
Abstract
Moral distress, or the inability to act congruent with moral beliefs, has been of concern for healthcare professionals especially since the COVID-19 pandemic. Hospital nurses are particularly affected in their roles with mounting administrative pressures and demands. We examined whether general and COVID-specific support in employing healthcare organizations predicted moral distress in a sample of inpatient hospital nurses. A total of 248 nurses completed the Measure of Moral Distress for Healthcare Professionals, Survey of Perceived Organizational Support, COVID Organizational Support survey, and the Hospital Ethical Climate Scale. We found that general and COVID-related organizational support were predictors of moral distress after controlling for age, gender, working in an intensive care unit setting, and ethical climate. Findings support the need for a comprehensive strategy to address moral distress, including institutional efforts to convey support and commitment. Strategies moral distress may be experienced differently based on gender identity.
Introduction
The COVID-19 pandemic has increased concerns about healthcare clinicians’ mental health and well-being (Pearman et al., 2020). Exhaustion from the relentless demands on the healthcare system, inadequate resources, and ongoing risk of infection has magnified clinicians’ stress, depression, and anxiety (Pearman et al., 2020). Over the last 2 years, these realities have also drawn attention to clinicians impacted by morally distressing experiences (Sheather and Fidler, 2021).
Moral distress is the initial and lingering feeling that occurs when a clinician witnesses or participates in behaviors discordant with what they morally or ethically believe they should do (Jameton, 1984). Clinicians may be involved in situations with patients, team members, or in response to organizational action that constrains or prevent them from engaging in desired ethical actions (Epstein et al., 2019). For example, clinicians may perceive patient suffering due to misinformation, futile care, or simply not having enough staff to care safely for the patient (Epstein et al., 2019). Moral distress can occur from witnessing other professionals’ unethical behaviors, incompetence, or poor communication (Epstein et al., 2019). Clinicians may feel lingering feelings of frustration, anger, and guilt that can accumulate over time, thus creating higher baselines of moral distress in the future, termed the Crescendo Effect (Epstein and Hamric, 2009). As a result, differing situations may cause similar feelings and contribute to moral distress occurring at greater intensities or frequencies (Epstein and Hamric, 2009). Long-term impacts may result in burnout and depressive symptoms, further contributing to turnover and staffing shortages (Lamiani et al., 2017, 2018).
Moral distress research has primarily focused on nurses in hospital settings (Lamiani et al., 2017), and this has revealed that hierarchies and lack of decisional authority heighten feelings of powerlessness despite nurses’ high level of patient responsibility (Altaker et al., 2018; Baker et al., 2011; Huffman and Rittenmeyer, 2012). Powerlessness is a central component to experiencing moral distress, which exacerbates feelings of helplessness, frustration, and guilt (Lamiani et al., 2017). Personal characteristics such as age, years of experience, attitudes, and perceptions have also been identified as impacting the intensity of distress. If unaddressed, moral distress builds over time, as outlined by the Crescendo Effect, then there is likely to be a positive association between age, years of experience, and distress (Epstein and Hamric, 2009). However, past findings are inconsistent (Dodek et al., 2016; Lamiani et al., 2017), perhaps due to small, single-institution, non-random samples. In addition, how gender may be influential in experiencing or coping with distress has not often been considered (O’Connell, 2015). Most studies do not address gender, and few seek to understand the specific relationship between gender and moral distress; a few examples of inconsistent findings in studies involving imbalanced (too few men to analyze) samples exist. For instance, in a sample of 31 nurses in the US, there were significant differences with females having a higher overall moral distress score compared to males (O’Connell, 2015); however, two other studies failed to find similar results (Dodek et al., 2016; Epstein et al., 2019).
In addition to personal attributes, work factors affect how moral distress is experienced. Professional comparisons reveal nurses report higher moral distress levels than physicians (Dodek et al., 2016; Epstein et al., 2019; Lamiani et al., 2017). And those in intensive care units are especially at risk where triggering situations associated with moral distress may be common (e.g. withdrawing life-sustaining treatment, false hope, lack of care continuity) (Dodek et al., 2016; Lamiani et al., 2017). The nature of the work itself and the sociopolitical environment in which nurses operate cannot be disentangled from understanding the experience of moral distress.
Organizational climate is considered “member perceptions of organizational features like decision-making, leadership, and norms about work” (Stone et al., 2005: 468). The climate, cultivated by policies and actions or lack thereof, is consistently identified as a root factor contributing to situations of moral distress (Epstein et al., 2019; Lamiani et al., 2017). Many domains and subdomains such as supervision, group behavior, work design, rewards and training, make up a hospital’s organizational climate. Various measures exist intended to assess these dimensions, including a measure of ethical conduct and perceived support. A hospital’s ethical climate is supported when nurses are engaged in ethical decision-making and reflection, included in decisional processes, shown respect among and for colleagues, and supported in collaborative nurse-physician relationships (Olson, 1998). Researchers have extensively explored ethical climate and moral distress showing an inverse relationship where a better perceived ethical climate is associated with less moral distress (Lamiani et al., 2017). Perceived organizational support is another domain of organizational climate but has been less investigated (Robaee et al., 2018). Perceived organizational support is considered the degree to which an employee feels connected to and valued by the organization (Eisenberger et al., 1986; Olson, 1998). Per its conceptualization, a supportive climate is not developed solely from pay or benefits but whether the individual feels the benefits come from an organization that cares about their well-being. In this way, employees feel committed to their organization, have more job satisfaction, and thus are less likely to leave (Eisenberger et al., 1997). Systematic reviews (Baran et al., 2012; Schneider et al., 2021) and a meta-analysis (Kurtessis et al., 2017) indicate organizational support is a protective factor for psychological well-being and has strong negative relationships with burnout, emotional exhaustion, stress, absenteeism, and turnover. However, there have been few studies directly measuring organizational support and moral distress.
