
Abstract
According to the motivated helplessness hypothesis, parental feelings of helplessness regarding vaccinating children against COVID-19 may serve a protective function against vaccine fear and hesitancy. Two correlational studies conducted among Israelis (Study 1) and an international sample (Study 2), examined whether self-reported perceived helplessness in vaccinating children may be related to lower vaccine-fear, and higher perceived vaccine-effectiveness, trust in authorities’ recommendations and willingness to vaccinate. Results indicated parents who felt they had no other choice but to vaccinate their children, exhibited less vaccine-fear, higher vaccine-effectiveness and greater intentions to vaccinate. Additionally, the relationships between vaccine-helplessness, vaccine-effectiveness and willingness to vaccinate were partially mediated by vaccine-fear. In Study 2, vaccine-helplessness was found related to higher trust in authorities’ recommendations, which was partially mediated by vaccine-fear. The implications of these findings for research on the psychological function of helplessness in the parental decision-making process of vaccinating children during a pandemic are discussed.
The COVID-19 pandemic has led to millions of deaths worldwide (World Health Organization [WHO], 2022) and tremendous psychological trauma (e.g. Robinson et al., 2022; Salari et al., 2020). In an expedited effort to combat pandemic’s destructive consequences, new vaccines have been developed (e.g. Pfizer-BioNTech), and, from December 2020, countries began to administer vaccines to the adult population (Mathieu et al., 2021). During May and June 2021, global health agencies expanded their emergency recommendations for administering COVID-19 vaccines in children 12–15 years of age (e.g. Food and Drug Administration [FDA], 2021; WHO, 2021). 1 Shortly thereafter, countries around the world started vaccinating 12–15 year old children. These efforts, however, met with considerable amount of parental fear and hesitancy regarding vaccine’s effectiveness and its possible side effects (Akarsu et al., 2021; Bell et al., 2020; Liu et al., 2022; Pan et al., 2021; Walker et al., 2021).
According to the motivated helplessness hypothesis (Lifshin et al., 2020), people can lessen their fear and hesitancy by thinking that they have no other choice but to vaccinate their children. If caregivers feel helpless in this decision, they may be freed from the fears and worries regarding vaccine’s efficacy and its possible side effects, and therefore more willing to vaccinate their children. The current research was designed to test this hypothesis.
Vaccine hesitancy, a delay or refusal of vaccines despite their availability, was declared by the WHO as a ‘top 10’ global health threat (WHO, 2019). Parents, especially of young children, seem to be more hesitant towards vaccination compared to non-parents (e.g. Funk, 2017; Simonson et al., 2021). Studies show that although the intention to vaccinate oneself against COVID-19 correlates strongly with the intention to vaccinate one’s children (e.g. Brandstetter et al., 2021; Liu et al., 2022; Teasdale et al., 2021), caregiver’s willingness to vaccinate their children is generally lower than their willingness to vaccinate themselves (Pan et al., 2021). A nationally representative U.S. study from April 2021 revealed that only 29% of parents were intending to vaccinate their child against COVID-19 (Hamel et al., 2021).
Vaccine hesitancy is a multifactorial phenomenon (Damnjanović et al., 2018). The most common reasons for parental hesitancy in vaccinating children against COVID-19 were concerns about vaccine safety, fear of possible side effects and low perceived vaccine-effectiveness (Bell et al., 2020; Evans et al., 2021; Liu et al., 2022; Pan et al., 2021; Pippert et al., 2021). In regard to perceived vaccine-effectiveness, caregivers were worried about the reliability of the new vaccine (e.g. Akarsu et al., 2021) and sceptical about whether it would be efficient in preventing the disease and its future variants (e.g. Walker et al., 2021). Parents also worried that the vaccine development process was too rapid, not allowing enough time for adequate testing to confirm its safety (e.g. Bell et al., 2020), and that the vaccine might induce severe unknown short and long term side effects (e.g. Evans et al., 2021; Pippert et al., 2021). Importantly, these hesitating caregivers are not anti-vaccines in general, but rather worried parents who are facing an important, yet difficult decision in the effort of protecting their child’s health during a pandemic.
Caregivers might be under serious psychological pressure to make the right decision about administering COVID-19 vaccine to their children. How can caregivers overcome their vaccine-related fear and hesitancy? One possibility is that if caregivers perceive themselves as helpless in the decision to vaccinate their children, then they won’t have to worry about the possible negative consequence of their decision, and therefore may be more willing to vaccinate their children. This possibility is proposed by the motivated helplessness hypothesis (Lifshin et al., 2020), which posits that a sense of helplessness in coping with threats in specific domains can serve an anxiety-buffering function, and protect people from experiencing fear, anxiety, guilt or threats to self-esteem. Thus far the motivated helplessness hypothesis was directly tested in three published studies, indicating that high perceived helplessness to avoid COID-19 infection protected people from COVID-19 related fears and state-anxiety (Lifshin and Mikulincer, 2021; Lifshin et al., 2020, 2022). Furthermore, reduced fear of being infected subsequently related to lower motivation for taking protective actions against COVID-19 (Lifshin et al., 2020).
On this basis, it is reasonable to assume that parents’ feelings of helplessness regarding the decision to vaccinate their children (‘vaccine-helplessness’) would also lessen fears and hesitancy with regard to vaccination (‘vaccine-fear’) and may therefore upturn their willingness to vaccinate their children against COVID-19. The prediction was that higher vaccine-helplessness among parents would be related to less vaccine-fear, which, in turn, would be associated to higher perceived ‘vaccine-effectiveness’ and more willingness to vaccinate. Following previous research (Lifshin et al., 2020, 2022), the curvilinear relationship between helplessness and fear in which both a high efficacy and high vaccine-helplessness would relate to lower vaccine-fear compared to moderate vaccine-helplessness was examined. The mediational effect of vaccine-fear in the relationship between vaccine-helplessness, perceived vaccine-effectiveness and willingness to vaccinate children was also tested.
