
Abstract
This study aims to examine changes in body image (BI) over time and factors related to BI among patients with prostate cancer who receive hormone therapy (HT). A cross-sectional design and longitudinal design were utilized. Patients with prostate cancer who received HT were recruited from the urology outpatient departments in two hospitals in Taiwan between August 2017 and December 2020. Cross-sectional data were collected from 177 patients who had started HT for prostate cancer. Longitudinal data were collected from 34 newly diagnosed patients before receiving HT and at 1, 3, 6, and 12 months after HT. The variables measured included hormonal symptoms and distress, self-efficacy, and BI. The results showed that BI dissatisfaction ranged from 6.1% to 17.2%. Hormonal symptoms and distress (e.g. lack of vitality) were correlated with BI dissatisfaction. Education on the side effects of HT and coping strategies can be provided to patients to prevent BI dissatisfaction.
Introduction
Body image (BI) refers to a person’s unique view of their own body, which is dynamic and subject to change due to external circumstances (Cash, 2008; Darnyshire, 1986). BI is also defined as an individual’s perception, thoughts, and feelings about their own body (Cash, 2008; Grogan, 2007). In a cognitive behavioral model, BI is based on a complex and dynamic coping process influenced by factors that include cultural socialization, interpersonal experiences, physical characteristics and changes, and personality. Cognitive understanding of an individual’s own BI can affect their behavior, in turn further affecting BI (Cash, 2008). BI disturbance may occur when a cancer patient is displeased with a perceived change in physical appearance and function (Bowie et al., 2022; Rhoten, 2016). BI dissatisfaction of patients has been demonstrated to be associated with increased anxiety and depression (Chopra et al., 2021; Rhondali et al., 2015; Scandurra et al., 2022) and decreased quality of life (Harrington and Badger, 2009).
Prostate cancer is the most commonly diagnosed cancer among men in 112 countries, and it ranks as the second leading cause of cancer death among men in 48 countries (Sung et al., 2021). In Taiwan, prostate cancer ranks fifth in male cancer incidence and sixth in cancer death causes (Health Promotion Administration, Ministry of Health and Welfare, Taiwan, 2022). Hormone therapy (HT) is a standard treatment for recurrent and/or metastatic prostate cancer. HT aims to lower male hormones through orchiectomy or medical castration to control the progress of cancer (Cornford et al., 2021). Prostate cancer and its treatment alter the original structure of the body, and patients with prostate cancer who undergo HT experience physical changes, such as reduced sexual function, shrinking genitalia, thinning body hair, weight gain, decreased muscle mass, hot flashes, enlarged breasts, and lack of vitality (Chien and Huang, 2022; Desai et al., 2021; Mainwaring et al., 2021). Qualitative studies have shown that disruptive bodily changes, sexual dysfunction, and poor economic capacity can affect the masculinity of patients with prostate cancer (Salifu et al., 2023). Moreover, cancer and the side effects associated with its treatment may change a patient’s self-confidence, self-efficacy (Bandura, 1977; Torbit et al., 2015), masculinity (Langelier et al., 2018; Salifu et al., 2023), or perception of one’s body, leading to dissatisfaction with one’s BI (Arıkan et al., 2020; Bowie et al., 2022; Cecil et al., 2010; Gentili et al., 2019; Harrington, 2011; Harrington et al., 2009; Mainwaring et al., 2021).
Studies have shown that BI dissatisfaction among patients with prostate cancer is 11%–34% (DeFrank et al., 2007). Patients with prostate cancer who receive HT have an inferior BI compared to those who do not receive HT (Saini et al., 2013). Patients with non-metastatic prostate cancer who receive HT have a significantly worse BI between the time prior to primary treatment and 2 years after treatment completion (Taylor-Ford et al., 2013). One study found that Belgian patients with prostate cancer at different cancer stages who received HT had a significantly worse BI score 6, 12, and 18 months post-treatment as compared to pre-treatment, but the scores at 3 and 24 months post-treatment is similar to those of pre-treatment (van den Driessche et al., 2016). Therefore, the present study examined the changes in the BI of patients with prostate cancer who receive HT before treatment and at 1, 3, 6, and 12 months after treatment in Chinese culture.
Age, waist circumference, and body mass index (BMI) affect the body shape and appearance of individuals (Cash, 2008). Previous studies have supported the hypothesis that the BI of patients with prostate cancer is affected by the duration of treatment but is inversely correlated with waist circumference and BMI (Harrington et al., 2009; van den Driessche et al., 2016). Younger patients with prostate cancer have lower satisfaction with their BI (Gentili et al., 2022).
Self-efficacy refers to an individual’s confidence in their ability to achieve a specific goal or task. Patients with higher general self-efficacy exhibit better health behavior, such as physical activity (Bandura, 1977; Thieser et al., 2021), which helps to improve BI (Cash, 2008; Gentili et al., 2019; Langelier et al., 2019). However, cancer and the side effects of HT may have a negative impact on general self-efficacy (Bandura, 1977; Foster and Fenlon, 2011). Lower general self-efficacy will have a negative impact on cancer-related self-efficacy, affecting self-management and self-care behaviors (Foster and Fenlon, 2011), which may further affect BI among cancer patients (Arıkan et al., 2020; Bowie et al., 2022; Foster and Fenlon, 2011). To elucidate the interplay of these factors, the present study examined the relationship between general self-efficacy and BI of patients with prostate cancer who receive HT.
