
Abstract
The extent to which parents experience guilt related to their child’s health may depend on their perceptions of their contribution to these outcomes. The impact of the child’s “other” biological parent’s (OBP) contribution to child health on guilt responses is understudied. Some models posit a diffusion-of-responsibility process, while others favor a heightened-risk-heightened-guilt model. The present study examines how perceived OBP contribution to child risk affects guilt among a sample of parents with self-reported overweight. Parents who perceived their child’s OBP to also have overweight experienced more guilt for passing down genetic and family environment-based obesity risk to their child, which suggests that perceptions of shared risk contribution promote guilt-related outcomes. Additionally, risk information endorsing a gene-environment interaction liability framing was the most responsive to OBP weight status. These results support a heightened-risk-heightened-guilt process. Future work should consider guilt when developing child health interventions to avoid undesirable emotional outcomes among parents.
Introduction
Guilt is a prevalent emotion experienced by parents, particularly in the context of child health (Constantinou et al., 2021; Gorlick et al., 2021; Jackson et al., 2007). Researchers have long regarded guilt as an emotion that can spur positive, reparative behavior (Donohue and Tully, 2019). It has been theorized that inducing parental guilt might elicit child-focused health behavior change (Persky et al., 2015). However, emerging evidence refutes this claim and suggests that parental guilt, at least when related to child weight and feeding behavior, may instead be associated with maladaptive coping behaviors like self-blame and emotional overeating (Craven and Fekete, 2019; Hagerman et al., 2020). Because evoking parental guilt in this context is generally an undesirable outcome, it is crucial to identify factors that influence guilt responses related to child weight and feeding. This, in turn, can inform approaches for health communication, family-based interventions, and related programs to minimize or address parental guilt. The focus of the current report is the influence of parental co-contribution to child risk for obesity later in life across multiple frames of risk communication.
Individual parents are almost never solely responsible for child weight outcomes and obesity risk. First, both biological parents pass down genetic material that can predispose children to obesity. As such, responsibility for genetic liabilities is generally assumed to be shared between both biological parents (Hopper, 2005). Second, parents shape the family home in which children are exposed to environmental risk factors. While some parents bear sole or primary responsibility for this, multiple parents or family members often jointly contribute to a child’s suite of environmental experiences (Xiao and Loke, 2021). Parents who do not directly participate in child-rearing might still bear responsibility for shaping the child’s environment through their lack of contribution. However, there is limited literature on the relationship between shared responsibility for child risk and parental guilt responses.
Guilt for genetic contributions
While genetic and environmental factors interact to determine one’s risk for common conditions like obesity (Ellulu and Jalambo, 2017), these elements are more frequently discussed individually. As such, guilt related to genetic inheritance has been studied as its own construct. Parents often report experiencing guilt due to the notion that they have passed down genes that increase their child’s risk of disease (Fanos and Puck, 2001). It is notable that parents themselves cannot be held responsible for the “creation” of their genetic code as this is passed down from previous generations. Regardless, such guilt frequently emerges particularly when the line of transmission appears to be clear (James et al., 2006). For example, parents who perceive themselves to have overweight or obesity tend to express heightened levels of guilt and self-blame related to their child’s future health and obesity risk (Bentley et al., 2017; Hollister et al., 2019; Hughes et al., 2010; Persky et al., 2021). No research to date, however, has examined whether and how parents’ perceptions of the child’s other biological parents’ contribution to risk influences the onset of guilt experiences.
Guilt for environmental contributions
Parents also express guilt for their role in creating the home food environment for their children (Boutelle et al., 2012; Davis et al., 2018). This parental guilt has primarily been explored in a way that reflects traditional gender roles. Mothers in particular tend to experience self-blame due partially to perceived external judgment for their failure to create a healthy home food environment (Gorlick et al., 2021; Jackson et al., 2007; Roberts et al., 2021) and for specific food choices they make for their children (Damen et al., 2020; Johnson et al., 2011). Fathers’ experiences of guilt related to child feeding are not as well-studied (Harris et al., 2020; Hollister et al., 2019), and earlier literature suggests that fathers may be less likely than mothers to express guilt about child feeding (Blake et al., 2009). However, there is limited work on the relationship between shared responsibility and guilt, and on the role of gender or gender roles in these processes.
