchical regression. A sensitivity power analysis using G*Power (Faul et al., 2009) indicated that a sample of 85 participants was adequate for our linear regression models.
Results
Qualitative results are presented first, followed by quantitative results.
Qualitative end-of-life hopes and fears
The following 11 themes were identified through thematic coding and applied to the open-ended EOL data.
Having loved ones present: Included references to being with friends and family (“Seeing my children, having them with me when my time expires.”) or being alone (“Being alone.”).
Religious or spiritual concerns: Included references to personal faith or spirituality (“Being in the presence of God.” and “Spiritual peace.” or “That I have not reconciled with God.”).
Suffering: Included references to pain and suffering (“Being warm and comfortable.” or “Having to go through a long, painful dying process, with many painful treatments.”).
Closure: Included references to saying good-bye (“To be able to say goodbye to everyone I love.”) and letting loved ones know that they are loved (“I want all my family to know that I love them.”).
Legacy: Included references to making a difference or an impact in the world (“I want to die knowing that I made a positive impact somewhere in the world”) or to someone else’s life (“I hope to have been helpful to others.”).
Fulfillment: Included references to living a full life (“I hope to have had a long life with awesome experiences.”) or a life free from regret (“That I have no regrets.” and “That I feel happy and fulfilled with my life.”).
Physical and Mental Competence: Included references to remain physically able or independent (“That I am independent mentally and physically.”) and fears regarding incompetence or incapacitation (“Unable to function mentally, physically immobile, incontinent.”) and (“being bedridden and unable to communicate with others.”).
Type of Death: Included references to specific types of or circumstances surrounding death (“Die of old age in my sleep” or “Dying unexpectedly”).
Impact on Others: Included references to grief and acceptance (“I hope my loved ones have time to accept my death and feel happy about the time we’ve had together.”) and becoming a burden to other people (“That I am not a burden for loved ones.”).
Family: Included references children or grandchildren (“I simply hope to see my children grow to adulthood and enjoy any grandchildren that they might have.”) or (“not being able to watch my kids finish growing up and having kids of their own.”).
Peace: Included references to a peaceful death, being ready for death, or accepting ones death (“To die peacefully.” and “I would like to go peacefully and with mental awareness.”).
Next, a cluster analysis was conducted. The cluster analysis provides a visual representation of the major themes reported by participants. The relative frequency of each word is represented by the size of the word. Thus, larger words indicate that a word appeared more frequently in the data. For example, when examining EOL hopes, “love,” “family,” and “pain-free” were large in relation to most other words as many participants prioritized being with their family and avoiding pain and suffering. When examining fears, words like “pain,” “alone,” and “suffer” occurred most frequently. See Supplemental Material for figures.
Frequency analyses were also conducted. The most common end-of life hopes mentioned by participants concerned the absence of suffering (18.6%), followed by closure with loved ones (10.5%), and types of death (9.3%). See Table 1. The most common end-of life fears mentioned by participants concerned the presence of suffering (22.1%), a lack of physical or mental competence (17.4%), and types of death (15.1%). See Table 1.
Frequency distribution of end-of-life hopes and end-of-life fears by qualitative theme.
