
Abstract
Using cross-sectional data from two samples of adult patients with type 2 diabetes (n = 123 and n = 111), we used an embodiment perspective to examine whether health experiences were related to the extent of individuals’ dissatisfaction with their bodies. The nature and strength of associations differed across the two unique samples examined, but weight status had the strongest and most robust association with body dissatisfaction in both samples. None of the associations differed as a function of gender or age. These findings contribute to an understanding of the complex relationship between physical and mental health in the context of diabetes.
Approximately 422 million adults globally have diabetes, 90% of which have type 2 diabetes, with prevalence rates continuing to increase worldwide (World Health Organization [WHO], n.d.). Body dissatisfaction is likewise common among adults; estimates indicate that up to 90% of women and 61% of men are dissatisfied with their bodies (Fiske et al., 2014; Gillen et al., 2018). These two common experiences in adulthood may be related, such that body dissatisfaction is high among patients with diabetes (e.g., Toselli et al., 2019), and could be one reason for the greater prevalence of mental health issues in this population. Although elevated weight status has been proposed as an explanation for why patients with diabetes are at an increased risk for body dissatisfaction (Gonzalez et al., 2011), a growing body of evidence suggests that body image is not only related to how one looks, but also to how one feels and their body’s overall functionality (Alleva and Tylka, 2021).
Using two distinct samples of patients with type 2 diabetes, the current study accordingly sought to understand whether three different health experiences—number of comorbid health conditions, functional limitations, and self-rated health—accounted for variability in body dissatisfaction. Given the robust association between weight status and body dissatisfaction (de Souto Barreto et al., 2011; Fallon et al., 2014; Toselli et al., 2019; Weinberger et al., 2016), we also sought to examine whether these associations still held after controlling for participants’ weight status.
We used an embodiment perspective to understand these potential associations, which has been applied to both health-related experiences that affect the aging body (Hurd Clarke and Korotchenko, 2011) and body image more generally (Piran, 2017). Embodiment refers to the “lived-in experiences of the body and how it engages with the world” (Alleva and Tylka, 2021: 150). When individuals experience an illness or limitations to their health, it disrupts their typical way of thinking about their body that is “phenomenologically absent from view” (p. 25), and instead, brings it to the forefront of their awareness (Williams, 1996). This awareness of the body as problematic and a source of discomfort can lead to body dissatisfaction (Piran, 2017).
Body image in the context of diabetes
Individuals with type 2 diabetes tend to be of elevated weight status (National Institute of Diabetes and Digestive and Kidney Diseases [NIDDK], n.d.), which is a common explanation for why individuals experience dissatisfaction with their bodies (e.g., Fallon et al., 2014; Weinberger et al., 2016). Experiencing body dissatisfaction is of particular concern for this population because it can be predictive of poor mental health (e.g., disordered eating behaviors (Bucchianeri and Neumark-Sztainer, 2014)) and metabolic control (Troncone et al., 2021), both of which have implications for adverse diabetes-related outcomes. Most of the research dedicated to examining body image and diabetes has focused on adolescents diagnosed with type 1 diabetes, given that adolescence and young adulthood are considered risk periods for the development of eating disorders (Winston, 2020).
Much less research has been conducted on body image among patients with type 2 diabetes, despite the condition being more prevalent during a time in the lifespan in which body and health-related changes occur that may impact individuals’ views of their body (Hurd Clarke and Korotchenko, 2011). In an early study on this topic, researchers found that women with type 2 diabetes were more likely to report body dissatisfaction than matched counterparts without a chronic condition (Anderson et al., 1997). In another qualitative study, Oftedal et al. (2010) interviewed adults living with diabetes to better understand common life values among this population and how those values might impact their self-management behaviors. Researchers identified preserving a positive body image as one of the six most common values that individuals with diabetes see as important in guiding their behaviors. Other research suggests that body dissatisfaction may lead to negative outcomes, such as poor psychosocial outcomes and worse metabolic control (McDonald et al., 2021; Troncone et al., 2021).
Given the potential impact of body dissatisfaction on diabetes outcomes, efforts to understand factors that contribute to poor body image among individuals with type 2 diabetes warrant attention. Other than weight status, variability in rates of body dissatisfaction among patients with type 2 diabetes could be partially explained by other health-related experiences that affect their “lived in” bodily experiences (Piran, 2017).
Health experiences and body image
Some evidence suggests that having more than one condition puts individuals at risk for poor body image (Hurd Clarke et al., 2008). For example, one study found that women with endometriosis and additional chronic illness reported more body dissatisfaction than peers without a chronic illness diagnosis (Geller et al., 2021). Although this idea has not been empirically tested in the context of diabetes, other studies of patients with diabetes suggest that having multiple chronic conditions is an important factor in understanding these patients’ psychological experiences (Byles et al., 2014). For instance, in a study that examined the link between diabetes and depression, researchers found that diabetes and depression were no longer significantly related when multimorbidities were added to the model (Ogunleye et al., 2015). If, according to the embodiment framework, health-related experiences affect views of one’s body, it is possible then that the more illness-related experiences (i.e. comorbidities) an individual has, the greater the potential implications for body image.