Cultural socialization is an important factor that affects BI (Cash, 2008). In contrast with that of Western countries, traditional Chinese culture emphasizes literary-martial balance as an important male trait (Edwards, 1994). However, the BI of patients with prostate cancer has been explored in Western countries (Bowie et al., 2022; Gentili et al., 2019, 2022; Harrington and Badger, 2009; Harrington et al., 2009; Horschke et al., 2020; Vyas et al., 2023) but has been less explored in Asian countries. Based on a cognitive behavioral model of BI, the primary objectives of the current study are as follows: (1) to understand the changes in the BI of patients with prostate cancer who receive HT before treatment and at 1, 3, 6, and 12 months after treatment, using a longitudinal study design; and (2) to understand the factors, specifically demographic and physical characteristics and associated changes (clinical characteristics and hormonal symptoms and distress), and personality (general self-efficacy), which affect the BI of patients with prostate cancer who receive HT, using a cross-sectional design.
Methods
Design and participants
Cross-sectional and longitudinal study designs with convenience sampling were adopted in this study, and a structured questionnaire was used to collect data. Patients were recruited and followed up with at the urology outpatient departments in two hospitals in Taiwan between August 2017 and December 2020. Patients who were receiving HT for prostate cancer were invited to participate in the cross-sectional study. Patients who were newly diagnosed with prostate cancer and scheduled to receive HT were invited to participate in the longitudinal study, and data were collected before HT and at 1, 3, 6, and 12 months after starting treatment. The inclusion criteria were as follows: (1) receiving or scheduled to receive HT, such as orchiectomy and medical castration; (2) of clear consciousness and able to communicate in Mandarin or Taiwanese; (3) not diagnosed with a mental health problem; (4) can move independently and take care of themselves at home; and (5) aged 20 years or above, agreed to participate in the research, and completed the consent form. Patients who were unaware of their prostate cancer were excluded.
A total of 203 patients met the inclusion criteria for the cross-sectional study during the study period. Among these, 26 declined to participate due to a lack of time or interest. A total of 177 individuals completed the questionnaire and were included in the statistical analysis (response rate = 87%). Forty patients met the inclusion criteria for the longitudinal study. Among these patients, one declined to participate due to the time commitment, and four were transferred to other hospitals for treatment and could no longer be contacted. Among the 35 participants who enrolled in this study, the number of patients who completed their follow-up at each subsequent time point was 33, 33, 32, and 29 at 1, 3, 6, and 12 months after treatment, respectively. A total of seven patients did not complete follow-up due to discontinuation of treatment (n = 3), chemotherapy treatment (n = 2), time factor (n = 1), or weakness (n = 1). One participant, who completed only the pretest questionnaire, was excluded. Finally, 34 participants were included in the statistical analysis. Using longitudinal data, the study focused on understanding changes in BI.
Sample size estimation
In the current study, the sample size was estimated by referring to the results of a previous study (Chen et al., 2012). The coefficient of the relationship between depressive symptom and BI was r = 0.37 (medium effect size; Cohen, 1988). For the cross-sectional design, G*Power 3.1 statistical software (Faul et al., 2007) estimated that at least 135 subjects were required for regression statistics with 14 independent variables, where the effect size f2 = 0.15 (medium effect size; Cohen, 1988), power = 80%, and α = 0.05. The possibility that a participant may temporarily withdraw consent or provide incomplete data was taken into consideration. Thus, 177 cases were enrolled in the cross-sectional design. In the longitudinal design, at least 32 subjects were required for repeated measurement ANOVA statistics with five measurements, where the effect size f = 0.20 (medium effect size; Cohen, 1988), power = 80%, and α = 0.05. A total of 34 newly diagnosed men were enrolled in this study to understand changes in BI, starting from pre-treatment to up to 12 months after starting treatment.
Measurements
Demographic and clinical characteristics
In this study, basic patient demographics and clinical characteristic data were collected in the cross-sectional and longitudinal designs. The basic demographics included age, education level, marital status, religion, occupational status, and annual household income (New Taiwan dollar, TWD). Clinical characteristics were obtained primarily from medical records, were confirmed by the patient, and included cancer stage, months since diagnosis, most recent serum prostate-specific antigen (PSA) concentration, and primary treatment modality. Waist circumference (centimeter, cm) and BMI (National Institutes of Health, 2000) were measured and calculated by trained researchers on the day of questionnaire data collection in the cross-sectional study and during the first questionnaire collection in the longitudinal study.