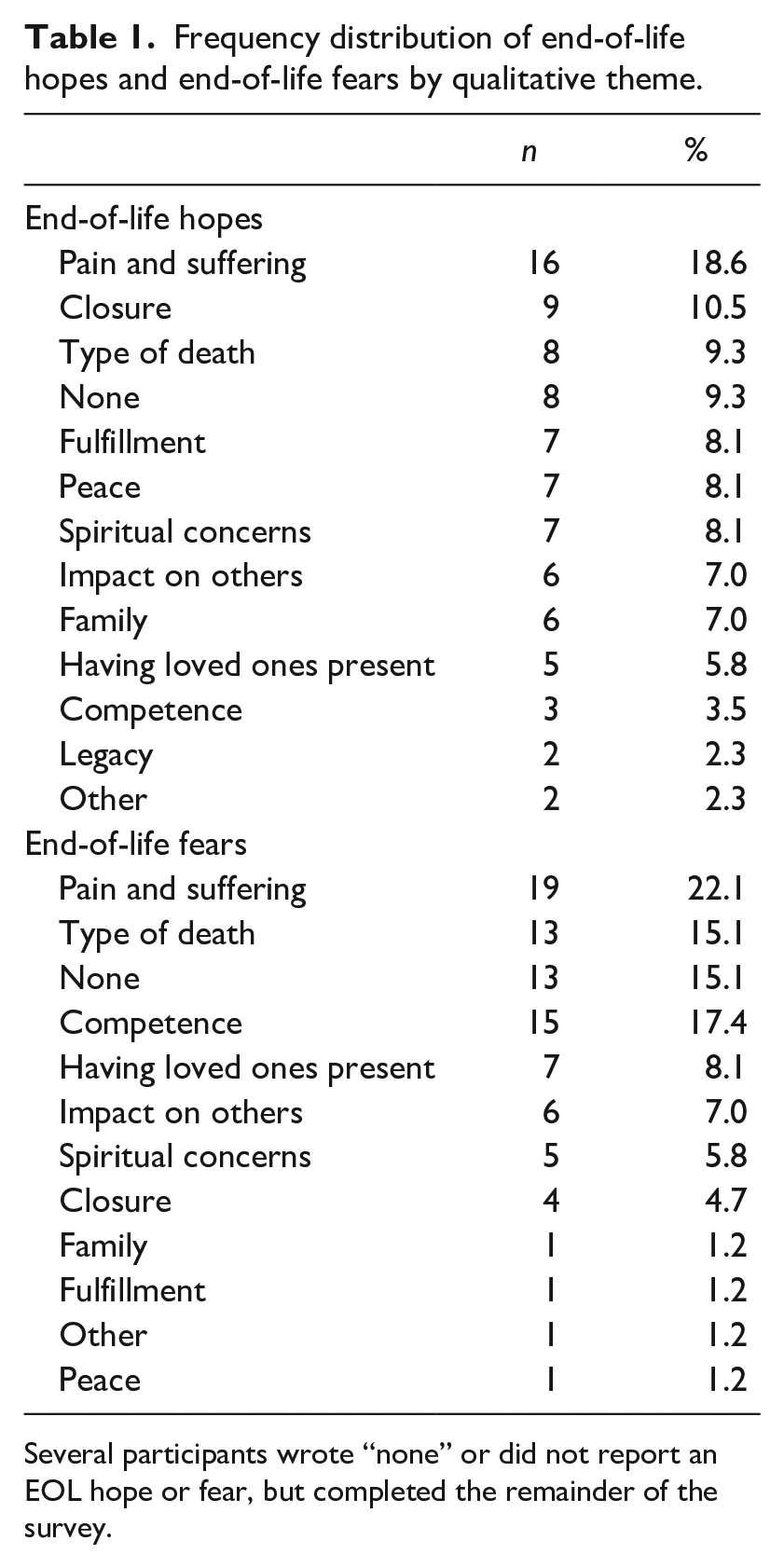
Several participants wrote “none” or did not report an EOL hope or fear, but completed the remainder of the survey.
Quantitative results
Next, we examined quantitative data. To compare the degree to which participants felt capable of achieving their EOL hopes and avoiding their EOL fears, a one-sample t-test was conducted. Overall, participants reported significantly higher levels of self-efficacy related to attaining their end-of-life hopes (M = 9.44, SD = 3.25) than avoiding their end-of-life fears (M = 7.96, SD = 3.20), t(75) = 3.33, p < 0.001.
Death anxiety was examined via scores on both the DAPR and RCL. Participant fear of death was relatively neutral on the DAPR (M = 3.52, SD = 1.41) fear of death subscale, indicating acceptance of death as a naturally occurring part of life. Next, we examined fear of death more specifically via the RCL. Unlike the DAPR which focuses solely on the individual, the RCL examines death anxiety related to one’s own dying and death as well as anxiety related to the dying and death of close others. Participants’ greatest fear was the dying process of a loved one (M = 3.29, SD = 0.89). Further, participants feared their own dying process (M = 3.17, SD = 0.89) more than death itself (M = 2.40, SD = 0.94), t(85) = −8.56, p = 0.000.
Last, to identify how death anxiety relates to medical (chronological age and general health) and psychological factors (depressive symptoms and self-efficacy for attaining EOL hopes and avoiding EOL fears) two hierarchical regressions were conducted separately for our two measures of death anxiety.