In addition, child’s age and health were measured as potential covariates, as parents of younger children and of those who may have health problems could influence parents decision to vaccinate their children (e.g. Goldman et al., 2020). Additionally, parents’ own vaccination status was measured as it might also affect attitudes and intentions in vaccinating children. Lastly, the hypothesis that high vaccine-helplessness would be associated with high trust in recommendations of the government and the WHO in dealing with COVID-19 was tested. It was expected that higher vaccine-helplessness may also assuage concerns regarding the reliability of authority’s recommendations.
These hypotheses were tested in two preregistered Studies. Study 1 (preregistration: https://aspredicted.org/blind.php?x=DBM_V97), was conducted in Israel. Study 2 (preregistration: https://aspredicted.org/49H_GK6), was an international study (with samples with adequate power among Americans, Australians, British and Canadians). The Studies were approved by the Institutional Review Board (IRB) at the IDC Herzliya. Ethical clearance number: P_2021131 and followed the guidelines set forth by the APA’s Ethical Principles of Psychologists and Code of Conduct Standard 8 (http://www.apa.org/ethics/code/index.aspx).
Study 1
Study 1 was conducted in Israel during June-August of 2021, 3 weeks into the Israeli campaign for vaccinating 12–15 years old children against COVID-19 (Efrati, 2021), when discussions about vaccination among Israeli caregivers were highly salient.
Method
Participants
An invitation to participate in a study about ‘attitudes towards COVID 19 vaccine’ was posted in online on Facebook groups/pages related to COVID-19 and on an Israeli surveys reddit page (r/surveys_in_hebrew). Hebrew-speaking parents (any parent who has a child regardless of child’s age) were invited to participate voluntarily. An a priori power analysis using G*Power (Faul et al., 2007) indicated that detecting a small-to medium effect (f2 = 0.05) in a multiple hierarchical regression with R2 increases that includes one tested predictors (the quadratic term of vaccine-helplessness) and seven total predictors (the linear term and other potential covariates) would require 159 participants.
Twenty-eight participants who (1) had missing data on key variables; (2) reported not completing the study seriously 2 ; (3) reported that their child was infected by the COVID-19 (n = 17) were removed. The final sample included 162 participants (116 women, 43 men and 2 who reported a different gender). Age ranged from 19 to 69 years (M = 42.56, SD = 9.18, Mdn = 41). A sensitivity analysis using G*Power (Faul et al., 2007) indicated that a small effect size could be detected in the entire sample (f2 = 0.005) at 80% power.
Materials and procedure
All materials for this study were in Hebrew. After consenting, participants completed four short measures in counterbalanced order: parent’s vaccine-helplessness (four items, e.g. ‘I have no choice but to vaccinate my children against the COVID-19’; Supplemental Appendix 1), vaccine-fear (four items, e.g. ‘In general, how much are you afraid of vaccinating your children against the COVID-19’; Supplemental Appendix 2), perceived vaccine-effectiveness (five items, e.g. ‘The vaccine against COVID-19 virus is good and effective’; Supplemental Appendix 3) and caregiver’s willingness to vaccinate their children (three items, e.g. ‘If today the World Health Organization would permit the COVID-19 vaccine for children, I would vaccinate my children’; see Supplemental Appendix 4). All responses were rated using a seven-point scale (1 = Strongly disagree, 7 = Strongly agree). Cronbach Alphas for all scales ranged from 0.82 to 0.97 (see Ms, SDs and bivariate correlations in Table S1 in Supplemental Material). Next participants were asked about their personal vaccination against COVID-19 (‘Have you been vaccinated against COVID-19 virus?’; Yes/No), and their children COVID-19 infection status (‘Did one of your children got infected by COVID-19 virus’?; Yes/No), as well as a question about their children’s general health (‘In general, is your child a healthy child?’; 1 = not at all healthy, 7 = very healthy). Last participants answered demographic questions regarding their age, gender, education, marital status, residential area, religion, religiosity and political orientation (1 = very right wing, 7 = very left wing).
Results
To test our main hypothesis, the linear and curvilinear contribution of vaccine-helplessness to vaccine-fear, perceived vaccine-effectiveness and willingness to vaccinate, was examined in three hierarchical regression analyses (a separate analysis for each measure). The first step of the regressions included potential statistically covariates. The second step included the mean-centred measure of vaccine-helplessness, representing the linear term. The third step, included the quadratic term of the vaccine-helplessness measure to test for the curvilinear relationship (see Table 1).
Regression analyses predicting vaccine-fear, perceived vaccine effectiveness and willingness to vaccinate as a function of the linear and quadratic terms of vaccine helplessness (N = 159).