Emerging evidence around the utility of perceived organizational support as a predictor of moral distress is inconclusive. For example, perceived organizational support moderated the relationship between moral distress and anticipated turnover in a study by Maningo-Salinas (2010). In addition, a study of nurses working in Tehran, Iran, explored perceived organizational support and moral distress using random quota sampling to select nurses affiliated with a large hospital network (Robaee et al., 2018). They did not find a significant relationship, but limitations of the study, such as concerns regarding confidentiality perceived by participants, may have affected the results (Robaee et al., 2018). While scarce in quantitative studies, qualitative studies have long described the impact on nurses’ when they feel devalued, unappreciated, and left out (Huffman and Rittenmeyer, 2012).
Thus, perceived organizational support may be especially concerning as nurses grapple with uncertainty, risk, and fear during the pandemic. Hospital administrations’ responses to the COVID-19 pandemic and waves of critically ill and dying patients have created new and amplified sources of distress (Rosa et al., 2020; Silverman et al., 2021). A qualitative study of 31 nurses in a large academic medical system recently explored moral distress during the COVID-19 pandemic (Silverman et al., 2021). While some nurses relayed adequate support and consideration from their administrators, many nurses felt their “sacrifice” went unacknowledged (Silverman et al., 2021: 19). They cared for the overwhelming numbers of sick and dying patients without sufficient staff, and unsuccessful efforts to advocate for patients to have visitors intensified distress experienced (Silverman et al., 2021).
In past epidemics, nurses’ morale and job satisfaction were more affected than other professionals (Tolomiczenko et al., 2005). Nurses need timely and thorough communication, acknowledgment, emotional support, and adequate resources from their organizations (Fernandez et al., 2020). During the SARS crisis, Canadian nurses were surveyed about their experience, coping, and perceived organizational support (Marjanovic et al., 2007). Nurses reported less anger, improved trust, and less avoidant behavior with higher perceived organizational support. Past epidemics seem to emphasize the need to measure the impact of organizational support, and recently, there has been a strong desire to hold hospitals accountable in addressing moral distress (Epstein et al., 2020).
Our study aimed to examine if nurses’ experience of general and COVID-specific organizational support predicted moral distress controlling for the perceived ethical climate in their healthcare organizations, age, gender, and working in an intensive care unit. Ethical climate and intensive care unit settings have been consistently associated with moral distress, where poorer ethical support and working in an intensive care unit result in higher distress (Altaker et al., 2018; Dodek et al., 2016; Donkers et al., 2021; Epstein et al., 2019; Lamiani et al., 2017). We also controlled for gender; despite the inconsistent relationship found in previous studies (Dodek et al., 2016; Epstein et al., 2019), we wanted to account for any possible influence gender differences may have on moral distress.
Methods
Participants
This cross-sectional exploratory study utilized data from a non-random sample of registered nurses (RN) with an active license located in Kentucky who has worked in an inpatient hospital setting within the previous 6 months. A total of 401 eligible participants accessed the study and answered a portion of the survey. Of these, 248 completed all measures included in this analysis.
Participants were recruited from a large 1 academic hospital (569 beds) and affiliated (189 beds) community hospital, and an unaffiliated (75 beds) community hospital. The online questionnaire was open for 5 weeks from February 17, 2021 until March 24, 2021. 2 The survey was posted using URL links, QR codes, and snowball sampling techniques where stakeholders (e.g. nursing floor managers/supervisors), colleagues, and participants shared study links and information to engage more potential participants. The use of social media and snowball sampling has been a successful strategy and encouraged in previous survey research studies for hard-to-reach population groups (Dusek et al., 2015; Leighton et al., 2021). While beneficial, we are unable to provide a response rate. The end of the survey included a separate link for an opportunity to enter a draw to win one of ten $20 Amazon gift cards.
Sample size
Sample size and power were estimated a priori using power analysis software, G*Power (Faul et al., 2007), with typical benchmarks for multiple regression f2 values at 0.02, 0.15, and 0.35 (Cohen, 1988). Medium effect sizes have been found in moral distress studies with sample sizes ranging 100–300 using correlational and regression analysis (Christodoulou-Fella et al., 2017; Hiler et al., 2018). Using G*Power, F test linear multiple regression analysis with a total of five predictors, power was set at 0.95 and alpha at 0.05 was used to compute sample size (Faul et al., 2007). Calculated results indicated at least 107 participants would be needed to detect a medium effect size (f2 = 0.15).
