
Abstract
This study examined whether body appreciation mediates the relationships between anti-fat microaggression experiences and perceived physical and mental health. Using a cross-sectional survey design, our study included 384 adult cisgender women in the United States. We found that anti-fat microaggression experiences had a negative association with body appreciation, and perceived physical and mental health. Body appreciation had a positive relationship to perceived physical and mental health. Our study further suggests that body appreciation is an important modifiable factor that mediates the relationships between anti-fat microaggression experiences and perceived mental and physical health. Implications for practice and research are discussed.
Introduction
Microaggressions are “verbal and nonverbal interpersonal exchanges in which a perpetrator causes harm to a target, whether intended or unintended” (Sue and Spanierman, 2020: 8). While they are generally brief, they “communicate hostile, derogatory, and/or negative slights to the target” (Sue and Spanierman, 2020: 8), and result from stigma. Microaggressions have a cumulative impact as well as create anticipation and fear of additional microaggressions among the oppressed population on the receiving end (Munro, 2017). Though not discussed in the academic literature as much as weight stigma, “stereotyping and devaluation on the basis of excess body weight,” (Himmelstein et al., 2018: 139), anti-fat microaggressions are a consequence of weight stigma and are harmful and pervasive for fat individuals. In fact, according to Munro (2017: 504), “there are few environments and interpersonal relationships that are untouched by weight stigma” and, therefore, anti-fat microaggressions. In a multinational study of adults, over half reported experiencing weight stigma (Lessard et al., 2021), and research suggests that women are more likely to experience weight stigma than men (Puhl et al., 2008). Microaggressions can occur daily in a person’s interpersonal relationships and environmental contexts, and they can severely impact both mental and physical health (Williams, 2020). Given this, it is important to understand the ways that weight stigma and anti-fat microaggressions affect health, and identify ways to mitigate their effects.
Literature review
The literature on anti-fat microaggressions is scant. However, contexts surrounding their occurrence can be informed by existing research on racial microaggressions. Further, anti-fat microaggressions result from weight stigma (Munro, 2017). Thus, our review of the literature focuses on racial microaggressions and weight stigma.
Racial microaggressions and health
The harmful psychological effects of racial microaggressions have been well documented. In a review of 138 studies published between 2007 and 2020, Spanierman et al. (2021) found that experiencing microaggressions was associated with worse self-esteem, higher levels of depression symptoms, anxiety, stress, and suicidal ideation. Additionally, in a study of Latinx Americans, Anderson and Finch (2017) found that among those who reported being more acculturated, higher stress from microaggressions was related to worse self-reported physical health. Research has also found a negative relationship between racial microaggressions and sleep quality (Ong et al., 2017), and that racial microaggressions are related to pain, lower energy levels, fatigue, and more (Nadal et al., 2017). Taken together, available research suggests that racial microaggressions are related to both physical and mental health.
Weight stigma and health
There is a significant amount of research supporting the relationship between higher weight stigma and poorer mental health outcomes. For example, Hunger and Major (2015) found that weight stigma mediated the relationship between body mass index (BMI) and self-reported mental health outcomes, including self-esteem, depression, and quality of life, among a sample of 171 adults in the United States (U.S.). Another study of a large representative sample of noninstitutionalized adults in the U.S., found significant associations between weight stigma and mood and anxiety disorders, while controlling for BMI (Hatzenbuehler et al., 2009). Similarly, Emmer et al. (2020) conducted a meta-analysis of 105 studies, 59,172 participants, and 497 effect sizes and found a medium to large effect size in the relationship between weight stigma and mental health with the higher the perceived stigma, the worse the mental health status. This suggests that there may be clinical significance in the relationship between weight stigma and mental health, in addition to statistical significance.
Weight stigma is related to physical health in myriad ways. Researchers found significant relationships between weight stigma and self-reported physical health outcomes (Hunger and Major, 2015), increased food consumption (Major et al., 2014; Schvey et al., 2011), and decreases in self-regulation (Major et al., 2014) in various samples of U.S. adults. Further, weight stigma is associated with greater disordered eating and comfort eating (Lee et al., 2021). In a systematic review of 33 studies, Wu and Berry (2018) found that higher weight stigma was positively and significantly associated with diabetes risk, cortisol level, oxidative stress level, C-reactive protein level, and eating disturbances. Finally, research suggests that weight stigma may be related to the worst health outcome—mortality, with an increased risk of nearly 60% (Sutin et al., 2015). Thus, weight stigma is related to poorer physical health and it is possible weight stigma shortens life expectancy.