Models of shared responsibility and guilt
There are multiple potential mechanisms through which perceptions of parental contribution could elicit feelings of guilt. The first possibility is that sharing perceived responsibility with a child’s “other” biological parent (OBP) could result in diffusion-of-responsibility, wherein individuals feel less responsible for a given situation when they perceive others to share responsibility. This, in turn, reduces the likelihood of experiencing self-blame or spurring reparative action (Hayashida et al., 2020; Rowan et al., 2022). As such, this process should result in less guilt on the part of the parent. One previous study demonstrated that mothers expressed more guilt about the genes they passed down and about their child feeding practices when they received educational information suggesting that they, alone, had contributed to their child’s heightened obesity risk as opposed to when that risk was perceived to be shared with the child’s OBP (Persky et al., 2015). This study did not evaluate mechanisms contributing to guilt levels, but the pattern of outcomes suggests a diffusion-of-responsibility interpretation.
A second possibility is that perceiving shared responsibility with one’s child’s OBP would result in increased self-blame and thus increased guilt. This relates to the notion that the number of contributors to child risk is not independent from the nature and level of that risk. For example, if both biological parents have higher weight and are perceived to contribute genes that increase a child’s risk of developing obesity, the responsibility is shared between them, and the level of risk associated with that responsibility is higher. This is because the child with two parents of higher weight, by definition, has a family history of overweight on both sides of the family, which is associated with higher risk (Magnusson and Rasmussen, 2002; Whitaker et al., 1997). A similar argument can be made for the family environment. For example, if both parents are predisposed to sedentary behavior and this becomes a family norm, responsibility may be perceived to be shared, and the child’s risk is higher because they have two parental models for sedentary behavior (Carson et al., 2020; Garriguet et al., 2017). While these examples are over-simplified, typically dual parental contribution to a child’s obesity risk is associated with a higher degree of risk (Reilly et al., 2005). As a result, parents who perceive that they and the child’s OBP dually contribute to the child’s risk may exhibit heightened risk perception for the child, wherein the higher likelihood or severity of negative outcome can elicit greater levels of guilt (Becheur and Valette-Florence, 2014; Chédotal et al., 2017).
These two processes may present a trade-off for the elicitation of parental guilt, or one may predominate. One factor that might influence these outcomes is the nature of the focal risk information or health education that parents are responding to. There is little literature on how such processes might unfold, and further exploration is needed. The role of genetics and genomics in risk prediction for obesity and other common health conditions is growing rapidly (Bidzimou and Landstrom, 2022; Yu et al., 2022), making it crucial to understand how messages that rely on genetic and/or gene-environment interaction risk framing may differentially trigger guilt. For example, risk information focused on the role of genetic factors influencing child risk may draw attention to the cumulative nature of genetic liabilities on obesity risk (Feldman et al., 2014; Schneiderman et al., 2014), prompting a focus on increases in child risk related to shared parental contribution.
The current study
This study evaluates parental guilt specific to genetics and the family home environment among parents who reported having overweight and who received a child-focused message regarding obesity risk later in life. We assessed the influence of parents’ perception that the child’s OBP also had overweight on guilt, both at baseline and in response to receipt of health education (Persky et al., 2021). We approached this study with several research questions.
1. Does parental perception of their child’s OBP’s weight influence their baseline guilt for passing down risk-promoting genes and/or for risk conveyed by the family home environment?
2. Does parental perception of their child’s OBP’s weight influence guilt resulting from exposure to educational materials about child risk? a. Do guilt responses depend upon the content of the risk messages (genetic focus, family environment focus, gene-family environment interaction focus, or control)? b. Are identified relationships mediated by parents’ risk perception for their child (cognitive and affective) and/or self-blame?
3. Are responses more consistent with a “diffusion-of-responsibility” or a “heightened risk-heightened guilt” process?
Method
Participants
Participants were recruited to a larger experimental trial which assessed the influence of obesity risk education on child feeding behavior among parents with self-reported overweight (Persky et al., 2021). We included all participants in the original trial in the present analysis with the exception of those who did not respond to relevant questions (N = 180; n excluded = 10). Participants were recruited by the study team from the Washington, D.C. metro area via online advertisements, posted flyers, and word-of-mouth, and all were paid for their participation. Inclusion criteria included being the parent of a 3–7 year old biological child of any weight where the participant reported having overweight, at least some responsibility for child feeding, and the ability to read and write in English. Exclusion criteria included having a vestibular or seizure disorder, high propensity for motion sickness, known pregnancy, uncorrected poor vision or hearing, past or current eating disorder, or participation of another household member or another biological parent of the relevant child in the study. Participants were block randomized such that each educational condition contained approximately half mothers and half fathers. This study was approved by the IRB of the National Human Genome Research Institute.
