
Abstract
COVID-19 conspiracy beliefs have a powerful detrimental influence on COVID-19 vaccine perceptions and behaviors. We investigate an expanded range of outcomes for COVID-19 conspiracy beliefs, and we test which vaccine hesitancy dimensions mediate these relations. Our results show that COVID-19 conspiracy beliefs relate to COVID-19 vaccination willingness and receipt, flu vaccination willingness and receipt, as well as vaccine word-of-mouth. Many of these relations are mediated by vaccine hesitancy dimensions that represent perceptions that vaccines pose health risks as well as perceptions that vaccines are not needed because the respondent is healthy. Our discussion identifies directions for future research.
Keywords
The decision to become vaccinated has been propelled to the forefront of academic and popular discourse since the widespread availability of COVID-19 vaccines, as many people have refused to receive these vaccines despite their significant benefits and modest risks (Knoll and Wonodi, 2021). While several causes have been proposed for vaccine refusal, COVID-19 conspiracy beliefs have been initially supported as a primary influence (Bertin et al., 2020). Conspiracy beliefs are based on misinformation (often shared via social media) that involve a “vast, insidious, preternaturally effective international conspiratorial network designed to perpetrate acts of most fiendish character” (Hofstadter, 1966, p. 14), and COVID-19 vaccines have been a recent target for the proliferation of conspiracy beliefs. An abundance of conjecture has been created to suggest that these vaccines serve the nefarious purposes of powerful people and cabals, including that COVID-19 was created by Bill Gates, COVID-19 vaccines contain microchips, and COVID-19 vaccines are used for population control (Georgiou et al., 2020).
Initial links have been supported between COVID-19 conspiracy beliefs and COVID-19 vaccination willingness and receipt (Georgiou et al., 2020; Hughes and Machan, 2021; Jovančević and Milićević, 2020), and authors have begun to study broader outcomes of these beliefs (Alper et al., 2021; Leibovitz et al., 2021). van Prooijen et al. (2021), for example, empirically supported that COVID-19 conspiracy beliefs relate to an increased likelihood of testing positive for COVID-19 and violating COVID-19 regulations as well as a decreased likelihood of COVID-19 testing and worse overall well-being. Such findings suggest that COVID-19 conspiracy beliefs relate to a broader range of detrimental outcomes than presently tested, such as refusing other vaccines or sharing vaccine information (i.e., word-of-mouth). The former of these outcomes, refusing other vaccines, may prove to be particularly impactful, as it would indicate that COVID-19 conspiracy theories detrimentally influence virus protection even beyond COVID-19.
Further, vaccine hesitancy is “the specific situation of having concerns about vaccines” (Dudley et al., 2020, p. 711), and its importance for vaccination behaviors was well known even before the COVID-19 pandemic (Dubé et al., 2013; MacDonald, 2015). Researchers supported that vaccine hesitancy is an immediate antecedent to vaccination behaviors for a host of vaccines (e.g., MMR vaccine, HPV vaccine), and many antecedents indirectly influence vaccine receipt via vaccine hesitancy (Luz et al., 2019; Sadaf et al., 2013). For this reason, vaccine hesitancy has been suggested to mediate the relations of COVID-19 conspiracy beliefs and outcomes (Allington et al., 2021; Georgiou et al., 2020). Also, while authors differ on the number and nature of dimensions, vaccine hesitancy is multidimensional (Howard, 2021; Shapiro et al., 2018). Certain dimensions but not others may mediate the relations of antecedents and vaccination outcomes, as for example, people may refrain from vaccination due to safety concerns but not due to financial costs. Therefore, considering vaccine hesitancy to be a unidimensional construct, as done in some prior research, limits our understanding of vaccination decision making, and it is necessary to utilize a multidimensional perspective of vaccine hesitancy to understand the relations of COVID-19 conspiracy beliefs and vaccination outcomes.