To effectively mitigate the impact of weight stigma on mental and physical health, it is important to understand the constructs that mediate the relationship. For example, in one study, Himmelstein et al. (2018) found that coping responses mediate the relationship between weight stigma and health/mental health among a national sample of U.S. adults, which has implications for future interventions. Given relationships between body appreciation, physical health, and mental health (e.g. Gillen, 2015; O’Neill et al., 2018; Ramseyer Winter et al., 2017), it is possible that body appreciation, defined as “accepting, holding favorable opinions toward, and respecting the body, while also rejecting media-promoted appearance ideals as the only form of human beauty” (Tylka and Wood-Barcalow, 2015: 53), may mediate the relationship between weight stigma/anti-fat microaggressions and perceived physical and mental health. Researchers have found that body appreciation is negatively related to anxiety, depression, and self-reported physical health (Ramseyer Winter et al., 2017), positively related to self-esteem (Gillen, 2015), and that age moderates the relationship between body appreciation and health-related quality of life (O’Neill et al., 2018). Taken together, research suggests that body appreciation is related to both physical and mental health.
Current study
The current study examined whether body appreciation mediated the relationships between anti-fat microaggression experiences and perceived physical and mental health among cisgender women. We chose to focus on perceived physical and mental health because of its relationship to objective health measures (Wu et al., 2013), and the availability of multidimensional measures. Additionally, objective health measures, such as diagnoses, require access to healthcare, which can be affected by SES, health insurance status, geographic location, and other structural and social factors (Litaker et al., 2005). Age, race/ethnicity, health insurance, and SES were included as covariates due to an expansive body of research that establishes them as social determinants of health (Solar and Irwin, 2010). Additionally, research suggests that body appreciation differs by age (e.g. Tiggemann and McCourt, 2013), race/ethnicity (e.g. Gillen, 2015), and SES (e.g. Ramseyer Winter et al., 2021). BMI, a proxy for body size, was included as a covariate due to research that suggests it is related to body image (e.g. Gillen, 2015). The following hypotheses were examined:
H1 = Body appreciation mediates the relationship between anti-fat microaggression experiences and perceived physical health.
H2 = Body appreciation mediates the relationship between anti-fat microaggression experiences and perceived mental health.
Methods
Procedure
The current study used a cross-sectional survey design, and convenience sampling was used to select participants. To qualify for the study, participants had to be 18 years of age or older, identify as a cisgender woman, live in the United States, and be able to complete the survey in English. Following IRB approval from the University of Missouri IRB (project number 2040882; approved 11/20/2020), participants were recruited for the study via social media (Facebook and Twitter) and were provided with a link to a Qualtrics online survey. Participants provided informed consent for participation electronically by selecting the appropriate response option and choosing to proceed forward with the survey, and were compensated with a $5 gift card for their participation. To keep survey responses anonymous, participants completed a separate electronic form to provide the information necessary for the gift card distribution. To assure data quality, data was checked visually for individual participants and through the use of descriptive analysis by multiple researchers to identify responses that were out of range or invalid.
Measures
Anti-fat microaggression experiences
Anti-fat microaggression experiences was measured with the 31-item Anti-Fat Microaggression Experiences Questionnaire (AFMEQ; Webb et al., 2019). Participants were asked to rate how often during the prior 6 months each item happened, because of their weight or body size, on a six-point scale (never, once or twice, about once a month, few times a month, weekly, several times a week or daily). Sample items included: “Someone gave me an offensive look,” “Someone made a comment suggesting I did not exercise or work out enough,” and “Felt like the media distorts the length of time it takes to lose weight safely.” Participants’ responses on the items were summed to create a scale score, where a higher score equaled a higher degree of anti-fat microaggression experiences. The internal consistency of the AFMEQ with the current sample was estimated to be high (Cronbach’s α = 0.941).
Body appreciation
We measured body appreciation with the Body Appreciation Scale-2 (BAS-2; Tylka and Wood-Barcalow, 2015), which included 10 items that participants reported as being true “never,” “seldom,” “sometimes,” “often,” or “always.” Sample items included “I feel love for my body” and “I appreciate the different and unique characteristics of my body.” A higher BAS-2 score, calculated by averaging the 10 items, indicated higher body appreciation. The internal consistency of the BAS-2 with the current sample was acceptable (Cronbach’s α = 0.860).
Perceived physical and mental health
Perceived physical and mental health were measured using the Short Form (SF)-12 Health Survey (Ware et al., 1996). The SF-12 includes 12 items, with varying response options, and two summary scores are produced: Physical Component Summary (PCS), representing perceived physical health, and Mental Component Summary (MCS), representing perceived mental health. The PCS and MCS were scored separately using norm-based scoring (M = 50, standard deviation = 10; Ware et al., 1995): Sample items included “In general, would you say your health is (excellent, very good, good, fair, poor),” and “During the past 4 weeks how much did pain interfere with your normal work (including both working outside the home and housework)? (not at all, a little bit, moderately, quite a bit, extremely).” Higher PCS and MCS scores indicated better perceived physical and mental health, respectively.