Procedure
Eligible participants were consented online and completed a pre-test questionnaire remotely. The pretest questionnaire included baseline measures of attitudes, beliefs, and practices related to child feeding and perceived obesity risk, as well as demographic characteristics. Parents were asked to consider one of their children (between 3 and 7 years old) during the study as the focal child while answering questions. During a lab visit, we randomly assigned participants to view a presentation on child obesity risk that focused on a particular mechanism through which risk is conferred: genetics, family environment, or a gene-family environment interaction. There was also a control condition that provided education on child health related to nutrition, physical activity, and sleep. Education was communicated through a PowerPoint presentation with recorded audio. Participants in the three risk-provision conditions received education indicating that their child’s risk for obesity was heightened due to the parent’s own elevated weight status. This educational information stated that if the child’s OBP also had higher weight, the child’s risk was additionally increased (see Figure 1). This information was taken from previous research (McBride et al., 2013) and is based on epidemiological data linking parental weight status with child obesity risk (Magarey et al., 2003).
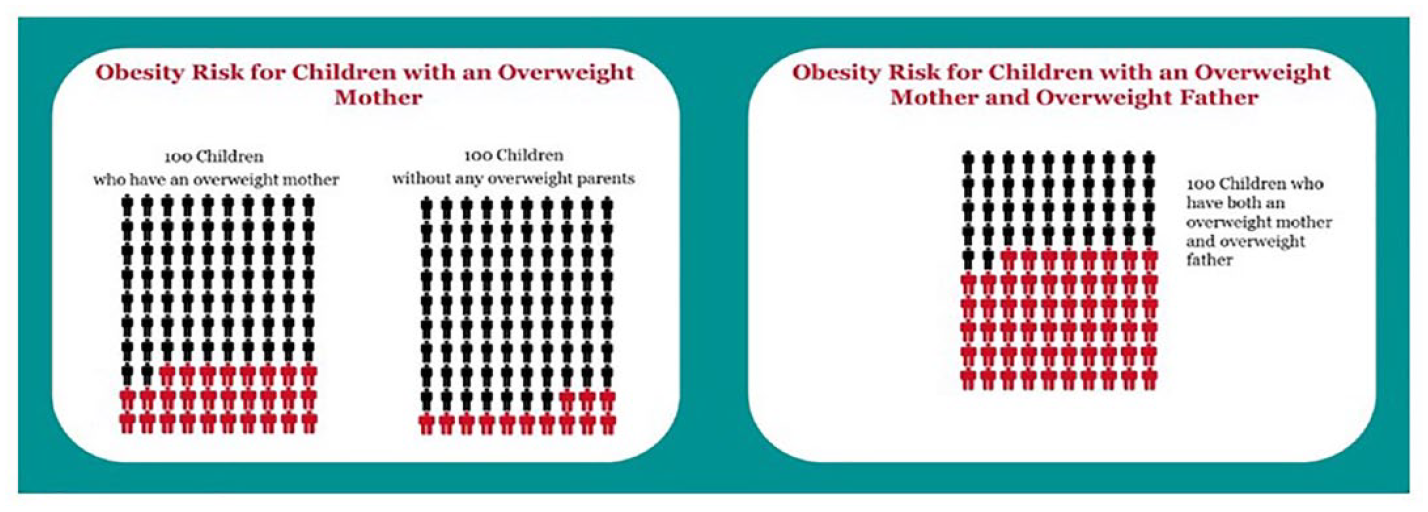
Obesity risk education related to the number of biological parents with overweight (mother version).
We matched materials such that mothers were referenced when participants were mothers and fathers were referenced for father participants. These figures were compared with the risk level for a child with two lean biological parents. Rather than asking parents to indicate which scenario best fit their child. We presented parents with all three risk levels.
Participants then completed a questionnaire about their reactions to the educational information. There were additional study components, though no data from these elements are included in the current analysis. More information about the study and content of the information modules can be found elsewhere (Persky et al., 2021).
Measures
Demographics and weight status were collected at eligibility screening and baseline via online questionnaire. Participants’ gender was assessed as male, female, or “other” at screening in response to the prompt “which gender do you identify with.” This resulted in categorization as mothers versus fathers in the trial; no participants selected “other.” To assess perceived weight status, parent participants rated the weight of themselves, their child, and the OBP on a five-point scale from “very underweight” to “very overweight” (Squiers et al., 2014). This was dichotomized into a category for “overweight” versus “non-overweight” for the child and OBP. Because all parent-participants were required to identify as overweight or heavier to be eligible for the study, we stratified participants into “overweight” versus “very overweight.”