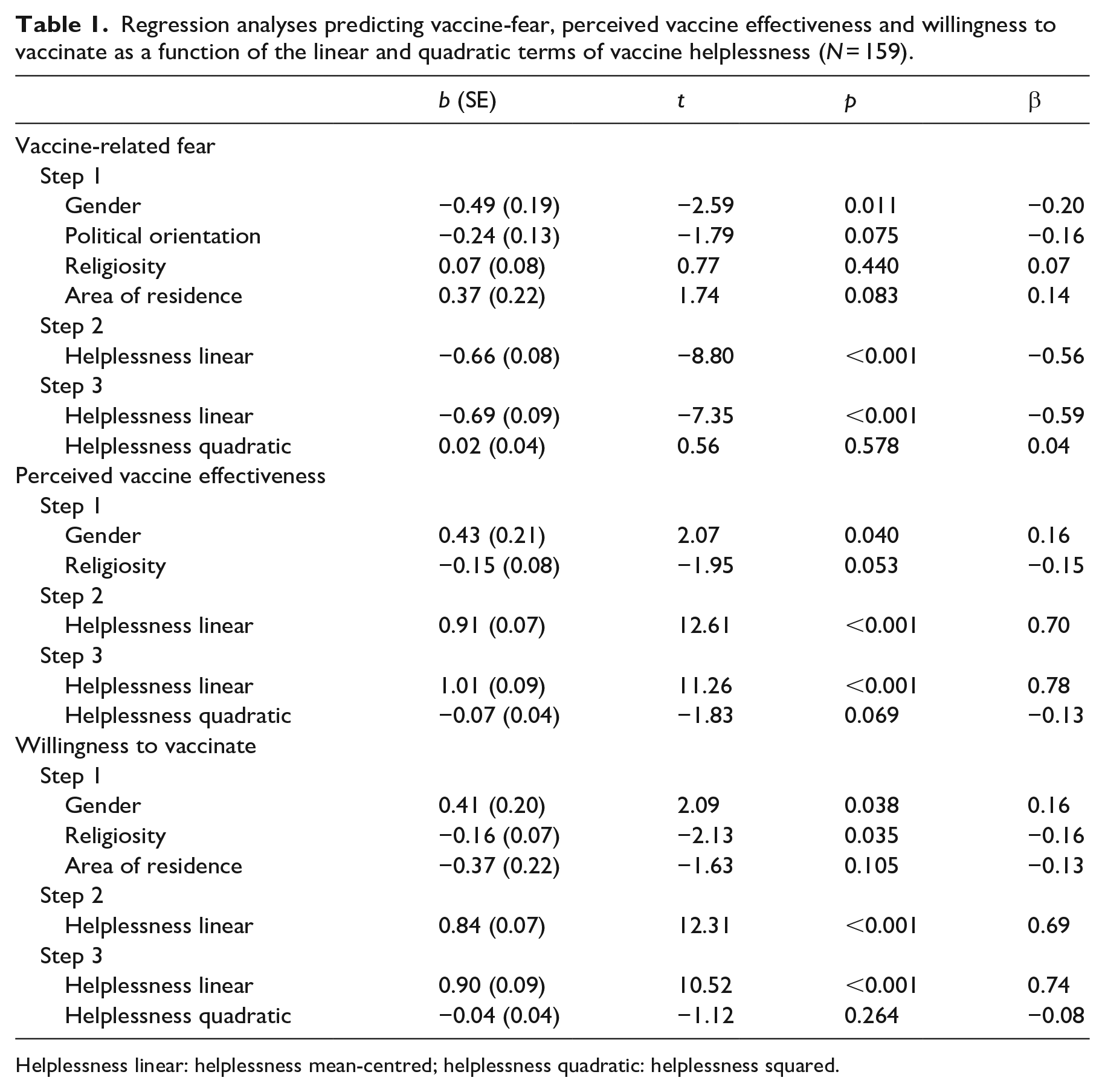
Helplessness linear: helplessness mean-centred; helplessness quadratic: helplessness squared.
The analysis for vaccine-fear indicated that the regression’s first step containing participants’ gender, political orientation, religiosity and residential area was statistically significant, F(4, 154) = 4.54, p < 0.01, R2 = 0.11, R2Adj = 0.08. The second step was also significant, ΔF(1, 153) = 77.40, Δp < 0.001, ΔR2 = 0.30, R2Adj = 0.39, as higher parents vaccine-helplessness was significantly associated with less vaccine-fear, b = −0.66, β = −0.56, t(153) = −8.80, p < 0.001. The third step including the quadratic vaccine-helplessness term was not statistically significant, ΔF < 1, Δp = 0.578 (see Figure S1 in the Supplemental Material).
The regression for perceived vaccine-effectiveness revealed that the first step (containing gender and religiosity) was statistically significant, F(2, 156) = 4.39, p < 0.05, R2Adj = 0.041. The second step was also significant, ΔF(1, 155) = 159.02, Δp < 0.001, ΔR2 = 0.479, R2Adj = 0.524, as higher helplessness significantly predicted higher perceived vaccine-effectiveness, b = 0.91, β = 0.70, t(155) = 12.61, p < 0.001. The third step including the quadratic term was only approaching statistical significant, ΔF(1, 154) = 3.36, Δp = 0.069, ΔR2 = 0.010, R2Adj = 0.531 (see Figure S2 in the Supplemental Material).
The regression for willingness to vaccinate revealed that the first step (containing gender, religiosity and residential area) was statistically significant, F(3, 155) = 4.61, p = 0.004, R2Adj = 0.064. The second step was also significant, ΔF(1, 154) = 151.58, Δp < 0.001, ΔR2 = 0.455, R2Adj = 0.525, as higher vaccine-helplessness significantly predicted more willingness to vaccinate, b = 0.84, β = 0.69, t(154) = 12.31, p < 0.001. The third step including the quadratic term was not statistically significant, ΔF(1, 153) = 1.26, Δp = 0.264 (see Figure S3 in the Supplemental Material).
Mediation analyses
The mediating role of vaccine-fear in the relationship between vaccine-helplessness on perceived vaccine-effectiveness and willingness to vaccinate was tested using model 4 in PROCESS (Hayes, 2012, version 3.2) with 10,000 bootstrapping resamples. The mean-centred measure of vaccine-helplessness was entered as predictor, vaccine-fear (mean-centred) as the mediator and perceived vaccine-effectiveness and willingness to vaccinate as outcomes. Mediation results are presented in Tables S3 and S4 in the Supplemental Material.
In the analysis predicting vaccine-effectiveness (controlling for gender, political orientation, religiosity and residential area), vaccine-helplessness related to higher perceived vaccine-effectiveness, b = 0.47, t = 7.18, p < 0.001, and vaccine-fear was related to lower vaccine-effectiveness, b = −0.66, t = −11.43, p < 0.001. As expected, there was a statistically significant positive indirect effect, as the relationship between vaccine-helplessness on perceived vaccine-effectiveness was mediated by vaccine-fear Meffect = 0.43, 95% CI [0.308, 0.574] (see Figure 1).