Data collection and ethical considerations
The anonymous internet-based survey, comprised of psychometrically sound instruments and demographic questions, was sent using Qualtrics Software (Qualtrics, Provo, UT). Qualtrics provides survey protections to block search engines from indexing and prevent ballot box stuffing using cookies. Privacy and confidentiality were reinforced by using a secure link to protect participants’ responses and disabling the IP address tracking. Informed consent was provided with a cover letter without a required signature to ensure anonymity. Participants could end the survey at any point before submission. Participants provided their e-mail contact information in a separate secured link if they chose to enter the award drawing. The University of Kentucky institutional review board approved the study: 63690.
Variables and measures
Moral distress
The Measure of Moral Distress for Healthcare Professionals (MMD-HP) (Epstein et al., 2019) was used to measure moral distress. The MMD-HP measures the frequency and intensity of morally distressing scenarios at system, clinical, and team levels (Epstein et al., 2019). The MMD-HP gages the frequency and intensity of 27 morally distressing scenarios ranked using a five-point Likert-type scale. For how often a scenario is experienced, the scale ranges from 0 to 4 (0 = never, 1 = very rarely, 2 = occasionally, 3 = frequently, and 4 = very frequently). For how distressing the scenario was or would be, the scale also ranges 0–4 (0 = none, 1 = slightly, 2 = somewhat, 3 = moderately, 4 = very distressing). Hypothetical responses are in the event that participants had never experienced the listed scenario, but if they would, how distressing would it be. Example items are “Be required to care for more patients than I can safely care for” and “Witness health care providers giving ‘false hope’ to a patient and family.” We computed the MMD-HP composite score by multiplying each frequency score (0–4) by the intensity score (0–4) then summing each of those scores (frequency × intensity, 0–16) to result in a total moral distress score (0–432). Items that have never been experienced or are not seen as distressing do not contribute to the total moral distress score. Higher MMD-HP scores indicate greater levels of moral distress. There is no established metric associated with cut off scores for moral distress, thus, high and low scores are determined based on percentiles within the sample response. The reliability for this study, α = 0.93, reflects the reliability measured in previous studies using the MMDHP (Epstein et al., 2019).
Organizational support
Two measures were used to assess perceived organizational support, the COVID-19 Organizational Support (COVID-OS) and the Survey of Perceived Organizational Support (SPOS).
COVID-19 Organizational Support (COVID-OS)
The COVID-OS was developed to assess healthcare professionals’ perceptions of support and communication by hospital administration during the COVID-19 pandemic (Zhang et al., 2020). In its original presentation, the COVID-OS consisted of eight questions on a 7-point Likert scale ranging from 1) strongly disagree to 7) strongly agree with items 2, 4, and 8 reverse coded (Zhang et al., 2020). In our study, the scale displayed as a 5-point Likert scale ranging from 1) strongly agree to 5) strongly disagree. We transformed the points to reflect the original 7-point Likert structure following recommendations by Dawes (2008) and IBM SPSS (2020a) algorithm. Example items are, “I am uncertain my organization would take care of my own needs (e.g. personal and family) if I get COVID-19” and “I feel I lack access to up-to-date information and communication from the healthcare system.” The COVID-OS was used as a total score calculated by finding the average of all items with a final score of 1–7. Higher scores reflect better quality of perceived support. The COVID-OS is a newly designed instrument with minimal psychometric testing, thus there is an absence of reliability testing published. However, the current study demonstrated a Cronbach’s alpha at 0.67, which is considered minimally acceptable for exploratory research (Ursachi et al., 2015).
Survey of Perceived Organizational Support (SPOS)
The SPOS assesses employees’ perception of their organization’s support and commitment to them (Eisenberger et al., 1986). The shorter 8-item version has been encouraged and is commonly used (Eisenberger et al., 1986; Worley et al., 2009). The 8-item SPOS used in this study was based on a 5-point Likert scale ranging from 0) strongly agree to 4) strongly disagree (items 2, 3, 5, and 7 are reverse-coded prior to computing the final scale). Example items include “the organization really cares about my well-being” and “the organization takes pride in my accomplishments at work.” The SPOS total score was computed by finding the average of the eight items, with a total possible score of 0–4. Higher scores indicate more perceived organizational support. The 8-item SPOS is a unidimensional measurement and has demonstrated convergent and discriminant validity as well as good reliability (α = 0.90) (Eisenberger et al., 1997; Lynch et al., 1999). Cronbach’s alpha for the current study is α = 0.92.
Demographic characteristics
The study included several measures for personal and professional characteristics. Personal characteristics included age (in years), education, ethnicity (African-American/Black, Asian, Caucasian/White, Hispanic/White, Hispanic Non-white, Native American or Alaskan Native, Native Hawaiian or other Pacific Islander, Other), and gender (female, male). Professional characteristics included work environment (intensive care (ICU)/non-ICU), employment status (full-time, part-time, PRN), years of nursing experience, primary patient population, and currently working with COVID patients (Yes/No).