Guilt was assessed using face-valid single items, both at baseline and following provision of risk education. These were created by the research team as no suitable measures existed. For example, “I feel guilty about the genetic risk for obesity that I may have passed down to [child name].” Responses were collected on a 1 to 7 scale from “strongly disagree” to “strongly agree.” We assessed self-blame similarly; we asked, “How much do you blame yourself for passing obesity genes to [child name]?,” and participants responded on a 1 to 7 scale from “not at all” to “a lot.” A similar item was used for family environment-related self-blame. These items were only collected following educational information provision. Risk perception (both cognitive and affective) was assessed after education provision. This consisted of two items assessing cognitive risk perception and two for affective risk perception for the child’s future obesity risk. Responses were assessed on a 1 to 7 scale (1 was lowest, 7 was highest). Items were adopted from previous work (Hagerman et al., 2020).
Data analysis
Demographic differences by OBP weight status were assessed by chi square and t-tests (see Supplemental Table S1). Relationships between OBP’s weight status and guilt were assessed through ANCOVA controlling for relevant pre-test levels of guilt, the participant-parent’s own weight status, the focal child’s weight status, and whether the participant-parent was living in a partnership with the child’s OBP. Change in guilt from baseline to post-education was assessed with paired-sample t-tests. Influence of the OBP’s weight status, the participant’s gender, and risk message type were assessed on primary dependent variables through ANCOVAs controlling for factors noted above plus relevant pre-test levels of guilt. This approach was also used to assess the effect of education type and OBP weight status on risk perception and self-blame, though the models did not contain a pre-test version of the measure. Mediation analyses were conducted using PROCESS (Hayes, 2022). For both genetic and family environment guilt, we used PROCESS model 8 (Supplemental Figure S2(a) and (b)), entering affective risk perception, cognitive risk perception, and self-blame as parallel mediators. Covariates listed above were also included in mediation models. The alpha level was held at p < 0.05 for all analyses.
Results
Demographics
The study sample was split evenly between participants who identified themselves as male and female. Participants who identified themselves as White tended to have OBPs with higher weight (χ2 = 5.79, p = 0.016) and Asian participants tended to have OBPs with lower weight (χ2 = 4.89, p = 0.027). There were no other significant differences by OBP weight status. Other demographic differences are reported in Supplemental Table S1.
Influence of OBP weight status on guilt about passing down genetic risk
There was no significant effect of OBP weight status on guilt about passing down genetic risk at baseline. Reported genetic guilt was lower following education than at baseline (t(188) = 4.50, p < 0.001) (see Table 1). In response to educational information, there was a main effect of OBP weight status on guilt about genetic risk such that parents who reported that the child’s OBP had overweight had higher levels of guilt (F(1,160) = 6.37, p = 0.013). There was also a significant interaction between OBP weight status and education type (F(1,160) = 6.34, p < 0.001). OBP weight was associated with a difference in guilt elicited in the genetic (F(1,168) = 4.37, p = 0.038) and the gene-family environment interaction (F(1,168) = 21.68, p < 0.001) groups but not the other two groups (see Figure 2). There were no other main effects or interactions.
Descriptive statistics by OBP weight status; n (%) or M (SD).