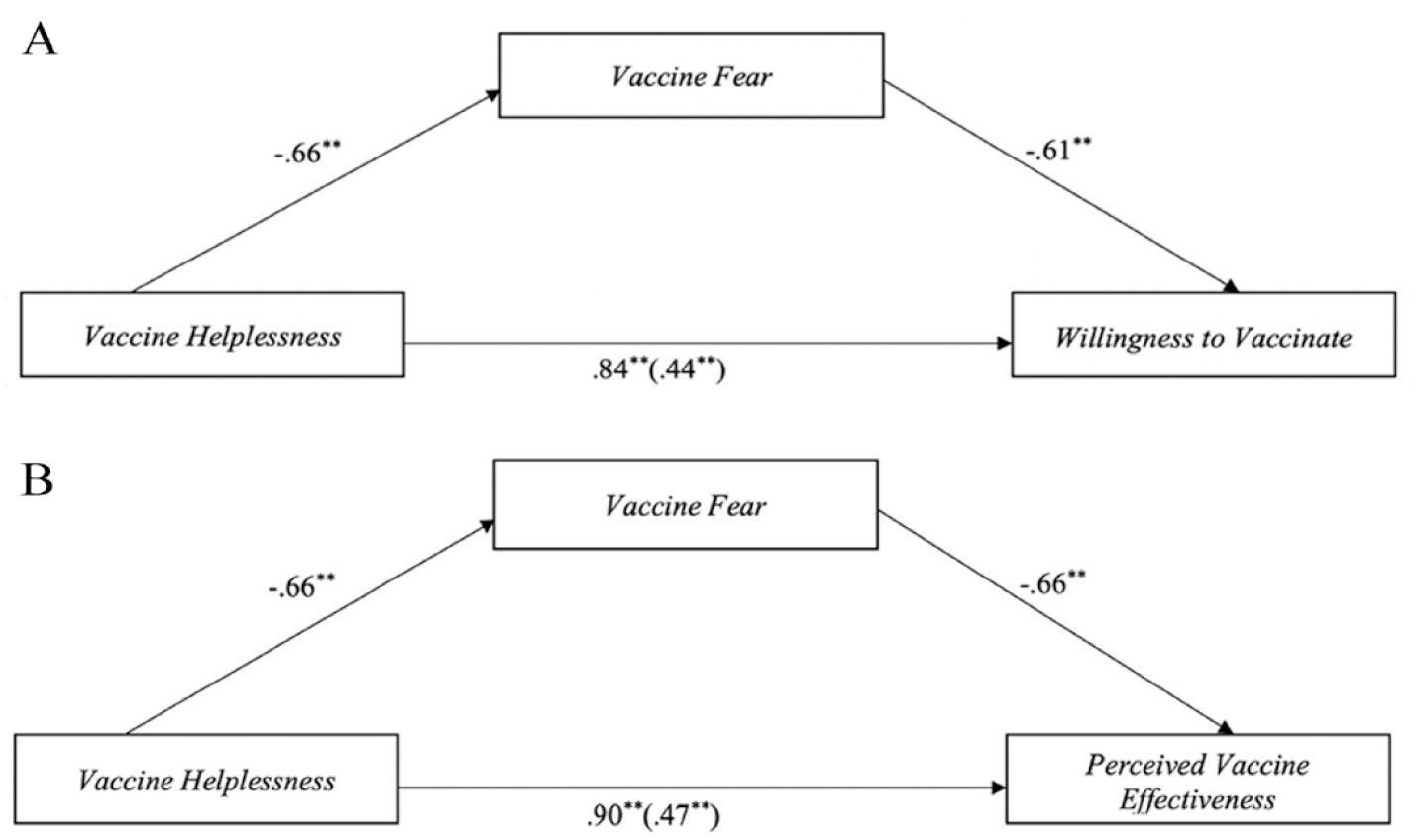
Mediation models depicting the indirect effects of vaccine helplessness on willingness to vaccinate and perceived vaccine effectiveness via reduced vaccine fear (N = 162).
In predicting willingness to vaccinate (controlling for gender, religiosity and residential area), helplessness was significantly related to less vaccine-fear, b = −0.66, t = −8.65, p < 0.001, and vaccine-fear was significantly related to less willingness to vaccinate, b = −0.61, t = −11.38, p < 0.001. Importantly, there was a statistically significant positive indirect effect, in which the relationship between helplessness on willingness to vaccinate was mediated by vaccine-fear Meffect = 0.41, 95% CI [0.292, 0.536] (see Figure 1).
Exploratory analyses
A series of exploratory analyses looking at the potential influence of children health, caregiver vaccination status and children COVID-19 infection status was conducted. These analyses indicated that the effects of vaccine-helplessness on vaccine-fear, perceived vaccine-effectiveness and willingness to vaccinate remained the same after including them as additional predictors (see Tables S5–S7 in Supplemental Material).
Discussion
Study 1’s findings support the motivated helplessness hypothesis: The more parents feel they have no other choice but to vaccinate their children against COVID-19, the less they fear from the possible negative consequences of the vaccine on their children, the more they believe in the effectiveness of the vaccine, and more willing they are to vaccinate their children. Moreover, as predicted, the relationship between vaccine-helplessness, perceived vaccine-effectiveness and willingness to vaccinate were mediated by reduced vaccine-fear. However, since these results were obtained only in Israel, which was one of the first countries to authorize vaccination of children, Study 2 sought to examine the generalization of its results among other countries who were in the process of approval or approved children vaccination. 3
Study 2
Study 2 was aimed at replicating the findings from Study 1 beyond Israel using a large online study among international participants from different countries (with adequate-powered samples from the U.K., U.S., Canada), during mid to the end of August 2021 when vaccination of children aged 12–15 was approved, or in the process of approval worldwide. In addition, Study 2 also examined whether vaccine-helplessness would relate to caregiver’s trust in authorities, and if children’s age may be a meaningful covariate. The hypothesis was that parents’ vaccine-helplessness would be associated with lower vaccine-fear, greater perceived vaccine-effectiveness, willingness to vaccinate and trust in authorities (government and WHO recommendations). As in Study 1, the prediction was that the positive relationship between vaccine-helplessness and vaccine-effectiveness, willingness to vaccinate and trust in authorities would be mediated by vaccine-fear.