Ethical climate
The Hospital Ethical Climate Scale (HECS) measures hospital ethical climate as perceived by nurses (Olson, 1998). The 26-item scale was based on a 5-point Likert-type scale, 1 = almost never true and 5 = almost always true, where higher scores indicate a more positive perception of ethical climate. HECS was used for its total score computed by finding an average of items with a possible range from 1 to 5. Example items include “hospital policies help me” and “conflict dealt with openly.” The survey has been shown to have construct, convergent, and discriminant validity with a reliability of α = 0.91 (Olson, 1998). Cronbach’s alpha for the current study is α = 0.95.
Analytic plan
Missingness analysis was conducted and determined the data were missing at random (Mertler and Reinhart, 2017). All statistical analyses were conducted using the computer statistics package SPSS Version 27 (IBM, 2020b). Descriptive statistics are provided with bivariate correlations as well as independent sample t-tests to examine group differences. Hierarchical linear regression analysis was conducted to address study aims. Regression analysis adjusted for covariates (age in years, gender, ICU/non-ICU or not specified, HECS). Based on previous literature and theory, we anticipate a positive relationship between age, working in the ICU, and being female, whereas better hospital ethical climate will be associated with a negative relationship. No substantial violations of assumptions, including homoscedasticity, absence of multicollinearity, and normal distribution of residuals, were observed.
Results
Descriptive statistics and bivariate analyses
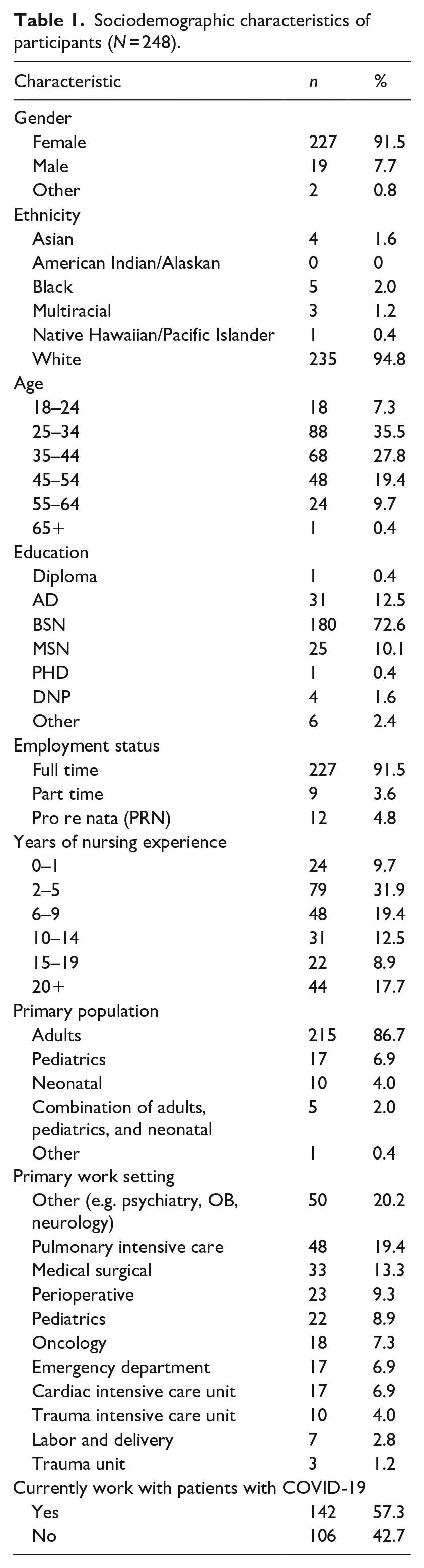
The sample was primarily White (94.8%), female (91.5%), and most had a baccalaureate degree (72.6%). Most participants were between 25 and 34 years old (35.5%) with 2–5 years of experience (31.9%). Participants mostly worked full time (91.5%) with adult populations (86.7%) in non-ICU settings (57.9%). The top three work settings were (1) other unit settings (e.g. psychiatry, procedural, OB) (20.2%), (2) pulmonary intensive care units (19.4%), and (3) medical-surgical (13.3%). Out of the 248 participants, roughly over half worked directly with patients with COVID-19 at the time of the survey (57.3%). Participant characteristics can be seen in Table 1. The sample population reflects the population of nurses in Kentucky, who are also predominately female (90.9%), White (92.6%), with a baccalaureate (37.9%) or associate degree (38%) in nursing (Kentucky Board of Nursing, 2021a, 2021b, 2021c). The majority of nurses in this sample had a Bachelor of Science in Nursing (n = 180).
Sociodemographic characteristics of participants (N = 248).
Organizational support
Perceived organizational support (SPOS) ranged 0–4 (M = 1.60 ± 1.03) and COVID-19 specific support ranged 1.56–7 (COVID-OS) (M = 4.14 ± 1.01).
Moral distress
Total moral distress scores ranged from 0 to 368 (M = 136.24 ± 76.66). Independent samples t-tests showed statistically significant differences in moral distress scores for some nurse groups. Nurses with a BSN (t (246) = 2.16), those working in ICU settings (t (246) = −3.47), and those who are currently working with COVID patients (t (246) = 3.54) or had worked with COVID patients (t (246) = 3.07) had significantly higher moral distress scores than their counterparts who did not.