Hormonal symptoms and distress
The hormonal component of the Expanded Prostate Cancer Index Composite, developed by Wei et al. (2000), was translated into Chinese by Chien et al. (2018). In the cross-sectional design, the translated version was used to measure hormone-related symptoms and distress among patients with prostate cancer. Questions on the following 11 symptoms and “bother,” answered using a Likert scale, were included: experiencing hot flashes, breast tenderness, depression, lack of energy, changes in body weight, distress due to hot flashes, distress due to breast tenderness/enlargement, distress due to body hair loss, distress due to feeling depressed, distress due to lack of energy, and distress due to change in body weight. The items (such as during the last 4 weeks, how often have you felt. . .?) and response options vary, based on each item; for example, the option of 0–5 points consequently for distress items are 0 = no problem, 1 = very small problem, 2 = small problem, 3 = moderate problem, and 4 = big problem. The hormonal component was scored and linearly scaled as a sum of 0–100 points, with higher scores as representing a better state (Chien et al., 2018; Wei et al., 2000). In this study, the Cronbach’s α for internal consistency was 0.76.
General self-efficacy
The Chinese version of the General Self-Efficacy Scale was used to measure general self-efficacy among patients with prostate cancer in the cross-sectional design of this study. The scale consisted of 10 items, such as it is easy for me to stick to my aims. . .. The scale was based on a 4-point Likert scale (1 = not at all true, 2 = hardly true, 3 = moderately true, 4 = exactly true) with total scores that ranged from 10 to 40; and a lower score indicated lower general self-efficacy (Schwarzer and Jerusalem, 1995). The scale has acceptable reliability and validity (Cheung and Sun, 1999; Zhang and Schwarzer, 1995). In this study, the Cronbach’s α for internal consistency was 0.97.
Body image
The Body Image Scale was developed by Hopwood et al. (2001); it is specific to cancer patients and encompasses affective, cognitive, and behavioral items. Items can be classified into an appearance/attractiveness subscale and a body satisfaction subscale (Hopwood et al., 2001). It has been used to measure the BI of prostate cancer patients (Bowie et al., 2020; Gentili et al., 2022; Harrington and Badger, 2009; Harrington et al., 2009; Langelier et al., 2018; Scandurra et al., 2022). The scale consists of 10 questions, answered on a 4-point Likert scale (0 = not at all, 1 = a little, 2 = quite a bit, 3 = very much), with total scores that range from 0 to 30. A higher score indicates higher levels of BI dissatisfaction (Hopwood et al., 2001), and a score of 10 or above indicates dissatisfaction with BI (Chopra et al., 2021; Rhondali et al., 2015). A score ⩾10 on the BI corresponds to the cut point of the Generalized Anxiety Disorder Scale (GAD, ⩾10) and the Patient Health Questionnaire (⩾10), which also can predict moderate depression and moderate anxiety (Rhondali et al., 2015). The scale has acceptable reliability and validity (Hopwood et al., 2001) and corresponds to the established cut points for moderate depression, moderate anxiety (GAD ⩾10), and clinically relevant distress (Distress thermometer ⩾4; Chopra et al., 2021).
Wang (2003) translated the English version of the Body Image Scale into Chinese. In this study, the Chinese version of the Body Image Scale was used to measure the BI of patients with prostate cancer in the cross-sectional and longitudinal designs. The Chinese version has been applied to patients with a variety of cancers and has acceptable reliability and validity (Chang et al., 2019; Chen et al., 2012, 2017). In the current study, patients who underwent HT seldom had an evident scar. Hence, Item 4 was revised from feeling less “feminine/masculine” as a result to feeling less “masculine” as a result; and Item 10 was revised from being dissatisfied with the appearance of “scars” to dissatisfaction with the appearance of “genital organs.” The content validity index of the scale was 0.97. The Cronbach’s α for internal consistency was 0.89 in the cross-sectional data and ranged from 0.90 to 0.93 at various measurement time points in the longitudinal study data.
Procedure
In this study, potential cases were transferred by urologists. After the researchers further evaluated and confirmed that these cases met the inclusion criteria, the patients were informed of the study’s content and purpose and invited to participate. After consent forms were obtained from patients who agreed to participate in this study, the patients were asked to complete questionnaires. Then, their waist circumference was measured, and their BMI was calculated in a private space of the outpatient clinic. Subsequently, the participants in the longitudinal study were asked to complete questionnaires for the second to fifth time during their outpatient follow-up at 1, 3, 6, and 12 months after receiving HT. A few participants were unable to complete the questionnaire during their follow-up schedule. Therefore, with the consent of the participants, the questionnaire was mailed in paper form.
Statistical analyses
All returned questionnaires were checked, and the data were organized using the Chinese version of Microsoft Excel. The data were then statistically analyzed using IBM SPSS Statistics (version 22). No missing values were found in the cross-sectional data of this study. For the longitudinal research data, a missing completely at random (MCAR) test was performed on five scores of BI (Little, 1988). The results showed that missing values occurred at random (chi-square = 4.85, p-value = 0.978). Therefore, no value was supplemented. Descriptive statistics, including the mean, standard deviation (SD), frequency, percentage, quartile, and median, were used to understand the distribution of data. In the cross-sectional data, the Kolmogorov Smirnov test indicated a non-normal distribution of the BI scores. Therefore, the BI scores were divided into two groups for inferential statistical analysis, a group with a BI score of 10–30 and a group with a score of 0–9 (Chopra et al., 2021; Rhondali et al., 2015). To understand the factors that affect the BI of patients, data for the cross-sectional design were analyzed using a two-sample t-test, chi-squared test, and logistic regression. Univariate analysis of the factors associated with BI was conducted first. Then, the factors that were revealed as significant in the univariate analysis were included in the multivariate logistic regression for analysis.
