
Abstract
This article reports qualitative outcomes from a randomized controlled trial comparing eight weeks of cognitive-behavioral group therapy for chronic pain (CBT-CP) and mindfulness-based group therapy (MBT) in individuals with chronic low back pain (CLBP). Approximately 10 months post-treatment, 108 participants completed structured qualitative interviews to express how the study treatment affected their life or health. Responses were qualitatively analyzed to generate a set of themes and subthemes, with between-groups comparisons to evaluate differences (if any) in treatment-response between MBT and CBT-CP. A majority of participants (n = 88, 81.5%) across both groups reflected positively on the study intervention and outcomes, identifying benefits in pain management (31.5%), meditation and mindfulness skills (25.9%), and relaxation skills (22.2%). Perceived benefits varied widely, suggesting no one intervention may be ideal for CLBP. Future research should examine tailoring interventions to target diverse clinical presentations to achieve optimal outcomes.
Keywords
Despite the limited effectiveness demonstrated for long-term opioid therapy (Jones et al., 2018), long-term prescription opioid use remains a pervasive issue (Shah et al., 2017) that often results in opioid misuse or use disorder (Vowles et al., 2015). A recent systematic review (De Sola et al., 2020) indicated that 5.8% of patients with chronic low back pain (CLBP) received long-term opioid therapy (LTOT), despite a dearth in robust data demonstrating LTOT’s efficacy or even safety (Bialas et al., 2020).
One reason for LTOT’s limited efficacy may be the vast heterogeneity in the experiences and treatment needs of individuals living with chronic pain. A recent study (De Sola et al., 2020) found that individuals may seek alternatives to opioids or reduce their dosage, even without guidance from their prescriber. Moreover, the researchers found that the emotional impact of chronic pain was “one of the most strongly affected areas, one that opioids could not improve and could even affect negatively” (De Sola et al., 2020).
Behavioral interventions, such as cognitive behavioral therapy (Gilliam et al., 2021) and mindfulness and supportive group therapy, have been posited as treatments for pain-related factors in CLBP (Garland et al., 2019, 2022). A systematic review and meta-analysis (Nury et al., 2022) of interventions for CLBP indicated that non-pharmacological interventions may be as effective as prescription opioids for improving pain-related disability and functioning. While previous research has identified potential mediators and primary targets of non-pharmacological approaches to pain-relief (Crowe et al., 2010; Jensen, 2011; Sturgeon, 2014), the majority of this research lacks insights into the perceived impact, if any, participants report experiencing from such treatments. A recent qualitative analysis (Crowe et al., 2010) revealed several psychosocial challenges associated with chronic pain, including the unpredictability of pain, the perceived loss of control with reactions to pain, and maladaptive self-referential thinking. A subsequent meta-synthesis (Snelgrove and Liossi, 2013) of qualitative CLBP research extended these findings to include avoidance behaviors, social functioning, and exercise, in addition to self-efficacy, as psychosocial factors implicated in CLBP. While CLBP literature has identified relaxation- and mindfulness-based behavioral interventions as potential non-pharmacological interventions for CLBP (Dunford and DClinPsy, 2010; Snelgrove and Liossi, 2013) conclusions of effectiveness have been limited by small sample sizes or insufficient periods of follow-up.
Qualitative research may begin to fill this gap by examining the impacts of non-pharmacological interventions on individuals’ daily lives. Such data are scarce yet needed to help elucidate the therapeutic processes and mechanisms of action for CLBP interventions. While previous qualitative research has independently investigated cognitive-behavioraltherapy (CBT) (Tsubaki et al., 2023) and mindfulness (Luiggi-Hernandez et al., 2018) CLBP interventions, limited research has qualitatively compared outcomes from cognitive- and mindfulness-based interventions for CLBP. One previous publication (Cattanach et al., 2021) illustrated participant-reported outcomes associated with mindfulness-based cognitive therapy, mindfulness meditation, and CBT for CLBP. Fifty-seven participants completed qualitative interviews two weeks post-treatment (Cattanach et al., 2021), their feedback suggesting that each intervention provided predominantly distinct benefits, with minimal overlap in reported mechanisms.
Building upon previous research, the present study examined longitudinal qualitative outcomes from individuals with CLBP approximately 10 months after completing mindfulness- and cognitive-based group interventions for CLBP. This qualitative analysis was performed as part of a larger randomized controlled trial (Zgierska et al., 2021) to examine the qualitative responses from participants to the question “How did being in this study impact your life or health?”