First, to examine the unique contributions of medical and psychological predictors of death anxiety, a hierarchical regression was conducted. Variables were entered in two steps. In step 1, fear of death on the DAPR was entered as the dependent variable; medical factors (chronological age and general health) were entered as independent variables. In step 2, psychological factors were entered (self-efficacy and depressive symptoms) as independent variables. The results of step 1 were significant, F(2, 71) = 8.80, p < 0.001. The variance accounted for by the medical factors equaled 0.20 (adjusted R2 = 0.18). General health was the only significant predictor, β = −0.31, p < 0.01. In step 2, the psychological factors were entered into the regression equation. The change in variance accounted for (ΔR2) was equal to 0.04 which was not significant, F (2, 69) = 1.73, NS. The unstandardized regression coefficients (B), intercept, and standardized regression coefficients (β) for the full model are reported in Table 2.
Unstandardized regression coefficients (B) and intercept, standardized regression coefficient (β), t-values, and p-values for variables as predictors of death anxiety on the DAP-R fear of death and RCL fear of death subscales.
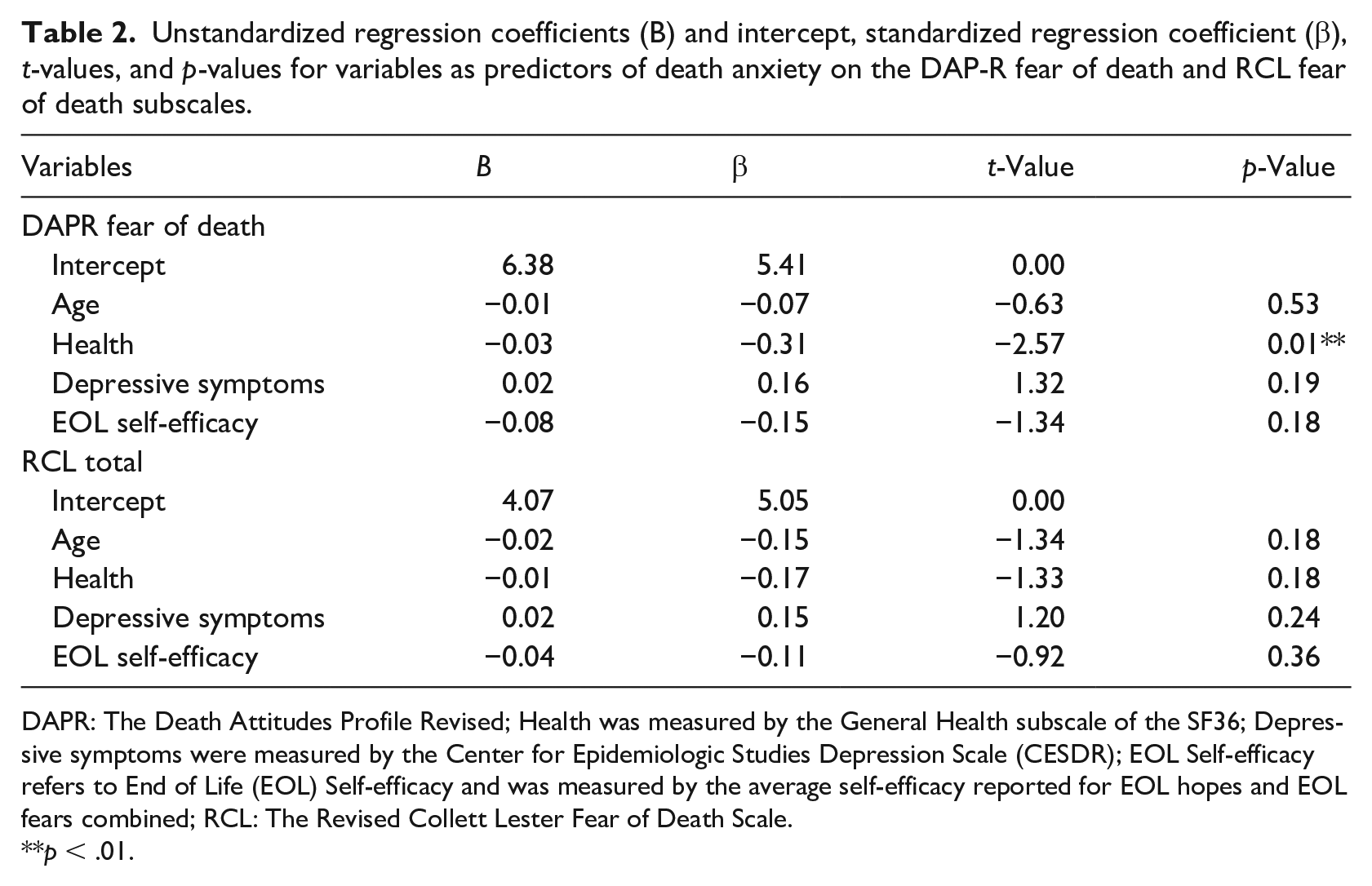
DAPR: The Death Attitudes Profile Revised; Health was measured by the General Health subscale of the SF36; Depressive symptoms were measured by the Center for Epidemiologic Studies Depression Scale (CESDR); EOL Self-efficacy refers to End of Life (EOL) Self-efficacy and was measured by the average self-efficacy reported for EOL hopes and EOL fears combined; RCL: The Revised Collett Lester Fear of Death Scale.