In the current article, we test not only whether COVID-19 conspiracy beliefs impact COVID-19 vaccination willingness and receipt, but we also test whether COVID-19 conspiracy beliefs impact flu vaccination willingness, flu vaccination receipt, and vaccination word-of-mouth. We chose to study flu vaccination due to its similarity to COVID-19 vaccination; adults must decide annually whether to receive it for themselves, as opposed to other vaccines that are received by youths and/or in specific circumstances (e.g., international travel). Researchers can better understand whether COVID-19 conspiracy beliefs impact broader outcomes than presently known by studying flu vaccination (as extant investigations have largely focused on COVID-19 vaccine receipt), and supporting the generalization of COVID-19 conspiracy beliefs to flu perceptions and behaviors could encourage investigations into more distal types of vaccines.
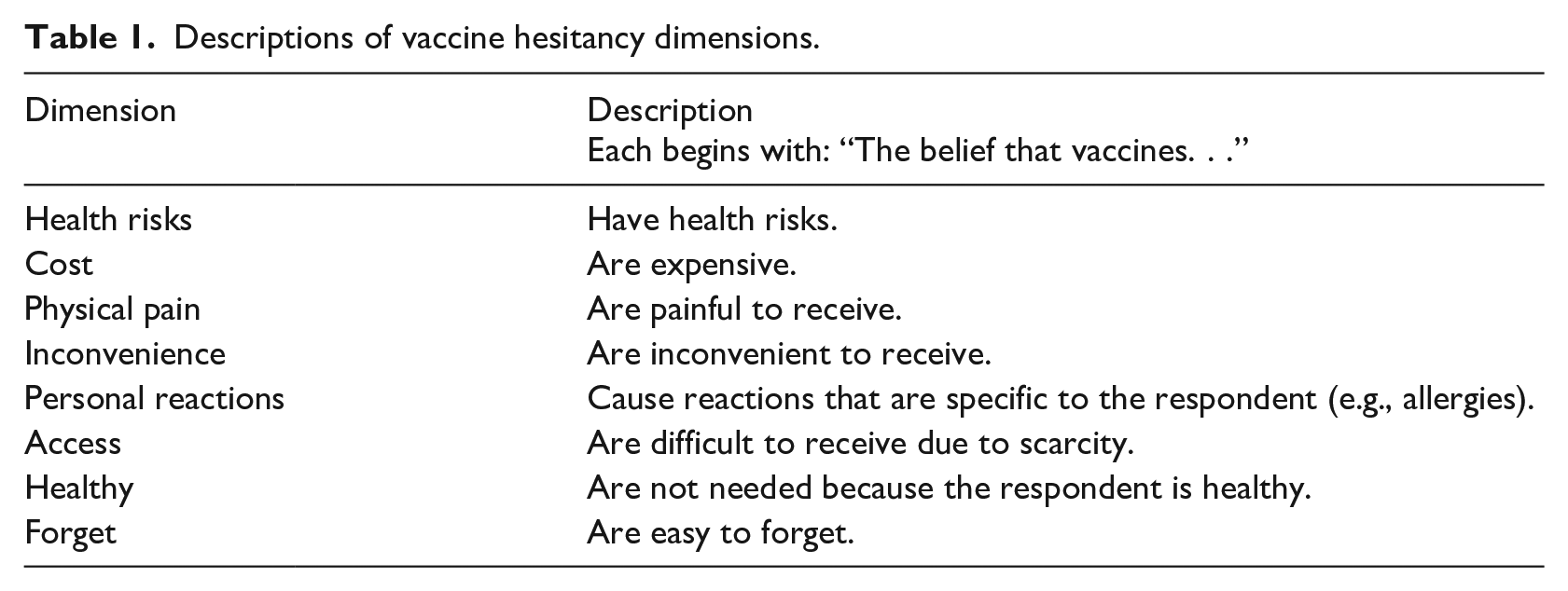
Furthermore, we apply a recently developed multidimensional conceptualization of vaccine hesitancy (Howard, 2021) to test which dimensions mediate the relation of COVID-19 conspiracy beliefs and the studied outcomes (Table 1). We predict that two dimensions of vaccine hesitancy are consistent mediators. Health Risks (the perception that vaccines cause detrimental health outcomes) and Healthy (the perception that vaccines are not needed because the respondent is healthy) reflect perhaps the most common negative information shared amongst those who hold vaccine conspiracy beliefs, and therefore are believed to be the cognitive justifications to remain unvaccinated for those who hold COVID-19 conspiracy beliefs.
Descriptions of vaccine hesitancy dimensions.