Previous studies have shown that BMI and self-efficacy are possible factors that influence BI (Arıkan et al., 2020; Harrington et al., 2009). Therefore, BMI, general self-efficacy, and hormone-related symptoms and distress were included in the multivariate logistic regression, regardless of whether they were significant in the univariate analysis. To understand the changes in a patient’s BI scores over time, data from the longitudinal study were analyzed using generalized estimating equations (GEEs; model types = linear, working correlation matrix = AR(1)). In this study, a Bonferroni adjusted p-value was adopted to avoid increasing the type-1 error rate due to multiple comparisons (Wright, 1992). The level of significance was set at p < 0.05, and two-tailed tests were conducted.
Ethical considerations
The cases were recruited after being reviewed and approved by the Institutional Review Board of the receiving hospital (Plan No.: 201602024B0C505). Based on the principle of the World Medical Association Declaration of Helsinki, this study kept data confidential, maintained the privacy of the participants, and completed the process of informed consent. Subjects were allowed to unconditionally withdraw from this study without affecting their medical rights.
Results
Basic data and clinical characteristics
In the cross-sectional data, the mean age of patients was 74.95 years (SD = 8.93), and 49.2% had a junior high school education (diploma) or above. The mean waist circumference was 90.62 cm (SD = 8.50), and 57.1% had a waist circumference of ⩾90 cm. The average BMI was 24.80 kg/m2 (SD = 3.89), and 54.2% had a healthy weight, according to their BMI. Most patients had Stage IV prostate cancer (n = 130, 73.4%), and most were treated with HT using medical castration (n = 157, 88.7%). In the longitudinal data, the mean age of the patients was 74.03 years (SD = 10.06), and 52.9% had a junior high school education or above. The mean waist circumference was 89.61 cm (SD = 8.37), and 50.0% had a waist circumference of ⩾90 cm. The average BMI was 24.43 kg/m2 (SD = 3.04), and 64.7% had a healthy weight, according to their BMI. Most patients had Stage IV prostate cancer (n = 32, 94.2%), and most were treated with HT using medical castration (n = 33, 97.1%). Compared with the patients in the cross-sectional study, a higher proportion of the patients in the longitudinal study had religion, Stage IV cancer, shorter diagnosis time, and higher recent PSA value (all p-values were <0.05; Supplemental Table 1).
Body image and its change over time
In the cross-sectional data, patients with prostate cancer who were receiving HT had a mean BI score of 2.56 (SD = 4.22; range = 0–21; Q1/Q2/Q3 = 0/1/4), with 7.9% who scored ⩾10. The first and second highest scores were for the items of self-conscious about appearance (0.61) and feeling less masculine (0.46). The lowest-scored item was avoiding people based on one’s appearance (0.10). In the longitudinal data, the mean BI score of patients before starting HT was 2.41 (SD = 3.78; range = 0–12; Q1/Q2/Q3 = 0/0/4). The BI score was 2.85 (SD = 4.57; range = 0–18; Q1/Q2/Q3 = 0/0/4), 1.82 (SD = 3.52; range = 0–15; Q1/Q2/Q3 = 0/0/3), 2.66 (SD = 4.12; range = 0–16; Q1/Q2/Q3 = 0/0/4), and 3.38 (SD = 6.04; range = 0–20; Q1/Q2/Q3 = 0/0/5) during follow-up at 1, 3, 6, and 12 months after starting treatment, respectively. Scores ⩾10 accounted for 8.8% at pre-HT and 12.1%, 6.1%, 9.4%, and 17.2% at 1, 3, 6, and 12 months after commencing HT, respectively. GEEs were used to analyze the changes in BI scores. Compared to pre-HT, patients exhibited similar mean BI scores at 1, 3, 6, and 12 months after starting HT (all p-values >0.05). The highest-scored item was self-conscious about appearance at all measurement time points (0.45–0.69). The lowest-scored item was avoiding people based on one’s appearance, at 1, 3, 6, and 12 months after starting HT (0.03–0.14). Finally, the lowest-scored item was dissatisfaction with the appearance of genital organs before treatment (0.09; Table 1).
Body image score distribution and change over time.