**p < .01.
Next, to examine the unique contribution of medical and psychological predictors of death anxiety on the RCL, a second hierarchical regression was conducted. Variables were entered in two steps. In step 1, fear of death on the RCL was entered as the dependent variable; medical factors (chronological age and general health) were entered as independent variables. In step 2, psychological factors were entered (self-efficacy and depressive symptoms) as independent variables. The results of step 1 were significant, F(2, 72) = 4.61, p < 0.01. The variance accounted for by the medical factors equaled 0.11 (adjusted R2 = 0.09). General health was the only significant predictor, β = −0.26, p < 0.05. In step 2, the psychological factors were entered into the regression equation. The change in variance accounted for (ΔR2) was equal to 0.03 which was not significant, F (2, 70) = 1.11, NS. The unstandardized regression coefficients (B), intercept, and standardized regression coefficients (β) for the full model are reported in Table 2.
Discussion
Standard EOL care in the US includes biomedical interventions to increase quantity of life but not psychosocial interventions to increase quality of life. Though this survival focus is understandable, our results demonstrated it is incomplete and often does not align with patient and family preferences. This longstanding discrepancy between what people want versus receive is due, in part, to a disproportionately medicalized system of training and care in which technical and procedural skills are prioritized while clinical communication that incorporates psychosocial factors is not. To help, the authors directly elicited EOL hopes and fears in a sample of healthy adults. Related research is rare (Llewellyn et al., 2017) and primarily qualitative in nature (e.g. Taneja et al., 2019). To our knowledge, this study was the first to collect both quantitative and qualitative data from a community-based adult sample for whom death and dying are not imminent. Several important details emerged.
First, although clinicians report patient and family related barriers to ACP communication (You et al., 2015), our findings revealed that when directly solicited, middle-aged and older adults can clearly describe their EOL hopes and fears in specific detail. Unsurprisingly, their content was not only medical but biopsychosocial in nature. The need to integrate biomedical and psychosocial care was originally conceptualized nearly 50 years ago (Engel, 1977) and has yet to be delivered as standard care. As underscored by our data and others (e.g. Crimmins et al., 2021), this ongoing failure is particularly problematic at the end of life. In our sample the most common EOL fears related to both mental and physical dimensions of pain, prolonged suffering, and loss of personal competence. Although many participants mentioned pain and suffering broadly, some were specific, for example one participant feared “losing my physical and mental abilities while still being “alive”” and another acknowledged “I do not want to be helpless. I do not want someone that I love to have to carry the burden of taking care of me and watching me die.” These psychosocial concerns were further supported by participants’ greater fear of their own dying process than of death itself, consistent with previous research (Dark-Freudeman et al., 2021). Clearly, participants fear a medicalized, burdensome, undignified death.
Notably, participants named psychosocial considerations (e.g. suffering, competence, burdening others) more frequently than spiritual and religious concerns. This has important clinical implications at the system level, as currently US health care often provides the opposite, that is, greater access to spiritual services from chaplains than psychological services from psychologists (Richardson, 2014). Correcting this disconnect is especially timely now given the current rise in the proportion of Americans with no religious affiliation (Thiessen and Wilkins-Laflamme, 2020). Our findings support current clinical attempts to deliver EOL psychological interventions that allow patients to prioritize dignity at the end of life (e.g. Chochinov et al., 2015; Wang et al., 2021) rather than focusing on longevity, aggressive medical treatments, and faith-based services.
