
Abstract
Given the importance of physical activity (PA) for both physical and mental health, the present study characterizes post-9/11 veterans’ leisure-time PA engagement over time. Further, this study examines the relationship between PA and posttraumatic stress symptoms (PTSS), as well as whether this relation differs by gender and time since military discharge. This study was a secondary analysis of a 12-month longitudinal observational investigation of 410 (39.5% female) post-9/11 veterans. Participants completed self-report questionnaires at baseline and 12 months. Over a third of post-9/11 veterans were not engaging in any weekly leisure-time PA at study baseline and PA engagement significantly decreased in the subsequent year. The longitudinal relationship between PA and PTSS depended on both gender and time since military discharge. These results underscore the importance of considering both gender and time since discharge when tailoring interventions to support leisure-time PA as a key health habit in post-9/11 veterans.
United States military veterans may have long-term disadvantages in terms of both physical and mental health relative to their non-serving peers. During active duty, service members are likely to have better physical health due to factors such as a high magnitude of physical training and promotion of physical activity during service (Meadows et al., 2018). However, once separated from the military, veterans’ physical and mental health begins to degrade relative to non-veteran peers, a disparity that increases over time. Although some resources are available to support the transition from military to civilian life (e.g. VA Transition Assistance Program (TAP)), in general, veterans tend to report poorer general health and health-related quality of life and higher levels of health risk behaviors compared to their civilian counterparts (e.g. Hoerster et al., 2012b; Lehavot et al., 2012; Luncheon and Zack, 2012). A particular concern is the prevalence of obesity in Operation Enduring Freedom/Operation Iraqi Freedom/Operation New Dawn (OEF/OIF/OND) veterans, which is estimated to be up to 44%, a higher prevalence than in their non-veteran peers (Breland et al., 2017).
Along with these physical health concerns, post-9/11 veterans also experience mental health problems, including depression, anxiety, and substance misuse (Lippa et al., 2015). Additionally, posttraumatic stress disorder (PTSD) is a prevalent condition facing post-9/11 veterans, who often return from deployments with severe trauma-related reactions. PTSD prevalence in OEF/OIF/OND veterans has been estimated at 23% (Fulton et al., 2015). In addition to those meeting full diagnostic criteria for PTSD, many veterans experience subthreshold posttraumatic stress symptoms (PTSS). PTSS include hyperarousal, negative alterations in cognitions and mood, avoidance of trauma-related stimuli, and intrusive thoughts and memories of traumatic events (American Psychiatric Association, 2013). Even among veterans with PTSD, clinical presentations vary widely (Galatzer-Levy and Bryant, 2013); therefore, measuring level of PTSS, rather than a diagnosis of PTSD dichotomously, provides a useful method for characterizing trauma-related distress.
PTSS are disruptive and difficult to treat, and may adversely affect veterans’ physical health (see Ryder et al., 2018, for a review). While manualized psychological treatments for PTSD have been developed to help reduce PTSS (e.g. Resick et al., 2017; Rutt et al., 2018), many veterans experiencing PTSS either do not seek treatment due to stigma or experience barriers to accessing care (Ouimette et al., 2011). Further, research shows that there may be gender differences in the effectiveness of trauma therapies, with evidence that women may benefit more than men from psychotherapy for PTSD (Olff, 2017). For those who do seek trauma-focused psychological treatment such as cognitive processing therapy or prolonged exposure, many still do not experience significant symptom improvement from said treatment (Steenkamp et al., 2015), creating a need for other strategies to reduce veterans’ PTSS.
One potential avenue for addressing physical and mental health concerns common among veterans is engagement in regular physical activity (PA), which has been associated with better physical and mental health, including PTSS, across many populations (Czosnek et al., 2019; Penedo and Dahn, 2005). In particular, leisure-time PA has been associated with better physical and mental health outcomes (e.g. Gallagher and Carr, 2021; Parker et al., 2021). Emerging work has focused on the potential mitigating impact of PA on mental health conditions, particularly PTSD. The cross-stressor adaptation hypothesis (Sothmann et al., 1996) posits that exercise of sufficient intensity and duration can cause habituation of physiological responses to exercise (e.g. increased heart rate), which in turn results in adaptations in an individual’s stress response system and concurrent improved tolerance of other non-exercise stressors.
Similarly, PA has been theorized to lessen PTSS through interoceptive exposure to “distressing” physical sensations (LeBouthillier et al., 2016). Empirical studies have demonstrated cross-sectional associations between exercise and improved PTSS (e.g. Zen et al., 2012). The promising impact of PA on PTSS may be especially relevant for post-9/11 era veterans, for whom PTSD is a prevalent issue. Given the familiarity with exercise in military culture, PA may be an important potential alternative (or complementary) treatment for PTSS.
Despite the rigorous PA requirements of active-duty service members, as well as the well-established physical and mental health benefits of engaging in PA, veterans overall tend to have poor PA engagement after separation from the military. Changes in PA structure and routine may be similar to experiences of other populations, such as former college athletes (Reifsteck et al., 2013). The World Health Organization (WHO) recommends ⩾150 minutes/week of moderate/vigorous PA for adults (Bull et al., 2020). Cross-sectional studies have suggested that veterans may be more likely than non-veterans to meet PA recommendations, but the majority of veterans still do not meet these recommendations (e.g. Bouldin and Reiber, 2012; Littman et al., 2009). A more recent study from the Million Veteran Program suggests very low levels of PA, with almost 75% of participants having “poor” PA engagement and only 3.8% meeting the American Heart Association’s definition of “ideal” PA engagement (i.e. ⩾150 minutes/week moderate intensity or ⩾75 minutes/week vigorous intensity; Nguyen et al., 2018). These numbers suggest the percentage of veterans meeting PA guidelines is lower than that found in the general U.S. population (e.g. Harris et al., 2013).