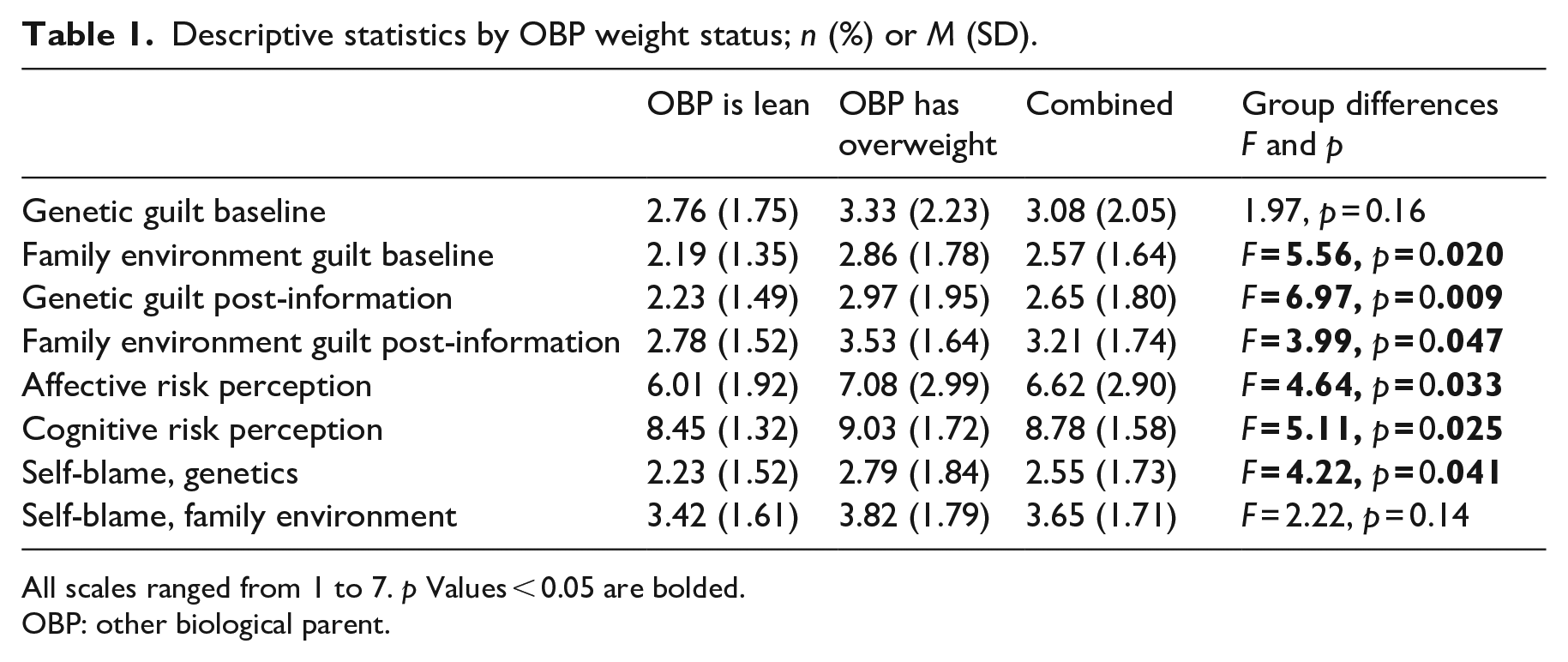
All scales ranged from 1 to 7. p Values < 0.05 are bolded.
OBP: other biological parent.
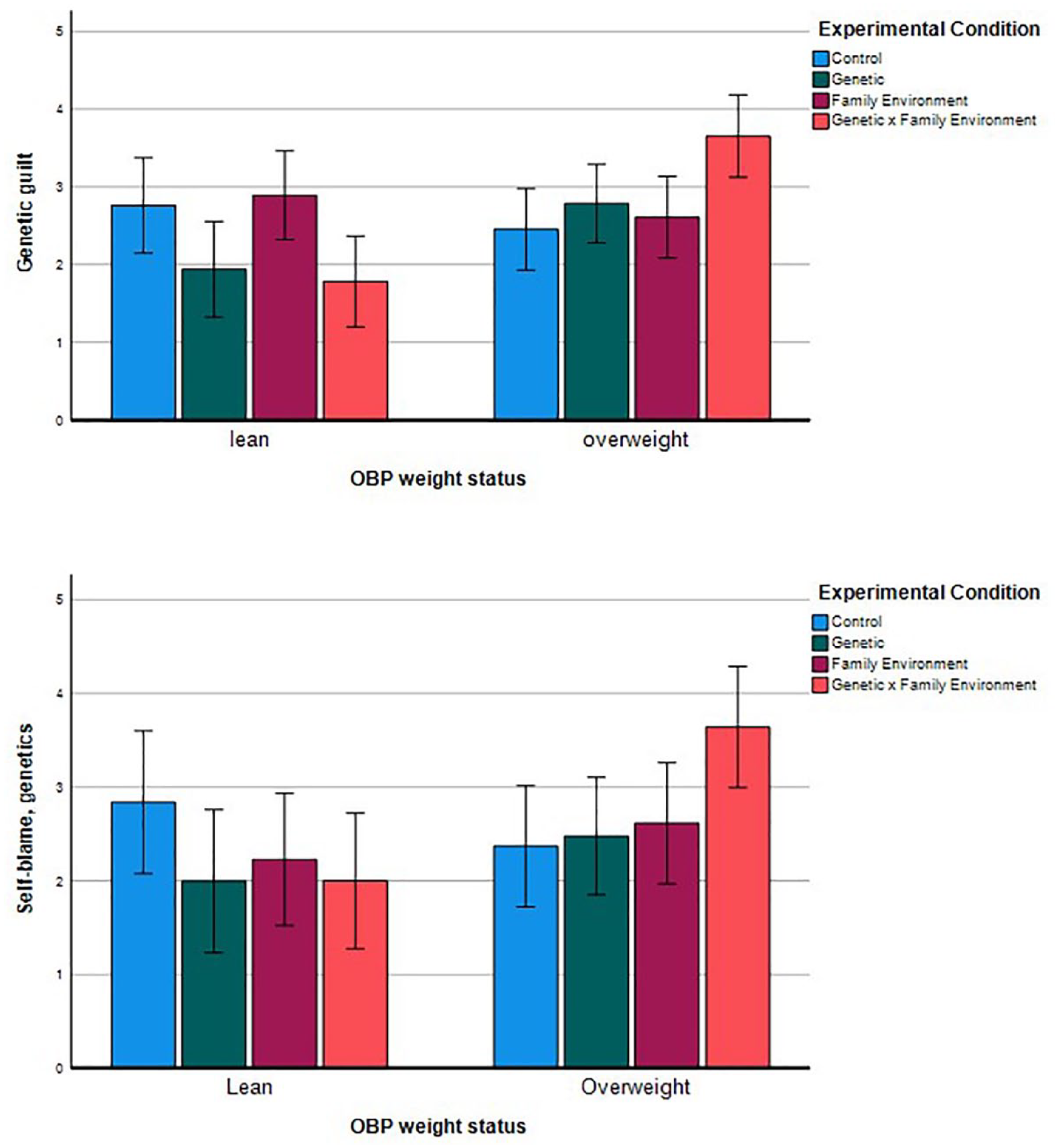
Genetic guilt and genetic self-blame by group.
Influence of OBP weight status on guilt about the family environment
At baseline, there was a significant effect of OBP weight status on guilt related to the home environment such that parents who reported that the OBP had overweight reported higher levels of guilt; (F(1,176) = 6.13, p = 0.014). Family environment guilt increased from baseline to post-education provision (t(188) = 3.59, p < 0.001). In response to educational information, there was a main effect of OBP weight status on guilt about the family environment such that parents who reported that the child’s OBP had overweight reported higher levels of guilt (F(1,160) = 4.69, p = 0.032). There were no other significant main effects or interactions.
Influence of OBP weight status on risk perception and self-blame
Risk perception
There was a main effect of OBP weight (F(1,169) = 4.64, p = 0.033) and an interaction between educational type and OBP weight status on affective risk perception (F(1,169) = 3.30, p = 0.022). Affective risk perception was higher when the OBP was reported to have higher weight, and this was driven by participants in the gene-environment interaction education group (F(1,169) = 9.73, p = 0.002). See Supplemental Figure S1 for details. For cognitive risk perception, there was a significant main effect of OBP weight (F(1,169) = 5.11, p = 0.025) such that cognitive risk perception was higher when the OBP had overweight. There was no interaction.