Through these efforts, the current article provides several implications for research and practice. First, we show that COVID-19 conspiracy beliefs are more detrimental than currently believed, as these beliefs cause people to share negative vaccine information and refuse other vaccines. Second, by studying mediating effects, we identify exactly why those who hold conspiracy beliefs are less likely to be vaccinated. Such a discovery can lead to interventions that break the link between COVID-19 conspiracy beliefs and detrimental outcomes. Third, Howard’s (2021) multidimensional conceptualization of vaccine hesitancy was recently developed, and the present investigation can provide further evidence that it is an appropriate lens to understand vaccine hesitancy. Fourth, these vaccine hesitancy dimensions each have differing associations with theoretical frameworks of health behaviors. The current article can initially link COVID-19 conspiracy beliefs with these theories, encouraging future research.
Method
The dataset used for the present investigation is included as Supplemental Material A.
Participants
Participants (47% female; ageMean = 38.32; ageStdDev = 11.72; 89% located in primarily English-speaking, Western countries) were recruited via Amazon’s Mechanical Turk (MTurk). Studies have shown that samples obtained via MTurk produce similar results to samples obtained via other sources (Agley et al., 2021; Aguinis et al., 2021; Chmielewski and Kucker, 2020). Participation was restricted to those who had completed at least 50 MTurk tasks with a 95% or better lifetime approval rate. All statistics, including reported sample sizes, also reflect the sample after removing 13 participants who failed more than one of seven attention checks (e.g., “Please mark strongly agree to show that you are paying attention”).
Procedure
On October 18, 2021, Participants enrolled via MTurk and immediately completed the first survey that included demographic items alone (n = 598). One week after the first survey, participants completed a second survey that included the COVID-19 conspiracy beliefs scale (n = 340). One week after the second survey, participants completed a third survey that included the vaccine hesitancy scale (n = 277). One week after the third survey, participants completed a fourth survey that included the vaccination outcomes measures (n = 254).
Measures
Unless otherwise noted, all scales used a 1 (Strongly Disagree) to 7 (Strongly Agree) format.
Independent variable
COVID-19 conspiracy beliefs
Eleven items from the 12-item scale of Wirawan et al. (2021) were administered. This scale includes items such as, “COVID-19 is a manmade disease,” and, “Bill Gates funded the COVID-19 conspiracy.” We did not include the original item, “COVID-19 vaccine and medication has been invented but is covered up,” because it is not applicable after the creation of COVID-19 vaccines. In the present sample, this scale produced a Cronbach’s alpha of .93, a mean of 2.58 (SD of 1.51), a skewness value of .80, and a kurtosis value of −.47. These values are typical of scales measuring conspiracy beliefs and COVID-19 conspiracy beliefs (Brotherton et al., 2013; Miller, 2020; Wirawan et al., 2021).
Mediator
Vaccine hesitancy
Howard’s (2021) Multidimensional Vaccine Hesitancy Scale (MVHS) was used. This scale includes 32 items, four items for each of eight dimensions. Each of these dimensions are described in Table 1. Example items are, “Vaccines can cause long-term health issues” (Health Risks), and, “I do not need vaccines because I rarely get sick” (Healthy). Each dimension had a Cronbach’s alpha of .90 or above.
Dependent variables
Vaccination willingness
Two items each were administered for flu vaccine willingness as well as COVID-19 vaccine willingness. The items read, “Please indicate how willing you would be to get a [flu vaccine/COVID-19 vaccine (or booster vaccine shot if already received vaccine)] next year if it was [free/US$40.00].” Participants responded on a 1 (Extremely Unwilling) to 7 (Extremely Willing) scale. The Cronbach’s alpha for flu vaccine willingness was .78, and the Cronbach’s alpha for COVID-19 vaccine willingness was .80. These two scales were adopted from Howard (2021), which were based on prior research.
Vaccination receipt
Single-item scales were administered for flu vaccination, other vaccinations, and COVID-19 vaccination. Participants were asked the following questions: “Have you received the flu vaccine within the past year?,” “Are you up to date on your vaccines other than the flu vaccine?,” “Have you ever received the COVID-19 vaccine?,” and “Have you tried to receive the COVID-19 vaccine but were unable to receive it due to factors outside of your control?” Participants could answer Yes (1) or No (0) to each. The last two items were combined to represent COVID-19 vaccination as a single variable, which was coded as 1 if participants responded Yes to either question and 0 if they responded No to both questions.