Overall, numerous questions remain unanswered with regard to veteran PA. First, most research thus far has been cross-sectional, which precludes understanding changes in PA behavior over time as veterans are further from military discharge and have established post-military lifestyles. Given that PA engagement is a repeated-occurrence activity that tends to fluctuate over time, and that the health benefits of PA are largely dependent on the amount and frequency of engagement, examining PA cross-sectionally is insufficient for understanding engagement in PA and associated health benefits.
Second, of the few studies that have attempted to examine veterans’ change in PA over time, research is still methodologically limited (e.g. cross-sectional design with retrospective report of active-duty PA; Buis et al., 2011) or focused on small subsamples of veterans (e.g. postmenopausal women; Washington et al., 2016). Further, specifically with respect to the link between PA and PTSD, the longitudinal relationship between exercise and PTSS remains unclear (Whitworth and Ciccolo, 2016). Recent longitudinal observational studies suggest PA may help mitigate PTSS over time (e.g. LeardMann et al., 2011; Whitworth et al., 2017a), and intervention research (e.g. Björkman and Ekblom, 2022; Pedersen and Saltin, 2015) provides further support for the efficacy of PA in improving mental health. However, research specifically examining the longitudinal relationship between intentional leisure-time PA engagement and PTSS in post-9/11 veterans following separation from the military is needed, especially given the unique mental and physical health needs of post-9/11 veterans (e.g. Park et al., 2021; Waszak and Holmes, 2017)
Third, little is known about gender differences in veteran PA. Most studies examining veteran PA are based on primarily male samples (e.g. Bouldin and Reiber, 2012; Hoerster et al., 2012a), and thus do not reflect the rapidly increasing female veteran demographic in the U.S. military (U.S. Department of Veterans Affairs (VA), 2017). Importantly, research in the general population suggests gender differences in PA levels, such that men tend to engage in more exercise than females on average (e.g. Hickey and Mason, 2017), and recent cross-sectional studies of veterans also suggest a gender difference in physical fitness, with female veterans reporting poorer physical fitness and less frequent PA than male veterans (Harrington et al., 2019). Further, PA engagement declines at a faster rate for women with PTSD symptoms than for women without trauma exposure or without PTSD symptoms (Winning et al., 2017).
A recent report found that the top 10 conditions of female veterans in the middle-age bracket (the largest group of women veterans) include cardiovascular risk factors (Frayne et al., 2018). Given evidence that PA can reduce cardiovascular risk factors (Lee et al., 2014), the prevalence of cardiovascular conditions in this report suggests the need to examine health behaviors such as PA in this group specifically. Additionally, a recent review found an association between PA and improved PTSD in veterans and stressed the need for more evidence in representative samples including more female veterans (Hall et al., 2015). While some research indicates PA is associated with fewer PTSS in men than in women (Whitworth et al., 2017b), other researchers have recognized that the underrepresentation of women in exercise trials prevents full understanding of the role of gender in the impact of exercise on PTSS (Pebole and Hall, 2019). Further, it is unclear how gender stigma and discrimination in the miliary may indirectly impact later PA by way of negative mental health consequences (Foynes et al., 2013). Thus, extant work does not accurately reflect the increasing presence of women in the military nor those transitioning to veteran status, reflecting an important gap in the literature.
Overall, despite the many benefits of PA on physical and mental health, little research has examined leisure-time PA in post-9/11 veterans over time, nor specifically examined gender differences or the relationship between leisure-time PA and PTSS over time. A better understanding of the timing of these relationships and potential gender differences has important implications for interventions. The present study aimed to (a) characterize how leisure-time PA changes over time, including differences by gender and time since discharge; and (b) explore how baseline leisure-time PA relates to PTSS over time, including differences by gender and time since discharge, in a sample of post-9/11 veterans. Importantly, we examined PA in three clinically-relevant ways: (1) any versus no PA (Lloyd-Jones et al., 2010), (2) meeting the WHO recommendations of ⩾150 minutes/week versus not, and (3) amount of PA.
Method
Participants
The present study is a secondary data analysis of the Survey of Experiences of Returning Veterans (SERV). The SERV is an observational longitudinal study assessing post-deployment experiences and well-being in a nationwide sample of post-9/11 veterans. To be eligible for the SERV study, participants must have served in Iraq, Afghanistan, or surrounding areas or waters. Full details about the SERV cohort and procedures can be found in Park et al. (2021). To be included in the present study, participants data was required for baseline and 12-month assessments (i.e. complete cases analysis).
Procedures
This study was approved by the Institutional Review Board of the Department of Veterans Affairs. Post-9/11 veterans were recruited via various means including through Veterans Affairs (VA), Student Veteran Associations, Facebook, YouTube, community listservs, flyer postings, and word of mouth. The SERV study intentionally oversampled female veterans. Participants provided written informed consent prior to completing the questionnaires via telephone interviews.
Measures
Demographic information
Participants completed a self-report survey that included reports of age, gender, race, ethnicity, and time since last military discharge.
Leisure-time physical activity
Leisure-time PA was assessed with an adapted version of the International Physical Activity Questionnaire Short Form (IPAQ; Craig et al., 2003). Participants were presented with a description of vigorous activities (i.e. “activities that take hard physical effort and make you breathe much harder than normal”) and moderate activities (i.e. “activities that take moderate physical effort and make you breathe somewhat harder than normal”). At both baseline and 12-month follow-up, participants were asked to report how many days over the past week and how much time per day they engaged in moderate or vigorous activity solely for recreation, sport, leisure, or exercise. Leisure-time PA in the present study was a combination of moderate and vigorous activity and was assessed in three ways: 1) any PA (any engagement = yes; zero engagement = no); 2) PA engagement of ⩾150 minutes/week versus not; and 3) as average minutes per day.