Covariates
Age (continuous variable), racial and ethnic background (White/Caucasian/European, Black/African American, or Other Person of Color), health insurance status (insured all of prior 12 months, uninsured at any time during prior 12 months), body mass index (BMI; continuous), and SES (continuous), were included as covariates in the study. BMI was calculated using self-reported height and weight (CDC, n.d.). Due to skewness values greater than +1, age (skewness = 1.142) and BMI (skewness = 1.672) were log-transformed for use in multivariate analyses.
SES was measured with the five-item Financial Strain Index (FSI; Hamby et al., 2011), which included response options of “very true,” “a little true,” or “not true.” Sample items included, “You are behind one month or more on your rent or mortgage payment” and “It would be hard for you to find the money to cover an unexpected expense, such as a medical bill or repair that was $500 or more.” A higher summed score indicated more financial strain, and this index was used as an indicator of SES (Cronbach’s α = 0.827).
Participant characteristics and descriptive statistics
The sample included 384 cisgender women, 18 years of age or older, living in the United States. The majority of participants reported being White/Caucasian/European (66.4%) and having health insurance for the prior 12 months (67.2%). The mean age of participants was approximately 33 years (SD = 7.43), and the mean financial strain index score was 8.35 (range = 5–15; SD = 2.84). A diverse range of body sizes, as measured by BMI, were represented in the sample (range = 15.94–62.64), and the mean BMI was 28.36 (SD = 8.17), which is characterized as “overweight” by the CDC (n.d.). Participants had mean BAS-2 score of 3.34 (range = 1.30–5.00; SD = 0.66), and the mean AFMEQ score was 83.89 (range = 31.00–141.00; SD = 26.67).
The SF-12 uses norm-based scoring to allow for comparisons to the general U.S. population. The mean PCS score in this sample was 46.87 (SD = 9.00), and the mean MCS score was 43.57 (SD = 10.17). These scores are lower than the mean PCS (M = 49.11, SD = 9.92) and MCS (M = 49.42, SD = 9.80) scores for women in the general U.S. population (Ware et al., 1995), and suggest that our sample perceived their physical and mental health to be lower than perceptions of women in the general U.S. population. See Table 1 for full details regarding the participants’ characteristics, and descriptive statistics for the study indicators.