Methods
The parent study, titled “Strategies To Assist with Management of Pain” (STAMP; NCT03115359), was a large, multi-site randomized controlled trial (RCT) comparing two 8-week group therapy interventions for individuals treated for Chronic Low Back Pain (CLBP) with opioid medications (≥15 mg/day morphine equivalent at time of initial screening) (Zgierska et al., 2021). Participants were adults (≥21 years old) with persistent (≥3 months) low back pain of at least 3 on the Brief Pain Inventory (BPI) 0–10 pain scale (Von Korff et al., 2000), and a score of at least 21 on the Oswestry Disability Index (ODI) 0–50 scale (Fairbank and Pynsent, 2000). Participants were randomized to receive one of two group psychotherapeutic modalities for chronic pain, Cognitive Behavioral Therapy (CBT-CP) or Mindfulness-Based Therapy (MBT). MBT offers skills for acceptance-based pain coping and encourages non-judgmental awareness of present-moment experiences (Banth and Ardebil, 2015; Kabat-Zinn et al., 1985), whereas CBT-CP focuses on shifts in experiences of pain, pain distraction, and adopting healthy coping skills to better live with pain (Otis, 2007). All study procedures were reviewed and approved by the Institutional Review Boards of the participating universities.
As part of a qualitative arm of STAMP, all study participants completed a brief, fully structured interview at study baseline and at study termination. Interviews were video recorded and analyzed using Transana™ software (Woods, n.d.). The video was considered the primary data for this analysis, with the transcript serving as a useful but secondary representation of the data (Dempster and Woods, 2011; Woods and Dempster, 2011). The present qualitative analysis focused on participant responses to the exit interview question “How did being in this study impact your life or health?”
Participant responses were divided into thematic utterances, defined as segments of text focusing on a single theme. All interview data were independently analyzed and coded by the first two authors, who met following each stage of the analysis to review identified themes and subthemes, address any discrepancies, and achieve congruence. This process was repeated until theoretical saturation was achieved (i.e., further analysis of participant responses would reveal no further insights). Once the independent coders reached full agreement, data was divided by study intervention to evaluate between-group differences in the themes reported in CBT-CP and MBT. Between-group comparisons were thematically analyzed to explore potential similarities and differences in longitudinal treatment outcomes between the two interventions. Data for the present study may be shared upon request, following completion of a data sharing use agreement.
Results
Sample description
See Table 1 for baseline demographic information for the sample. Participants reported a mean age of 59.4 years (SD = 9.6), and 63.0% were female. Participants were predominately white (80.6%) and non-Hispanic (84.3%). At the time of their intake appointment, participants reported an average morphine-equivalent opioid dosage of 103 mg/day (SD = 145), range = 2.0–1020 mg/day), an average reported pain level for the previous week of 5.5 (SD = 1.5) on the BPI 0–10 point pain scale, and an average worst pain in the past week of 8.0 (SD = 1.4). Participants reported an average ODI score of 46.6 (SD = 13.2). They scored 28.4 (SD = 8.1) on average for the 12-item Short Form Survey (SF-12) Physical Scale and 42.5 (SD = 12.0) on the SF-12 Mental scale (Kosinski et al., 2007). Overall, 85.2% of our participants reported problems with CLBP for over 5 years, and 95.4% reported that pain was a problem every day or nearly every day over the past 6 months.