Posttraumatic stress symptoms
The PTSD symptom checklist (PCL-Civilian; Wilkins et al., 2011) was used to assess PTSS at baseline and 12-month follow-up. The PCL-C is a widely used 17-item self-report questionnaire that corresponds with diagnostic criteria for PTSD. Participants rated their experience of each symptom in the past month on five-point Likert scales from 1 (Not at all) to 5 (Extremely). Items are summed to provide a total score. Internal consistency reliability was 0.96 and 0.97 at baseline and 12-month follow-up, respectively.
Data analysis plan
All analyses were conducted with SPSS Version 29. To first determine if there were any differences in baseline variables based upon study inclusion (i.e. completed baseline and 12-month assessments), a logistic regression model was created, predicting inclusion by baseline study variables. To describe our sample, means and standard deviations, medians and interquartile ranges, and frequencies and proportions were utilized where appropriate, and we assessed differences in study variables by gender using t-tests and chi-square tests where appropriate. To determine if PTSS changed over time, paired t-tests were conducted. To determine if gender predicted changes in PTSS, linear regression models were created predicting 12-month PTSS by gender while controlling for baseline PTSS.
To characterize leisure-time PA (Aim 1), we described (1) any versus no PA engagement, (2) PA engagement of ⩾150 minutes/week versus not, and (3) PA amount, at baseline and 12 months. We assessed differences by gender and time since military discharge using chi-square tests, Wilcoxon tests, and linear regression where appropriate. To determine if leisure-time PA changed over time, McNemar’s tests and paired Wilcoxon tests were conducted where appropriate. To determine if gender or time since military discharge predicted changes in PA, logistic and linear regression models were created where appropriate predicting 12-month PA by gender or time since military discharge separately while controlling for baseline PA.
To determine if the relationship between baseline PA (i.e. any engagement, ⩾150 minutes/week engagement, amount of PA) and PTSS at 12 months and changes in PTSS differed by gender and/or time since military discharge (Aim 2), a three-way interaction model was created using the SPSS PROCESS macro (Hayes, 2017). If any interactions were significant (p < 0.05), simple slopes of relationships were examined at short, moderate, and long times since military discharge relative to the sample, as estimated by the 16th, 50th, and 84th percentiles, respectively. For more robust estimates, bootstrapping was deployed for all models (k = 1000), and controlled for demographic covariates (i.e. age, race, and ethnicity). For all interaction models assessing change in PTSS, we predicted 12-month PTSS, controlling for baseline PTSS.
Results
Participant characteristics
A total of 673 participants completed the baseline survey and 410 completed both baseline and 12-month follow-up. Only participants who completed the baseline and 12-month follow-up surveys were included in the present study (n = 410). Participants who completed the 12-month surveys were 2.26 times likely to be men compared to women (p < 0.001) and 1.02 times likely for each unit decrease in PTSS at baseline (p < 0.001); all other ps > 0.09. See Supplemental Table 1 for full details.
In Table 1, we summarize and compare participant characteristics overall and as stratified by gender. Of the 410 included participants, the mean age was 35.8 years (SD = 9.1) and 39.5% were women. Additionally, 78.0% identified as White, 15.6% as Black or African American, 5.0% as Native American or Alaskan Native, 3.4% as Asian, and 1.2% as Native Hawaiian or Pacific Islander (note that individuals were able to select multiple racial identities, so percentages total over 100%). Few participants (12.2%) reported being Hispanic or Latinx. Most veterans’ last branch of military service was the Army (59.5%; n = 244), with fewer veterans being from the Air Force (14.6%; n = 60), Navy (13.2%; n = 54), or Marines (12.7%; n = 52). Men were younger (p = 0.02), more likely White (p = 0.02), and had marginally higher PTSS at 12 months (p = 0.05) but not at baseline (p = 0.20); all other ps > 0.24. Mean PTSS decreased from baseline (M = 46.1, SD = 18.4) to 12 months (M = 41.6, SD = 18.3), about an 8% change (p < 0.001), and did not differ by gender (p = 0.11).
Participant characteristics overall and as stratified by gender.