Although the simple presence of one or more chronic conditions may put individuals at risk for body dissatisfaction, the extent to which functioning is impaired from these conditions also may be important to consider in understanding body dissatisfaction. Changes in body function, like those associated with chronic conditions or aging, can negatively influence body appraisal (Thomas et al., 2019). It has been suggested that such functional limitations may lead to body dissatisfaction because they can hinder valued physical activity (Hurd Clarke et al., 2008) and are inconsistent with societal views of bodies that are physically fit, attractive, or “normal” (Alleva and Tylka, 2021; Markey et al., 2020). This objective experience of loss in functionality that can accompany chronic conditions may affect individuals’ views of, or satisfaction with, their body (Alleva and Tylka, 2021).
Some evidence suggests that experiencing these functional limitations makes appearance-related body satisfaction less salient in later life as there is a shift in focus from how the body looks to how the body functions (Hurd Clarke and Korotchenko, 2011; Tiggemann, 2004). Yet, individuals still remain dissatisfied with their appearance even into late life (Hurd Clarke et al., 2008). Thus, more needs to be understood about the connection between objective limitations to functioning and individuals’ views of their bodies.
Although these more objective health experiences may affect individuals’ thinking about their bodies, their overall assessment of their health also may be relevant to understanding body image perceptions. One such measure, “age-comparative” self-rated health, is subjective and comparative, asking participants to rate their health in comparison to same-aged peers (Jylhä, 2009). Self-rated health reliably predicts health outcomes, including functional decline (Lee, 2000), poorer metabolic control among adults with diabetes (Undén et al., 2008), and even mortality (Jylhä, 2009).
A fair amount of research suggests that body dissatisfaction and weight concerns are related to lower self-rated health (e.g. de Oliveira da Silva et al., 2018; McLaren and Kuh, 2004; Meland et al., 2021), but most of these studies have examined how these weight concerns or body dissatisfaction might predict self-rated health rather than vice versa. It is likely, however, that there is a cyclical relationship between the two constructs. Consistent with understanding health as an embodied experience, in this study, we examined how the extent to which individuals comparatively viewed their health may be related to their view of their body.
The current study
We used an embodiment perspective to understand how different health experiences in the context of type 2 diabetes were related to body dissatisfaction. Our first aim (Aim 1) was to examine whether number of comorbid health conditions, functional limitations, and self-rated health were related to the extent that individuals were dissatisfied with their bodies. We predicted that all measures would be associated with body dissatisfaction to some extent; specifically, having more comorbid health conditions and functional limitations would be related to greater body dissatisfaction and perceiving one’s health as better than one’s peers would be related to less body dissatisfaction. Our second aim (Aim 2) was to determine the health experience that had the strongest association with body dissatisfaction, while controlling for the other experiences (i.e., unique associations between each measure of health and body dissatisfaction). This aim was not pre-registered and is thus exploratory. Our third aim (Aim 3) was to examine whether these associations still held after controlling for participants’ weight status (BMI). This aim also was not pre-registered and is thus exploratory.
Method
Participants and procedure
Data from two studies were used to address hypotheses: “Study 1” and “Study 2.” Both studies included samples of adults with type 2 diabetes and were approved by the Institutional Review Board at Rutgers University.] Our key study aim was preregistered through the Open Science Framework (OSF). This anonymous pre-registration can be viewed at: https://osf.io/6pcwz/?view_only=6451a2c51e044d06ab9d790a060ed0d8
Participant characteristics for each study are provided in Table 1. The samples differed significantly on all variables reported except marital status, such that compared to participants in Study 2, those in Study 1 were significantly more likely to be male, White, and have an education greater than a high school degree, and also were significantly younger and had diabetes for less time.
Participant characteristics by study.