Vaccine word-of-mouth
Three items were administered for positive word-of-mouth and negative word-of-mouth, which were shown to be independent factors in an exploratory factor analysis (provided upon request). A positive word-of-mouth item is, “I talk to others about the benefits of vaccines,” and a negative word-of-mouth item is, “I share negative information about vaccines on social media.” Both scales had Cronbach’s alphas of .86 or above.
Results
Supplemental Material B Table 1 includes correlations and Cronbach’s alphas. COVID-19 conspiracy beliefs significantly correlated to all vaccine hesitancy dimensions and outcomes (all p < .01). These relations were positive with the vaccine hesitancy dimensions and negative with all outcomes with the exception of negative word-of-mouth, which was a positive relation.
Supplemental Material B Tables 2 and 3 include all stepwise regression results, wherein COVID-19 conspiracy beliefs alone was entered into the first step and the vaccine hesitancy dimensions were added in the second step. In the second step of these analyzes, COVID-19 conspiracy beliefs was a significant predictor of four of six outcomes (all p < .05), and the vaccine hesitancy dimensions differed in their number of significant relations. Health Risks significantly related to five of six outcomes; Healthy significantly related to four of six outcomes; Access significantly related to three of six outcomes; Inconvenience, Personal Reactions, and Forget significantly related to one outcome (all p < .05). For these effects, COVID-19 conspiracy beliefs and vaccine hesitancy negatively related to the outcomes apart from two cases. Access’s significant relations with outcomes were positive, and negative word-of-mouth’s significant relations with antecedents were positive.
Supplemental Material B Table 4 includes tests of indirect effects using percentile bootstrap estimates via Hayes’s PROCESS macro (2017; Model 4). The relation of COVID-19 conspiracy beliefs and its outcomes was significantly mediated by Health Risks in five of six relations, Healthy in four of six relations, Access in two of six relations, Personal Reactions in one of six relations, and Forget in one of six relations (all 95% C.I. exclude 0). All indirect effects produced negative relations with two exceptions. Access produced positive indirect effects on outcomes, and negative word-of-mouth had positive indirect effects with antecedents. Figure 1 presents a visual representation of all study results.
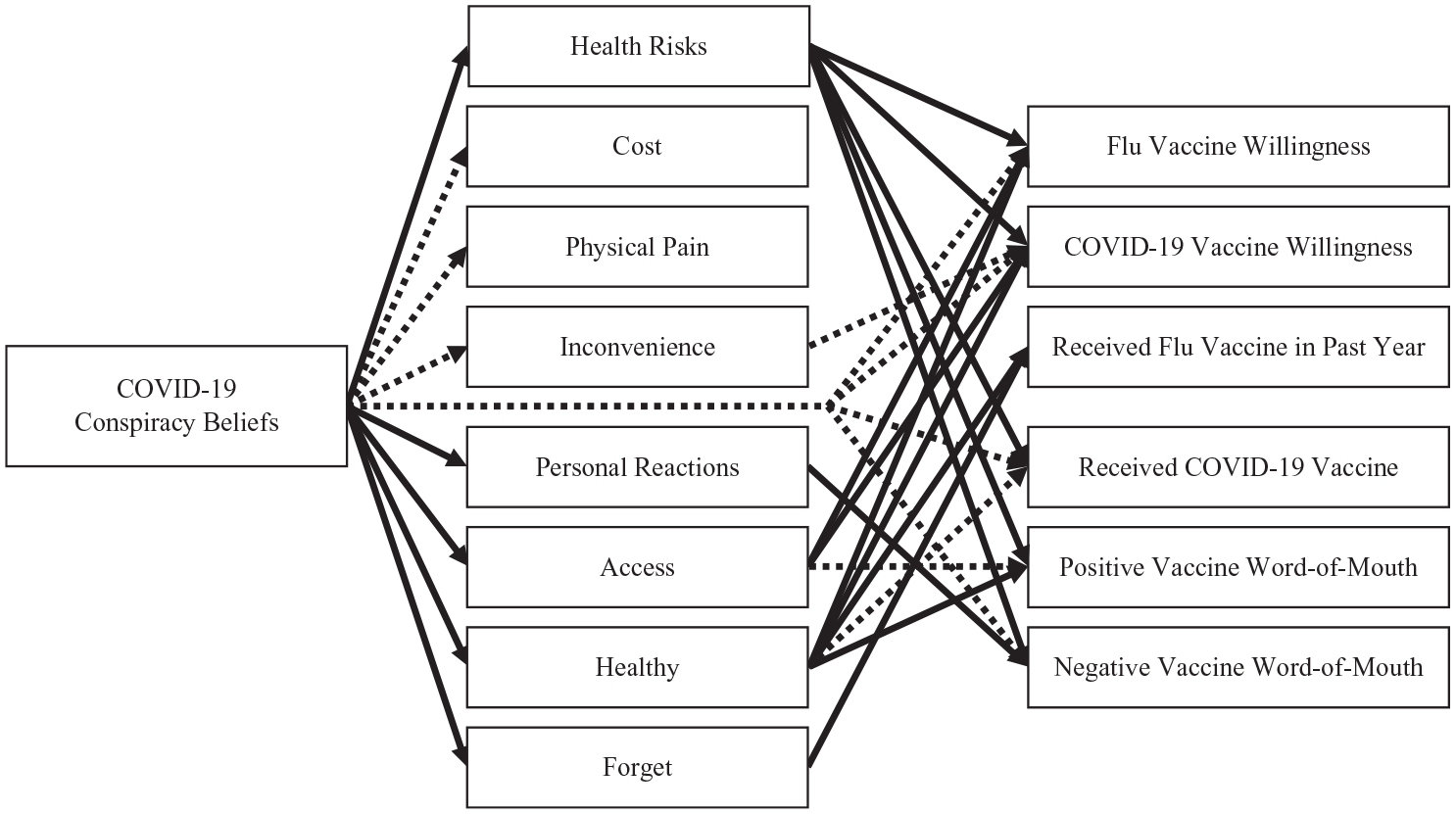