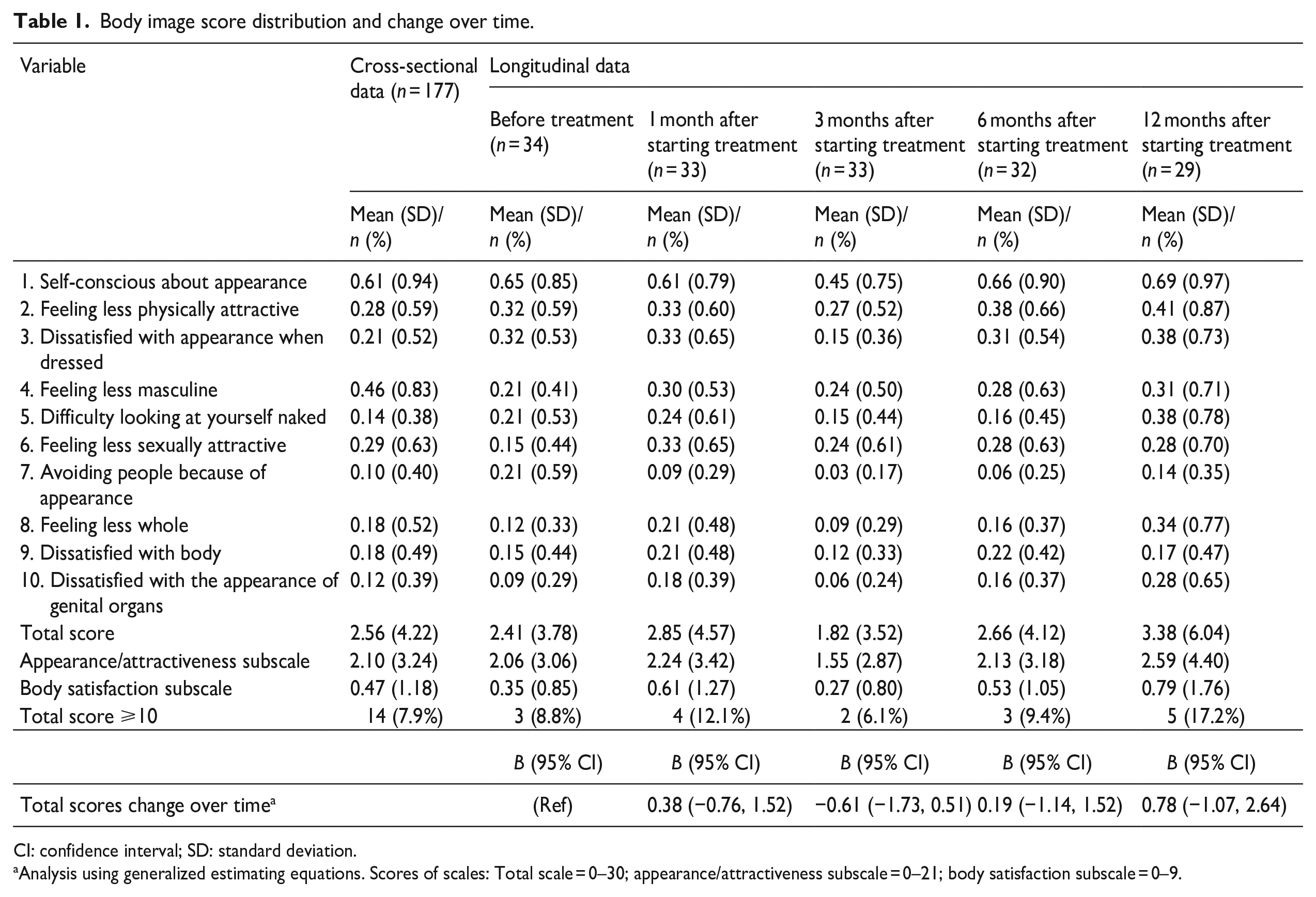
CI: confidence interval; SD: standard deviation.
Analysis using generalized estimating equations. Scores of scales: Total scale = 0–30; appearance/attractiveness subscale = 0–21; body satisfaction subscale = 0–9.
Factors associated with body image
Univariate analysis of the data from the cross-sectional design showed a significant difference between patients’ educational level and BI (p = 0.026). The overall scores of patients’ hormonal symptoms and distress (t = 4.91; p < 0.001) and BI also were significantly different (Table 2). In the multivariate analysis, education level, BMI, hormonal symptoms and distress, and general self-efficacy were analyzed by multivariate binary logistic regression. Of these, hormonal symptoms and distress were significantly correlated with BI (odds ratio (OR) = 0.91, CI = 0.87, 0.96, p < 0.001). Every one-point increase in a patient’s hormonal symptoms and distress reduces the probability of BI dissatisfaction 0.91 times (Supplemental Table 2).
Factors related to body image understanding using cross-sectional data (N = 177).