Baseline Characteristics of Adults With CLBP Treated with Opioids (n = 108).
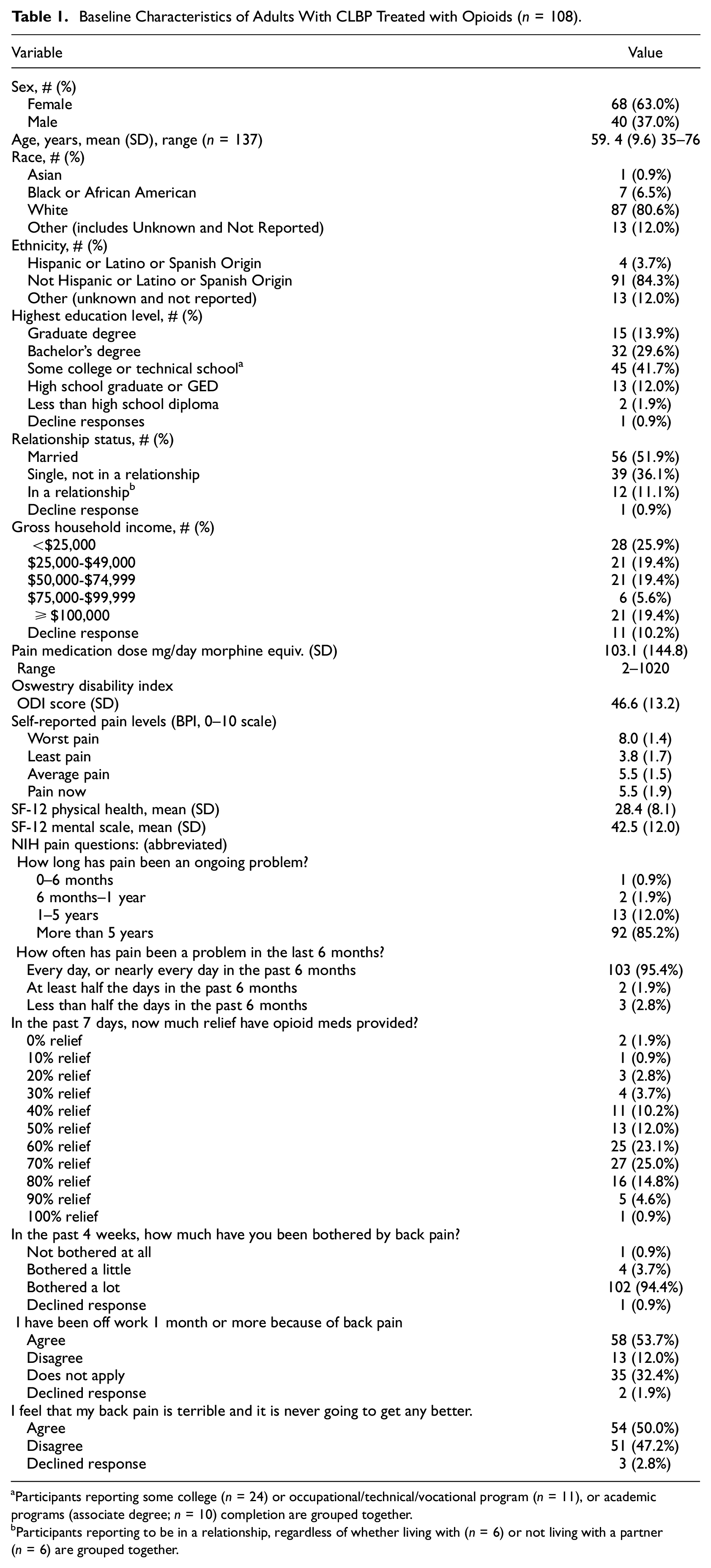
Participants reporting some college (n = 24) or occupational/technical/vocational program (n = 11), or academic programs (associate degree; n = 10) completion are grouped together.
Participants reporting to be in a relationship, regardless of whether living with (n = 6) or not living with a partner (n = 6) are grouped together.
STAMP study interventions occurred in three locations, with 33 participants (30.6%) in this analysis participating in Massachusetts, 33 participants (30.6%) in Utah, and 42 participants (38.9%) in Wisconsin. There were 54 participants (50.0%) in the CBT-CP group and 54 participants (50.0%) in the MBT group across the three locations.
Qualitative themes
Data reported in the present analysis came from the first 108 STAMP study participants who completed both the baseline and exit interviews. A sample size of 108 was determined to be large enough to allow for sufficient representation of both intervention groups across all three locations, and was considered adequate to achieve theoretical saturation during the qualitative portion of this analysis.
Qualitative Thematic Analysis (Elo and Kyngäs, 2008) was independently performed by two study authors, who together identified 280 unique utterances from these 108 participants. Four major themes emerged from this analysis: positive reflections, mixed reflections, no positive reflections, and treatment dislikes. Positive reflections encompassed any utterances that indicated clear positive associations with aspects of the intervention or outcomes a participant associated with the intervention. Mixed reflections captured all utterances indicative of mild or temporary benefits associated with the intervention, or those with mixed positive and negative elements in a single response. “No positive reflections” comprised participants that reported no positive impacts to their life or health, including any reported negative impacts from study participation. The final theme, “treatment dislikes,” covered aspects of the intervention that were perceived as unhelpful or suboptimal. Notably, a participant could report disliking a particular aspect of the treatment intervention, yet still feel that the overall intervention was beneficial.
See Table 2 for a breakdown of the themes and sub-themes found. An overwhelming majority of utterances (n = 218, 77.9%) by 88 participants (81.5%) were categorized in the “positive reflections” theme. A total of 35 utterances (12.5%) by 24 participants (22.2%) were categorized under “mixed reflections” theme, and 14 utterances (5.0%) by 13 unique participants (12.0%) were thematically categorized as “no positive reflections.” Finally, there were 13 utterances (4.6%) from 8 individuals (7.4%) that noted a specific feature of the intervention that the participant did not like or thought could be improved. Note that utterances are mutually exclusive, so the total number of utterances adds up to 280 across all categories in Table 2.