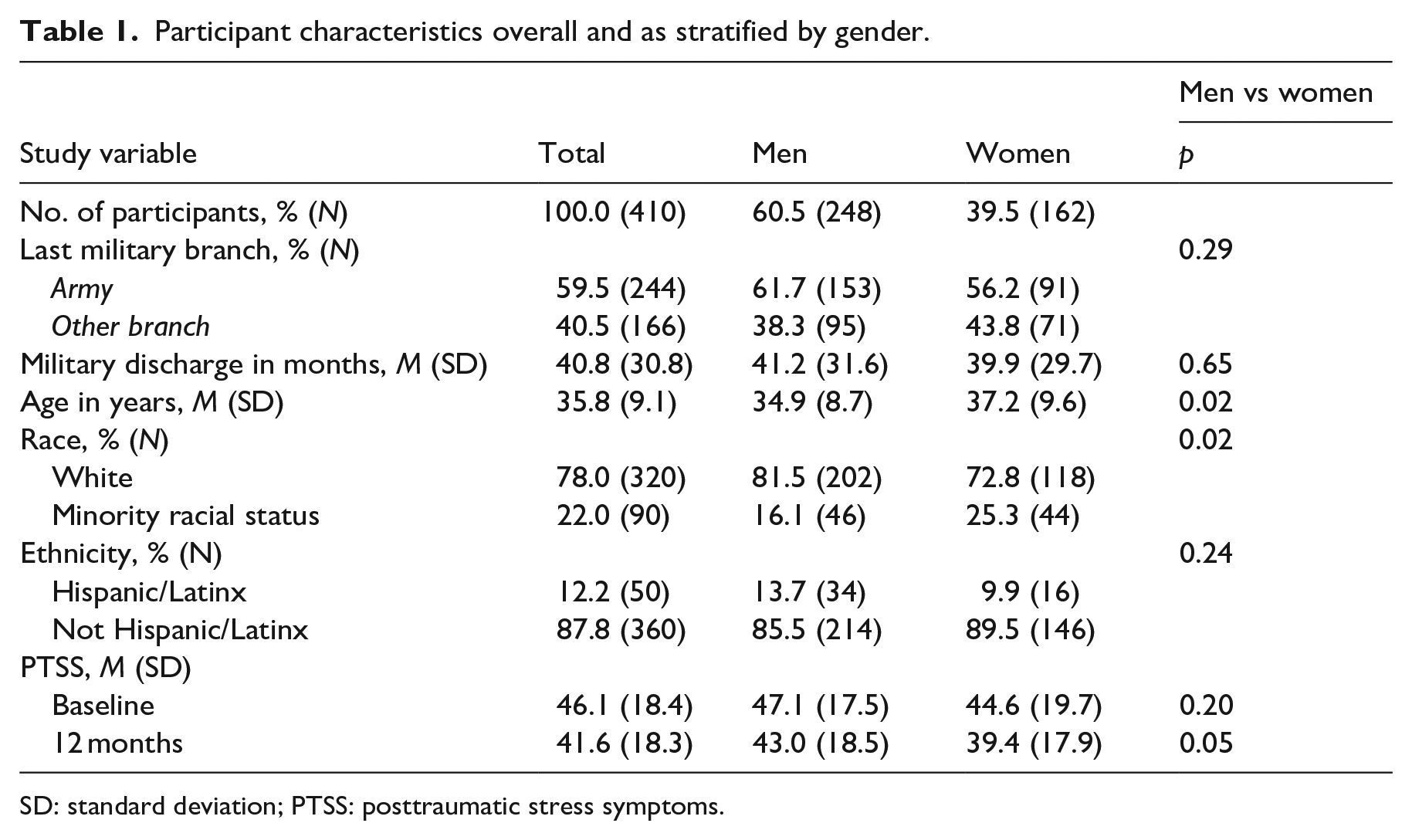
SD: standard deviation; PTSS: posttraumatic stress symptoms.
Aim 1: Characterizing physical activity in study sample
In Table 2, we summarize and compare PA as stratified by gender at baseline and 12 months.
Physical activity overall and as stratified by gender.
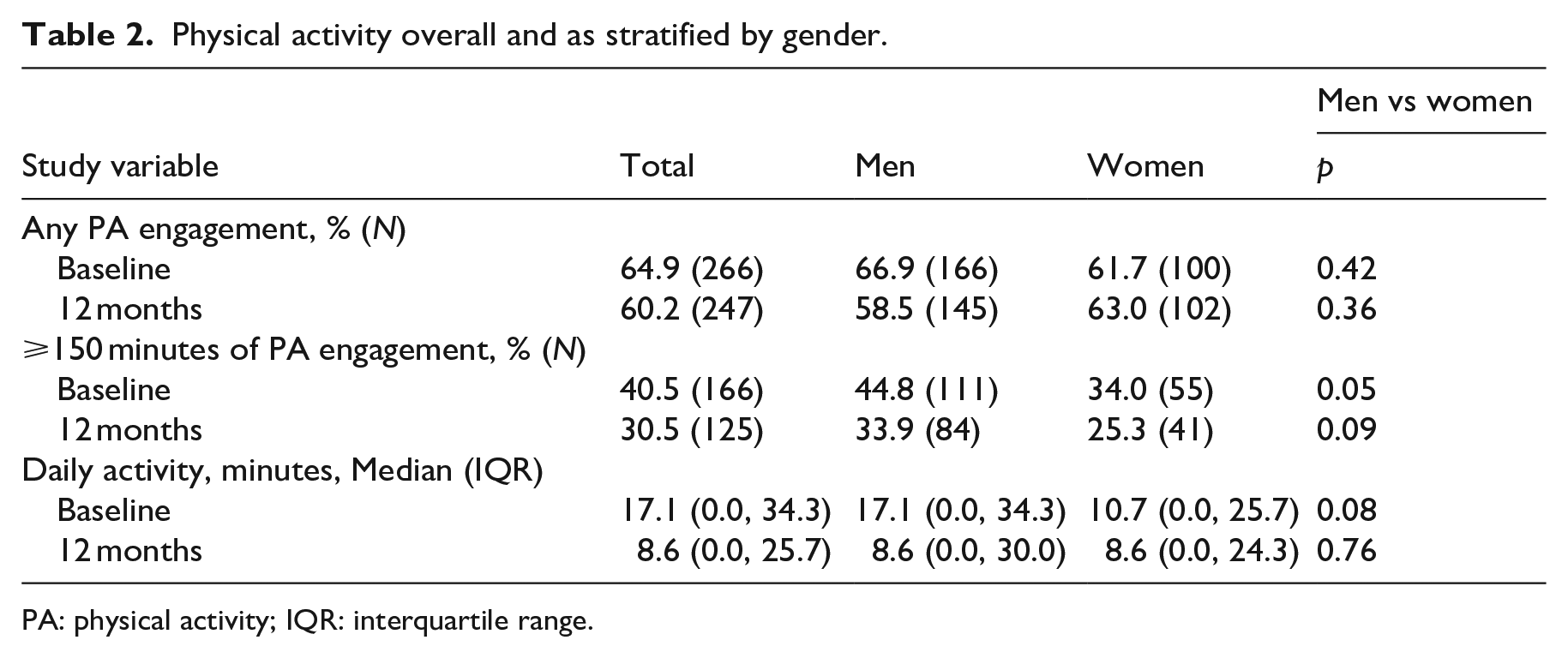
PA: physical activity; IQR: interquartile range.