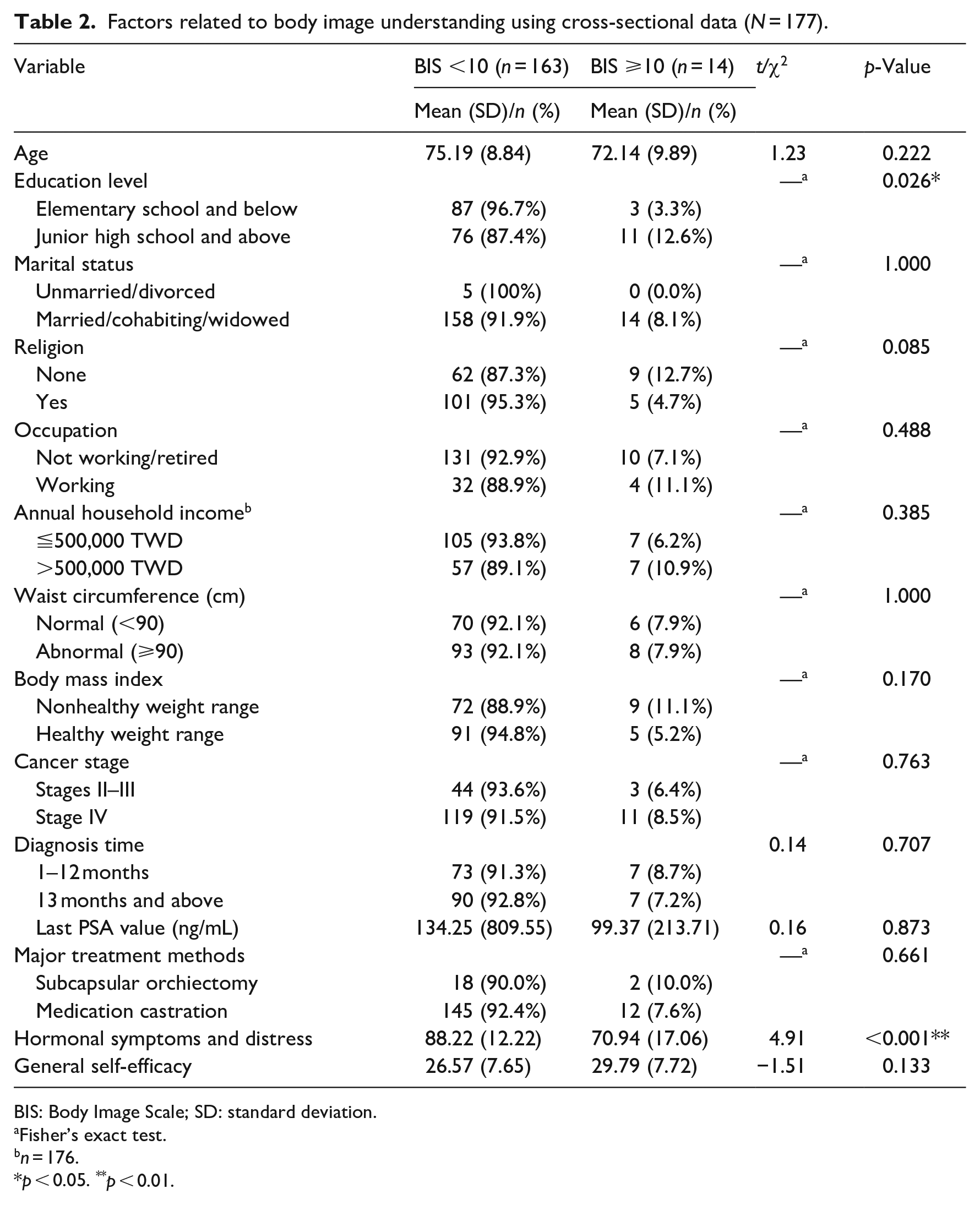
BIS: Body Image Scale; SD: standard deviation.
Fisher’s exact test.
n = 176.
p < 0.05. **p < 0.01.
Discussion
This study uses cross-sectional and longitudinal studies to explore BI changes and the associated factors in prostate cancer patients who receive HT. The results showed that (1) the proportion of BI dissatisfaction ranged from 6.1% to 17.2%; (2) there were no significant changes in the BI of patients from pre-treatment to 12 months post-treatment; (3) fewer hormonal symptoms and less distress were related to less BI dissatisfaction; and (4) the relationship between the patient’s general self-efficacy and BI was not statistically significant. As expected, compared with the patients in the cross-sectional study, a higher proportion of the patients in the longitudinal study had Stage IV cancer, a shorter diagnosis time, and a higher recent PSA value. The reasons included the following: The cases in the longitudinal study were newly confirmed, and the first time the cases were received was before the start of HT treatment. Further, patients with Stage IV or metastatic cancer had a shorter survival period than did patients with early prostate cancer. Therefore, fewer patients with Stage IV cancer were included in the cross-sectional study than in the longitudinal study.
In this study, compared to pre-HT, patients with prostate cancer presented similar BI scores at 1, 3, 6, and 12 months after commencing HT. This result is dissimilar to that of previous studies (Taylor-Ford et al., 2013; van den Driessche et al., 2016). Such dissimilarities may arise from differences in treatment modalities. This study recruited prostate cancer patients who received only HT. In contrast, the other two studies enrolled prostate cancer patients who received only HT and patients who received active treatment combined with HT. Patients who received a combination of HT and active treatment may experience more side effects, such as urinary incontinence, penis shortening, fatigue, wound scarring, and erectile dysfunction; these side effects may aggravate BI dissatisfaction (Bowie et al., 2022; Klaeson et al., 2013). Further, the longitudinal data of this study showed that the BI of prostate cancer patients was better in the third month after receiving HT than in other time points. This finding may be related to the fact that patients who had been treated for 1–3 months exhibited a significant decrease in serum PSA value and improved control of the disease (Desai et al., 2021), affecting the patients’ perception and attitude toward their BI (Cash, 2008). Further research and exploration are needed.