Frequency of Utterances and Participants Reflecting on Study Impact. a
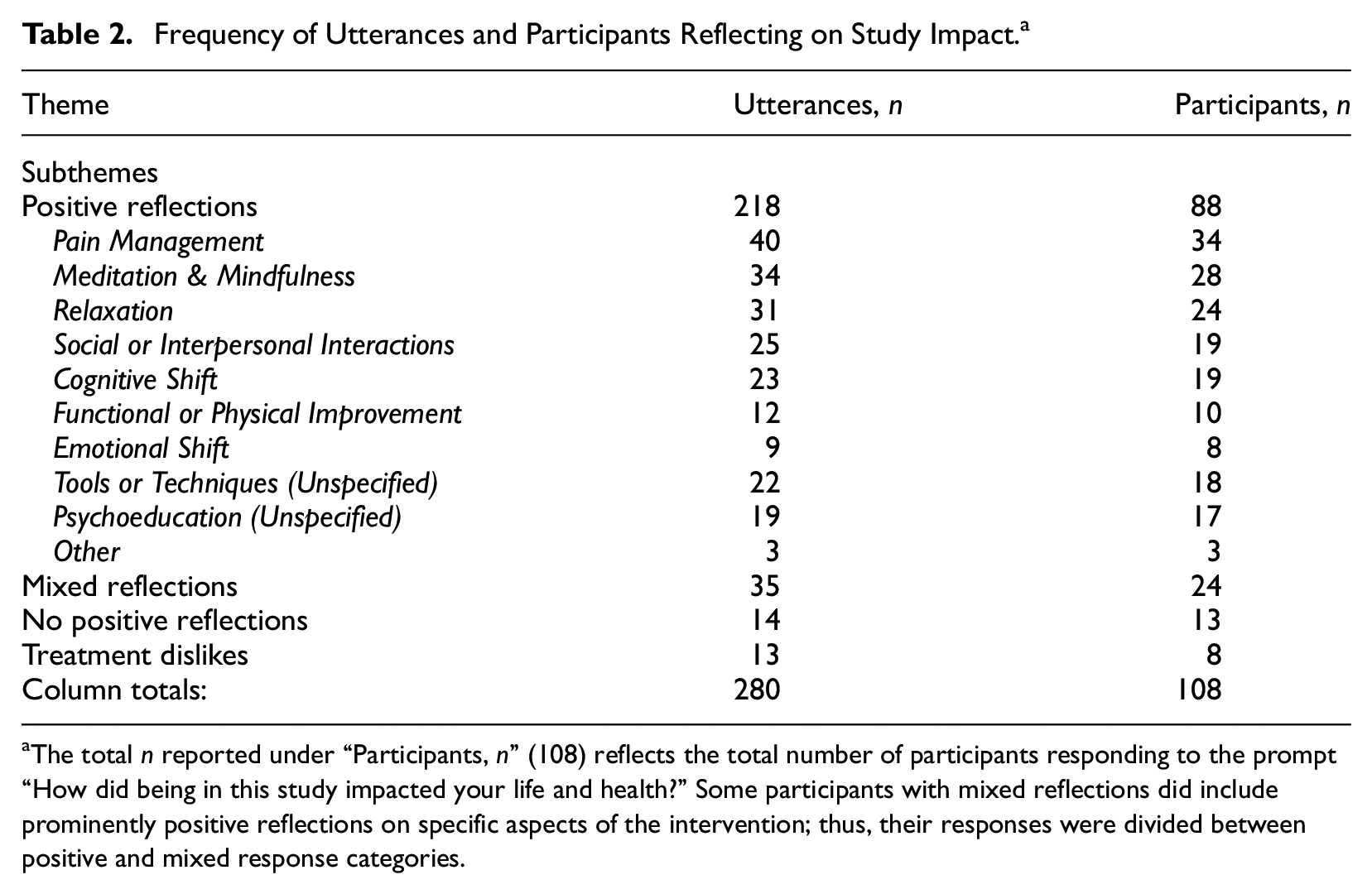
The total n reported under “Participants, n” (108) reflects the total number of participants responding to the prompt “How did being in this study impacted your life and health?” Some participants with mixed reflections did include prominently positive reflections on specific aspects of the intervention; thus, their responses were divided between positive and mixed response categories.
