
Abstract
The concept of stress as a cause of ill health has received much attention in social sciences. The distinction between stress exposure and perceived stress emphasizes the importance of cognitive dimension of stress. This quantitative study (N = 213) conducted in Ukraine in November 2022 collected self-reported cognitive data on stress exposure, perceived stress, and self-rated heath. The goals of the study included (1) testing if stress exposure and perceived stress differ in terms of breadth and depth of their impact; (2) isolating psychosocial factors that reduce stress; and (3) testing if individuals who have relocated within Ukraine or abroad to escape the war had worse health outcomes than those who remained at their domiciles. The results suggest that while perceived stress was a stronger predictor of negative health outcomes, optimism and social support served as protective psychosocial factors. Having moved abroad predicted higher stress levels and more adverse health symptoms.
Introduction
Stress has been systematically linked to adverse health outcomes (Segerstrom and O’Connor, 2012; Thoits, 2010). Epidemiological research has empirically shown that stress affects health both directly (through dysregulation of several physiological systems) and indirectly (via unhealthy coping behaviors) (Segerstrom and O’Connor, 2012; Sterling, 2021). Stressful events vary in terms of their frequency; their ability to affect health depends on where in the individual life trajectory they occur (Cohen et al., 2019). Chronic stress is considered more detrimental for health than acute stress. The impact of chronic stressors on health has received much research attention but its mechanisms are still not fully understood (Goldstein and McEwen, 2002). While stress exposure does not uniformly translate into diseases, understanding the range of factors that make its consequences more insidious is important to develop a better understanding of how the psychosocial stress works to instigate pathology.
While there is little agreement on the definition of stress and stressors (Cole, 2010; Epel et al., 2018; McEwen, 2019), stress is usually understood as an internal experience of strain, distress, fear or negative emotions that occurs as a result of a perceived threat to one’s mental or physical well-being, and is accompanied by an evolved biological response that facilitates adaptive reaction (Hughes et al., 2018; Katsampouris et al., 2022). A stressor is typically understood as a set of external circumstances that threaten the well-being of individuals, strain their resources and require adjustment in order to cope with the stressful situation.
Our understanding of stress physiology has expanded appreciably over the course of the past 50 years providing us with a more nuanced theoretical picture of the mechanism by which stress affects human condition (Hughes et al., 2018). Currently there are several theoretical models explaining stress-health links (allostasis, polyvagal theory, neurovisceral integration, calibrated adaptation, social safety theory etc.). While the existing models differ in the details of their causal arguments, they converge on the destructive impact of childhood stress on health in later life (Bosch et al., 2012; Felitti, 2009; Slavich, 2016). On the other hand, social and psychological factors that buffer the onset of biological risks have been established (Cohen et al., 2019; Epel et al., 2018; Fitzgerald et al., 2021; McEwen, 2019; McEwen and Stellar, 1993). For example, higher resilience to stress and adversity has been documented for older and more educated individuals (Brinkhof et al., 2023). Interventions to slow down or even reverse the process of immunosenescence caused by poverty are being developed; most of them focus on lifestyle change (e.g. diet, exercise) (Asif et al., 2020; Fitzgerald et al., 2021; Gomez-Pinilla et al., 2011), cognitive style (via meditation, West et al., 2022), and family-centered interventions (Brody et al., 2016; Hoye et al., 2020). As a result, stress research became more complex conceptually and came to face more measurement-related challenges.
More recently, the distinction between stress exposure (i.e. facing an objectively measurable stressor) and perceived stress severity (i.e. a subjective experience of stress resulting from individual’s facing a stressor) has been gaining traction in stress research, as the latter has been shown to demonstrate a superior predictive ability in terms of negative health outcomes compared to the former, highlighting the role of cognition in the stress process. Measurement-wise, perceived stress tends to yield more precise results which makes it preferable as a stress-assessment tool (Shields et al., 2023).
War and trauma
An armed conflict presents some of the most intense stressors that can be found in a society. War conditions are objectively life-threatening, affecting individuals through their emotional experiences (fear, distress, grief), pain, material losses, and privation. As war threatens lives of both civilians and military personnel, war stressors are among the most traumatic life events (Song et al., 2024). While for those individuals who find themselves in the conflict zone war stress is typically episodic (i.e. interspersed events with some time intervals between them), for the refugees—as well as for the combatants—war impact is more chronic in character due to the fact that being displaced changes individual’s routine, social status, their level of security and likelihood of sexual assault in the new place of residence or during transition (Miller and Rasmussen, 2017). Combatants have the highest likelihood of developing psychiatric symptoms induced by their war experiences (Lim et al., 2022); it is worth noting that not only reservists abut also volunteers of both genders with little military training went to the front in Ukraine.