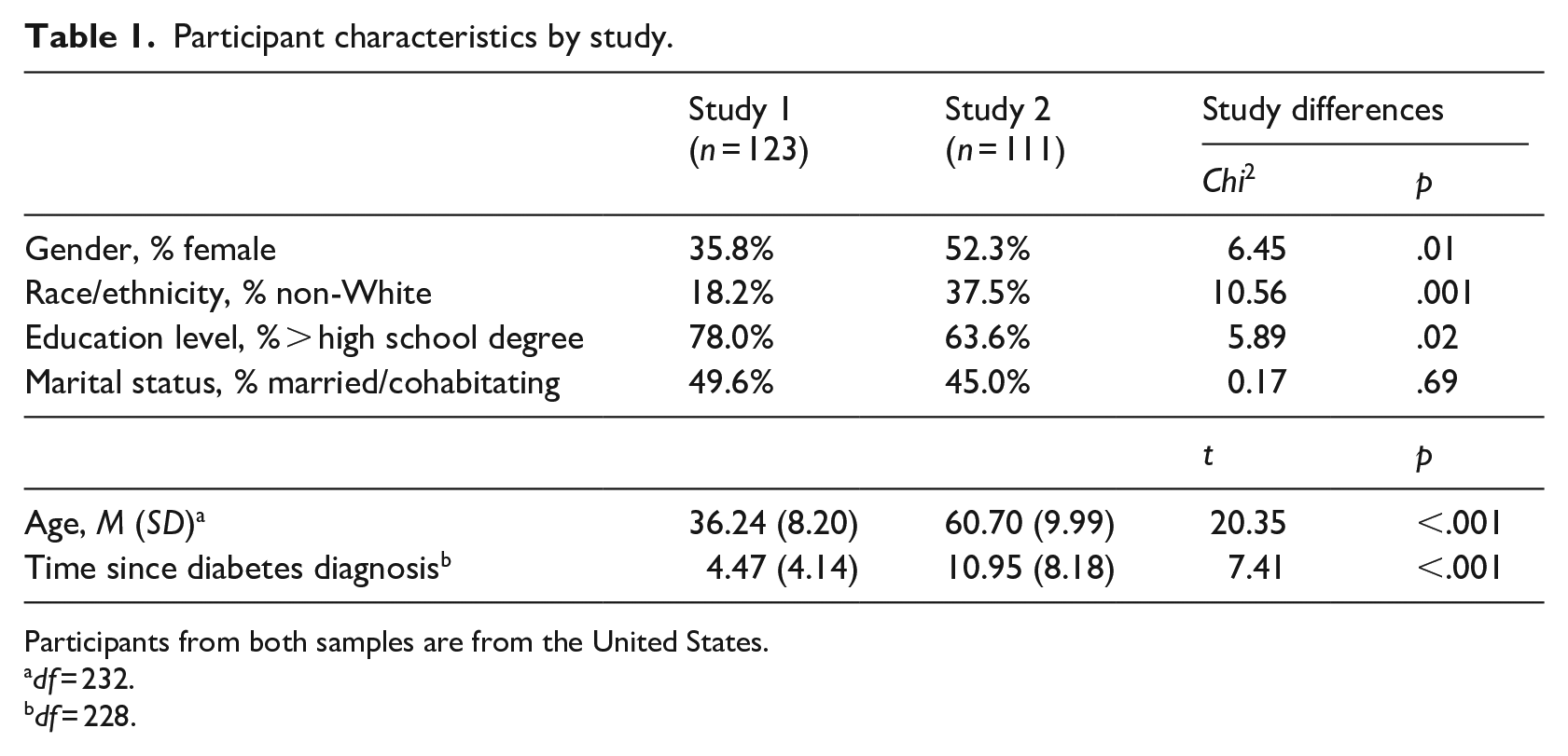
Participants from both samples are from the United States.
df = 232.
df = 228.
Study 1
Data for this study were collected as part of a larger study examining links between general health, chronic illness, and body image. Adults with chronic illnesses were recruited using social media, web pages relevant to people with such illnesses (e.g., support groups), and Amazon MTurk. Eligibility criteria included diagnosis with a chronic illness or chronic pain condition, including but not limited to diabetes, being 18 years or older, and being fluent in English. Approximately half of the participants were recruited using MTurk and approximately half were recruited from other online sources (all of the participants used in the current study were from the MTurk sample).
The initial sample included 461 individuals who provided consent and participated in the survey. Individuals were excluded from analyses if they had a condition other than type 2 diabetes (n = 312) or did not have complete data on the body image measures (n = 26); those without body image data were significantly older, had more comorbid health conditions, were more likely to be female, and were more likely to have greater than a high school degree than those with complete body image data. The final analytic sample for Study 1 included 123 individuals 22–66 years old.
Participants provided online consent and then completed a self-administered questionnaire via Qualtrics, which took approximately 15 minutes, on average, to complete. Amazon MTurk participants were compensated with the current standard rate for MTurk participants; other participants were entered into a drawing to win a $100 gift card.
Study 2
Data for this study were collected as part of a larger study examining diabetes-related experiences in mid to late life. Individuals with type 2 diabetes residing in the greater Philadelphia area were recruited via local businesses, health care provider offices, online, and through attendance at local community events. Eligibility criteria included being 45–85 years old; seeing a diabetes healthcare provider at least once per year; being fluent in English; and being free of any significant cognitive impairment. The initial sample included 119 individuals who provided consent and participated in the survey. Individuals were excluded from analyses if they did not have complete data on the body image measures (n = 8); the final analytic sample for Study 2 included 111 individuals 44–83 years old.
Participants provided written consent and then completed two self-administered questionnaires and participated in a structured interview with a research assistant, which took approximately 2 hours total. Participants were compensated $20 and entered into a drawing to win an additional $100.
Measures
Comorbid health conditions
In Study 1, number of comorbid health conditions was assessed by counting the number of chronic conditions participants indicated in response to the open-ended question, “Have you been diagnosed with any other medical conditions (other than diabetes) that affect your health in any way currently?”
In Study 2, number of comorbid health conditions was assessed by counting the number of affirmative responses to 13 possible conditions common in later life (e.g., hypertension, arthritis; National Council on Aging, 2021).
Functional limitations
In Study 1, nine items were adapted from the widely used SF-36 to assess functional limitations (Hays et al., 1993). Participants rated on a three-point scale (1 = “not limited at all” to 3 = “yes, limited a lot”) the extent of difficulty in completing activities related to upper extremity strength (e.g., “lifting or carrying groceries”) and mobility (e.g., “walking one block”). The items were averaged to create a composite measure of functional limitations (α = .93).