Method
Participants
An invitation to participate in a study was posted on Reddit in subreddits related to research (r/sample size), and to COVID-19. English-speaking parents (any parent who has a child regardless of child’s age) were invited to participate voluntarily. An a priori power analysis using G*Power (Faul et al., 2007) indicated that detecting a medium-large effect (f2 = 0.30; based on the relationship between vaccine-helplessness and vaccine-fear in Study 1) in a hierarchical multiple regression with R2 increases that includes three tested predictors and nine total predictors (the linear term and other potential covariates) would require 42 participants for 80% power. Nevertheless the aim was to collect at least 60 participants from each country (94% power).
The responses from 470 participants who (1) had missing data on key variables; (2) reported not completing the study seriously; (3) reported that their child was infected by COVID-19 (n = 56); reported that their child was vaccinated against COVID-19 (n = 136) were removed. The final sample included 481 participants (191 males, 285 females and 5 non-binary/other), at the age range of 22–55 years (M = 37.29, SD = 5.87, Mdn = 37, Mode = 40). A sensitivity analysis using G*Power (Faul et al., 2007) indicated that a small effect size could be detect in the entire sample (f2 = 0.023) at 80% power. Sensitivity analyses in countries with a large enough sample size (N > 60), indicated that a small to medium effect size could be detect in Canada (N = 64, f2 = 0.18), U.S. (N = 218, f2 = 0.05), Australia (N = 104, f2 = 0.11) and the U.K. (N = 66, f2 = 0.18).
Materials and procedure
All materials for this study were in English. After consenting, participants answered the four short measures described in Study 1 in counterbalanced order: vaccine-helplessness (two items were added in Study 2, see Supplemental Appendix 1 in the Methodology file), vaccine-fear, vaccine-effectiveness perception and caregiver willingness to vaccinate (one item was added in Study 2; see Supplemental Appendix 4 in the Methodology file). Cronbach Alphas ranged from 0.86 to 0.96. Table S2 in Supplemental Material presents Ms, SDs and bivariate correlations for these four total scores.
As in Study 1, participants answered questions regarding their personal vaccination against COVID-19 (Yes/No), their children’s COVID-19 vaccination status (Yes/No) and their children infection status COVID-19 (Yes/No). Participant also answered two questions assessing their trust in authorities’ recommendations in handling COVID-19 (‘How much do you trust the recommendations of the World Health Organization?’; ‘How much do you trust the recommendations of your government regarding COVID-19’) on a seven-point scale (1 = not at all, 7 = very much). As in study 1, participants answered demographic questions, as well as questions regarding their children age (whether one of their children is under the age 18, 12 or 3 years of age (Yes/No)).
Results
To test our main hypothesis, regression analyses as described in Study 1 were conducted (see Table 2). The analysis for vaccine-fear showed that the first step (containing participants’ religiosity and political orientation) was statistically significant, F(2, 478) = 48.92, p < 0.001, R2 = 0.17, R2Adj = 0.17. The second step was also statistically significant, ΔF(1, 477) = 38.45, Δp < 0.001, ΔR2 = 0.32, R2Adj = 0.23, as higher parents’ vaccine-helplessness was significantly associated with less vaccine-fear, b = −0.27, β = −0.26, t(477) = −6.20, p < 0.001. The third step including the quadratic term for vaccine-helplessness was not statistically significant, ΔF < 1, Δp = 0.429 (see Figure S4 in the Supplemental Material).