Participant characteristics and descriptive analysis (N = 384).
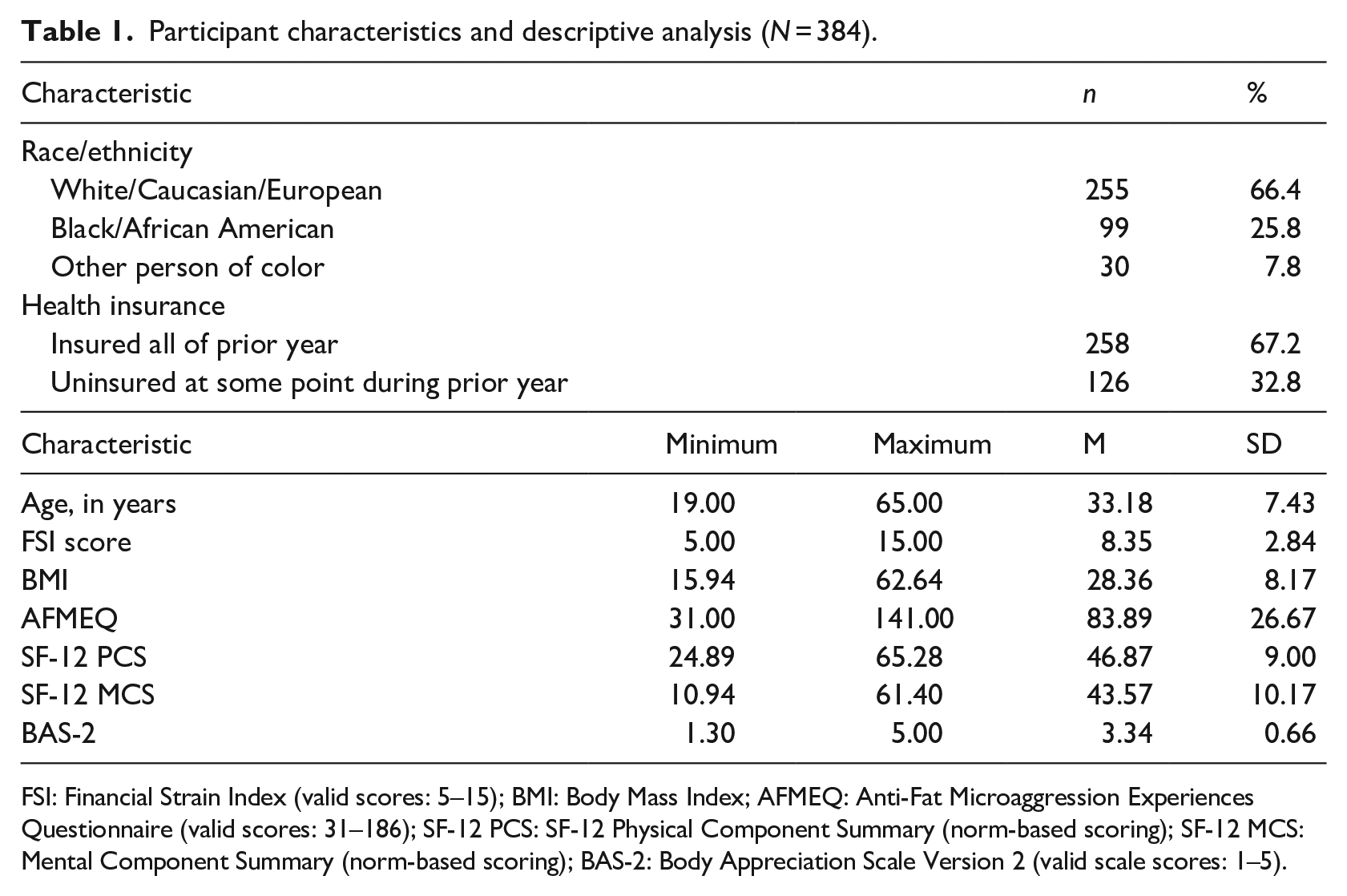
FSI: Financial Strain Index (valid scores: 5–15); BMI: Body Mass Index; AFMEQ: Anti-Fat Microaggression Experiences Questionnaire (valid scores: 31–186); SF-12 PCS: SF-12 Physical Component Summary (norm-based scoring); SF-12 MCS: Mental Component Summary (norm-based scoring); BAS-2: Body Appreciation Scale Version 2 (valid scale scores: 1–5).
Analytic plan
SPSS 27 was used to test the hypothesized mediation models (see Figure 1). The Process Macro (Hayes, 2022) was used to complete a series of linear regression analyses based on 5000 bootstrap samples, controlling for age, race/ethnicity, health insurance status, BMI, and SES, to examine the direct and indirect relationships between: (1) AMFEQ, BAS-2, and PCS and (2) AMFEQ, BAS-2, and MCS. Given that the Sobel test incorrectly assumes a normal distribution for the indirect effect (MacKinnon et al., 2007), bias-corrected bootstrapped confidence intervals were instead used to provide accurate confidence intervals, better statistical power for detecting indirect effects, and a lower risk of type 1errors (MacKinnon et al., 2004). Mediation was indicated if the 95% bias-corrected bootstrapped confidence intervals for the indirect effects didn’t contain zero (MacKinnon et al., 2004).
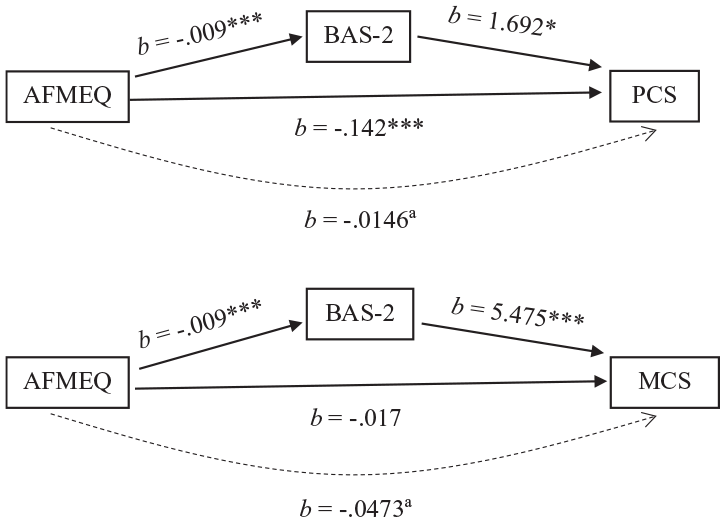
Mediation models. Both models control for race/ethnicity, age, SES, health insurance, and BMI.
Results
AFMEQ, BAS, and PCS mediation model
A bootstrapping method was completed using the SPSS Process Macro (Hayes, 2022) to examine direct and indirect relationships between AFMEQ, BAS-2 (i.e. body appreciation), and PCS (i.e. perceived physical health). Table 2 presents results for the complete PCS regression model. The model was statistically significant (F(7, 282) = 25.816, p < 0.001)and explained approximately 39% of the variance in perceived physical health (R2 = 0.391). Controlling for all covariates, regression analyses indicated that AFMEQ was a significant predictor of body appreciation (b = −0.009, p < 0.001), and a significant predictor of perceived physical health while also controlling for body appreciation (b = −0.142, p < 0.001). Body appreciation (i.e. BAS-2) was also significantly related to perceived physical health (b = 1.692, p < 0.05). Socioeconomic status, as measured by the Financial Strain Index, was the only covariate with statistical significance in the full model (b = −0.774, p < 0.001).
Regression results (n = 290).