In Study 2, six items were adapted from Katz et al. (1963) and Lawton and Brody (1969) to assess functional limitations. Participants rated on a five-point scale (1 = “can’t do at all,” to 5 = “very difficult”) the extent of difficulty in completing activities related to upper extremity strength (e.g., “lift or carry something as heavy as 15 pounds, such as a full bag of groceries”) and mobility (e.g., “walk a quarter of a mile”). The items were averaged to create a composite measure of functional limitations (α = .87). These items have been used successfully in other studies of older adults (e.g., August et al., 2007).
Self-rated health
In both studies, self-rated health compared to same-age peers (i.e., “age-comparative” self-rated health) was assessed with one item. Participants were asked to rate their health on a five-point scale, “Compared to most people your age, would you say your health is ...” (1 = “much worse than people your age” to 5 = “much better than people your age”). This measure has been shown to be a robust predictor of morbidity and mortality (Jylhä, 2009) and allows for age-appropriate comparisons.
Body mass index
In both studies, body mass index (BMI) was assessed using participants’ self-reported height and weight.
Body dissatisfaction
In both studies, body dissatisfaction was assessed using the Contour Drawing Rating Scale (CDRS; Thompson and Gray, 1995). Participants were asked to select 1 of 9 gender-specific figures (1 = very underweight, 9 = very overweight) that represented what they thought they currently looked like (i.e., current body) and what they would like to look like (i.e., ideal body). From these items, a body dissatisfaction score was calculated by subtracting scores on “current body” from scores on “ideal body.” Absolute values of these scores were used so that a score of 0 indicates satisfaction and a score > 0 indicates some level of dissatisfaction. The test-retest reliability for this measure has been reported to be good (.79; Thompson and Gray, 1995), and this measure has been found to be associated with weight status and dieting behaviors in other adult samples (e.g., Markey and Markey, 2005).
Covariates
We considered covariates that have been reported in the literature to be relevant to body dissatisfaction and diabetes, including gender, age, race/ethnicity (dichotomized into White vs non-White), and time since diabetes diagnosis. Variables that had significant bivariate associations with body dissatisfaction were included in analyses; only gender and age met this criterion and were thus included in analyses.
Analytic plan
SPSS version 28 was used for descriptive analyses and to test study aims. Prior to analyses, data were checked for completeness. Other than missing data on body image, there were 0–1.6% missing data in Study 1 and 0–6.3% missing data in Study 2. Given the small amount of missing data, listwise deletion was used (Graham, 2009). All regression assumptions were met in both data sets.
To test study aims, a series of linear multivariable regression analyses were performed to examine how health experiences were related to body dissatisfaction in each study sample. Each measure was examined in separate models (Aim 1), in models that controlled for the other health experiences (Aim 2), and in models that also controlled for BMI (Aim 3). In addition to model effect size (adjusted R2), partial correlations (pr) were calculated for each health experience when examined in models together to determine the variable-specific effect size.