Results of the bivariate correlations supported a significant negative correlation between moral distress and age (r (246) = −0.24, p ⩽ .001), ethical climate (r (246) = −0.39, p ⩽ 0.001), perceived organizational support (r (246) = −0.59, p ⩽ 0.001), and COVID-19 specific support (r (246) = −0.52, p ⩽ 0.001). There was a significant positive association for those who worked in an intensive care setting (r (248) = 0.22, p ⩽ 0.001). Gender was not significantly associated with any variable, including moral distress. Descriptive statistics and bivariate correlations for the regression analysis can be seen in Table 2.
Descriptive statistics and correlations for regression variables (N = 248).
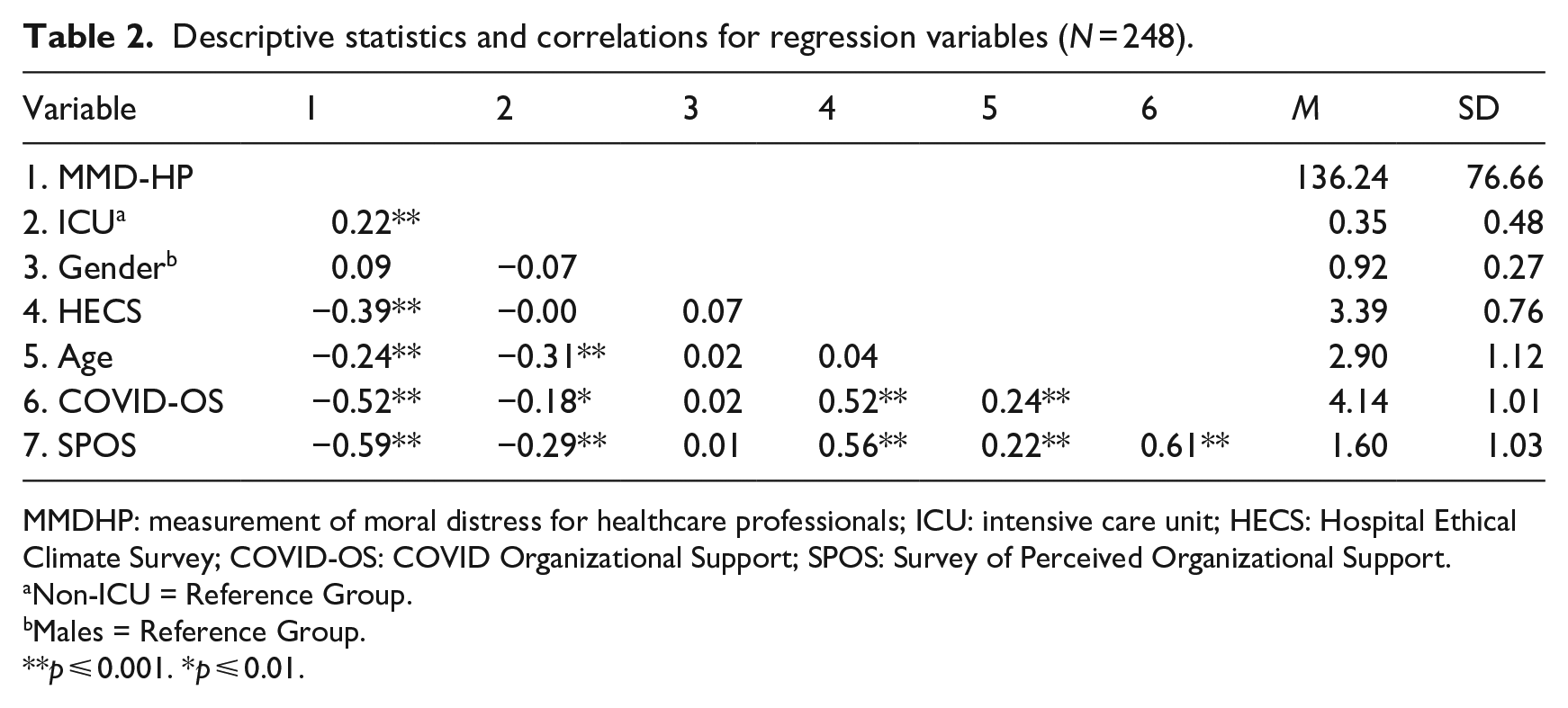
MMDHP: measurement of moral distress for healthcare professionals; ICU: intensive care unit; HECS: Hospital Ethical Climate Survey; COVID-OS: COVID Organizational Support; SPOS: Survey of Perceived Organizational Support.
Non-ICU = Reference Group.
Males = Reference Group.
p ⩽ 0.001. *p ⩽ 0.01.
Regression analysis
To address the primary aim of the study, hierarchical-multiple regression was used to examine the organizational support measures (COVID-OS and SPOS) as predictors of moral distress (MMD-HP), after controlling for the influence of influence of ICU setting, gender, hospital ethical climate (HECS) and age. Control variables ICU setting (β = 0.17, p ⩽ 0.01), gender (β = 0.13, p ⩽ 0.05), HECS (β = −0.39, p ⩽ 0.001), age (β = −0.17, p ⩽ 0.05) and were entered at Step 1, explaining 24% of the variance in moral distress (F (4, 243) = 9.38, p ⩽ 0.001). As expected, working in an ICU setting was associated with significantly higher levels of moral distress and higher HECS scores and older age were associated with lower MMD-HP scores. Gender was also a significant predictor, with higher levels of moral distress associated with female gender.