Researchers concur that war stress exposure has vast destructive potential for health of all categories of population, especially refugees, first responders and emergency service workers, body handlers, as well as those who endured or witnessed acts of violence, the destruction of civil infrastructure, saw dead bodies or their parts, or helped bury them etc. (Karam and Ghosn, 2003). The consequences of war with respect to mental health include trauma, PTSD, acute stress response, depression, substance misuse, inaccessibility of mental health care, as well as higher likelihood of cardiovascular disease, immune disorders, and shorter life span (Helpman et al., 2015; Miller and Rasmussen, 2010). On the other hand, optimism, hope, and high self-esteem are considered to be protective factors against war stressors (Besser et al., 2015).
The results of epidemiological research on war stress emphasize high prevalence of depression and PTSD among those who have lived in the conflict zone but these findings are inconsistent (ranging from 0%–99% for PTSD and from 3%–85.5% for depression (Morina et al., 2018). War’s impact on children is also cited. Children exposed to violence are more likely to resort to aggressive behavior and show delays in developing prosocial behavior when growing up (Song et al., 2024). Scoglio and Salhi (2021) report that from 25%–93% refugee children witness acts of violence or murder.
Furthermore, the war-related stress studies tend to rely on war survivors or veterans, as conducting data collection during the active conflict is difficult. As the armed conflict in Ukraine is still ongoing, current data on mental health of Ukrainians are scarce and only preliminary conclusions can be made (Pavlova et al., 2022). The available data indicate worsening of the psycho-emotional state of Ukrainian civilians (97.8%), depression (84.3%), exhaustion (86.7%), loneliness (51.8%), nervousness (84.4%), and anger (76.9%) (Kurapov et al., 2023). The results further suggest that women suffer more from war-induced stress than men (Kurapov et al., 2023). Another study highlights high levels of stress exposure among the Ukrainian participants, where each respondent encountered on average nine stressors from the checklist; 25.9% of participants met the clinical criteria for PTSD and additional 14.6%—for complex PTSD (Karatzias et al., 2023).
Study aims and hypotheses
The study conducted via online survey in Ukraine in November 2022 collected self-reported cognitive data on stress, health, and war-related experiences of Ukrainians since the beginning of the full-scale invasion in February 2022 and was guided by three purposes. First, the study aims to explore the relationship between stress and health status, focusing specifically on the differential effects of stress exposure and perceived stress on self-rated health. Secondly, the survey collected data to map the relationships between the risk factors versus protective factors (social circumstances and psychological resources) that factored in the associations between stress exposure, perceived stress and health during the active phase of war in Ukraine. Thirdly, the study explored the links between social capital (e.g. perceived and actual social support, social network size etc.) and various facets of migration experiences. The goals of the study included (1) testing if stress exposure and perceived stress differ in terms of breadth and depth of their impact, that is, the number and severity of effects on health outcomes; (2) isolating psychosocial factors that reduce stress or function as buffers against stress directly or indirectly; and (3) testing if individuals who had to move to safer regions of Ukraine or abroad because of the armed conflict had worse health outcomes than those who remained at their domiciles. Stress exposure and perceived stress were previously found to differ in terms of breadth and depth of their impact (Shields et al., 2023). In the light of previous findings on the distinction of the effects of stress exposure and perceived stress on health, the study tests the following hypothesis:
Hypothesis 1: Perceived stress measure will predict a greater number of adverse health outcomes measures than stress exposure measure.
As stress has been shown to be detrimental to many aspects of health, it is important to understand what can reduce its effects. Most stress researchers focus on stress as a risk factor for developing unhealthy lifestyle or adopting maladaptive behaviors, rather than explore those factors that can act as buffers against stress and hardships, such as availability of social support, or psychological features such as optimism, self-esteem, and maintaining a positive outlook on life. Meanwhile, they are important factors that can be instrumental in reducing stress under conditions of war, as they have been shown to help individuals focus on positive experiences, pursue their goals in spite of adversity and cultivate the resources of resilience that are available (Chen and Miller, 2012; Matthews et al., 2010; Windle et al., 2018). Based on these results, we expect that in Ukrainian participants:
Hypothesis 1a: Optimism measure will predict lower levels of perceived stress.
Hypothesis 1b: Optimism measure will predict higher levels of positive mental health (expressed as quality of life and subjective well-being measures).