In posthoc analyses, gender and age were examined as moderators of the associations between health experiences and body dissatisfaction by creating interactions between each (centered) health experience with gender or (centered) age and adding them to each of the above models. The nature of the one significant interaction identified was determined by calculating simple slopes for each gender and at ±1 SD of the mean of functional limitations.
Results
Descriptive results
Table 2 shows the means, standard deviations, and intercorrelations among key study variables, as well as sample differences in key variables. Compared to participants in Study 2, those in Study 1 reported significantly less comorbid health conditions and worse self-rated health.
Means, standard deviations, and intercorrelations among key study variables.
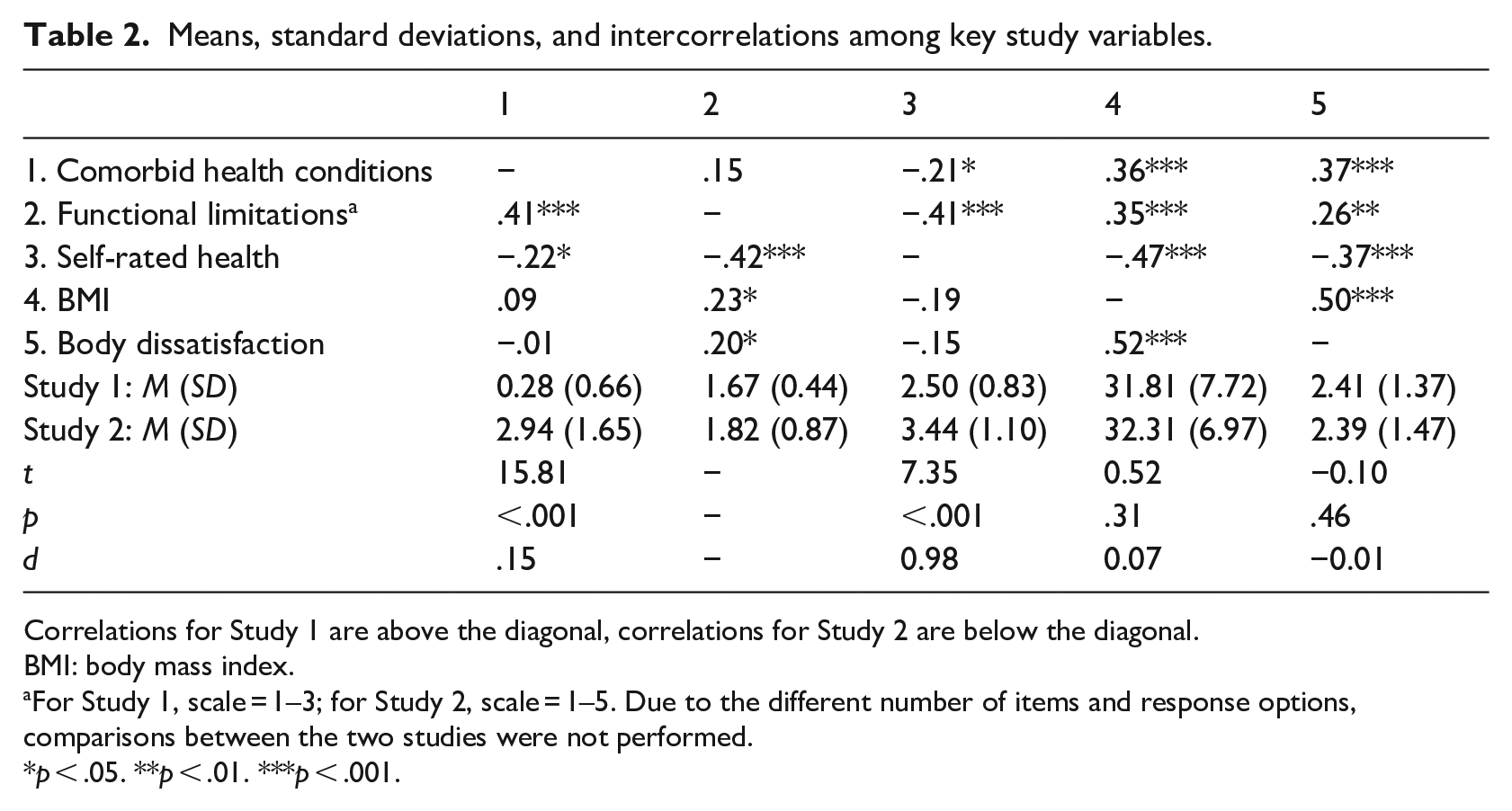
Correlations for Study 1 are above the diagonal, correlations for Study 2 are below the diagonal.
BMI: body mass index.
For Study 1, scale = 1–3; for Study 2, scale = 1–5. Due to the different number of items and response options, comparisons between the two studies were not performed.
In both Study 1 and 2, there were significant associations between most of the health experiences. In addition, all health experiences were significantly associated with body dissatisfaction in Study 1, whereas only functional limitations and BMI were significantly associated with body dissatisfaction in Study 2.
Hypotheses tests
Table 3 shows the results of regression analyses that examined associations between each health experience and body dissatisfaction (Aim 1; top half) and unique associations between each health experience and body dissatisfaction after controlling for the other health experiences (Aim 2; bottom half). For Study 1, all three health experiences were significantly associated with body dissatisfaction; specifically, individuals who had greater comorbid health conditions and functional limitations also reported significantly greater body dissatisfaction, whereas individuals who self-rated their health as better than their peers also reported significantly less body dissatisfaction. For Study 2, only functional limitations was significantly associated with body dissatisfaction, such that individuals who had greater functional limitations also reported significantly greater body dissatisfaction.
Regression analyses examining the associations between health experiences and body dissatisfaction.
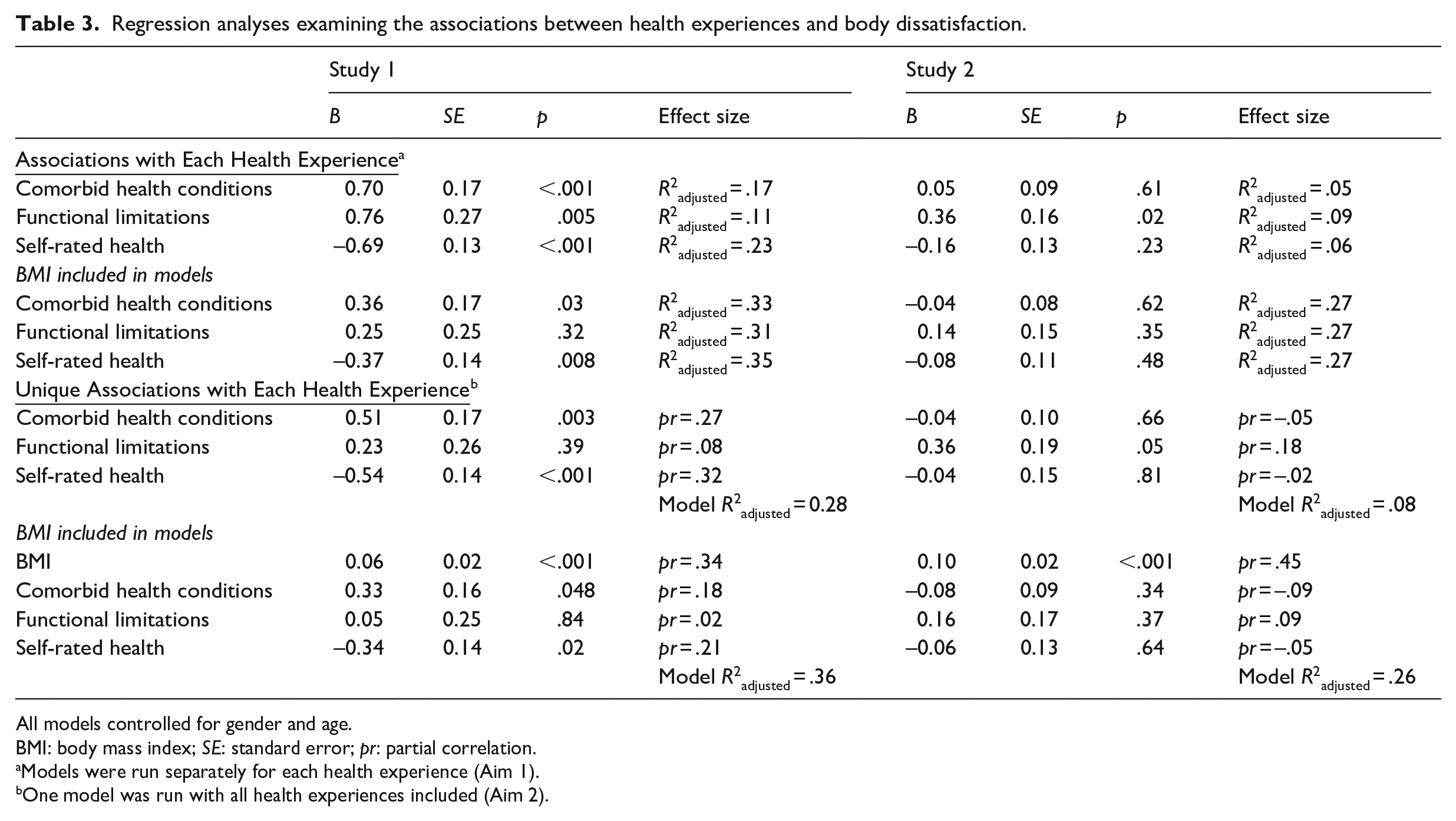
All models controlled for gender and age.
BMI: body mass index; SE: standard error; pr: partial correlation.
Models were run separately for each health experience (Aim 1).
One model was run with all health experiences included (Aim 2).
In analyses that examined associations between health experiences and body dissatisfaction when controlling for the other health experiences, results revealed that only comorbid health conditions and self-rated health remained significantly associated with body dissatisfaction in Study 1. For Study 2, functional limitations became marginally associated with body dissatisfaction.