Visual representation of study results. Note: All arrows represent statistically significant relations. Solid arrows represent relations involved in significant indirect effects. Dashed arrows represent relations not involved in significant indirect effects.
Discussion
Our goal was to test the relation of COVID-19 conspiracy beliefs with a broad range of vaccination outcomes and to assess the mediating role of vaccine hesitancy’s dimensions. The results show that COVID-19 conspiracy beliefs not only relate to COVID-19 vaccination outcomes, but it also relates to flu vaccination outcomes and word-of-mouth. Several vaccine hesitancy dimensions significantly mediated these reactions, but the most consistent mediators were the dimensions of Health Risks and Healthy. These results pose many implications.
First, the relations of COVID-19 conspiracy beliefs are broader than previously observed. Not only do these beliefs relate to a broader range of behaviors (e.g., word-of-mouth), but they also relate to behaviors associated with other vaccines (e.g., flu). We studied perceptions and behaviors related to flu vaccines because of their similarities to COVID-19 vaccines; both flu and COVID-19 vaccines are widely recommended, and adults can consider whether to receive them annually. Future research, though, should assess whether COVID-19 conspiracy beliefs affect perceptions and behaviors regarding more dissimilar vaccines. For instance, parents must decide whether their children should receive the MMR vaccine, and the choice to receive vaccines for oneself may have varying influences than the choice for one’s children to receive vaccines. Similarly, some vaccines are required for certain activities (e.g., military, international travel), and personal perceptions may have a smaller influence on the decision to receive these vaccines. Therefore, the current results provide initial evidence that COVID-19 conspiracy beliefs influence broader vaccine perceptions and behaviors, but it should not be assumed that these perceptions influence all types of vaccination perceptions and behaviors.
Second, those who hold COVID-19 conspiracy beliefs refrain from receiving other vaccines and share negative information regarding vaccines, which could influence others to refuse vaccinations. Additional efforts should be allocated toward dispelling myths regarding vaccines even after the COVID-19 pandemic, as persistent misinformation could prevent current and future generations from being vaccinated against illnesses beyond COVID-19. Public health interventions should focus on delivering accurate information via channels that are known to share misinformation, such as social media (Allington et al., 2021; Georgiou et al., 2020).