Self-blame
There was a significant main effect of OBP weight status (F(1,169) = 4.22, p = 0.041) as well as a significant interaction with education type (F(1,169) = 3.09, p = 0.029) on self-blame for passing down genetic risk. Self-blame for passing down genetic risk was higher when the OBP was perceived to have overweight; this was driven by the gene-environment interaction group (F(1,169) = 11.17, p = 0.001). See Figure 2 for details. There were no significant main effects or interactions related to self-blame for the child’s home environment.
Mediation analysis
Mediation analyses were conducted for genetics-oriented and family-environment-oriented guilt in separate models, each containing all three potential mediators (see Supplemental Figure S2 for models tested). Follow-up moderated mediation analyses were then conducted for genetics-oriented and family-environment oriented guilt in separate models, containing education messaging condition as a moderator, and all three potential mediators in parallel (Supplemental Figure S2).
Main effects
Analysis revealed a direct effect of OBP weight status on genetic guilt (B = 0.26, SE = 0.12, t = 2.09, p = 0.038). No indirect effects of OBP weight status on genetic guilt through the mediators of affective risk perception, cognitive risk perception, and self-blame were found. See Supplemental Table S2 for details.
Analysis revealed no direct effect of OBP weight status and no indirect effect of OBP weight status on family-environment guilt through the mediators of affective risk perception, cognitive risk perception, and self-blame. See Supplemental Table S3 for details.