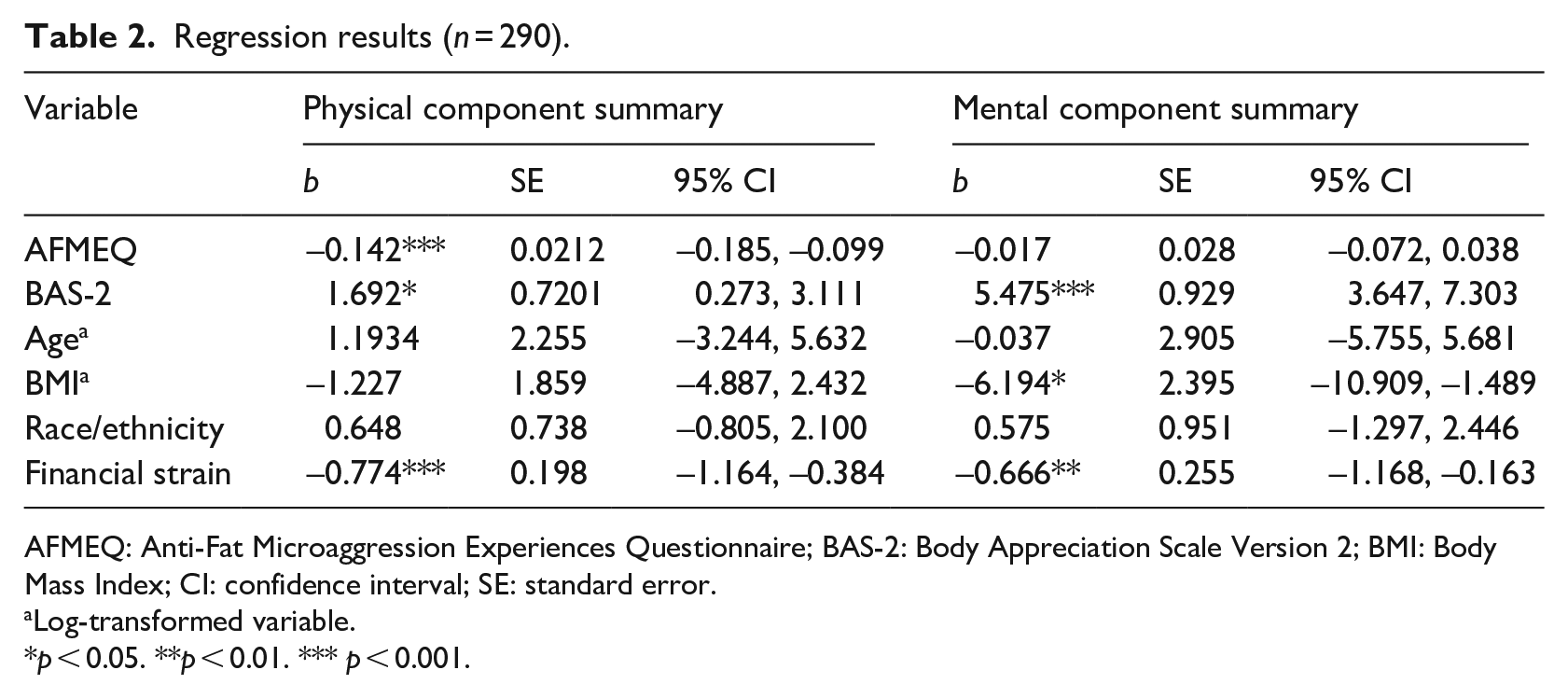
AFMEQ: Anti-Fat Microaggression Experiences Questionnaire; BAS-2: Body Appreciation Scale Version 2; BMI: Body Mass Index; CI: confidence interval; SE: standard error.
Log-transformed variable.
p < 0.05. **p < 0.01. *** p < 0.001.
Results also showed a significant indirect effect, specifically an indirect negative relationship between AFMEQ, body appreciation, and perceived physical health (b = −0.0146, Bias-Corrected Bootstrapped 95% CI = −0.0303, −0.0010). The mediator, body appreciation, accounted for approximately 9% of the total effect on perceived physical health. These results indicated partial statistical mediation by body appreciation of the relationship between AFMEQ and perceived physical health (see Figure 1), supporting our hypothesis. See Table 3 for full mediation analysis results.
Mediation results (n = 290).