Third, these public health interventions can also aim to increase vaccination rates in those who hold COVID-19 conspiracy beliefs, and our results suggest that an effective approach would be to target perceptions that vaccines are dangerous (Health Risks) or not necessary for healthy people (Healthy). While this may not cause people to abandon COVID-19 conspiracy beliefs, it may partially counteract the negative outcomes of these beliefs. An effective avenue may be to develop adaptive interventions based on the participant’s beliefs, such that certain information is provided if they hold specific COVID-19 conspiracy beliefs or vaccine hesitancy perceptions. The sequential multiphase optimization strategy may be an effective intervention development method for creating these adaptive interventions (Howard and Jacobs, 2016).
Fourth, the current results further support that Howard’s (2021) multidimensional conceptualization is a useful approach for understanding vaccine hesitancy. These dimensions each produced appropriate internal consistency estimates, and our results supported that these dimensions should be differentiated because they had differing relations with our outcomes. If vaccine hesitancy was conceptualized in a unidimensional manner, these differences would remain unnoticed. Perhaps most notably, each vaccine hesitancy dimension had detrimental relations (e.g., negative relation with vaccination receipt) apart from Access, the perception that vaccines are difficult to receive. Those who may have difficulties obtaining vaccines may be more motivated to receive them. Although this should not be a route to promote vaccination, it does indicate that other dimensions should be targeted first to promote vaccination.
Fifth, the most consistent mediators in the present investigation were Health Risks and Healthy. Health Risks is associated with heightened risks, whereas Healthy is associated with diminished benefits; these associations suggest that health behavior theories of risk-taking may be fruitful in understanding the impact of COVID-19 conspiracy theories. Notably, the approach/avoidance framework (Elliot, 2006) suggests that people have two primary cognitive systems, one associated with approaching positive stimuli and another associated with avoiding negative stimuli. COVID-19 conspiracy theories may cause individuals to possess both heightened avoidance and lowered approach tendencies toward vaccines, resulting in detrimental vaccination outcomes. Researchers should determine whether the broader aspects of the approach/avoidance framework are viable for understanding COVID-19 conspiracy beliefs, leading to many future investigations and potential interventions.
Sixth, our study was a focused investigation, but future research should investigate the presently studied relations in the context of broader models. The COM-B model proposes that capability, motivation, opportunity, and their dimensions are the primary influences of behavior (Michie et al., 2011), and it has been used to identify predictors of preventative behaviors at multiple levels of analysis (e.g., system-level, provider-level, patient-level; McDonagh et al., 2018). Studying predictors at higher levels of analysis (system- and provider-level) may be particularly fruitful. For instance, political norms (system-level) may influence conspiracy beliefs and vaccine hesitancy (patient-level) to ultimately influence vaccination behaviors, which can advance prior research linking political affiliation to conspiracy beliefs (van Prooijen et al., 2015; Vitriol and Marsh, 2018). Researchers could likewise replicate the current results in more conservative conditions by including other predictors identified via the COM-B model, such as contextual influences and individual differences. Therefore, the integration of modern theory on preventative behaviors should be a primary direction for future research.
Seventh, we conducted unreported analyzes with typical control variables (age, gender, location, and education), and all inferences remained consistent between these analyzes and our reported analyzes. These results can be provided upon request. We chose to report results without control variables due to simplicity and previously expressed concerns regarding the “overcontrol” of variables in psychological research (Spector and Brannick, 2011); however, while we believe that our results are robust, it should not necessarily be assumed that they would replicate when including any control variables and/or other relevant predictors. Testing broader models, as recommended above, can address this concern. Supplemental Material B presents a model with political orientation and personality integrated into the current investigation. Political orientation is known to predict conspiracy beliefs (Enders et al., 2020), and dimensions of the Big Five (e.g., openness and/or conscientiousness) and Dark Triad have been shown to predict political orientation (Ahadzadeh et al., 2021; Bell et al., 2021), conspiracy beliefs (Vecchione et al., 2011), vaccine hesitancy, and vaccination behaviors (Howard, 2022a). Integrating these predictors may not only show that conspiracy beliefs is still a significant predictor when accounting for other relevant predictors, but they may also demonstrate that these various predictors of vaccination are closely intertwined. Such an integrative model may be key in understanding the process of developing vaccine hesitancy and vaccination.