While stress response is an adaptive reaction in itself, repeated or protracted stressful episodes can induce psychological and physiological changes that are noxious. Stress is one of the risk factors for depression (Tafet and Nemeroff, 2016). Depression, in its turn, is one of the most serious health concerns of the modern world, responsible for the aggravated situation with disease and disability in epidemiological profiles of many countries (Yang et al., 2015). Apart from profoundly affecting individuals’ mental reactions, their daily activities and quality of life, depression also has many comorbidities and makes the prognosis of many chronic diseases more complicated (Byers and Yaffe, 2011; Cizza et al., 2010; Epel et al., 2004; Knol et al., 2006; Krishnan and Nestler, 2008; Whitehead et al., 2002). War creates stressful environments and life-threatening conditions which are known to breed depression. We therefore expect that in Ukrainian participants:
Hypothesis 2: Depression measure will predict a higher likelihood of adverse physiological symptoms (expressed as poorer self-rated health and wellness).
Hypothesis 2a: Higher levels of perceived stress will predict a higher likelihood of depression.
Hypothesis 2b: Optimism measure will predict a lower likelihood of depression.
Migration is a separate factor in health and has its specific stressors. “Push” and “pull” theories of migration highlight different motivations for individuals to relocate, their expectations and their satisfaction with the new place of residence or its prospects (Castles, 2010; Valenta, 2010). Adaptation outcome and stress levels upon migration depend on the motivation to move (Johansson et al., 1997; Levecque et al., 2007). In the context of war, individuals or families are forced to seek physical safety; some escape from the zones of armed conflict to become internally displaced individuals (IDPs) or refugees. A refugee status is a determinant of health by itself. Millions of Ukrainians from different regions of the country moved west to safer Ukrainian territories or sought asylum abroad. The available published reports from studies of IDPs in Ukraine indicate various somatic and mental health problems, including PTSD. The results converge on war-induced displacement’s undermining health resources of Ukrainians 1 . It is therefore plausible to hypothesize that in Ukrainian participants:
Hypothesis 3: Experience of being displaced or moving abroad after February 2022 will be associated with more symptoms of negative mental health and poorer self-rated general health.
Method
Participants
The data collection was conducted in Kyiv, Ukraine in November 2022. The data was collected online by means of a Google-form to enable recruiting respondents who have left Ukraine. The Ethics Committee waived the need for ethics approval and the need to obtain consent for the collection, analysis and publication of the anonymized, retrospective data obtained via online survey for this non-interventional study. Completing the survey was taken as the indication of consent. Participants were recruited by using social media platforms and emailed invitations within personal social networks of individuals enrolled in Fall classes at the Department of Sociology at the National University of Kyiv-Mohyla Academy University. The final sample (n = 213) consisted of 139 females, 70 males and four participants self-identified as other, with the age range of 16–75 years. Approximately 23.9% of participants were married, 40.4% were single, 31.5% had a boyfriend or girlfriend, 3.3% were divorced and two individuals made no answer. About 71.4% of participants were childless and 27.6% had one child or more. About 72.3% of respondents had siblings. Approximately half of the participants were gainfully employed at the time of the survey. Most of the surveyed individuals had some college education and reported having equally educated parents. Most of the respondents (70%) came from large Ukrainian cities. The sample was diverse in terms of relationship status, family composition, SES and housing arrangements. The details of sample composition are offered in Supplemental Table A1. For those who have moved abroad after February 2022, Germany (13), Poland (6) and the United Kingdom (5) were among the most frequent destinations of migration mentioned by the participants.
Measures
Stress
The survey was designed to assess the effects of different kinds of stressors on health outcomes. Two measures of stress were used in the study. To assess the actual stress exposure, in the beginning of the survey a series of items listing various stressful events/experiences was introduced. The stressful events inventory contained 10 items each representing an external factor associated with the dangers of war. Descriptive statistics for stress exposure items are presented in Supplemental Table A1. To evaluate the integral effect of stress exposure in addition to evaluating the contribution of each of the stressors, the cumulative index of stress exposure was computed (Table 1). This stress exposure measure was conceived not as an interpretable theoretical dimension but as a summation of the experiences relevant to war conditions.
An abridged version of Cohen’s perceived stress scale (Cohen et al., 1983, originally 14 items, α = 0.72) was employed to assess the perceived stress severity (11 items, α = 0.85). The Ukrainian version of the scale had adequate validity and has shown efficacy with various Ukrainian-speaking samples before and during the full-scale invasion with comparable results (α = 0.82–0.85) (Maltseva, 2021; Maltseva, n.d.-a, b). Apart from these two stress measures, the survey collected self-rated data about the positive and negative symptoms of mental and physical health, to give a complete and nuanced picture of the effects of war-related experiences on both sides of the mental health continuum.