Finally, results from analyses that examined the above associations when controlling for BMI (Aim 3) are presented in Table 3 below results for Aims 1 and 2, respectively. For Study 1, comorbid health conditions and self-rated health remained significantly associated with body dissatisfaction; BMI also was significantly (and positively) associated with body dissatisfaction. For Study 2, BMI was the only significant predictor of body dissatisfaction.
Posthoc analyses
Given previous work suggesting that gender and age may be important to consider in understanding diabetes experiences (e.g., Siddiqui et al., 2013) and body image (e.g., Fallon et al., 2014; Gillen and Markey, 2015; Quittkat et al., 2019), we undertook additional posthoc analyses that examined gender and age as possible moderators of the associations between health experiences and body dissatisfaction. These analyses were exploratory due to limits to statistical power to detect interactions. Only one significant interaction emerged between functional limitations and gender in predicting dissatisfaction in Study 1—but only when all health experiences (including BMI) were in the model together. Simple slopes were not significant for either gender, however. No significant interactions emerged in any of the other models in Study 1 and between any of the health experiences and either gender or age in predicting body dissatisfaction in Study 2.
Discussion
Given the prevalence of both type 2 diabetes (WHO) and body dissatisfaction (Fallon et al., 2014; Gillen et al., 2018) among adults, efforts to understand experiences related to these commonly co-occurring issues are important for intervention efforts. Through the lens of the embodiment perspective, we found that although health experiences in the context of diabetes were related to body dissatisfaction, the nature and strength of these associations differed across the two unique samples examined, potentially due to differences in the composition of the samples (e.g., age, gender). Our findings also revealed that weight status was the strongest and most consistent predictor of body dissatisfaction in both samples.
We found that individuals who reported more functional limitations had greater body dissatisfaction in both studies when other health experiences were not considered; this health experience remained significant and (other than BMI) had the strongest association with body dissatisfaction in Study 2, whereas it become nonsignificant when other health experiences were taken into account in Study 1. This finding is consistent with other research that has found that functional limitations are important in understanding body dissatisfaction, particularly among older adults (de Souto Barreto et al., 2011; Hurd Clarke et al., 2008). Researchers have suggested that limits to strength and mobility are responsible for the decrease in body satisfaction as they hinder physical activity (de Souto Barreto et al., 2011), which has been identified as an important predictor of body image (Hausenblas and Fallon, 2006). A possible reason functional limitations had a stronger and more robust association with body dissatisfaction in Study 2 than in Study 1 could be a function of the age of the samples. Body image may take on a different meaning as individuals age, in that satisfaction with the functional aspects of the body take priority over satisfaction with appearance (Roy and Payette, 2012; Tiggemann, 2004). In later life, the body as a “tool for action” is emphasized and limits to functionality conflict with societal standards for successful aging (Hurd Clarke et al., 2008).