Moderated mediation
Self-blame partially mediated the relationship between OBP weight status and genetic guilt, however this occurred only for parents in the gene-environment interaction educational condition (B = 0.86, SE = 0.38, CI = [0.14, 1.62]). A direct relationship between the gene-environment interaction educational condition and genetic guilt remained (B = 0.999, SE = 0.24, t = 4.14, p = 0.0001). No other relationships were found. See Supplemental Table S4 for details.
For family environment guilt, analysis revealed that affective risk perception partially mediated the relationship between OBP weight status and family-environment guilt, again, only for parents in the gene-environment interaction educational condition (B = 0.36, SE = 0.17, CI = [0.058, 0.74]). No other indirect or direct effects were found. See Supplemental Table S5.
Discussion
Parents’ perceptions of the extent to which their contribution to their child’s risk is shared versus unshared with the child’s OBP can significantly affect guilt responses in relation to both passing down genetic risk to their child and their role in establishing the child’s home environment. In both cases, the perception that the child’s OBP has higher weight was associated with heightened guilt for the participant-parent following the provision of obesity risk education materials. The patterns of results exhibited here are consistent with the interpretation that perceiving risk contribution to be shared leads to heightened guilt responses. We found no evidence supporting a diffusion-of-responsibility process in response to the concept of shared risk contributions. This finding suggests that educational materials, family-based interventions, and similar efforts which endorse the shared nature of risk conferral between parents may be more likely to increase parental guilt than reduce it. The generalizability of this finding will require further research.
For genetics-related parental guilt specifically, there were no pre-existing differences in guilt levels at baseline in relation to OBP weight status. This may be due in part to a general lack of consideration of genetic precursors for child weight among lay individuals or unawareness that parent weight history confers genetic risk to one’s children. Following the provision of risk education including a genetic component, genetic guilt decreased from baseline levels. While unexpected, this decline may reflect an understanding that genetic risk factors are not “created” by parents and thus parents may not be blameworthy for their transmission. It was not possible to establish the precise reason for this effect using data from the current study. Among the three risk frames presented, the gene-environment interaction frame was most responsive to OBP weight status. This may be due to its focus on the ways in which increased genetic risk provides an additional liability in the face of high environmental risk. Thus, to the extent that the OBP was perceived to have overweight, they could be viewed as having a greater or synergistic contribution to the child’s risk overall, consistent with the concept of gene-environment interaction.
Increased self-blame in the gene-environment interaction education condition was revealed to partially explain the influence of OBP weight status on genetic guilt. While risk perception was anticipated as the likely mechanism for increased guilt related to OBP weight status, self-blame is also an internally consistent response to receiving reports of synergistic, heightened risk education information for one’s child. Because risk perception was included in the mediation model alongside self-blame, this finding suggests that the self-blame in response to shared parental responsibility is based on factors other than enhanced child risk levels. Participant-parents may believe their own contribution to be more severe, or more worthy of blame, to the extent that their child’s future weight feels more precarious (due to combination of two risk frames and increased risk conferred by the OBP).
Turning to family environment guilt, OBP weight status influenced guilt levels at baseline. This distinction from genetic guilt may be due to a tendency to consider characteristics of the home environment more regularly within the context of child weight. Alternatively, it could be related to a perceived or real difference in characteristics of the home environment between families where the OBP is of higher versus lower weight. These explanations cannot be disentangled in the current analysis.
Upon provision of educational information, family environment guilt increased significantly, independent of the educational framework. Guilt related to the family environment may be so ubiquitous or normative (Pulakos, 1996; Reed, 2008) that any reminder of child risk is enough to increase its salience. Mediation models suggest that the effect of OBP weight on family environmental guilt was partially mediated by affective risk perception. The dominance of affective risk perception is sensible given the affective nature of guilt (Baumeister et al., 1994; Tangney et al., 2007). Interestingly, mediation analysis also revealed an indirect effect through affective risk perception for the gene-environment interaction educational frame specifically. This may again relate to heightened effects of explicitly naming of two routes of parental influence on child risk.