Correlation of measures.
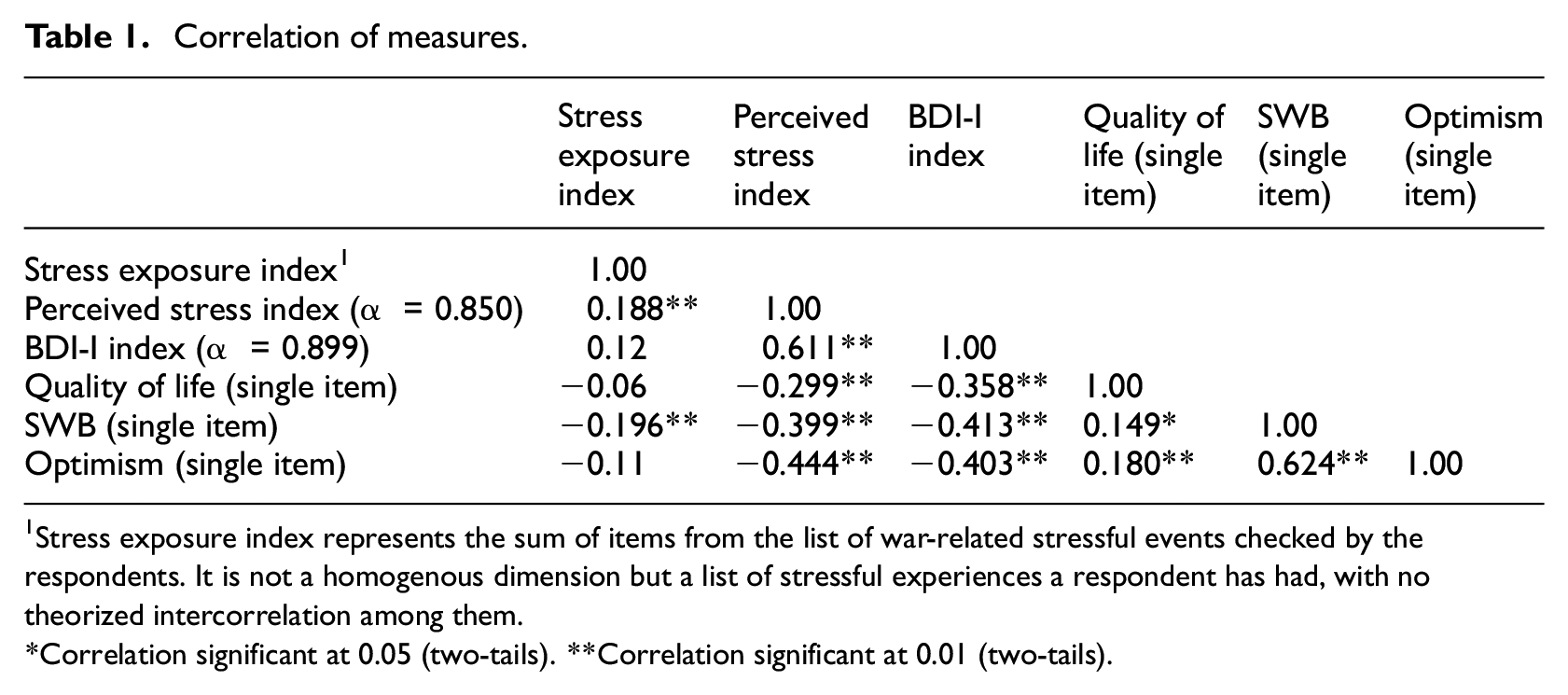
Stress exposure index represents the sum of items from the list of war-related stressful events checked by the respondents. It is not a homogenous dimension but a list of stressful experiences a respondent has had, with no theorized intercorrelation among them.
Correlation significant at 0.05 (two-tails). **Correlation significant at 0.01 (two-tails).
Psychological risk factors compromising health
The instrument included a validated measure of depression (BDI-I, Beck et al., 1961, 21 items, α = 0.85). The scale had adequate validity (α = 0.89) and was used with various Ukrainian-speaking samples previously (α = 0.91−0.93) (Maltseva, 2021). To assess the effects of neuroticism and aversive traits on war-induced distress, NEO-PI (100 items) and the Dark Triad scale (27 items) 2 were also used in this study. Only a measure of depression is discussed here.