Other health experiences—namely, number of comorbid conditions and self-rated health—appeared to be more important than functional limitations in Study 1 compared to Study 2, and even remained significantly associated with body dissatisfaction after taking into account participants’ weight status. Given that individuals in this sample were young adults, on average, having more than one health condition is rarer (Boersma et al., 2020) and may be considered an “off-time” developmental experience, which tends to have adverse effects (Neugarten, 1976), including diminished self-worth (Boerner and Wang, 2010). Interpreting this in the context of the embodiment framework, experiencing comorbid health conditions at a younger age may be a “biographical disruption” (Bury, 1982) that manifests in dissatisfaction with one’s body. We did not find evidence that having multiple chronic conditions was associated with body image dissatisfaction in Study 2, however. At least one other study of older adults (Rakhkovskaya and Holland, 2017) also did not find this association. Other aspects of multimorbidities that might be more disruptive to individuals’ views of their body in later life (e.g., illness severity, burden, influence on appearance), therefore could be more important for older adults’ body image (Hurd Clarke et al., 2008; Rakhkovskaya and Holland, 2017).
In line with past work (e.g., de Oliveira da Silva et al., 2018), we also found that when participants in Study 1 perceived their overall health as worse than their peers, they experienced greater body dissatisfaction. As both self-rated health and body image involve individuals’ own perceptions of their health and well-being (Jylhä, 2009; Roy and Payette, 2012), this finding is not entirely surprising. Although having a poor view of one’s health could contribute to a more negative view of one’s body, it is just as likely that body dissatisfaction contributes to a negative evaluation of health. It is unclear why this same association was not found among participants in Study 2, although other studies have likewise failed to find this association (e.g., Sand et al., 2017). It could be that self-rated health is more likely to be associated with a different measure of body dissatisfaction (e.g., functioning), especially in later life. It is also possible that cultural context plays a role in these findings, as much of the literature on this topic has been conducted in different countries with conflicting results (e.g., de Oliveira da Silva et al., 2018; Sand et al., 2017). More research is needed to establish the validity of these conjectures.
Consistent with the extant literature (e.g., de Souto Barreto et al., 2011; Fallon et al., 2014; Toselli et al., 2019; Weinberger et al., 2016), weight status was the strongest and most robust predictor of body dissatisfaction in both samples. Researchers have reasoned that the way individuals of higher weight status view their bodies is adversely affected by social experiences, including sociocultural norms that value thinness and feeling stigmatized by others (Wu and Berry, 2018). Despite having serious (or numerous) health issues, weight may still play a central role in how individuals view their bodies, even in later life (Hurd Clarke et al., 2008). As individuals with type 2 diabetes tend to be of higher weight status (NIDDK), the implications of this link are particularly relevant for patients with type 2 diabetes. Individuals with both diabetes and those with body image concerns are at high risk for depression and other mental health issues (Darwish et al., 2018; Silva et al., 2019); provider discussions about behavioral health are therefore essential in this population.
Although weight loss has been found to be associated with better diabetes control and outcomes (ADA, 2020), providers need to be careful about stigmatizing patients of higher weight status, which can contribute to further health issues (Tomiyama et al., 2016). Providers thus should focus on empowering their patients to engage in health-enhancing behaviors such as eating nutrient dense foods and engaging in regular exercise to promote better health more broadly (versus a focus on weight control), with a consideration of patients’ motivation, health beliefs, and life circumstances (Zare et al., 2020). Moreover, consistent with recommendations by other researchers (e.g., Rakhkovskaya and Holland, 2017), providers may want to utilize screening tools to assess patients’ body image concerns—in addition to (or instead of) measuring weight.
Although age and gender have been identified as important in understanding health experiences and body satisfaction (e.g., Quittkat et al., 2019; Siddiqui et al., 2013), these factors did not significantly moderate the links between health experiences and body dissatisfaction in either sample. Given the relatively modest sample sizes, it is possible that there was simply not enough statistical power to detect moderating effects. Age and gender nonetheless could be responsible for differences in the results seen across the two studies, given the significant differences in age and gender composition—that is, Study 1 was comprised of majority male, young to middle-aged adults, whereas Study 2 was comprised of majority female middle-aged to older adults. Although there were other significant differences in the sample composition of the two studies, there was no significant difference between the two studies in weight status or overall body dissatisfaction, as participants in both studies had a relatively high weight status (mean BMI > 30) and were generally dissatisfied with their bodies.
Limitations and future directions
The results of the current study should be interpreted in the context of its limitations. The data were cross-sectional, so the direction of effects could not be determined; the associations are likely bidirectional. In addition, the sample sizes for each sample were relatively modest, raising concerns about statistical power. Further, the samples were not very racially/ethnically or socioeconomically diverse and participants who had complete body image data were significantly different in some ways than those who did not, reducing the generalizability of the findings. The use of two samples, however, helps improve generalizability and suggests that sociodemographic characteristics may be important to consider in future research on understanding correlates of body image in the context of type 2 diabetes.