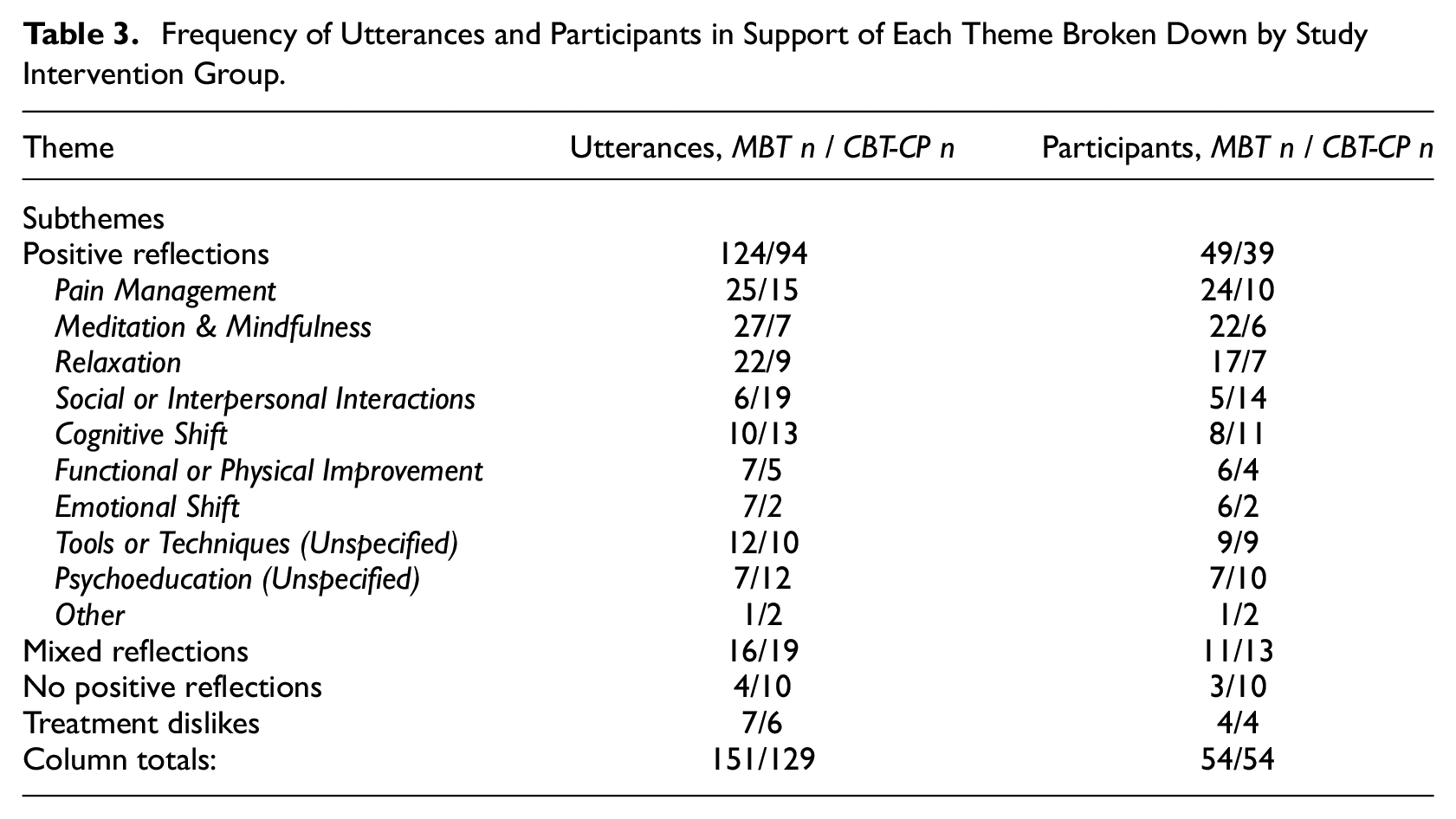
Table 3 shows qualitative themes broken down by study intervention group to investigate potential differences between interventions. When dividing between study intervention groups, 82% of the utterances made by 91% of MBT participants offered positive reflections on study participation, compared to 73% utterances from 72% of participants receiving CBT-CP. Mixed reflections were roughly even between groups. Only 5.6% of participants randomized to MBT provided no positive reflections in 2.6% of utterances, compared to 18.5% of the CBT-CP group, with 7.6% utterances.
Frequency of Utterances and Participants in Support of Each Theme Broken Down by Study Intervention Group.
Exemplary quotes under each theme/subtheme are presented for each intervention group in Table 4.
Exemplary Quotes Under Each Theme, Organized by the Intervention Each Participant Received.
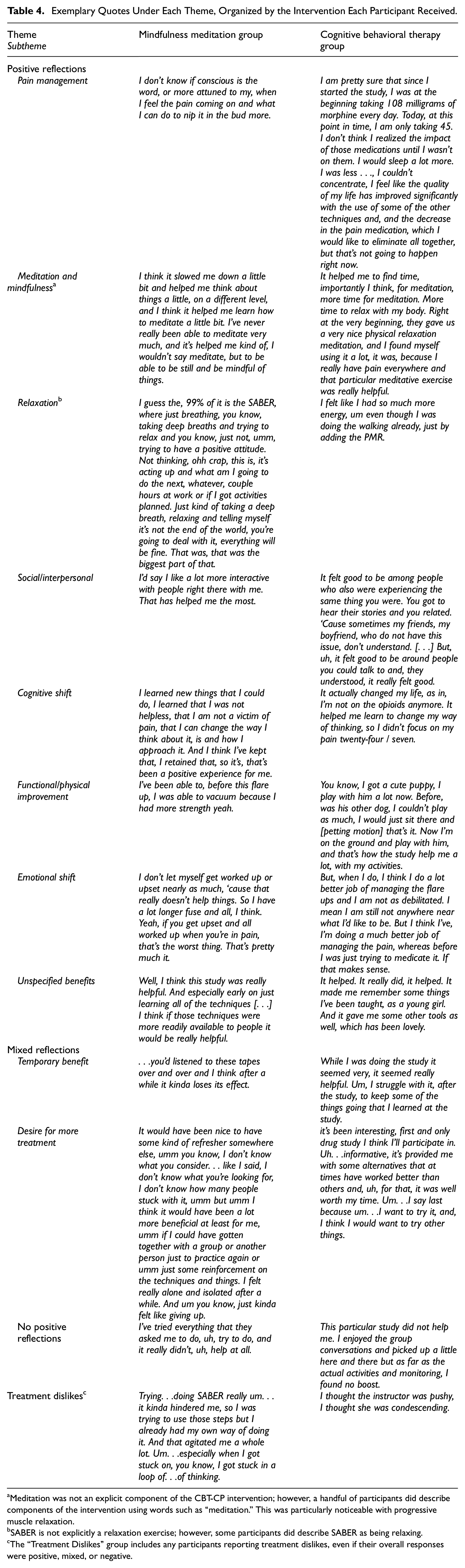
Meditation was not an explicit component of the CBT-CP intervention; however, a handful of participants did describe components of the intervention using words such as “meditation.” This was particularly noticeable with progressive muscle relaxation.