Psychological protective factors
To test the expectations above, a variable measuring one’s evaluation of one’s current life was added. For this item, the informants were asked to rate their current life on the scale from 1 (the worst life imaginable) to 10 (the ideal scenario) to create the life quality variable. Two other single item measurements assessing the positive outlook on life were subjective well-being (SWB) (“This world is a good place,” 1 item) and optimism (“All in all, I consider myself an optimist,” 1 item). Both items were rated on a scale from 1 to 4, 1 being “not at all accurate” and 4 being “absolutely accurate.”
The total number of variables in the survey was 198. Except the clinical scale for depression, all the propositions were rated on the Likert scale from 1 to 4. Standard demographic information about respondents’ life, childhood and health status (40 items) was collected at the end of the survey. The instrument was administered in Ukrainian. Indices were computed for all scales. The correlations of all metrics (including the Cronbach’s alphas for all scales) used in the study are presented in Table 1.
Results and discussion
After data cleaning, descriptive statistics and validity testing for scales, to test the propositions embedded in the hypotheses, linear regression analysis in SPSS was used (IBM Corp. Released, 2017). The results of regression analysis are presented in Table 2.
Simple linear regressions.
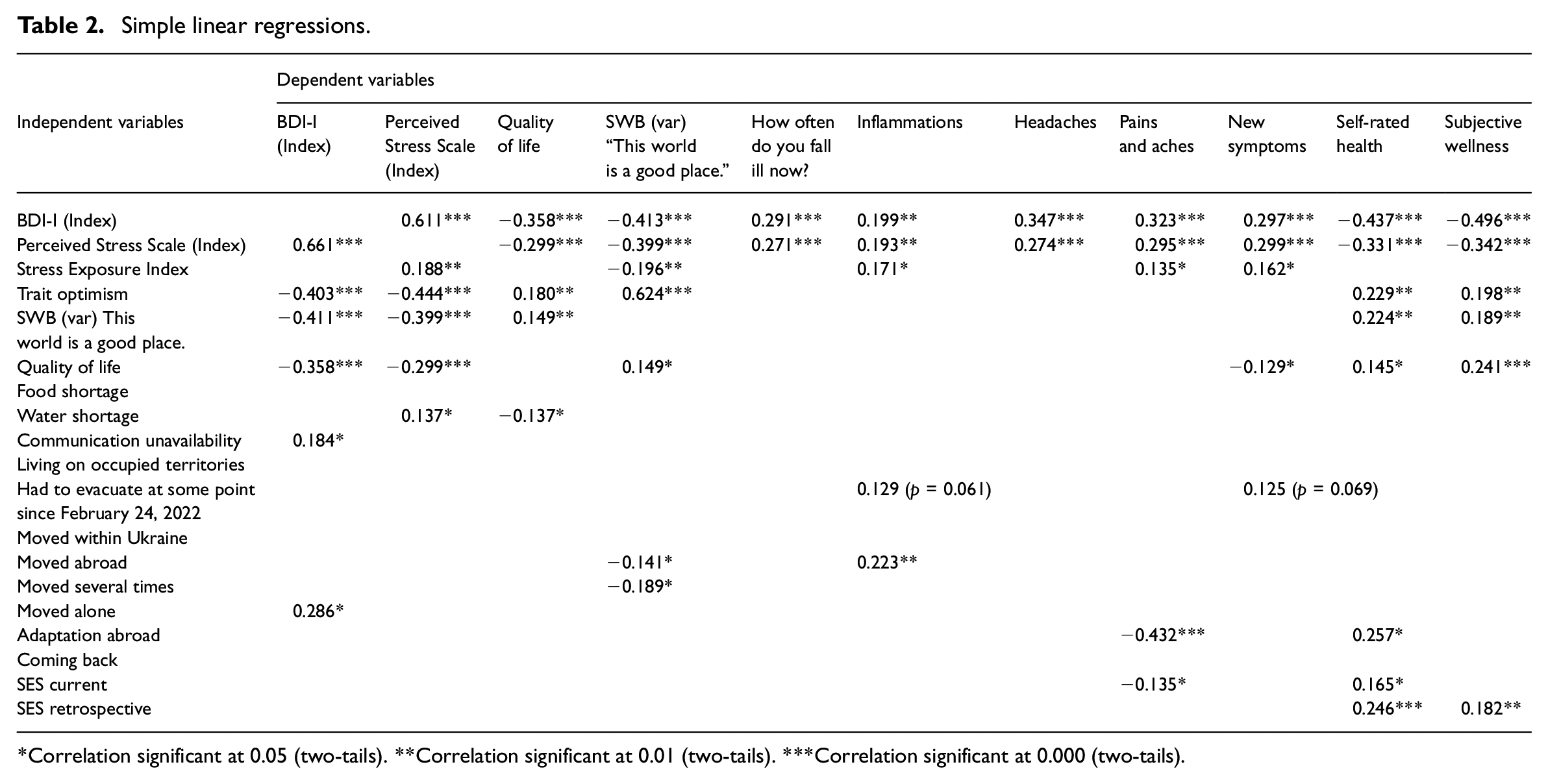
*Correlation significant at 0.05 (two-tails). **Correlation significant at 0.01 (two-tails). ***Correlation significant at 0.000 (two-tails).