After entry of SPOS and COVID-OS scales at Step 2, the total variance explained by the model was 41%, F (2, 241) = 27.81, p ⩽ 0.001. Controlling for influence of ICU setting, gender, HECS, and age, the inclusion of the organizational support measures explained an additional 17% of the variance in moral distress F (2, 243) = 34.12, p ⩽ 0.001. See Table 3 for regression analysis coefficients and model summary statistics.
Hierarchical regression results for moral distress (N = 248).
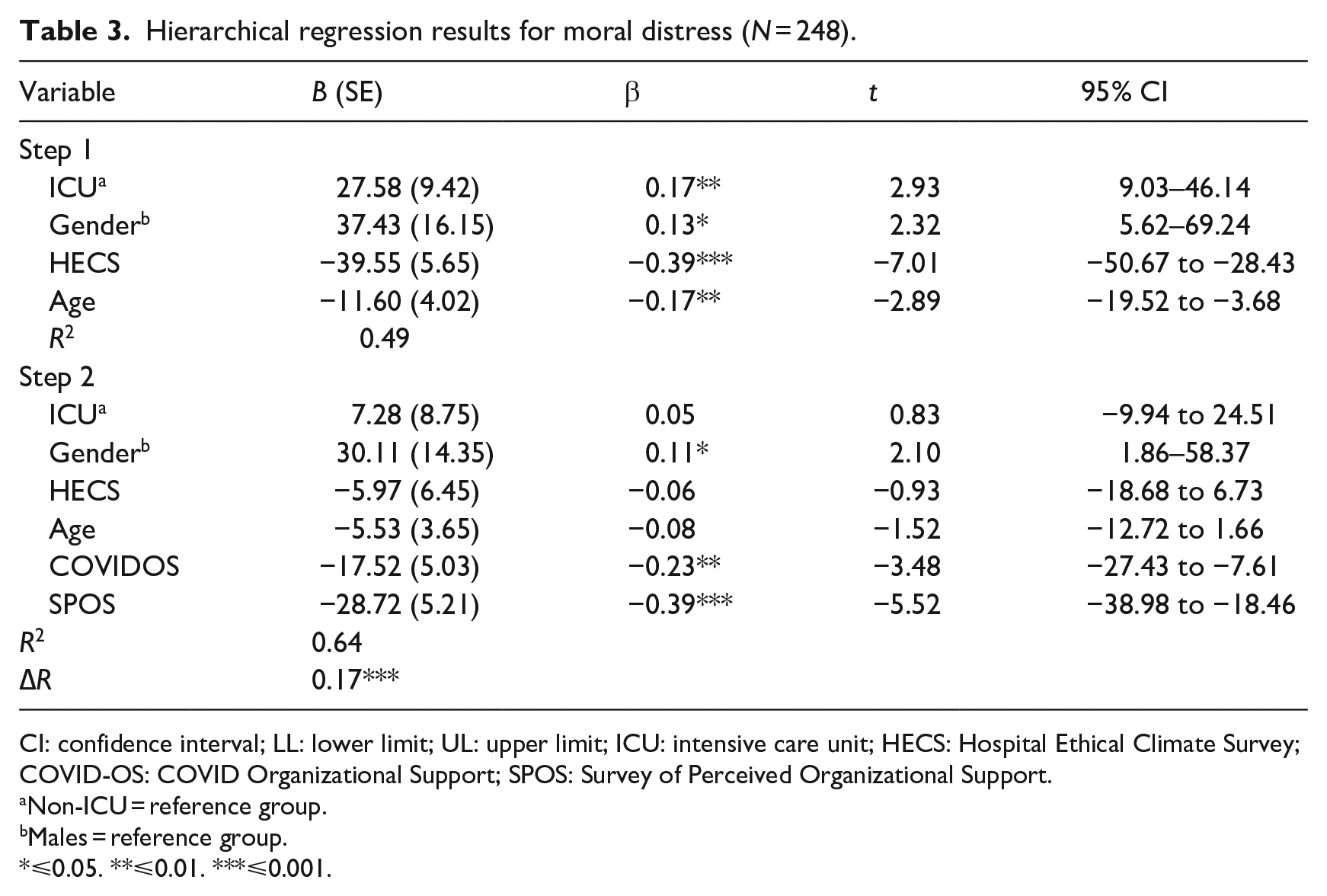
CI: confidence interval; LL: lower limit; UL: upper limit; ICU: intensive care unit; HECS: Hospital Ethical Climate Survey; COVID-OS: COVID Organizational Support; SPOS: Survey of Perceived Organizational Support.
Non-ICU = reference group.
Males = reference group.
⩽0.05. **⩽0.01. ***⩽0.001.