Moreover, this study found that the overall mean BI scores of patients with prostate cancer who underwent HT ranged from 1.82 to 3.38. The BI of these patients was better than of those who received treatment in the United States (overall mean Body Image Scale score: 6.97, while receiving active treatment combined with HT or HT only; Harrington et al., 2009) and in Italy (overall mean Body Image Scale score: 8.86, at cancer stage T1–T3, while receiving active treatment combined with HT; Saini et al., 2013). In the current study, the highest-scoring aspect of BI dissatisfaction was self-consciousness about appearance. After receiving treatment, the question item that received the lowest score was avoiding people based on one’s appearance. This result is similar to the findings of a study in Italy (Saini et al., 2013). In contrast, the highest-scoring aspect of BI dissatisfaction in the United States was feeling less sexually attractive; the item with the lowest score was dissatisfaction with the appearance of a scar (Harrington et al., 2009). There are two potential reasons for the different highest and lowest aspects of BI dissatisfaction among Chinese patients in the current study compared with patients from other countries. First, more than 70% of the patients in the current study had Stage IV cancer and were more concerned about their health than with sexual attractiveness and sexual function (Chien and Huang, 2022). Second, 100% of the patients were receiving HT only. Compared with active treatments combined with HT, HT is less invasive, does not require removal of the prostate, and does not result in obvious scars and urinary incontinence (Bowie et al., 2022).
HT involves an orchiectomy and medical castration (Cornford et al., 2021). In traditional Chinese culture, body, hair, and skin are given by one’s parents and should not be “disrupted”; further, individuals need to maintain their whole body even through death (Shih, 1996). Hence, this study supposed that, compared with men who receive medical castration, men who receive a bilateral orchiectomy would experience more BI dissatisfaction, such as feeling that the treatment led to their body’s being less whole. This hypothesis, however, was not supported. One possible reason is that men with a subcapsular orchiectomy maintain the appearance of having an ordinary scrotum.
The results of this study showed that hormonal symptoms and distress among men with prostate cancer, such as distress caused by hot flashes, breast tenderness/enlargement, depression, lack of energy, and changes in body weight, were significantly associated with BI dissatisfaction. Previous studies have found that side effects due to HT can cause men to perceive their physical selves in different ways. For example, physical changes toward femininity (e.g. breast enlargement, testicular reduction, penile shortening), hot flashes, fatigue, decreased muscle strength, increased BMI, and sexual dysfunction were associated with physical changes that altered not only a patient’s physical appearance and function but also his self-perception of the masculine body and led to BI dissatisfaction (Cash, 2008; Harrington et al., 2009; Mainwaring et al., 2021; Taylor-Ford et al., 2013; van den Driessche et al., 2016). BI dissatisfaction affects health-related quality of life in patients with prostate cancer who receive HT (Harrington and Badger, 2009; Taylor-Ford et al., 2013). Providing information about the side effects of HT and on prevention and coping strategies, before or at the beginning of treatment, can help these patients to manage, prevent, and mitigate the side effects caused by HT (Gentili et al., 2019; Hamilton et al., 2015; Wibowo et al., 2020). This can contribute to preventing BI dissatisfaction among patients with prostate cancer who receive HT.
In contrast to previous studies on other cancer patients (Arıkan et al., 2020), this study did not find a significant relationship between general self-efficacy and BI dissatisfaction, and, as such, the hypotheses of the study were not supported. This may be because this study measures general self-efficacy instead of self-efficacy for a specific disease or symptom management. Self-efficacy can contribute to an individual’s adopting certain health behaviors, such as exercise (Bandura, 1977), which may result in less BI dissatisfaction (Cash, 2008; Hamilton et al., 2015; Langelier et al., 2019). A study on patients with breast cancer has shown that better self-care-related self-efficacy contributes to an improved BI dissatisfaction (Arıkan et al., 2020). According to self-efficacy theory (Bandura, 1977), patients with better self-care-related self-efficacy are expected to have higher self-confidence in self-care of the symptoms and issues related to the disease and treatment (Bandura, 1977; van Dongen et al., 2020). This may improve the physical symptoms and distress and maintain the body’s appearance and function in patients with prostate cancer, thereby reducing their BI dissatisfaction (Cash, 2008). Further research is needed, however, to explore the relationship between self-efficacy and BI.