To evaluate the differential effects of war-induced stress with respect to residence disruption, a cumulative index of stress exposure (10 items) was compared across the groups of participants who have moved within Ukraine, who have moved abroad, and who have not moved at all. Then the data on stress and health status was subjected to a series of analyses using t-test, analysis of correlations and regression analysis. These results complement the analysis presented in Table 2.
Stress exposure and perceived stress
The effects of stress exposure and perceived stress on health were assessed in linear regression analysis, focusing on mental (both positive and negative) and physiological health outcomes. Table 2 indicates that different kinds of stress have different effects on various aspects of life and health dimensions. The results are congruent with earlier findings regarding stronger predictive effects of perceived stress over stress exposure, confirming both a greater breadth and magnitude of perceived stress effects on health. One perception of an event as stressful can vary across individuals and is prone to interpretation, but the impact of perceived stress on health measures was greater than that of actual stress exposure measure (Table 2). Perceived stress was also a predictor of a greater number of health outcomes, which supports Hypothesis 1. These results lend support to the argument about the cognitive component of stress and its causal mechanism is worth further exploration.
Interestingly, food and water shortages were reported as less stressful compared to lack of cellular phone connection or mobile internet that enable access to the news and communication with the loved ones.
Protective psychosocial resources against stress
Among the psychological resources that protect against the destructive effects of perceived stress and onset of depression we can list the optimistic outlook on life, perceiving the world as just and availability of family and friends to offer social support if an individual is abroad (Table 2). Lower perceived stress was predicted by higher levels of optimism (Table 2). Optimism also predicted symptoms of positive mental health as manifested in better quality of life and higher subjective well-being (Table 2). Thus the data support Hypotheses 1a and 1b. To enhance the reliability of findings, further testing using multi-item scales for optimism is advisable.
Depression measure predicted all the negative health outcomes and undermined the positive evaluation of the quality of life (Table 2), as proposed in Hypothesis 2. While stress exposure had no effect on depression measure, the perceived stress index had a strong positive effect on depression (Table 2). These findings support Hypothesis 2a. Optimism showed buffering qualities with respect to the likelihood of depression (Table 2). The Hypothesis 2b is therefore supported. As hypotheses were tested based on self-reported data on depression, it lends them qualified support; using several clinical measures of depression is necessary for achieving more conclusive results.
While high SES was a predictor of better self-rated health and wellness, its hypothesized ability to buffer perceived stress and depression during the war was not supported (Table 2). Yet there were some interesting findings for the effects of childhood SES versus current SES with respect to self-rated health and wellness measures. Namely, current SES was less influential than childhood SES (Table 2). In the light of life history theory, this finding might suggest that high childhood SES participates in the processes building up the resources of resilience that help overcome adversity throughout the life course as part of the slow life history orientation strategy (Figueredo et al., 2017).
Stress, forced migration and health
Figure 1 shows that both the individuals who have moved within Ukraine and those who have sought safety outside Ukraine had higher stress levels that those Ukrainians who stayed at home. Those Ukrainians who have moved within Ukraine and those who have evacuated abroad had higher perceived stress levels than the averaged stress profile in the sample. Those Ukrainians who have moved outside Ukraine reported the highest levels of stress among the surveyed participants. This supports the proposition in Hypothesis 3.