Eighth, future research should replicate prior studies on vaccine hesitancy conducted before the COVID-19 pandemic. Notably, Ekram et al. (2019) content analyzed YouTube videos from 2014 on HPV vaccines. They found that most videos were negative in tone, and the primary concerns focused on detrimental health outcomes and conspiracy theories. This closely relates to the present investigation showing that COVID-19 conspiracy beliefs produced their strongest relations with the vaccine hesitancy dimensions of Health Risks and Healthy. On the other hand, vaccination is now a more contentious topic than prior to the COVID-19 pandemic (Georgiou et al., 2020; Hughes and Machan, 2021). While messages may be similar, the increased attention to negative information regarding vaccination may cause word-of-mouth to have an even stronger influence on others’ vaccination outcomes. Thus, future studies may discover both similarities and differences with prior investigations, both of which could inform understandings of conspiracy beliefs and how they function differently across time and vaccine type.
Ninth, conspiracy beliefs are believed to develop relatively quickly, and this is especially true with the changing nature of the COVID-19 pandemic (Howard, 2022b). Future researchers should replicate the current results across timespans to identify how the changing nature of conspiracy beliefs may influence vaccine perceptions and behaviors.
Tenth, future research should address limitations of the current study. We utilized a time-separated design to reduce common method bias, but future researchers should use a longitudinal design with each variable measured on all occasions to assess change in outcomes. Likewise, MTurk enables the collection of diverse participants, but future research should replicate the current results using alternative sampling sources. The current sample slightly skewed toward being more liberal on a 1 (Strongly Conservative) to 9 (Strongly Liberal) scale (mean = 5.87, S.D. = 2.44). While this skew reflects current trends of self-reported political polling (Gallup, 2021; Howard, 2022b), future researchers should replicate the current results using a balanced sample because political orientation relates to conspiracy beliefs (Imhoff et al., 2022; van Prooijen and van Vugt, 2018). The current sample was similarly well educated (highest degree: 9% high school, 17% some college, 11% 2-year, 39% 4-year, 19% graduate, 4% doctorate), indicating that future research should investigate more educationally representative populations. The current sample was also largely representative of the United States. At the time of the first survey, 58% of Americans were fully vaccinated, which was roughly the 65th percentile of vaccination rate by country (Our World in Data, 2022). Our results should be replicated in contexts with differing vaccination practices to test the generalizability of the current results.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053221096013 – Supplemental material for The mediating role of vaccine hesitancy in the relations of COVID-19 conspiracy beliefs and vaccination outcomes: Which dimensions matter?
Supplemental material, sj-docx-1-hpq-10.1177_13591053221096013 for The mediating role of vaccine hesitancy in the relations of COVID-19 conspiracy beliefs and vaccination outcomes: Which dimensions matter? by Matt C. Howard and Maggie M. Davis in Journal of Health Psychology
Supplemental Material
sj-docx-3-hpq-10.1177_13591053221096013 – Supplemental material for The mediating role of vaccine hesitancy in the relations of COVID-19 conspiracy beliefs and vaccination outcomes: Which dimensions matter?
Supplemental material, sj-docx-3-hpq-10.1177_13591053221096013 for The mediating role of vaccine hesitancy in the relations of COVID-19 conspiracy beliefs and vaccination outcomes: Which dimensions matter? by Matt C. Howard and Maggie M. Davis in Journal of Health Psychology
Research Data
sj-xlsx-2-hpq-10.1177_13591053221096013 – for The mediating role of vaccine hesitancy in the relations of COVID-19 conspiracy beliefs and vaccination outcomes: Which dimensions matter?
sj-xlsx-2-hpq-10.1177_13591053221096013 for The mediating role of vaccine hesitancy in the relations of COVID-19 conspiracy beliefs and vaccination outcomes: Which dimensions matter? by Matt C. Howard and Maggie M. Davis in Journal of Health Psychology
Footnotes
Data sharing statement
The current article is accompanied by the relevant raw data generated during and/or analysed during the study, including files detailing the analyses and either the complete database or other relevant raw data. These files are available in the Figshare repository and accessible as Supplemental Material via the SAGE Journals platform. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.