Any PA engagement
About two-thirds of participants (65%; n = 266) engaged in any PA at baseline, and 60% (n = 247) engaged in any PA at 12 months. At baseline, 33% of male veterans (n = 82) and 38% of female veterans (n = 62) did not engage in any PA. At 12 months, 42% of male veterans (n = 103) and 37% of female veterans (n = 60) did not engage in any PA. Engagement in any PA did not differ by gender at either timepoint (ps > 0.36). The rate of any PA engagement did not change significantly over time (p = 0.12) and did not differ by gender (p = 0.19).
WHO PA guidelines
At baseline, 41% (n = 166) of veterans met the WHO recommendation of ⩾ 150 minutes of moderate/vigorous PA per week. A greater proportion of female veterans did not meet this criterion compared to male veterans at baseline (p = 0.05); approximately two-thirds of females (66%; n = 107) and half of males (55%; n = 137) did not engage in at least 150 minutes of PA per week. At 12 months, 31% met this criterion (n = 125). Two-thirds (66%; n = 164) of males and 75% (n = 121) of females did not meet this criterion at 12 months, and differences were not statistically significant (p = 0.09). Overall, meeting PA recommendations dropped 25% over time (p = 0.001) and did not differ by gender (p = 0.18).
Amount of PA
Median daily PA engagement was about 17 minutes for males and 11 minutes for females at baseline, and about 9 minutes for both males and females at 12 months. Daily PA did not differ by gender at either timepoint (ps > 0.08). Overall, median daily PA decreased 50% from baseline to 12 months (p < 0.001), and despite decreases being around 50% in men and 20% in women, gender differences were not statistically significant (p = 0.40).
Engaging in any PA, engaging in ⩾150 minutes of PA, and daily PA at baseline and 12 months, as well as changes in any PA variables over time, did not differ by time since military discharge (ps > 0.45).
Aim 2: Relationship between PA and PTSS
In Table 3, we present results from interaction models predicting 12-month PTSS and changes in PTSS from baseline to 12 months by any baseline PA engagement (yes/no), gender, and time since military discharge. There was a significant three-way interaction between baseline PA engagement, gender, and time since military discharge in predicting PTSS at 12 months (p = 0.01) and, marginally, in predicting changes in PTSS (p = 0.06). For men who had been