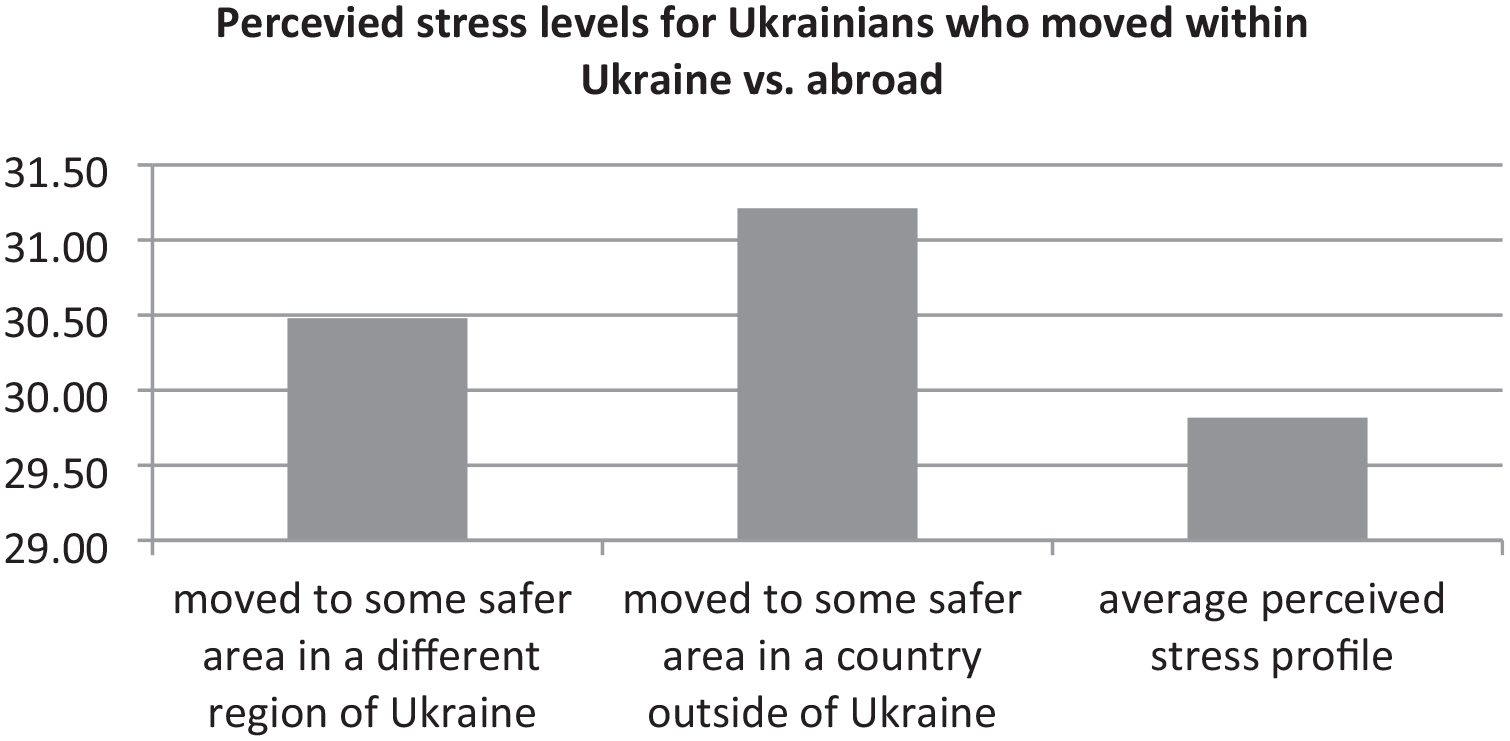
Perceived stress index: group comparison.
The individuals who have moved within Ukraine and especially those who have moved abroad also reported having more inflammation and even developing new symptoms (Table 2). Although the latter result only approaches the statistically significant level and therefore can only offer qualified support to Hypothesis 3, it deserves attention.
Albeit the effects of residence disruption (leaving one’s domicile and seeking refuge in a safer region within Ukraine or abroad) on various dimensions of health did not show uniformly statistically significant results in the sample, there were some regularities that are worth exploring further. For example, while the experience of forced migration showed no effects in self-rated health or wellness, those who have moved to seek refuge abroad (especially if they had to move several times before reaching their destination) reported having faster onset of inflammatory processes, suggesting a more severe stress reaction. Adaptation abroad (liking one’s new place of residence) affected the health outcomes directly in predictable ways (Table 2). These findings also lend qualified support to Hypothesis 3.
Two-sample t-test was performed to test if the Ukrainians who at some point had to move to a safer place reported better self-rated health and wellness than those who did not ((t(df) = −17.34, p = 0.000, two-tailed)). The results support the first part of this proposition, suggesting that individuals who had to move to a safer location rated their health status as better but did not report feeling better than those who did not move. This result does not contradict the available results of monitoring studies 3 . In regression analysis this finding is echoed by the results for individuals who reported liking their new place of residence (Table 2).