Another limitation was that the body image assessment used in both studies focused on satisfaction with body size (versus other aspects of body image, such as body functioning). Some studies have found distinguishing between these assessments to be important in later life (Reboussin et al., 2000), whereas other studies have found a significant link between satisfaction with body functioning and appearance (de Souto Barreto et al., 2011). Although we still found aspects of physical health that were related to this measure in our sample, future research should incorporate more multidimensional assessments of body image. In addition, two of the measures used—comorbid health conditions and functional limitations—were not assessed exactly the same way in both studies, potentially leading to differences in results.
Finally, although BMI was used in the current study for time and cost-related reasons, some researchers have criticized its utility, as it does not take into account the distribution of fat, discriminate between fat and lean body mass, consider racial/ethnic differences in body composition, and is not always reliably linked to health outcomes (Rothman, 2008; Tomiyama et al., 2016). The American Diabetes Association nonetheless still recommends that providers calculate patients’ BMI (ADA, 2020), and findings from our study and others suggest that BMI is an important correlate of individuals’ body image.
Conclusion
Despite these limitations, this study contributes to a greater understanding of the association between health experiences and body image among individuals with type 2 diabetes through the lens of embodiment. The findings suggest that different physical health experiences may have consequences for patients’ view of their bodies, but, with the exception of weight status, what those specific experiences are vary for diverse populations of patients with type 2 diabetes. These findings underscore the complex interplay between physical and mental health issues in the context of diabetes, as well as the importance of providers identifying and treating mental health concerns alongside physical health ones.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053221091610 – Supplemental material for Examining health experiences and body dissatisfaction in two unique samples of patients with type 2 diabetes
Supplemental material, sj-docx-1-hpq-10.1177_13591053221091610 for Examining health experiences and body dissatisfaction in two unique samples of patients with type 2 diabetes by Kristin J August, Maggie R Albright-Pierce and Charlotte H Markey in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053221091610 – Supplemental material for Examining health experiences and body dissatisfaction in two unique samples of patients with type 2 diabetes
Supplemental material, sj-docx-2-hpq-10.1177_13591053221091610 for Examining health experiences and body dissatisfaction in two unique samples of patients with type 2 diabetes by Kristin J August, Maggie R Albright-Pierce and Charlotte H Markey in Journal of Health Psychology
Supplemental Material
sj-docx-3-hpq-10.1177_13591053221091610 – Supplemental material for Examining health experiences and body dissatisfaction in two unique samples of patients with type 2 diabetes
Supplemental material, sj-docx-3-hpq-10.1177_13591053221091610 for Examining health experiences and body dissatisfaction in two unique samples of patients with type 2 diabetes by Kristin J August, Maggie R Albright-Pierce and Charlotte H Markey in Journal of Health Psychology
Research Data
sj-sav-4-hpq-10.1177_13591053221091610 – for Examining health experiences and body dissatisfaction in two unique samples of patients with type 2 diabetes
sj-sav-4-hpq-10.1177_13591053221091610 for Examining health experiences and body dissatisfaction in two unique samples of patients with type 2 diabetes by Kristin J August, Maggie R Albright-Pierce and Charlotte H Markey in Journal of Health Psychology
Research Data
sj-sav-5-hpq-10.1177_13591053221091610 – for Examining health experiences and body dissatisfaction in two unique samples of patients with type 2 diabetes
sj-sav-5-hpq-10.1177_13591053221091610 for Examining health experiences and body dissatisfaction in two unique samples of patients with type 2 diabetes by Kristin J August, Maggie R Albright-Pierce and Charlotte H Markey in Journal of Health Psychology
Supplemental Material
sj-sps-6-hpq-10.1177_13591053221091610 – Supplemental material for Examining health experiences and body dissatisfaction in two unique samples of patients with type 2 diabetes
Supplemental material, sj-sps-6-hpq-10.1177_13591053221091610 for Examining health experiences and body dissatisfaction in two unique samples of patients with type 2 diabetes by Kristin J August, Maggie R Albright-Pierce and Charlotte H Markey in Journal of Health Psychology
Supplemental Material
sj-sps-7-hpq-10.1177_13591053221091610 – Supplemental material for Examining health experiences and body dissatisfaction in two unique samples of patients with type 2 diabetes
Supplemental material, sj-sps-7-hpq-10.1177_13591053221091610 for Examining health experiences and body dissatisfaction in two unique samples of patients with type 2 diabetes by Kristin J August, Maggie R Albright-Pierce and Charlotte H Markey in Journal of Health Psychology
Footnotes
Data sharing statement
The current article is accompanied by the relevant raw data generated during and/or analysed during the study, including files detailing the analyses and either the complete database or other relevant raw data. These files are available in the Figshare repository and accessible as Supplemental Material via the SAGE Journals platform. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Rutgers University NSF RU Fair grant (first author) and a Rutgers University Research Council grant (third author).
Ethics approval
This study was approved by the Institutional Review Board at Rutgers University (E17-351 and 13-425Mx).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.