discharged from the military for the longest duration, any PA at baseline predicted less PTSS at 12 months (p = 0.004), and a reduction in PTSS over study time (p = 0.04). These effects on PTSS at study end were marginally significant for men who had been discharged for a moderate amount of time (50th percentile; p = 0.055), and nonsignificant for men who had most recently been discharged (p = 0.59); effects on changes in PTSS were non-significant for men discharged a moderate and recent amount of time (ps = 0.44 and 0.85, respectively). A different interaction pattern was observed for women. For women who had either most recently been discharged from the military or had been discharged for only a moderate duration (50th percentile), any PA engagement at baseline predicted less PTSS at 12-month follow-up (ps = 0.002, 0.01, respectively), but did not predict significant changes in PTSS over study time (ps > 0.27). This effect at study end became weaker and nonsignificant for the group of women who were furthest from military discharge (p = 0.71). Results for ⩾150 minutes/week PA engagement were similar in predicting 12-month PTSS, but were non-significant in predicting changes in PTSS over time (ps > 0.08).
Three-way interaction models of PTSS by any physical activity, gender, and time since military discharge (N = 410).
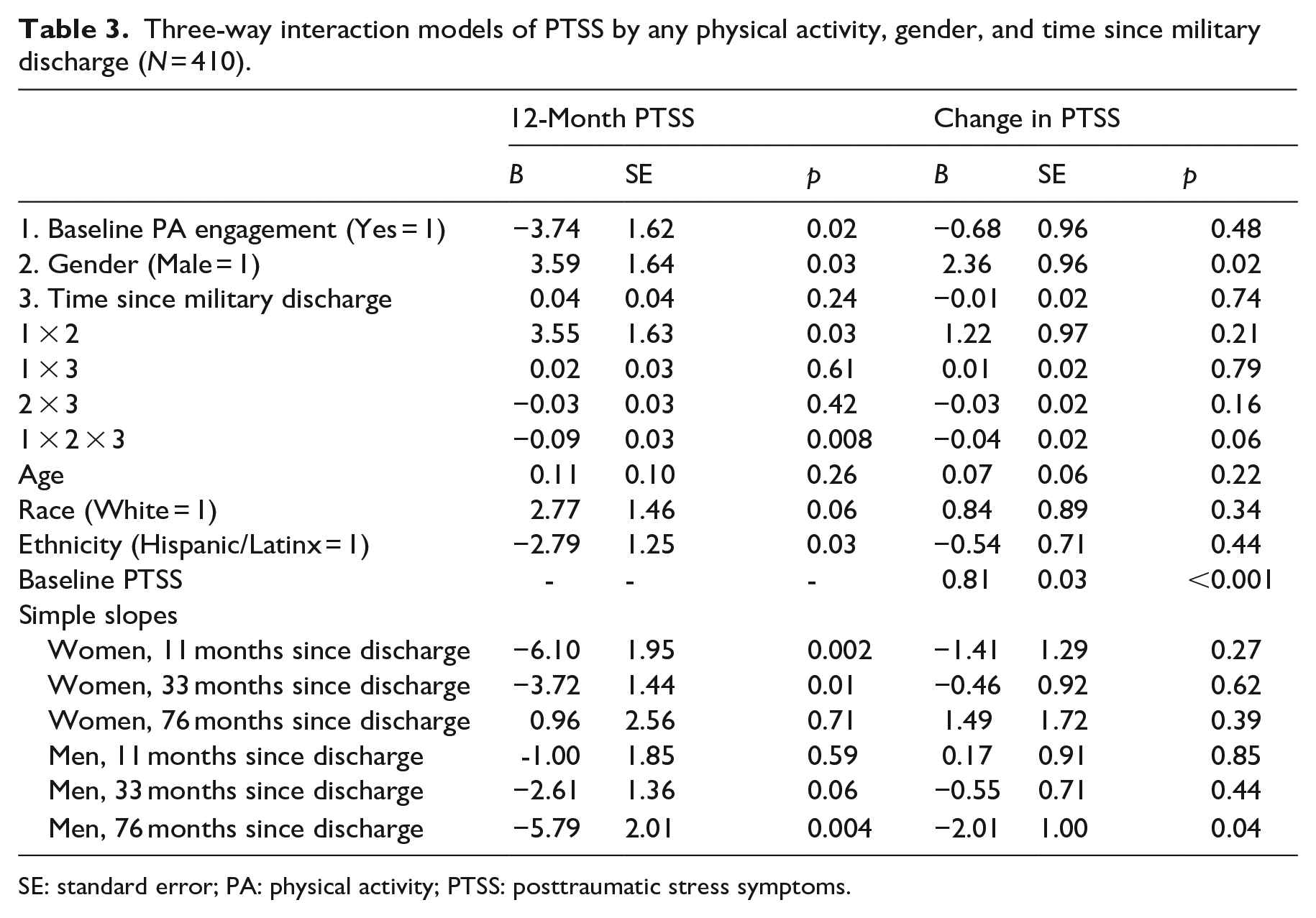
SE: standard error; PA: physical activity; PTSS: posttraumatic stress symptoms.
In Table 4, we present results from interaction models predicting 12-month PTSS and changes in PTSS from baseline to 12 months by baseline PA amount, gender, and time since military discharge. The three-way interaction between baseline PA amount, gender, and time since military in predicting PTSS at 12 months was not significant (p = 0.24), however, there was a conditional two-way interaction between baseline PA amount and gender for recent military discharge (B = 7.58, SE = 4.05, p = 0.045). Specifically, greater PA at baseline predicted lower PTSS at 12 months for women (B = −16.29, SE = 5.30, p = 0.002), while it did not for men (p = 0.83). No interactions were significant for changes in PTSS (ps > 0.22).
Three-way interaction models of PTSS by amount of physical activity, gender, and time since military discharge (N = 410).
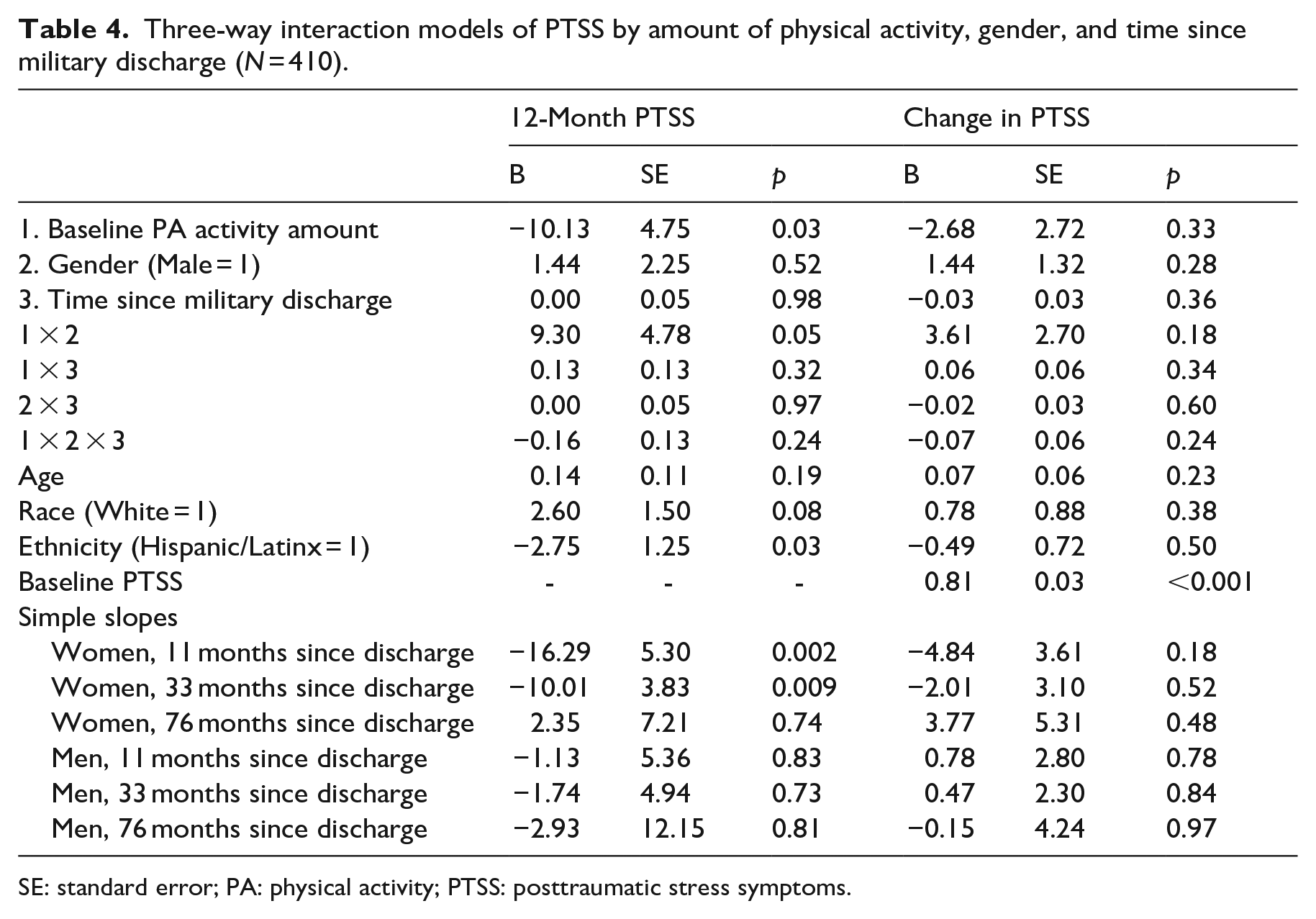
SE: standard error; PA: physical activity; PTSS: posttraumatic stress symptoms.