There were some additional findings that were marginally related to the working hypotheses. The effects of cumulative stress exposure on health status during the war were measured to complement the findings regarding the differential effects of various types of stressors (difficulty accessing food, drinking water, mobile phone connection etc.) on self-reported measures of positive and negative mental health as well as self-rated physical health and wellness. To do that an index of stressful traumatic events was constructed based on the list of stressful events (Table A1). The exposure to stress in the sample ranged from 0 to 13. The informants who reported at least one stressful event were then split into quartiles and an average self-rated health score was computed for each quartile. The first quartile (corresponding to the lowest number of stressful events) span 1–3 points for stressful events experienced by the participants, the second quartile 4–6 points, the third quartile 7–9 points and finally the fourth quartile 10–13 points. Although the relationship between the number of stressful events experienced by the participants and self-rated health did not have a linear shape, the data suggest that (1) with the increase of the number of stressful events the self-reported health declined and (2) after six stressful events the further increase in number of events did not affect changes in self-rated health (Figure 2). This dynamics echoes the results of Karatzias et al. (2023) and also earlier results of Anda et al. (2006) for adverse childhood experiences.
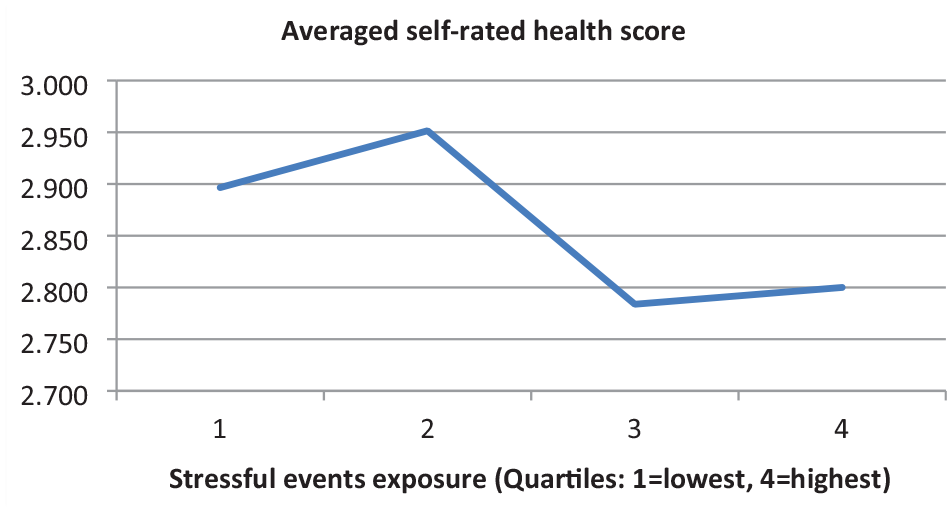
Gradient in health due to stress exposure (quartiles).
Conclusions
This Ukrainian study set out to evaluate the differential effects of stress exposure and perceived stress on health outcomes, psychosocial factors that could serve as the risk factors and protective factors, and the impact of migration experiences on self-rated health during the war. The following regularities were found. First of all, perceived stress was the major risk factor for negative health outcomes that has emerged in the analysis. Perceived stress exacerbated the realities of war bearing on both mental and physiological self-reported health measures. Cumulative stress exposure during war was also taxing for health outcomes. Social support and optimism, on the other hand, were important for successful coping, higher quality of life and better mental health during war. Finally, while being removed from the war hostilities increased physical safety, there are indications that those individuals who had to evacuate (especially outside Ukraine) suffered an earlier onset of negative health outcomes (or a harsher stress response) and will require professional help upon their return to Ukraine.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241259728 – Supplemental material for Stress exposure, perceived stress, protective psychosocial factors, and health status in Ukraine after the full-scale invasion
Supplemental material, sj-docx-1-hpq-10.1177_13591053241259728 for Stress exposure, perceived stress, protective psychosocial factors, and health status in Ukraine after the full-scale invasion by Kateryna Maltseva in Journal of Health Psychology
Footnotes
Data sharing statement
The data that support the findings of this study are currently not publically accessible because of the continued state of martial law in Ukraine but can be made available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The Ethics Committee of the National University of Kyiv-Mohyla Academy waived the need for ethics approval and the need to obtain consent for the collection, analysis and publication of the anonymized, retrospective data obtained via online survey for this non-interventional study.
Informed consent
Please see above.
Pre-registration
The study was not pre-registered.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.