Regression analyses predicting vaccine-fear, perceived vaccine effectiveness and willingness to vaccinate as a function of the linear and quadratic terms of vaccine helplessness (N = 481).
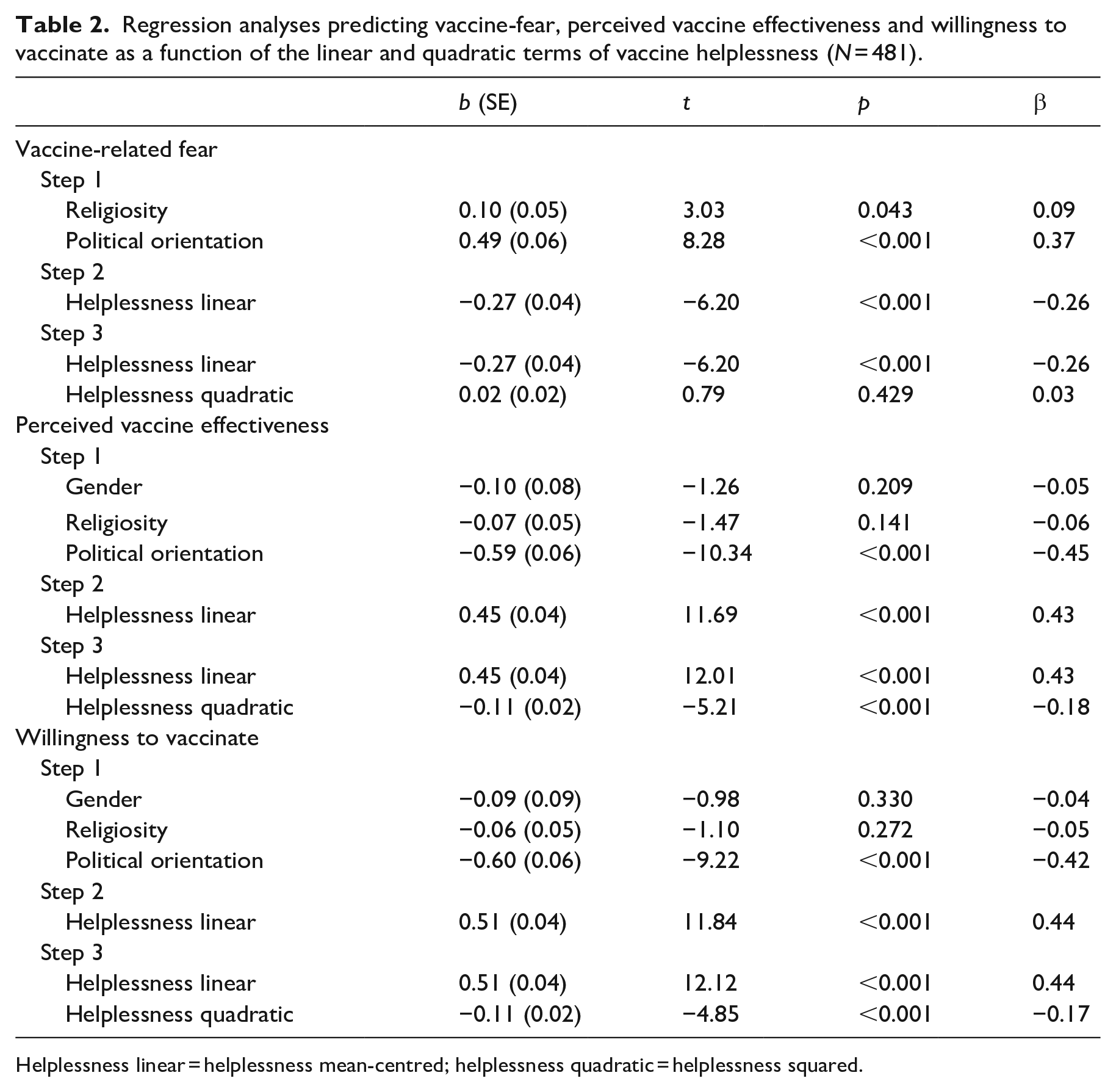
Helplessness linear = helplessness mean-centred; helplessness quadratic = helplessness squared.
The regression for perceived vaccine-effectiveness revealed that the first step (containing gender, religiosity and political orientation) was statistically significant, F(3, 472) = 49.99, p < 0.001, R2Adj = 0.236. The second step was also statistically significant, ΔF(1, 471) = 136.60, Δp < 0.001, ΔR2 = 0.171, R2Adj = 0.407, as vaccine-helplessness was significantly associated with higher perceived vaccine-effectiveness, b = 0.45, β = 0.43, t(471) = 11.69, p < 0.001. The third step was also statistically significant, ΔF(1, 470) = 27.13, Δp < 0.001, ΔR2 = 0.032, R2Adj = 0.438, as the quadratic term for vaccine-helplessness was negatively associated with perceived vaccine-effectiveness, b = −0.11, β = −0.18, t(470) = −5.21, p < 0.001 (see Figure S5).
The regression for willingness to vaccinate revealed that the first step (containing gender, religiosity and political orientation), F(3, 472) = 38.75, p < 0.001, R2Adj = 0.193 and the second step were statistically significant, ΔF(1, 471) = 140.06, Δp < 0.001, ΔR2 = 0.184, R2Adj = 0.376, as higher helplessness was significantly associated with more willingness to vaccinate, b = 0.51, β = 0.44, t(471) = 11.84, p < 0.001. The third step was also statistically significant, ΔF(1, 470) = 23.48, Δp = 0.001, ΔR2 = 0.029, R2Adj = 0.405, as the quadratic term for vaccine-helplessness was negatively associated with willingness to vaccinate, b = −0.11, β = −0.17, t(470) = −4.85, p < 0.001 (see Figure S6).
These regressions were repeated for each country with adequate power (N > 60) and report the results in the Supplemental Material (Tables S8–S10). These analyses replicated the linear relationships between vaccine-helplessness and vaccine-fear in Canada, U.S., Australia, and marginally statistically in the U.K., with no significant curvilinear effects. These analyses also showed a significant association between vaccine-helplessness and perceived vaccine-effectiveness and willingness to vaccinate in all the assessed countries (Canada, U.S., Australia and the U.K.). In U.S. and Australia, significant negative curvilinear effects of vaccine-helplessness on perceived vaccine-effectiveness and willingness to vaccinate were found (See Figures S7–S10).
Mediation analyses
The mediational role of vaccine-fear in the relationship between vaccine-helplessness and perceived vaccine-effectiveness and willingness to vaccinate was tested as described in Study 1 (see Tables S11 and S12).
In the analysis predicting vaccine-effectiveness (controlling for gender, religiosity and political orientation), vaccine-helplessness was significantly related to higher vaccine-effectiveness, b = 0.45, t = 11.69, p < 0.001, and vaccine-fear was significantly related to lower vaccine-effectiveness, b = −0.48, t = −14.52, p < 0.001. Replicating the finding of Study 1, a statistically significant positive indirect effect was found, by which the relationship between vaccine-helplessness on perceived vaccine-effectiveness was mediated by vaccine-fear, Meffect = 0.13, 95% CI [0.084, 0.189] (see Figure 2).