When examining self-efficacy related to EOL hopes and fears, evidence for the importance of a biopsychosocial approach was even more apparent. Healthy adults not only feared a medicalized death, but believed they lacked the ability to prevent these fears from becoming reality. Unfortunately, published evidence suggests they are right. Despite efforts to incorporate ACP into medical care, related discussions often do not occur. Only 1/3 of Americans have completed some form of AD while 29% have completed a living will specifically outlining their healthcare wishes (Yadav et al., 2017). Similarly, appropriate referral to palliative or hospice care often does not occur or occurs too late (Crimmins et al., 2021). Those who do receive palliative care often do not receive psychological services (Ann-Yi et al., 2018) and what they do receive is often considered inadequate (McInnerney et al., 2021). Our results are consistent with this sobering clinical reality and underscore the need for a person-centered focus on maintaining personal control, identity, and a “sense of self” at the end of life (Lloyd et al., 2016; Wang et al., 2021).
Taken together, our qualitative and quantitative results suggest community dwelling adults are already aware and fearful of medicalization and its impact on death and dying but are willing to discuss their EOL hopes and fears. This has significant clinical implications and is consistent with extant literature in support of addressing EOL more openly and frequently. Educating patients about ACP has proven effective across myriad modalities (Diegelmann et al., 2022) and results in greater knowledge about, confidence in, and completion of ACP (Schickedanz et al., 2021). Clinically, we recommend that person-centered ACP discussions protect patients’ dignity by openly eliciting their EOL hopes and fears and directly translating these hopes and fears into treatment planning and decision making.
Next, our findings have implications not only for individuals navigating their own EOL hopes and fears, but also those who have experienced or anticipate experiencing loss. Many participants feared death of a loved one more than death itself. This is consistent with data from intensive care settings that reveal a 51% rate of post-traumatic stress disorder (PTSD) symptoms in decedents’ caregivers (Hartog et al., 2015). Further, nearly 25% of informal caregivers perceive a lack of psychological support from medical institutions providing EOL care for their loved ones (Heese et al., 2013). Optimal EOL care requires addressing these unmet psychological needs.
Lastly, our results demonstrated how the onset of health problems triggers fears associated with navigating the end of life in our current healthcare system, as physical health was more predictive of death anxiety than chronological age or psychological factors. This finding contrasts with the common assumption that advanced age, alone, buffers death anxiety and other psychological distress (Russac et al., 2007), underscoring the relevance of individual experience (Mock and Eibach, 2011) and perceived distance from death (Shrira et al., 2014). The limited predictive utility of chronological age in our sample is consistent with geriatrics and gerontology literature across populations (Kotter-Grühn et al., 2016), including the end-of-life context (Stephan et al., 2018). Nevertheless, chronological age is frequently used as a determinant of clinical decision making and resource allocation. Our data suggest this longstanding pattern is rooted in age-based stereotypes and bias, not evidence.
Limitations and future directions
While our focus on EOL possible selves is novel, several limitations must be acknowledged. Most obvious is our convenience sample. Though our data show that EOL hopes and fears were well defined among healthy adults, generalizability of these results may be limited due to sample demographics. Although we believe many of the EOL hopes and fears reported by our sample are universal, previous research has shown cohort and cultural differences in EOL decision making often exist (Cain et al., 2018). As a result, while our participants named psychosocial issues more frequently than religious and spiritual matters, EOL hopes and fears may still differ by culture and religion. To enhance cultural competence, future possible selves research should examine EOL perspectives across different cultural and religious groups, including the growing demographic of unaffiliated (i.e. non-religious). This would help clarify which EOL hopes and fears are universal and which may be culture-specific. Next, we did not examine participants’ previous experience with dying or death, or whether they were currently suffering from illness. Prior exposure might impact EOL hopes and fears and individual levels of death anxiety. Because this was the first direct study of EOL possible selves among middle-aged and older adults, we also did not assess whether participants had completed advance directives, a common albeit insufficient indicator of EOL care quality. Similarly, we did not measure the extent to which participants had engaged in EOL discussions with health care providers, and if they did, whether discussion included their EOL hopes and fears. National trends suggest these clinical discussions are infrequent, limited in duration and quality, and occur late in illness trajectories (Crimmins et al., 2021). Future research should therefore directly measure the psychological content and impact of ACP discussion to differentiate met and unmet psychological needs of healthy adults.