Discussion
The present study aimed to (1) characterize how post-9/11 veterans’ leisure-time PA changes over time, and (2) explore how PA relates to PTSS. Importantly, we assessed male and female veterans to address current gaps in our understanding of potential gender differences in these relationships. Given that the amount of time since separating from the military likely influences these relationships, we also examined time since separation with respect to our research questions, a frequently overlooked aspect of post-deployment veteran outcomes. Overall, findings reveal that post-9/11 veterans evidence low levels of PA and that PA engagement tends to decline over time. Further, and consistent with prior studies in civilian samples (e.g. Whitworth et al., 2017a), leisure-time PA was associated with lower PTSS, although this depended on both gender and time since military discharge.
Consistent with previous studies (e.g. Brown et al., 2019; Littman et al., 2009), overall veteran PA engagement was generally poor, with a large portion (i.e. 33% of male veterans and 38% of female veterans) not engaging in any weekly PA at study baseline and further declining over time. These rates of leisure-time physical inactivity are similar if not slightly higher than those recently estimated in the general U.S. population (e.g. between 18% and 33%; An et al., 2016). Despite the physical fitness requirements of military service members, many veterans showed low levels of PA cross-sectionally at baseline and demonstrated decreases in PA engagement over a one-year period. Inadequate levels of PA engagement in veterans are likely due to multiple factors, including a reduction in structure in civilian life compared to active military members who have fitness tests as an occupational requirement (Meadows et al., 2018). Further, physical or mental health comorbidities may act as barriers toward PA engagement (Walker et al., 2021). Given the importance of health behaviors such as PA for both physical and mental health outcomes, these findings warrant consideration of enhanced veteran health interventions.
Additionally, and consistent with gender differences in leisure-time PA shown in civilian populations (e.g. Azevedo et al., 2007), findings of the current study reveal that female veterans were less likely to meet PA recommendations after separation from service than their male counterparts. This lower rate of PA engagement may be due to evidence showing that women with more PTSS experience particularly rapid declines in PA relative to women without PTSS or without trauma exposure in a non-veteran sample (Winning et al., 2017). This gender difference in PA may also be due in part to differing motives for engaging in exercise based on gender. For instance, among civilians, men have been shown to report higher challenge, competition, social recognition, and strength/endurance exercise motives while women show higher weight management exercise motives (Kilpatrick et al., 2005). The present findings suggest that in addition to low levels of PA engagement across post-9/11 veterans, female veterans may be particularly vulnerable to low activity levels. Thus, there is a critical need to engage all veterans in PA maintenance interventions upon separation from the military as well as a more specific need to target female veterans’ PA engagement by understanding gender-specific motivators and barriers to help bridge the gap.
Given the importance of PA for maintaining physical as well as mental wellbeing, our second aim was to examine the relationship between leisure-time PA and PTSS over time. Consistent with previous cross-sectional (e.g. Zen et al., 2012) and longitudinal (e.g. Whitworth et al., 2017a) studies, findings of the present study indicate that, in general, engaging in any PA (compared to no PA) is associated with lower PTSS both cross-sectionally and longitudinally. However, our findings also reveal a more nuanced understanding of this complex relationship, depending on veterans’ gender and their time since discharge from the military. For instance, for men who were further from military discharge, engaging in any PA at baseline predicted less PTSS 1 year later and a reduction in symptoms over the course of a year. Importantly, however, the amount of PA engagement in male veterans did not predict PTSS 1 year later, nor a reduction in symptoms. Thus, the amount of PA in male veterans does not seem to matter as much as just being generally active (in contrast to not engaging in any PA). This finding suggests that helping male veterans who are further from military discharge initiate any leisure-time PA, no matter how brief, may yield some therapeutic mental health benefits in addition to well-established physical benefits.
For female veterans, any leisure-time PA engagement at baseline predicted less PTSS at study end for those who were recently discharged from the military, but not for those who had been separated from the military for a longer duration. In contrast with male veterans, PA may be especially useful for women who are earlier in the process of separating from the military. Continued exercise after separation from service may serve as a type of continued structure in female veterans’ lives, and routine and structure in the face of stressors are important for maintaining mental wellbeing overall (Hou et al., 2020). Further, the amount of PA did matter for female veterans. That is, higher PA frequency at baseline was associated with lower PTSS at 12-month follow-up; this relationship was true for women regardless of time since discharge. These findings add nuance to existing literature that suggests that men who engage in PA experience fewer PTSS than do women who engage in PA by adding context to how and when PA may be helpful for women with PTSD (Whitworth et al., 2017b).