As mentioned above, all results from this analysis are consistent with the notion that perceptions of shared risk contribution with one’s child’s OBP results in increased, rather than decreased, guilt. This finding diverges from the only other known study in this domain (Persky et al., 2015) which found that mothers who were the sole contributor to their child’s risk via higher weight status exhibited higher levels of guilt than mothers who shared that contribution with the child’s OBP. This discrepancy likely occurred because in the current study, participants were explicitly given risk levels associated with both shared and unshared risk (i.e., whether the OBP had higher weight status or not). In the previous work, mothers received only the figure relevant for their family, as determined by previously reported OBP weight status. As such, participants in the previous study were unable to compare their child’s risk levels to that of other groups. These mothers may therefore have been unaware that their child’s risk would be elevated when the child’s OBP was of higher weight. This difference may be instructive for understanding contexts in which the current findings will or will not generalize.
While the literature on parental guilt largely focuses on mothers, the current study directly compared a balanced sample of mothers and fathers. It is therefore telling that we found no evidence of gender differences in parental guilt whatsoever, either at baseline or in response to educational information provision. This may be related to the fact that we explicitly recruited fathers for a child feeding-related trial with father-specific advertisements (Yaremych and Persky, 2022). This raises the possibility that attitudes and beliefs of the fathers in the current sample may not be representative of the general population of fathers. Regardless, there is at least subset of fathers whose guilt responses resemble those of mothers in the context of their children’s obesity risk. This is consistent with the larger literature which suggests that fathers’ parenting beliefs and behaviors are becoming more similar to mothers as gender roles and social norms evolve (Kuo et al., 2018).
Limitations
This analysis has several limitations that may temper conclusions. First, the sample size was determined by the original study from which data for the current analysis was drawn rather than specifically determined by anticipated effect sizes. In addition, many constructs were assessed with single- or two-item measures, as they were not the primary focus of the larger study. At the time of the study there were no validated scales available to assess parental guilt related to genetic or home environment risk conferral. Next, we observed variation in the demographic characteristics of parent-participants who reported that their child’s OBP was lean versus overweight. Participants who identified as White were more likely to report an OBP with overweight, while those identifying as Asian were more likely to report a lean OBP. We also found variation in the extent to which the child’s OBP is the person with whom the parent-participant is partnered at present and with whom the home family environment is created. The rates of partnership between the participant and the child’s OBP were high (87% on average), and there were no differences in rates of partnership associated with OBP weight status. This analysis was unable to address family composition and dynamics including child custody arrangements, families living apart, and related situations which may contribute to a more complex familial context. The parent-participant may not have been the child’s primary caregiver; inclusion criteria only required reports that the child lived with the participant “some of the time.” These factors require additional examination in their potential contribution to guilt processes. Finally, we were not able to differentiate between sex assigned at birth and gender identity among parent-participants or among OBPs, so while OBPs are, by definition, opposite sex from parent-participants, there may be undetected differences in gender identity for some participants.
Conclusion
In all, the current analysis found no evidence supporting a diffusion-of-responsibility effect wherein guilt would be reduced when responsibility is shared between biological parents. This counters suggestions that family-based models of risk diffusion might naturally reduce guilt. In the context of guilt related to genetic inheritance, heightened parental guilt was especially likely when we framed risk messages as an interaction between genes and the environment. We found similar, though indirect, effects for family environment-related guilt. The use of interactive causal framing is expected to grow in the future because it is more accurate than single-cause models, is necessary for informing precision medicine approaches, and is a recommended approach for risk communication (Condit and Shen, 2011; Li et al., 2019; Persky et al., 2021; Sørensen et al., 2022). The current findings suggest that it might be useful, or even necessary, to explicitly address guilt among parents in conjunction with education about child risk to circumvent undesirable parental guilt responses.
Supplemental Material
sj-jpg-1-hpq-10.1177_13591053241233336 – Supplemental material for How shared versus unshared parental contribution to child risk influences guilt responses
Supplemental material, sj-jpg-1-hpq-10.1177_13591053241233336 for How shared versus unshared parental contribution to child risk influences guilt responses by Kaylee Foor, Siri Ravuri and Susan Persky in Journal of Health Psychology
Supplemental Material
sj-jpg-2-hpq-10.1177_13591053241233336 – Supplemental material for How shared versus unshared parental contribution to child risk influences guilt responses
Supplemental material, sj-jpg-2-hpq-10.1177_13591053241233336 for How shared versus unshared parental contribution to child risk influences guilt responses by Kaylee Foor, Siri Ravuri and Susan Persky in Journal of Health Psychology
Footnotes
Data sharing statement
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Intramural Research Program of the National Human Genome Research Institute.
Ethical approval
This study was approved by the IRB of the National Institutes of Health #10-HG-0076.
Informed consent
All participants provided informed consent prior to participation in this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.