SABER is not explicitly a relaxation exercise; however, some participants did describe SABER as being relaxing.
The “Treatment Dislikes” group includes any participants reporting treatment dislikes, even if their overall responses were positive, mixed, or negative.
Positive reflections
A majority of utterances (n = 218, 77.9%) from 88 participants (81.4%) were categorized in the “positive reflections” theme, meaning the utterance reflected on a positive aspect of the study or its effect on the life or health of the participant. Positive reflections were divided into several subthemes, in which participants identified aspects of the study interventions they found helpful, or specific ways in which the study impacted their life or health. These subthemes included pain management, meditation and mindfulness, relaxation, social or interpersonal interactions, cognitive shift, functional or physical improvement, emotional shift, unspecified tools and techniques, and unspecified psychoeducation. Three utterances (1.1%) from three participants (2.8%) were too ambiguous to categorize and were included in an “Other” category.
Pain management
The most common positive reflection, this subtheme included utterances specifically referring to how the study interventions impacted the participant’s ability to manage their pain. Thirty-four participants (31.5%) indicated experiencing positive impacts on pain management, with a total of 40 utterances (14.3%). Pain management utterances were somewhat more common in the MBT group (25 utterances, 24 participants) than the CBT-CP group (15 utterances, 10 participants). Ten utterances (3.6%) by 10 participants (9.3%) indicated that the intervention they received increased their ability to cope with their pain (as opposed to reducing their pain). Conversely, 12 participants (11.1%) in 15 utterances (5.4%) attributed reduced reliance on opioids to their participation in the study.
Meditation and mindfulness
Another common subtheme was meditation and mindfulness, mentioned both together and separately. Approximately one in four participants (n = 28, 25.9%) referred to either meditation or mindfulness, with a total of 34 utterances (12.1%). A breakdown of this category demonstrated that a total of 18 utterances (6.4%) by 17 participants (15.7%) specifically mentioned meditation, while 16 utterances (5.7%) from 12 participants (11.1%) specifically reflected on mindfulness. Positive reflections concerning meditation and mindfulness were predictably much more common from members of the MBT intervention group, with 27 utterances from 22 participants in this theme compared to seven utterances from six CBT-CP group members.
Participants in the CBT-CP group did not receive any form of meditation intervention; however, some participants tended to pair the concept of meditation with relaxation techniques in CBT-CP, such as progressive muscle relaxation (PMR). While meditation is not formally incorporated into PMR, participants nonetheless described these experiences as “meditative.” Similarly, one participant in the CBT-CP group reported using meditation techniques to control pain, despite not being included in the study intervention.
Relaxation
Twenty-four participants (22.2%) mentioned relaxation as a positive aspect of the study, citing intervention components such as PMR or breathing in 31 utterances (11.1%). This does not include references to breathing that were paired with meditation or mindfulness. The theme of relaxation came up more than twice as often from MBT members (22 utterances from 17 individuals) than CBT-CP members (9 utterances from 7 participants).
Social or interpersonal interactions
Nineteen participants (17.6%) in 25 utterances (8.9%) mentioned social or interpersonal interactions as helpful or important. These utterances were much more frequent from participants in the CBT-CP group (19 utterances, 14 participants), compared to MBT (6 utterances, 5 participants). Many of these reflections were specifically in reference to the interactions with group members, with statements indicating the importance of shared lived experience to these participants.
Cognitive shift
Nineteen participants (17.6%) made 23 utterances (8.2%) about shifts in their thinking, often indicating decreased helplessness and increased self-efficacy in managing their pain. Cognitive shifts were mentioned at similar rates in the two groups, with 13 utterances by 11 participants in the CBT-CP group, and 10 utterances among 8 participants in the MBT group.