Additionally, in contrast to men in this sample, engaging in baseline PA did not significantly predict changes in PTSS over study time for women, which may be due in part to women reporting generally lower PTSS across study time. Male veterans in this sample had more severe PTSS at baseline and thus had greater opportunity for improvement within a 1-year period, while women may not have evidenced enough variance in PTSS to see a reduction within this relatively brief window of time. Engagement in PA at baseline may have had a more latent effect on later PTSS for women. It is also possible that for women veterans, the beneficial effects of PA on PTSS are most relevant when closer to potentially traumatic experiences (i.e. active duty); there may be a mechanism of PA for aiding in initial trauma processing that provides long-term benefit. This mechanism may be particularly relevant for women given that they tend to have higher levels of physiological symptoms of PTSD (Hourani et al., 2015), and therefore the proposed mechanism of exercise aiding in reduction of PTSS by way of habituation to physiological sensations (Sothmann et al., 1996) may be more relevant for women than for men. Given evidence that has shown that hyperarousal symptoms are the symptom cluster shown to have the strongest association with reductions in PA after trauma (Vancampfort et al., 2016), PA could be a means of exposure for tolerating these heightened physiological sensations. However, as this study is among the first to explore gender differences in the relation between PA and PTSS over time and consider the effect of time since discharge, additional research is needed to explore potential explanations underlying these findings.
The findings of the present study have important clinical implications. U.S. military veterans frequently struggle with both their physical and mental health (Thomas et al., 2017). As both physical inactivity and occurrence of PTSD are known risk factors for health problems such as cardiovascular disease (e.g. Beristianos et al., 2016; Pedersen, 2017), PA may have both direct (e.g. improved blood pressure, cholesterol, immune response; Miles, 2007) and indirect (e.g. through reduction in PTSS) effects on health outcomes. Generally, the overall low level of PA in post-9/11 veterans and their decrease in PA over time suggests the importance of a greater focus on gender-specific interventions that foster healthy exercise habits among this population. For example, it appears to be especially important for interventions to target PA engagement for female veterans earlier on as they separate from the military, given that PA engagement within this time window appears to be associated with the most therapeutic benefit. Additionally, there seems to be a dose-response effect for women veterans recently discharged, such that more PA is associated with less PTSS. Thus, interventions should capitalize on this window of time as women veterans are recently separating from the military and beginning to readjust to civilian life and health behavior habits. For male veterans, on the other hand, a focus on PA may be less important upon initial discharge from the military compared to other potentially therapeutic factors. Interventions focusing on cognitive changes or exposure (Steenkamp et al., 2015) may be more useful initially for addressing male veterans’ PTSS, and then later shifting the focus toward engaging in PA for enhanced health benefits. Structural supports within VA systems may be needed to engage male veterans in such interventions as they get further from military discharge. Overall, more tailored approaches taking into consideration factors such as veterans’ gender and time since discharge are likely needed to provide the most benefit for veterans.
Limitations of the present study include use of self-report surveys for leisure-time PA and PTSS, which are subject to reporting and recall bias. Future studies should consider the use of objective measures, such as accelerometers, to assess PA or corroborate self-reported exercise engagement. Additionally, the threshold for meeting the WHO PA recommendations of ⩾150 minutes/week was based on veterans’ self-reported leisure-time PA only. The present study also examined a 1-year snapshot of veterans at various stages in their transition from active duty to civilian life; subsequently, results may have been stronger or weaker if we followed a cohort that were all uniformly approached close to military discharge. Additionally, although the present study focused on the important impact of PA on PTSS, the relation between PA and PTSS is likely bidirectional, with studies in civilian samples demonstrating PTSD onset to also have a detrimental impact on health behaviors including PA (e.g. Winning et al., 2017). Future research is needed to better understand these complex relationships, and it is essential that exercise interventions aimed at reducing PTSS also consider the PTSS-related barriers to initiating or maintaining PA habits. Finally, conditions such as chronic pain or physical disabilities may act as barriers to engaging in exercise post-deployment; considering feasibility and adapting exercises if necessary is essential to ensure continued engagement, especially since PTSD and chronic pain tend to be comorbid (Beck and Clapp, 2011). Despite these limitations, the present study possesses many strengths (e.g. longitudinal design, oversampling of female veterans who have generally been under-represented in veteran PA research) and fills important gaps in our current understanding of veterans’ leisure-time PA engagement over time as well as how PA relates to PTSS.
Conclusions
The present study demonstrated that post-9/11 veterans evidence generally low levels of leisure-time PA as well as decreases in their PA engagement over time. Leisure-time PA is also associated with lower PTSS, though this relation depends on both gender and veterans’ time since military discharge. Overall, the present findings provide important insights regarding when and for whom PA is associated with optimal reduction of PTSS among post-9/11 veterans. Given the importance of PA for maintaining physical and mental health, these findings suggest the need for PA as a low-cost intervention and, based on uncovered gender differences in patterns of PA and PTSS, this population may be best served with gender-specific PA interventions. Future research is needed to better understand the potential benefit of time- and gender-specific PA interventions for optimal wellbeing in post-9/11 veterans.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241233380 – Supplemental material for Physical activity, posttraumatic stress, and gender: A longitudinal study of post-9/11 veterans
Supplemental material, sj-docx-1-hpq-10.1177_13591053241233380 for Physical activity, posttraumatic stress, and gender: A longitudinal study of post-9/11 veterans by Katherine E Gnall, Shane J Sacco, Sinead M Sinnott, Crystal L Park, Carolyn M Mazure and Rani A Hoff in Journal of Health Psychology
Footnotes
Data sharing statement
Although the data used in this study are not publicly available because they are owned by the Veteran’s Health Administration (VHA), data may be made available upon request to the last author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Veteran’s Affairs CSR&D Grant ZDA1 and the National Institutes of Health F31AT012315 to KEG.
Ethics approval
This study was approved by the Institutional Review Board of the Department of Veterans Affairs.
Informed consent
Participants provided written informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.