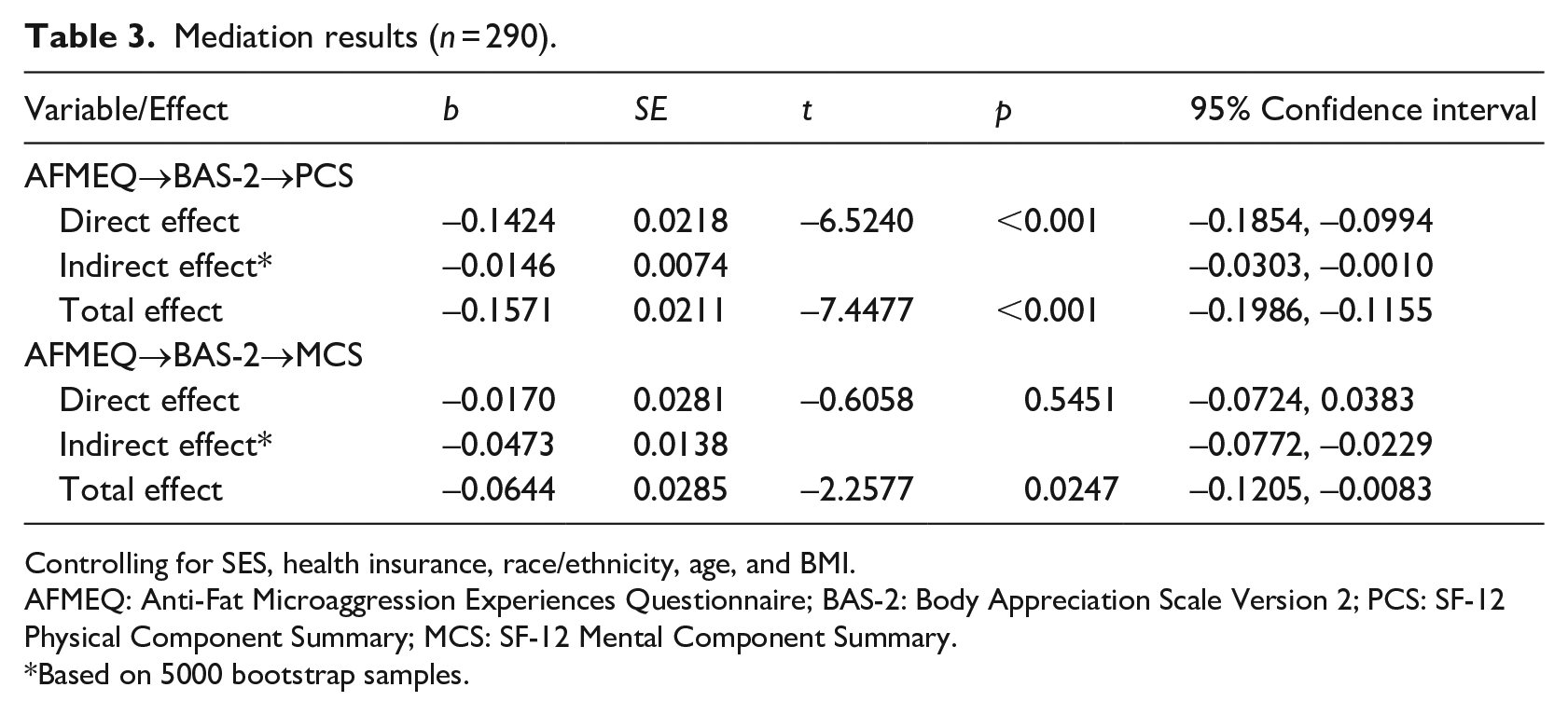
Controlling for SES, health insurance, race/ethnicity, age, and BMI.
AFMEQ: Anti-Fat Microaggression Experiences Questionnaire; BAS-2: Body Appreciation Scale Version 2; PCS: SF-12 Physical Component Summary; MCS: SF-12 Mental Component Summary.
Based on 5000 bootstrap samples.
AFMEQ, BAS, and MCS mediation model
A bootstrapping method was again completed using the SPSS Process Macro (Hayes, 2022) to examine direct and indirect relationships between AFMEQ, BAS-2 (i.e. body appreciation), and MCS (i.e. perceived mental health). Table 2 presents results for the complete MCS regression model. The model was statistically significant (F(7, 282) = 11.657, p < 0.001)and explained approximately 22% of the variance in perceived mental health (R2 = 0.224). Controlling for all covariates, regression analyses indicated that AFMEQ was a significant predictor of body appreciation (b = −0.009, p < 0.001), and was a significant predictor of perceived mental health without body appreciation included in the model (b = −0.064, p < 0.05). However, AFMEQ was not a significant predictor of perceived mental health while also controlling for body appreciation (b = −0.017, p = 0.545). Body appreciation (i.e. BAS-2) was also significantly related to perceived mental health (b = 5.475, p < 0.001). Two covariates, BMI (b = −6.194, p < 0.05) and SES (b = −0.666, p < 0.01), were also significantly related to perceived mental health in the full model.
Results also showed a significant indirect effect, specifically an indirect negative relationship between AFMEQ, body appreciation, and perceived mental health (b = −0.0473, Bias-Corrected Bootstrapped 95% CI = −0.0772, −0.0229). The mediator, body appreciation, accounted for approximately 73% of the total effect on perceived mental health. These results indicated complete statistical mediation by body appreciation of the relationship between AFMEQ and perceived mental health (see Figure 1), supporting our hypothesis. See Table 3 for full mediation analysis results.