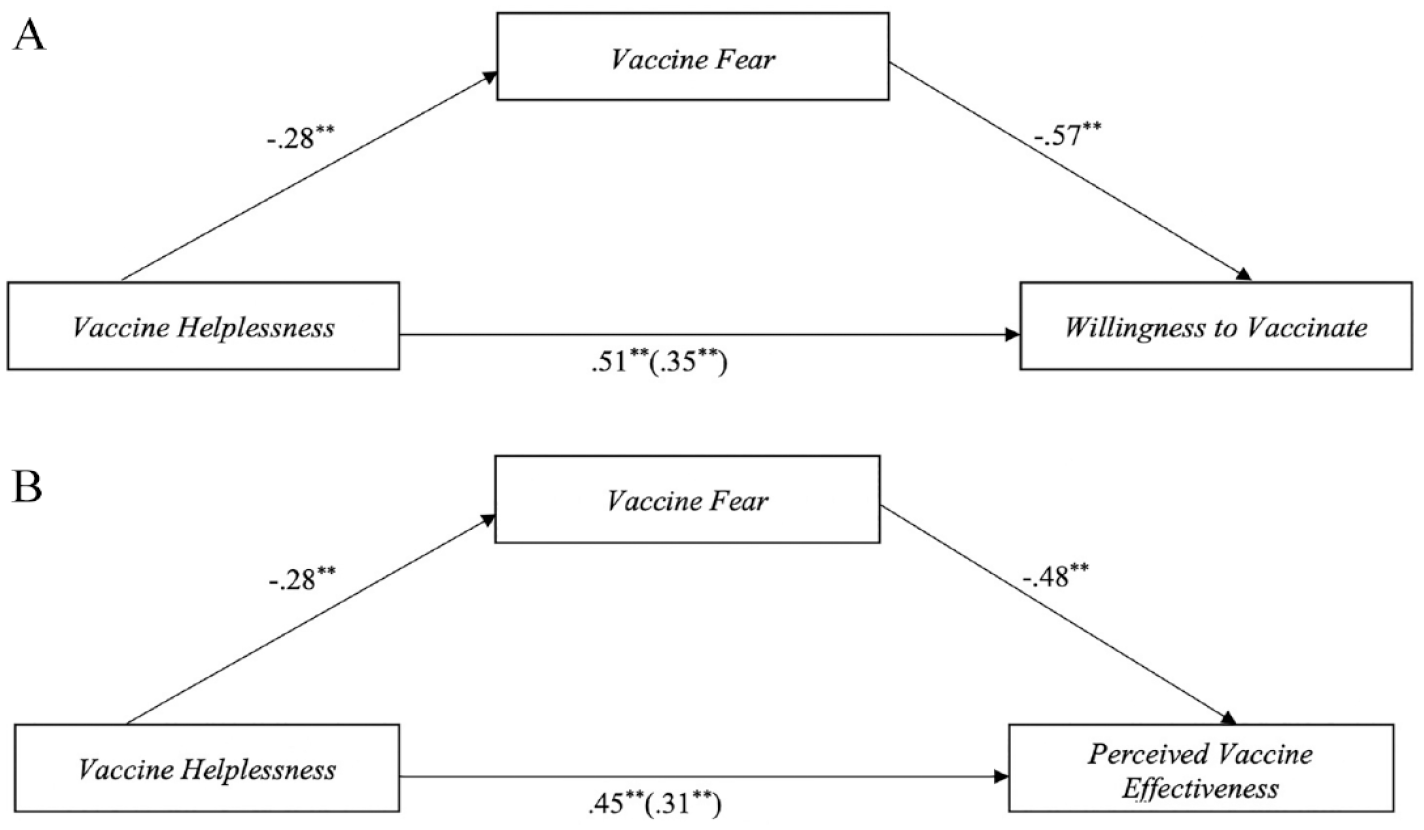
Mediation models depicting the indirect effects of vaccine helplessness on willingness to vaccinate and perceived vaccine effectiveness via reduced vaccine fear (N = 481).
In the analysis predicting willingness to vaccinate (controlling for gender religiosity and political orientation), vaccine-helplessness was significantly related to less vaccine-fear, b = −0.28, t = −2.29, p < 0.001, and vaccine-fear was significantly related to lower willingness to vaccinate, b = −0.57, t = −15.65, p < 0.001. Importantly, a statistically significant positive indirect effect was found, by which the relationship between vaccine-helplessness on willingness to vaccinate was mediated by vaccine-fear Meffect = 0.16, 95% CI [0.099, 0.225] (see Figure 2).
Exploratory analyses
A series of exploratory analyses looking at the potential influence of child age group, child health, caregiver vaccination status and children COVID-19 infection status were conducted (see Tables S13–S24). These analyses indicated that the results remained the same among participants with varied children age group (under 3, 3–12, 12–18), and when controlling for child general health, children COVID-19 infection status and caregiver vaccination status.
Lastly, the hypothesis that vaccine-helplessness would predict higher trust in government’s and WHO’s recommendations in dealing with COVID-19 (see Tables S25 and S26) was examined. Result indicated a positive linear relationship between vaccine-helplessness and trust in government’s recommendations, b = 0.31, β = 0.30, t(469) = 7.67, p < 0.001, and the WHO, b = 0.27, β = 0.25, t(469) = 6.43, p < 0.001. Furthermore, the relationships between helplessness and trust in government’s and WHO’s recommendations were mediated by reduced vaccine-fear, Meffect on trust in government’s recommendations = 0.16, 95% CI [0.109, 0.211]; Meffect on trust in WHO recommendations = 0.17, 95% CI [0.116, 0.222].
Discussion
Study 2 replicated Study 1’s findings consistently across different countries. Specifically, the more parents felt helpless in the decision to vaccinate their children against COVID-19, they tended to feel less fear regarding the vaccine-related side effects, which, in turn, was associated with higher perceived vaccine-effectiveness, willingness to vaccinate and trust in government’s and WHO’s recommendations.
General discussion
The purpose of this study was to apply the motivated helplessness hypothesis in understanding the psychological underpinning of caregivers’ decision-making process in vaccinating children against COVID-19. The hypothesis was that caregivers who feel they have no other choice but to vaccinate their children will be less concerned over the vaccine’s possible side effects, perceive the vaccine as more effective, and in turn more willing to vaccinate their children. In line with our (preregistered) predictions, in two studies, across different countries, high levels of helplessness in vaccinating children were related to lower levels of vaccine-fear, higher vaccine perceived-effectiveness and more willingness to vaccinate one’s child. Further, as predicted, the relationships between helplessness, perceived vaccine-effectiveness and willingness to vaccinate were partially mediated by vaccine-fear. These results were also found when controlling for the effects of child age, child general health, parent vaccination status and child infection status. In Study 2, high levels of vaccine-helplessness also related to greater trust in government’s and WHO’s recommendations, and that these relationships were partially mediated by vaccine-fear.