In the second step, both predictor variables were statistically significant with SPOS being the strongest predictor (b* = −0.38, p ⩽ 0.001). Moral distress decreased 28.72 points for every 1-point increase in SPOS. For every 1-point increase in COVID-OS, moral distress decreased by 17.52 points. In the full model, other than gender, the control variables were no longer significant: ICU setting (β = 0.05, p = 0.41), HECS (β = −0.06, p = 0.36), and age (β = −0.08, p = 0.13). Gender remained a significant predictor (β = 0.11, p < 0.05); compared to males, females scored 30.11 points higher on the MMDHP.
Discussion
Findings from this study provided support for the relationship between perceived organizational support and moral distress during the pandemic. Past studies have indicated the lack of necessary resources (e.g. staffing, equipment, supplies) and ethical climate are meaningful predictors of moral distress (Lamiani et al., 2017). This study adds that in addition to the need for adequate supplies and engaging in ethical debate, the degree to which nurses feel cared for and supported by their organization is crucial. Available resources and supplies may be a component of organizational support, but as Eisenberger et al. (1986) describe, feeling supported is more than salary, resources, and awards. This finding builds on Stone et al. (2005) work of building an integrative model of organizational climate, providing additional detail as to the strength of the related domains and subdomains as it pertains to staff’s well-being.
Our findings align with past qualitative data (e.g. Silverman et al., 2021) but differ from quantitative studies that included measurements of perceived organizational support (Maningo-Salinas, 2010; Robaee et al., 2018). Congruent with qualitative research, organizations must demonstrate caring and inclusive behaviors to mitigate moral distress (Huffman and Rittenmeyer, 2012). Therefore, it is perplexing that the two published quantitative studies measuring perceived support failed to find a significant predictive relationship with moral distress. The negative findings may be due to small sample sizes and measurement error, or it may be that the COVID-19 pandemic has elevated the importance of feeling heard, seen, and appreciated. Our data collection occurred immediately following the first peak of cases during the COVID-19 pandemic; therefore, our findings may reflect the impact of the COVID-19 pandemic on nurses’ experiences. Continued research into nurses and other healthcare professionals’ experiences during and after COVID-19 may offer further insight into these relationships.
In the current study, moral distress scores were higher than past studies conducted before the COVID-19 pandemic (Epstein et al., 2020; Latimer et al., 2021). In previous samples, including nurses who care for patients with a left ventricular assisted device (LVAD) and nurses who were hospital-based, the average score was 126 (Latimer et al., 2021) and 112 (Epstein et al., 2020), respectively. Findings from our study reflect higher moral distress scores and still may not reflect all the sources of moral distress, including those created by the pandemic. For example, nurses either had to accept the higher risk of personal infection or exposing their families or alternatively choose to leave their assignment or position (Cacchione, 2020). While not directly measured as a source of distress in the current study, caring for patients while navigating visitor restrictions, absent or insufficient personal protective equipment, or being staffed in or working with nurses outside usual departments may have posed considerable constraints (Silverman et al., 2021). These realities may have exacerbated familiar sources of distress (e.g. end-of-life care, team communication breakdowns) and resulted in an increased need to feel supported. Unfortunately, it may also be why organizations provide less support, as they are also managing complex and uncertain conditions with their own risk and fears (Silverman et al., 2021).
Our study supports that gender is a crucial consideration for understanding moral distress among nurses, and our findings are consistent with O’Connell’s (2015) study where females had higher moral distress than their male coworkers. However, this is not a typical result, as Epstein et al. (2019) nor Dodek et al. (2016) found gender differences. Notably, few studies include gender as a focus of their research or included in their methodology, a considerable limitation. In a 2019 report of over 2537 nurses and nurse-midwives from 117 countries with supporting literature and in-depth interviews with nurse leaders, it is estimated that despite the nursing profession is over 70% female, only 25% hold leadership positions (Newman et al., 2019). Hospital hierarchies can inhibit nurses’ decision-making abilities despite gender (Newman et al., 2019). Still, the reality is that over 70% of the US hospital workforce is female, yet males possess the majority of higher paid and status roles (World Health Organization, 2019). Our understanding of moral distress may be improved by exploring interactions between gender and power in hospital structures. This interaction may also explain the professional differences found between nurses and physicians, where most physicians are male (World Health Organization, 2019). Furthermore, even when women hold positions of power or status, they face stereotyping and bias which undermine their positions of authority and may contribute to less sense of power over decision-making and influence and thus more distress (Newman et al., 2019; World Health Organization, 2019).
Limitations
Our study contributes meaningfully to the literature on moral distress but is not without limitations. Measurement errors due to social desirability, recall bias, selection bias, and instrumentation can potentially affect the findings’ reliability. Additionally, results regarding COVID-specific support should be interpreted with caution, given the marginal reliability coefficient for the COVID-OS instrument (α = 0.67). While acceptable, reliability was lower than the other measurements used; however, the measure still provides meaningful information about what is important to nurses during the COVID-19 pandemic. Generalizability is also specific to the sample studied. For instance, the sample consisted of almost twice as many participants with BSN degrees compared to other education groups, which may have influenced the study findings. This study’s sample was also predominately White females, while reflective of the Commonwealth’s demographics, nurses of color may experience moral distress and subsequent adverse outcomes differently. Studies examining whether non-white nurses have higher levels of moral distress are limited, but one study found ethnicity significantly predicted moral distress in a sample of 238 nurses (82% White, 18% other) (Altaker et al., 2018). Longitudinal studies and samples with more diversity (e.g. gender, ethnicity, language) are necessary to improve our understanding how persons who may have experienced multiple layers of disenfranchisement experience and cope with moral distress. Lastly, study integrity may have been compromised as there was no full-proof way to ensure non-RN respondents participated. While we included screening questions and embedded Qualtrics tools to prevent ballot stuffing, it is possible participants were deceitful in the number of times they took the survey or about who they were. Studying moral distress remains a priority for research into the future.