Discussion
Though microaggressions are often ambiguous and difficult to recognize as discrimination, they are well-documented as forms of bias and discrimination. Individuals with high body weight face societal stigma, known as weight stigma, which includes numerous negative weight-based stereotypes, discrimination, and prejudice in many societal domains, including healthcare (Himmelstein et al., 2017; Spahlholz et al., 2016). Even though we know that microaggressions exist and disproportionately impact women (Puhl et al., 2008; Spahlholz et al., 2016), modifiable factors that mediate the relationship with health outcomes have been understudied. The objective of this study was to understand the relationship between anti-fat microaggression experiences, body appreciation, and perceived physical and mental health among adult cisgender women. Consistent with our hypotheses, we found that body appreciation mediated the relationships between anti-fat microaggression experiences and perceived physical and mental health.
First, our study provided evidence for negative relationships between experiencing anti-fat microaggressions and physical and mental health for cisgender women. Specifically, anti-fat microaggression experiences was directly and indirectly negatively related to perceived physical and mental health. This is consistent with several longitudinal studies demonstrating that microaggressions are linked to numerous poor health outcomes (Williams, 2020), including: greater inflammation, memory declines, and reported loneliness (Zahodne et al., 2019); alcohol-related problems (Hatzenbuehler et al., 2011); and poorer emotional health (Luo et al., 2012). Body-related and weight-related stigma have also been associated with important health outcomes, such as unhealthy behaviors and poor self-care (Hunger et al., 2015; Muennig, 2008), healthcare access and quality of care received (Alegria Drury and Louis, 2002; Phelan et al., 2015), healthcare avoidance (Mensinger et al., 2018), exacerbation of “obesity”-associated diseases (Muennig, 2008; Puhl and Heuer, 2010), increased blood pressure (Kube et al., 2016; Major et al., 2012), and mortality (Sutin et al., 2015). Clearly, the cascade of psychological and physiological mechanisms resulting from microaggressions and weight-based stigma have negative implications for mental and physical health, exacerbating diseases and reinforcing cycles of unhealthy behaviors and adverse health outcomes. Given this, it is important to identify interventions and modifiable factors that may mediate the relationship between anti-fat microaggressions and physical and mental health for adult cisgender women.
This is the first known study to explore the relationship between anti-fat microaggressions, body appreciation, and perceived mental and physical health. Anti-fat microaggression experiences was negatively related to body appreciation, and body appreciation was positively related to perceived physical and mental health. Our mediation model showed that the indirect effect of anti-fat microaggressions through body appreciation accounted for 73% of the total effect on perceived mental health, and 9% of the total effect on physical health. Other research has similarly found that body appreciation is positively related to physical and mental health outcomes (e.g. Gillen, 2015; O’Neill et al., 2018; Ramseyer Winter et al., 2017). Body appreciation has also been found to negatively predict body-related shame (Avalos et al., 2005). Furthermore, body shame and dissatisfaction due to weight-related microaggressions that decrease body appreciation may lead to physical anxiety (Cash et al., 2004), excessive exercise (Yager et al., 2017), unhealthy diet (Slevec and Tiggemann, 2011), and eating disorders (Hoek and van Hoeken, 2003; Stice and Shaw, 2002), which can negatively impact physical and mental health outcomes. Thus, body appreciation is an important modifiable factor, and our findings suggest that interventions focused on improving body appreciation may help buffer the effect of anti-fat microaggression that women face in their environment, resulting in better mental and physical health outcomes.
Given the high percentage of the total effect on perceived mental health that was attributed to the indirect effect through body appreciation, interventions related to body appreciation may be particularly beneficial for improving mental health outcomes. Exercise interventions (Campbell and Hausenblas, 2009), body functionality-based approaches (Alleva et al., 2018) and using 3D scanning technology and personalized avatars to train participants to focus on ways they appreciate their bodies (Ramseyer Winter et al., 2019a) are examples of strategies that have demonstrated effectiveness for improving body image. Importantly, the study of women aged 18–25 years by Ramseyer Winter et al. (2019b) found that their 3D scanning intervention not only increased body appreciation, but also decreased anxiety among participants. Additional research is needed to examine body appreciation interventions in the context of relationships between anti-fat microaggression experiences and perceived mental (and physical) health, and interventions within healthcare environments should be explored.
The indirect effect of anti-fat microaggression experiences on perceived physical health, through body appreciation, only explained 9% of the total effect. Additional research is needed to understand other potential modifiable constructs that could mitigate the effect of anti-fat microaggression experiences on perceived physical health. Research is also needed to determine sources of weight-related microaggressions and weight stigma that cisgender women face in their environment. Given that weight-related microaggressions can be encountered in many settings and relationships, integrative and multisystemic approaches may be needed to address the occurrence of anti-fat microaggressions that cisgender women experience in their environment, including the healthcare environment.