These findings suggest that when people feel they have no other choice but to vaccinate their children, they are free from concerns related to the possible negative consequences of their decision. When people are freed from these concerns, they may then be more willing to vaccinate their children. On the other hand, parents who think that they do have a choice in vaccinating their child (low levels of helplessness) might be more fearful about the consequences of their choice, sceptical regarding vaccine’s effectiveness, and therefore may be less willing to administer it to their child. Overall, these finding provide support for the hypothesis that feelings of helplessness may protect parents against fear regarding the possible negative consequences related to vaccinating children for COVID-19.
These results are generally in line with the motivated helplessness hypothesis (Lifshin et al., 2020), as they show that feelings of helplessness may serve a psychological protective function in facing fears and threats. As such, feeling out of control and helpless seems to help people alleviate threat-related fears and move on with their lives. Although the theory may predict a curvilinear relationship between helplessness and fear, such that low helplessness would also be related to lower fear, this was not the case in the current study, as the relationships was primarily linear. Nevertheless, these findings are congruent with research within the theory’s framework, suggesting that in cases were the threat may be very high or prolonged, the relationship would be linear (Lifshin and Mikulincer, 2021). In this context, when dealing with a deadly virus and a newly produced vaccine, and when children health is at stake, thinking that one may have other choices but to vaccinate them may give rise to increased fear.
Pandemics hold in store destructive potential to health care systems, families and global society, and vaccines appear to be the most efficacious ‘weapons’ to combat the pandemics spread and their following devastating consequences (e.g. Rennert et al., 2022). Despite that, vaccine hesitancy is still one of the greatest health challenges that the world is currently facing (WHO, 2022) and parental vaccination hesitancy seem to be even vaster (e.g. Pan et al., 2021). As such, it is vitally important to understand the psychological factors that stand at the core of this hesitancy, and specifically identify the factors that affect parents’ perceptions and fears in the decision-making process of vaccinating their children (e.g. Liu et al., 2022).
The current study shed light on the psychological process regarding the decision to vaccinate children during a pandemic, showing that when parents perceive themselves as helpless in the decision to vaccinate their children, they are less fearful from its possible side effects, perceive the vaccine as more effective, trust more the authorities’ recommendations and are more willing to vaccinate. Thus, future research should further examine the role of motivated helplessness in vaccine intentions.
This study has several important limitations. Primarily, both of our studies are correlational, and so our ability to deduce a causal relationship between helplessness, fear, vaccine-effectiveness and willingness to vaccinate is limited. The direction of causality between the variables might be different and other variables might explain this relationship. Nevertheless, the fact that the findings were in line with our preregistered hypotheses and replicated in two studies and across different countries provides additional confidence in our results interpretation. Still, further experimental research is needed to have more confidence regarding the causal path of our correlational findings (e.g. Lifshin et al., 2022).
Another limitation is that despite having internationally diverse sample, our samples were not representative of each country and most countries were predominantly English-speaking western cultures. Finally, it is important to consider that these findings may be limited to the context of the COVID-19 pandemic. Specific pandemic characteristics, the vaccine production and the way it was managed by authorities might have created unique conditions that have affected the current findings. However, the psychological function of motivated helplessness should apply in any context in which people are dealing with decisions that may have negative consequences to the self and significant others. Future research should examine the role of motivated helplessness in other health-related decisions.
To conclude, this study provides more evidence to the motivated helplessness hypothesis in the context of COVID-19 pandemic. Our findings reveal how parents’ sense of helplessness regarding vaccinating their children may be a defence against fear and consequently contribute to the willingness to vaccinate. To deal with a pandemic effectively, one should take into account not only its health challenges, such as developing vaccines and other protective measures, but also the psychological challenges, such as worries and fears, which people face during a pandemic and the psychological mechanisms that allow them to manage these challenges.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053231170055 – Supplemental material for Parental motivated helplessness in vaccinating children against COVID-19: Its association with fear, effectiveness and willingness to vaccinate
Supplemental material, sj-docx-1-hpq-10.1177_13591053231170055 for Parental motivated helplessness in vaccinating children against COVID-19: Its association with fear, effectiveness and willingness to vaccinate by Mabelle Kretchner, Uri Lifshin and Mario Mikulincer in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053231170055 – Supplemental material for Parental motivated helplessness in vaccinating children against COVID-19: Its association with fear, effectiveness and willingness to vaccinate
Supplemental material, sj-docx-2-hpq-10.1177_13591053231170055 for Parental motivated helplessness in vaccinating children against COVID-19: Its association with fear, effectiveness and willingness to vaccinate by Mabelle Kretchner, Uri Lifshin and Mario Mikulincer in Journal of Health Psychology
Supplemental Material
sj-docx-3-hpq-10.1177_13591053231170055 – Supplemental material for Parental motivated helplessness in vaccinating children against COVID-19: Its association with fear, effectiveness and willingness to vaccinate
Supplemental material, sj-docx-3-hpq-10.1177_13591053231170055 for Parental motivated helplessness in vaccinating children against COVID-19: Its association with fear, effectiveness and willingness to vaccinate by Mabelle Kretchner, Uri Lifshin and Mario Mikulincer in Journal of Health Psychology
Footnotes
Data sharing statement
The current article is accompanied by the relevant raw data generated during and/or analysed during the study, including files detailing the analyses and either the complete database or other relevant raw data. These files are available in the Figshare repository and accessible as Supplemental Material via the Sage Journals platform. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing. The data files from the current study are also available in the Open Science Foundation repository at ![]() .
.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Pre-registration
These studies were pre-registered: Study 1 (https://aspredicted.org/blind.php?x=DBM_V97) Study 2 (![]() ).
).
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.