Functional or physical improvement
Ten participants (9.3%) made 12 utterances (4.3%) reporting improvement in their functioning as a result of participating in the study. Of these participants, 4 specified improvements in sleep quality (3 utterances), while 4 others discussed how they feel less physically debilitated (4 utterances). One participant also expressed benefit in occupational functioning, and a single participant reported generally improved concentration as a result of study participation. These utterances were distributed evenly between groups.
Emotional shift
Eight participants (7.4%) made nine utterances (3.2%) about an emotional shift they attributed to the study. Such shifts included reported decreases in stress and anger, replaced instead with acceptance. Emotional shifts were more commonly reported in the MBT group than the CBT-CP group.
Unspecified tools and techniques/psychoeducation
Thirty-four participants (31.5%) reflected positively on the study content and impact, but their utterances (n = 41; 14.6%) provided limited information to elaborate. Twenty-two utterances (7.9%) from 18 participants (16.7%) expressed appreciation for unspecified tools and/or techniques provided during the study. Similarly, 19 utterances (6.8%) from 17 participants (15.7%) indicated that these individuals appreciated psychoeducation provided during the study. While these participants did not elaborate on the psychoeducation they were referring to, many did report gaining important knowledge or insights through study participation.
Mixed reflections
Twenty-four participants (22.2%) provided mixed reflections for how participation in the study impacted their lives or health. Thirty-five utterances (12.5%) fell under in this theme, approximately equivalent between groups. Mixed reflections were divided into two sub-themes:
Temporary benefit
Nine participants (8.3%), in nine utterances (3.2%), stated that they experienced temporary benefit from study participation. Interestingly, two participants reported that the study intervention was specifically helpful for coping with acute pain experienced following subsequent surgeries. Six of the nine participants in this theme were in the CBT-CP group.
Seven of these participants elaborated on reasons for only receiving temporary benefit from the study intervention. Three indicated forgetting or struggling to continue study material after the study, while another participant experienced decreased benefit from repeatedly listening to the same relaxation tapes. Additionally, three other participants struggled to maintain treatment benefit after experiencing a new injury following enrolling into the study.
Desire for more treatment
Seven participants (6.5%) explicitly expressed a desire for additional treatment (10 utterances). Four of these participants made five utterances indicating some desire to receive additional treatment beyond the study intervention, such as psychotherapy for depression or a combined CBT + MBT intervention. Conversely, four participants expressed a desire to receive more of the study intervention.
No positive reflections
Thirteen participants (12.0%), in 14 utterances (5.0%) suggested that they did not find participation in the STAMP study to have had a positive impact on their life or health. Ten of these came from the CBT-CP group and three from the MBT group. Four participants (all CBT-CP), when asked how being in the study impacted their life or health, replied with the same brief phrase, “it didn’t.”
Three participants (2.8%), in three utterances (1.1%), stated that they did not benefit because they did not participate in study activities. Only one participant explicitly indicated a desire to seek out an alternative treatment, due to experiencing no benefit in study participation. One participant attributed the lack of benefit from the study to an overall deterioration in health and functionality over the course of the study period. Notably, this was the only participant to report an overtly negative impact from study participation.
Treatment dislikes
Eight participants (7.4%) identified specific aspects of the study which they did not like in 13 (4.6%) utterances. No common subthemes emerged in treatment dislikes, as no more than two participants shared the same dislike. One participant described the intervention as a bit too “textbook-y,” and another participant indicated poor rapport with their study therapist. Yet another participant disliked a mindfulness exercise that others found helpful, SABER (Stop, Acknowledge, Breathe, Expand, Respond).
Importantly, participants reporting treatment dislikes represent <10% of the sample, and a number of these participants also included mixed or even positive reflections in their response. Thus, this section was distinguished from “no positive reflections,” as participants may have disliked an aspect of the study, yet still found other aspects helpful.
Discussion
To date, the present analysis represents the largest qualitative study of mind-body interventions for chronic pain. A total of 108 participants completed the qualitative portion of the STAMP study, reaching theoretical saturation. Overall, participant responses were predominantly positive. Results suggest that most participants in both groups felt that they benefited from the study intervention. Only 12.4% did not identify positive impacts from the study. Overall, differences between groups aligned with the differing content between the two interventions provided in the STAMP study.
The present analysis extends previous research by nearly doubling the sample size of previous research (Cattanach et al., 2021), explicitly comparing mindfulness- and cognitive-based CLBP, and conducting longitudinal qualitative interviews approximately 10-months posttreatment. Moreover, longitudinal qualitative data collection provided a critical opportunity to evaluate the potential long-term benefits of tools and techniques from each intervention that endured nearly 1 year following treatment completion. Findings both affirm and build upon previous research in several important ways. Most notably, the largest subtheme of positive reflections suggests that both interventions improved pain management following completion of the study, supporting past findings that non-pharmacological interventions may be effective in improving pain management outcomes in individuals prescribed opioids for chronic pain. On the other hand, the large number of positive reflections that were not categorized under pain management (n = 178; 81.7% of positive utterances) underscore the complex psychological sequelae people living with CLBP face that might be targeted in non-pharmacological interventions for chronic pain. Together, these results suggest a continued need to refine non-pharmacological interventions for CLBP, including cognitive behavioral and mindfulness-based therapies.