To the best of their knowledge, the authors believe that this study, which used a structured questionnaire and combined cross-sectional and longitudinal data, is the first to describe the BI of patients with prostate cancer who receive HT. This study characterizes the BI of these patients and can be used as a reference for future research and clinical care. This study, however, also has certain limitations. First, the current study used quantitative methods, which do not provide insight into a patient’s subjective feelings and experiences regarding BI. Therefore, a mixed methods design is recommended to obtain a holistic view of the BI of these patients. Second, the number of prostate cancer patients who receive HT only is small when compared to those who receive radiotherapy and radical prostatectomy. Therefore, both longitudinal and cross-sectional studies were used simultaneously to understand changes in BI over time and the influencing factors. However, the findings in the present longitudinal study are limited by the small sample size used, making it difficult to interpret causality among the variables of interest. In the future, large-sample studies are needed. Third, a convenience sampling design was adopted in the current study, and only patients with prostate cancer who received HT were recruited in the two hospitals, while patients who received other types of treatment were excluded. Therefore, the results of this study cannot be extrapolated to patients who receive other concurrent treatments. In addition, more than respectively 70% or 90% of the patients in the cross-sectional and longitudinal studies had Stage IV cancer, limiting the ability to generalize the results to patients with localized prostate cancer. Future studies should include patients with prostate cancer who are in various cancer stages and receiving different treatments in multiple settings. Finally, this study used a limited number of variables, for example, sexual dysfunction, masculine self-esteem, hegemonic masculine ideas, based on the small sample size. Previous studies have supported the relationships between sexual dysfunction and BI dissatisfaction (Bowie et al., 2022; Mainwaring et al., 2021), lower masculine self-esteem and lower hegemonic masculine ideas (Gentili et al., 2022), and lower masculine self-esteem and BI dissatisfaction (Langelier et al., 2018). Thus, the effects of sexual function, masculine self-esteem, and hegemonic masculine ideas on BI were not investigated in the current work. Future studies should investigate these variables to understand their effects on BI in different ethnic groups.
In summary, the percentage of BI dissatisfaction ranged from 6.1% to 17.2%. Hormonal symptoms and distress are correlated with BI dissatisfaction in patients with prostate cancer who receive HT. In the future, management strategies for prevention and improvement of hormonal symptoms and distress can be provided before or at the beginning of treatment to mitigate their impact on the patients’ BI.
Research on the BI of patients with prostate cancer who receive HT in Asian countries is limited, but clinical implications can be drawn. The results of this study highlight the importance of identifying and assessing the problems related to the BI of these patients and of teaching them to prevent or reduce the effects of hormonal symptoms and distress on their BI. It is recommended that healthcare professionals take an open-minded approach, that is, to listen, empathize, and assess patients’ perceptions and feelings about their BI. The medical team can provide tailored health education and interventions before or during the initial stages of HT to help patients to understand the advantages and disadvantages of the current treatment methods and their possible side effects and coping strategies. Previous studies have shown that psychological intervention can help to improve the BI of breast cancer patients (Sebri et al., 2021), and aerobic or resistance exercises contribute to improving BI in patients with prostate cancer (Langelier et al., 2019). Hence, these interventions can help to reduce the negative effects on patients’ BI and improve healthcare quality.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053231223930 – Supplemental material for Body image in patients with prostate cancer undergoing treatment with hormone therapy: Observational study using both a cross-sectional and longitudinal design
Supplemental material, sj-docx-1-hpq-10.1177_13591053231223930 for Body image in patients with prostate cancer undergoing treatment with hormone therapy: Observational study using both a cross-sectional and longitudinal design by Pei-Yi Chen, Kuan-Lin Liu, Cheng-Keng Chuang, Chun-Te Wu, See-Tong Pang, Ying-Hsu Chang, Kai-Jie Yu and Ching-Hui Chien in Journal of Health Psychology
Footnotes
Acknowledgements
We are grateful to the National Science and Technology Council, Taipei City, Taiwan, R.O.C. for subsidizing our study.
Author contributions
Pei-Yi Chen: Resources, Formal Analysis, interpretation of data, Writing—Original Draft. Kuan-Lin Liu: Conceptualization, Resources, Formal Analysis, interpretation of data, Writing—Original Draft. Ching-Hui Chien: Conceptualization, Methodology, Resources, Formal Analysis, Data Curation, Visualization, Writing—Original Draft, Review and Editing, Supervision, Project Administration, Funding Acquisition. Cheng-Keng Chuang: Conceptualization, Resources, Writing—Review and Editing. See-Tong Pang: Resources, Writing—Review and Editing. Chun-Te Wu: Resources, Writing—Review and Editing. Ying-Hsu Chang: Resources, Review and Editing. Kai-Jie Yu: Resources, Review and Editing.
Data sharing statement
Data supporting this study’s findings are available from the corresponding author upon reasonable request. The data are not publicly available due to the consideration of ethics, the researchers shall maintain the privacy of the participants, and research data should be used only for academic articles.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Science and Technology Council, Taipei City, Taiwan, R.O. C. (project no. NSTC 106-2314 -B-227-009; 107-2314-B-227-007; 108-2628-B-227-001).
Ethics approval
The study project was approved by Chang Gung Medical Foundation Institutional Review Board (No. 201602024B0C505).
Informed consent
All participants verbally agreed to participate in this study and provided written informed consent.
Consent to publish
All authors agreed to publish this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.