Conclusions
Instruments used in this study provide reasonable ways to assess the workforce climate and determine whether hospital organizations are adequately supporting nurses and other healthcare professionals. Nurses’ priorities and needs may have changed since the onset of the COVID-19 pandemic, as nurses make sense of what has happened; the need to feel they mattered may be more critical now (Epstein et al., 2020). Asking, affirming, assessing and acting, the four A’s of moral distress, have been a longstanding recommendation by the American Association of Critical-Care Nurses for nurse leadership (Rushton, 2006). Incorporating additional elements of concern related to feeling heard, appreciated, and understood may be beneficial in future interventional strategies. Additionally, our study highlights the undeniable influence of organizational structures, procedures, and behaviors on moral distress.
Organizational and administrative policy should be examined and refined to create a supportive climate (Epstein et al., 2020). Existing narratives have focused on individual responsibility for self-care and preventing long-term adverse outcomes like depression and burnout; however, there must be a shared responsibility from each level of the organization. While hospitals intended to create a caring narrative by calling their workforce heroic and honoring their sacrifices, when nurses feel unable to do their best, they may not feel like a hero which further contributes to guilt and shame (Silverman et al., 2021). Nurse managers, too, struggle with their sources of moral distress (Nasrabadi et al., 2018); therefore, healthcare organizations must develop a comprehensive strategy to ensure that nurses feel included and valued beyond the hero discourse (Epstein et al., 2020; Mohammed et al., 2021). Administrative action by creating spaces and time, such as online or in-person debriefing, can help answer the need for camaraderie and grief expression (Silverman et al., 2021). The use of committees comprised of administration, management, and staff may be an effective way to identify needs, promote communication, and engage in effective partnerships.
Students, newly graduated and practicing nurses will benefit from strategies to navigate moral distress. Education needs to include methods to empower nurses to engage in policy development and hold organizations accountable in their relationship toward a healthier work climate (Epstein et al., 2020). Nurses across levels of preparedness could benefit from understanding the complexities that contribute to organizational climate and relate this to the many layers of entwinement where moral distress can occur.
Research Data
sj-sav-2-hpq-10.1177_13591053221111850 – for Moral distress during COVID-19: The importance of perceived organizational support for hospital nurses
sj-sav-2-hpq-10.1177_13591053221111850 for Moral distress during COVID-19: The importance of perceived organizational support for hospital nurses by Abigail L Latimer, Melanie D Otis, Gia Mudd- Martin and Debra K Moser in Journal of Health Psychology
Research Data
sj-sps-1-hpq-10.1177_13591053221111850 – for Moral distress during COVID-19: The importance of perceived organizational support for hospital nurses
sj-sps-1-hpq-10.1177_13591053221111850 for Moral distress during COVID-19: The importance of perceived organizational support for hospital nurses by Abigail L Latimer, Melanie D Otis, Gia Mudd- Martin and Debra K Moser in Journal of Health Psychology
Research Data
sj-spv-3-hpq-10.1177_13591053221111850 – for Moral distress during COVID-19: The importance of perceived organizational support for hospital nurses
sj-spv-3-hpq-10.1177_13591053221111850 for Moral distress during COVID-19: The importance of perceived organizational support for hospital nurses by Abigail L Latimer, Melanie D Otis, Gia Mudd- Martin and Debra K Moser in Journal of Health Psychology
Research Data
sj-txt-4-hpq-10.1177_13591053221111850 – for Moral distress during COVID-19: The importance of perceived organizational support for hospital nurses
sj-txt-4-hpq-10.1177_13591053221111850 for Moral distress during COVID-19: The importance of perceived organizational support for hospital nurses by Abigail L Latimer, Melanie D Otis, Gia Mudd- Martin and Debra K Moser in Journal of Health Psychology
Footnotes
Acknowledgements
We want to acknowledge and express appreciation for faculty and staff who provided guidance and support for this study as a part of Dr. Latimer’s social work dissertation (Latimer, 2021).
Data sharing statement
The current article is accompanied by the relevant raw data generated during and/or analysed during the study, including files detailing the analyses and either the complete database or other relevant raw data. These files are available in the Figshare repository and accessible as Supplemental Material via the SAGE Journals platform. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. However, during the writing of this manuscript the primary author was a post-doctoral scholar funded on Patient Centered Outcomes Research Institute (PCORI) contract # AD-2019C3-17982, Online Cognitive Behavioral Therapy for Depressive Symptoms in Rural Patients with Coronary Heart Disease.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.