Between-group comparisons revealed that MBT participants were slightly more positive in their feedback, with 82.1% of their statements being positive, compared to 72.9% positive comments from CBT-CP participants. Participants who received MBT were also more likely to identify pain management skills, mindfulness, meditation, relaxation, and emotional shifts as outcomes following study intervention. Participants in the CBT-CP group were more likely to talk about the social and interpersonal benefits of the intervention. Notably, significant overlap in terminology emerged between the two groups; a number of CBT-CP participants mentioned mindfulness or meditation, while MBT participants discussed relaxation and breathing benefits at rates higher than the analysis team anticipated. Participants across both groups described shifts in thinking, with slightly more utterances for the CBT-CP group. These overlapping reflections between the two groups suggest some shared qualities or even mechanisms underlying the two interventions, even if not explicitly called out in the content of the interventions themselves.
Notably, four participants expressed a desire to continue receiving some form of study treatment, a sentiment reinforced by seven participants reporting “temporary benefit” from the study intervention. Participants attributed limitations in the duration of benefit to acquiring new injuries, struggling to continue practicing content learned in the study intervention, and/or requiring new treatment materials (i.e. relaxation tapes). These findings suggest that some individuals living with chronic pain might benefit from booster or maintenance sessions to reinforce previous treatment gains.
Limitations
The present study was limited in several important ways. Importantly, the sample with which this study was conducted was predominately white, female, and married. Given the risk of implicit bias and stigmatization in opioid prescribing (FitzGerald and Hurst, 2017; Keister et al., 2021) and mental health treatment-seeking (Misra et al., 2021; Schnyder et al., 2017), as well as social support in chronic pain outcomes (Evers et al., 2003), future studies should enhance the diversity of the sample to better generalize findings across demographics.
Another inherent limitation is the possibility of a biased sample in the present dataset. Participants who found the study intervention helpful might be more motivated to complete their exit interviews 10 months following the end of the intervention group meetings, while those participants who did not find the study intervention helpful might be more likely to drop out of the study.
Additionally, the study held limited inferential power due to the nature of qualitative methodology; therefore, the finding of more frequent positive statements about MBT than CBT-CP may not hold “statistical significance.” The present analysis was restricted to a single question posed in the interview; additional follow-up questions and elicitation of more information may have provided deeper understanding of the reasons why a small number of participants reported no impact from the study on their overall life and health.
Conclusion
The present analysis represents the largest qualitative study of mind-body interventions for opioid-treated chronic pain, to date, with a sample size that complimented the unique qualitative comparative analytic approach to evaluating between-group differences.
A number of potential long-term benefits from mindfulness- and cognitive-based approaches were reported, including improved pain management, mindfulness, relaxation, positive shifts in cognition and affect, and functional/physical improvement. Participants reported a range of treatment content that was particularly helpful, including mindfulness and meditation, relaxation exercises, and psychoeducation. Similarly, participants indicated that offering additional resources such as booster sessions or alternative relaxation tapes could reinforce treatment benefits and enhance the longevity of clinical benefit.
Implications for future research
Due to the complexity of clinical presentations and treatment needs in people living with CLBP, future research should examine ways in which interventions can be adapted to include booster maintenance sessions to reinforce behavior changes. A personalized medicine approach to intervening for chronic pain may be a useful strategy, as clinicians could tailor treatment content and length to meet an individual’s treatment needs, while minimizing infrastructural and individual burden. Future studies may also benefit from interviewing individuals with CLBP who are not treated with opioids as an additional comparison group. Critically, future research should prioritize recruitment of a more diverse sample to enhance generalizability of findings and inform clinical interventions for individuals from underrepresented and marginalized communities.
Footnotes
Data sharing statement
Data for the present study may be shared upon reasonable request, following completion of a data sharing use agreement with the University of Wisconsin Madison. The datasets generated during and/or analyzed during the current study are not publicly available due to institutional policy and the sensitive nature of the data collected.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: David Woods, the second author of this paper, is the author and publisher of Transana, the qualitative analytic software used to analyze all video from the STAMP study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The reported work was funded through a Patient-Centered Outcomes Research Institute (PCORI) Award (OPD-1601-33860). The views and statements in this publication are solely the responsibility of the authors and do not necessarily represent the views of the PCORI, its Board of Governors or Methodology Committee. This project also received funding and institutional support through University of Wisconsin-Madison School of Medicine and Public Health, and its Department of Family Medicine and Community Health; Brigham and Women’s Hospital, Harvard Medical School; University of Utah College of Social Work; and Pennsylvania State University Department of Family and Community Medicine.
Ethics approval
All study procedures were reviewed and approved by the Institutional Review Boards of the participating universities.