Conclusion
In sum, the current study provides evidence that healthy adults are willing and able to articulate their views about death and dying in specific detail. While the end of life is psychologically sensitive, many people are not “in denial” and reflect on death well before it appears medically necessary. Optimal end-of-life communication therefore requires a proactive, biopsychosocial, person-centered approach to the living and dying process.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053221089726 – Supplemental material for Advance care planning: End-of-life hopes and fears among community dwelling adults
Supplemental material, sj-docx-1-hpq-10.1177_13591053221089726 for Advance care planning: End-of-life hopes and fears among community dwelling adults by Alissa Dark-Freudeman and Benjamin A Bensadon in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053221089726 – Supplemental material for Advance care planning: End-of-life hopes and fears among community dwelling adults
Supplemental material, sj-docx-2-hpq-10.1177_13591053221089726 for Advance care planning: End-of-life hopes and fears among community dwelling adults by Alissa Dark-Freudeman and Benjamin A Bensadon in Journal of Health Psychology
Supplemental Material
sj-docx-3-hpq-10.1177_13591053221089726 – Supplemental material for Advance care planning: End-of-life hopes and fears among community dwelling adults
Supplemental material, sj-docx-3-hpq-10.1177_13591053221089726 for Advance care planning: End-of-life hopes and fears among community dwelling adults by Alissa Dark-Freudeman and Benjamin A Bensadon in Journal of Health Psychology
Supplemental Material
sj-pdf-4-hpq-10.1177_13591053221089726 – Supplemental material for Advance care planning: End-of-life hopes and fears among community dwelling adults
Supplemental material, sj-pdf-4-hpq-10.1177_13591053221089726 for Advance care planning: End-of-life hopes and fears among community dwelling adults by Alissa Dark-Freudeman and Benjamin A Bensadon in Journal of Health Psychology
Supplemental Material
sj-sav-5-hpq-10.1177_13591053221089726 – Supplemental material for Advance care planning: End-of-life hopes and fears among community dwelling adults
Supplemental material, sj-sav-5-hpq-10.1177_13591053221089726 for Advance care planning: End-of-life hopes and fears among community dwelling adults by Alissa Dark-Freudeman and Benjamin A Bensadon in Journal of Health Psychology
Supplemental Material
sj-sav-6-hpq-10.1177_13591053221089726 – Supplemental material for Advance care planning: End-of-life hopes and fears among community dwelling adults
Supplemental material, sj-sav-6-hpq-10.1177_13591053221089726 for Advance care planning: End-of-life hopes and fears among community dwelling adults by Alissa Dark-Freudeman and Benjamin A Bensadon in Journal of Health Psychology
Supplemental Material
sj-spv-10-hpq-10.1177_13591053221089726 – Supplemental material for Advance care planning: End-of-life hopes and fears among community dwelling adults
Supplemental material, sj-spv-10-hpq-10.1177_13591053221089726 for Advance care planning: End-of-life hopes and fears among community dwelling adults by Alissa Dark-Freudeman and Benjamin A Bensadon in Journal of Health Psychology
Supplemental Material
sj-spv-7-hpq-10.1177_13591053221089726 – Supplemental material for Advance care planning: End-of-life hopes and fears among community dwelling adults
Supplemental material, sj-spv-7-hpq-10.1177_13591053221089726 for Advance care planning: End-of-life hopes and fears among community dwelling adults by Alissa Dark-Freudeman and Benjamin A Bensadon in Journal of Health Psychology
Supplemental Material
sj-spv-8-hpq-10.1177_13591053221089726 – Supplemental material for Advance care planning: End-of-life hopes and fears among community dwelling adults
Supplemental material, sj-spv-8-hpq-10.1177_13591053221089726 for Advance care planning: End-of-life hopes and fears among community dwelling adults by Alissa Dark-Freudeman and Benjamin A Bensadon in Journal of Health Psychology
Supplemental Material
sj-spv-9-hpq-10.1177_13591053221089726 – Supplemental material for Advance care planning: End-of-life hopes and fears among community dwelling adults
Supplemental material, sj-spv-9-hpq-10.1177_13591053221089726 for Advance care planning: End-of-life hopes and fears among community dwelling adults by Alissa Dark-Freudeman and Benjamin A Bensadon in Journal of Health Psychology
Supplemental Material
sj-txt-11-hpq-10.1177_13591053221089726 – Supplemental material for Advance care planning: End-of-life hopes and fears among community dwelling adults
Supplemental material, sj-txt-11-hpq-10.1177_13591053221089726 for Advance care planning: End-of-life hopes and fears among community dwelling adults by Alissa Dark-Freudeman and Benjamin A Bensadon in Journal of Health Psychology
Footnotes
Data sharing statement
The current article includes the complete raw dataset collected in the study including the participants’ data set, syntax file and log files for analysis. These files are all available in the Figshare repository and as Supplemental Material on the SAGE Journals platform.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.