There are several limitations of this study. First, we are not able to establish causality due to the cross-sectional study design. Longitudinal studies are needed to establish temporality of anti-fat microaggressions and to establish the dynamic relationships between our study variables. Given this, it is important to note that statements regarding statistical mediation should not be confused with statements of causal mediation. Relatedly, the finding of statistical complete mediation in the perceived mental health (i.e. MCS) model should be interpreted with caution. Other variables not included in this study may also explain the relationship between AFMEQ and MCS, and sample size can affect the statistical power to be able to detect a direct effect (Hayes and Rockwood, 2017). Second, our sample was selected using convenience methods and were recruited using social media, limiting the representativeness and generalizability of our findings. Future research would benefit from the use of probability-based sampling methods. Additionally, all variables were measured via self-report. Inaccurate reporting by the participants would affect the validity of our findings.
Body-related microaggressions/discrimination transcends across race/skin color/tone, and gender. The current study only included cisgender women, and the majority identified as White/Caucasian/European. The current study is highly representative of a majority/advantaged population, but the relationships in this study are also important to understand among minority populations that face disadvantages, especially those with intersecting identities (e.g. race, gender) (Himmelstein et al., 2017). Evidence suggests that racial minority populations are more likely to attribute differential treatment to race, and the association between attributions to race and negative emotions are stronger among minority populations than majority White populations (Wang et al., 2011). Larger studies representing minority populations that account for intersecting identities are needed. Finally, the use of BMI is problematic (Satinsky and Ingraham, 2014), and research suggests that its relationship with health is unclear (Nuttall, 2015), but it is currently the best proxy for body size.
Conclusion
Overall, our study found that body appreciation mediates relationships between anti-fat microaggression experiences and perceived mental and physical health for adult cisgender women. It is well-documented that the consequences of weight stigma and microaggressions experienced in the environment are vast, and women are disproportionately affected by weight-related bias and stigma compared to men (Puhl et al., 2008; Spahlholz et al., 2016). We must start to understand the impact of anti-fat microaggressions and the modifiable mediating factors, such as body appreciation, on women’s health outcomes, and the measurable physical and mental harm they cause. The research and practice communities should work together to identify approaches to (1) address anti-fat microaggressions and discrimination that cisgender women experience in the environment and (2) develop interventions focused on building body appreciation.
Research Data
sj-docx-5-hpq-10.1177_13591053221103421 – Relationships between experiencing anti-fat microaggressions, body appreciation, and perceived physical and mental health
sj-docx-5-hpq-10.1177_13591053221103421 for Relationships between experiencing anti-fat microaggressions, body appreciation, and perceived physical and mental health by Elizabeth A O’Neill, Kate Trout and Virginia Ramseyer Winter in Journal of Health Psychology
Research Data
sj-sav-1-hpq-10.1177_13591053221103421 – Relationships between experiencing anti-fat microaggressions, body appreciation, and perceived physical and mental health
sj-sav-1-hpq-10.1177_13591053221103421 for Relationships between experiencing anti-fat microaggressions, body appreciation, and perceived physical and mental health by Elizabeth A O’Neill, Kate Trout and Virginia Ramseyer Winter in Journal of Health Psychology
Research Data
sj-spv-2-hpq-10.1177_13591053221103421 – Relationships between experiencing anti-fat microaggressions, body appreciation, and perceived physical and mental health
sj-spv-2-hpq-10.1177_13591053221103421 for Relationships between experiencing anti-fat microaggressions, body appreciation, and perceived physical and mental health by Elizabeth A O’Neill, Kate Trout and Virginia Ramseyer Winter in Journal of Health Psychology
Research Data
sj-spv-3-hpq-10.1177_13591053221103421 – Relationships between experiencing anti-fat microaggressions, body appreciation, and perceived physical and mental health
sj-spv-3-hpq-10.1177_13591053221103421 for Relationships between experiencing anti-fat microaggressions, body appreciation, and perceived physical and mental health by Elizabeth A O’Neill, Kate Trout and Virginia Ramseyer Winter in Journal of Health Psychology
Research Data
sj-spv-4-hpq-10.1177_13591053221103421 – Relationships between experiencing anti-fat microaggressions, body appreciation, and perceived physical and mental health
sj-spv-4-hpq-10.1177_13591053221103421 for Relationships between experiencing anti-fat microaggressions, body appreciation, and perceived physical and mental health by Elizabeth A O’Neill, Kate Trout and Virginia Ramseyer Winter in Journal of Health Psychology
Footnotes
Data sharing statement
The current article is accompanied by the relevant raw data generated during and/or analysed during the study, including files detailing the analyses and either the complete database or other relevant raw data. These files are available in the Figshare repository and accessible as Supplemental Material via the SAGE Journals platform. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.