
Abstract
Subjective social status (SSS), the perception of one’s social standing compared to others in society, and socioeconomic status (SES) are interconnected but distinct determinants of health. Intermediary factors such as distress and health behaviors can contribute to this relationship. This pre-registered study hypothesized that, in the early months of the COVID-19 pandemic, nonspecific psychological distress would indirectly link SSS and SES to perceived changes in three health behaviors: sleep quality, physical activity, and alcohol consumption. Data from 412 US adults were collected from April to June 2020 through an online cross-sectional survey. Findings indicated that lower SSS was indirectly associated with lower current sleep quality, worsened sleep quality, and decreased physical activity since the pandemic onset via greater psychological distress. Path analyses controlled for age, gender, race, COVID-19-related worry, and shelter-in-place status. Results are discussed in light of findings from COVID-19 research and the broader literature on SES health disparities.
The initial months of the 2019 coronavirus disease (COVID-19) pandemic presented significant challenges as the virus rapidly spread, leading to global stress (De Sousa et al., 2021). The pandemic’s notable impact and subsequent policy changes disrupted and affected crucial aspects of everyday life. Specifically, the COVID-19 pandemic threatened various domains including physical health, social relationships, daily routines, finances, and mental health (e.g. Tambling et al., 2021). The all-encompassing nature of the pandemic, combined with its characteristics like novelty, unpredictability, and uncontrollability, had significant implications for the health and well-being of millions of people worldwide (Rettie and Daniels, 2021).
Psychological distress is often considered indicative of anxiety and depression and tends to emerge in response to repeated or prolonged exposure to stressors, coupled with a lack of sufficient psychological resources to effectively cope with them (APA, 2023; Gallo and Matthews, 2003). Despite the disruptive nature of the COVID-19 pandemic, challenging experiences were not experienced equally across populations. This is particularly relevant among individuals from different socioeconomic backgrounds who, in turn, experienced varying consequences of this global stressor. For example, a worldwide study conducted during the first few months of the pandemic, between March and May of 2020, found that those who reported less education also reported experiencing more psychological distress (Jiang et al., 2022). A similar pattern emerged in a sample of United States (US) adults when household income was considered instead of education (Daly and Robinson, 2021). These findings align with existing empirical studies and theoretical frameworks, such as the reserve capacity model (Gallo and Matthews, 2003), which suggests that individuals with lower socioeconomic status (SES) tend to experience perceived stress more frequently (Cohen and Janicki-Deverts, 2012) and more severely (Almeida et al., 2005) than their higher SES counterparts. Perceived stress and psychological distress, more broadly, can influence health behaviors (Kraft and Kraft, 2021). To explain the connection between SES and health outcomes, the reserve capacity model (Gallo and Matthews, 2003) suggests that the frequent and intense perceived stress and the negative emotions associated with stress are notably experienced by those with lower SES due to a lower and less frequently replenished reserve of physical and psychosocial resources. As a result, the model posits that negative emotions and cognitions are mechanisms that explain why low SES is related to deleterious patterns of health behaviors. This study aims to understand the associations between SES, psychological distress, and health behaviors during the onset of the COVID-19 pandemic.
SES and health behaviors
Amidst the onset of the COVID-19 pandemic, it became apparent that individuals encountered difficulties maintaining healthy behaviors (e.g. Chen et al., 2022). Multiple studies reported a high prevalence of sleep difficulties during the early months of the pandemic. For instance, Beck et al. (2021) reported sleep issues in 74% of their French sample, while a meta-analysis of 13 countries found that approximately 35% of study participants experienced sleep problems (Jahrami et al., 2021). SES has long been known to influence the choice and quality of health behaviors that significantly impact physical health (Pampel et al., 2010), and this association persisted throughout the pandemic. During the first month of the COVID-19 outbreak, individuals with the lowest income reported more sleep issues compared to those with the highest income (Beck et al., 2021).
Other health behaviors, including alcohol use and physical inactivity, also display differences across the socioeconomic gradient (Nandi et al., 2014). For example, one study assessed self-reported educational attainment, income, and weekly physical activity among more than 17,000 individuals in the Netherlands and found that lower SES individuals were prone to reduced physical activity after May 2020 compared to their higher SES counterparts (De Boer et al., 2021). Similar trends were observed in other studies conducted during the same period (e.g. Grubben et al., 2022). In contrast, the association between SES and alcohol consumption during the pandemic has been less conclusive. A meta-analysis of studies across 38 countries indicated that alcohol use increased with higher SES (Kyaw Hla et al., 2021), while others found the opposite relationship (Laghi et al., 2022). In the latter study, young adults from Italy with lower SES exhibited higher odds of problematic alcohol use, as measured by frequency and quantity of drinks, compared to those with higher SES between April and May of 2020 (Laghi et al., 2022).
Psychological distress and health behaviors
The pandemic led to a significant increase in symptoms of depression and anxiety compared to pre-pandemic levels (Wanberg et al., 2020). Notably, there was a surge in distress in the US between mid-March and April 2020 as the country implemented policies to curb the spread of the virus (Daly and Robinson, 2021). In turn, heightened distress coincided with changes in health behaviors, as meta-analyses and systematic reviews found positive associations between distress and depressive symptoms with alcohol consumption across 58 countries (Acuff et al., 2022), sleep problems across 39 countries (Alimoradi et al., 2021) and reduced physical activity across 10 countries (Violant-Holz et al., 2020).
Distress during the pandemic also contributed to retrospective reports of how health behaviors changed following the start of the pandemic. For the most part, studies reported that behaviors either did not change or worsened. Within a French sample, sleep issues increased in 54% of participants (Beck et al., 2021), while no change in sleep duration was found among 50% of participants in an Australian sample (Stanton et al., 2020). Among other health behaviors, this study also found that physical activity decreased in 48% of the sample and 55% of participants reported no change in alcohol consumption following the onset of the pandemic (Stanton et al., 2020). Regarding psychological distress, one US-based study found that distress was associated with an increase in alcohol consumption both in terms of the number of drinks and the number of days of consumption among university students following a pandemic-related university closure compared to the week before closure (Lechner et al., 2020). Similar associations were found by Stanton et al. (2020), where psychological distress, manifested as symptoms of depression, anxiety, and stress, was associated with reduced physical activity, poorer sleep quality and reduced time asleep, more frequent alcohol use, and increased smoking among Australian adults. Building on these findings, the present study aims to assess SES as a predictor of psychological distress and subsequent changes in health behaviors.
Subjective social status
In addition to SES, one’s perceived socioeconomic standing relative to others, known as subjective social status (SSS), is an equal predictor of overall well-being. SSS is associated with negative affect and lower self-rated health (Operario et al., 2004), along with various aspects of well-being, including perceptions of control and depression (Singh-Manoux et al., 2003). While SSS and SES demonstrate a moderate correlation, evidence suggests that SSS adds predictive value to physical health outcomes beyond the influence of SES (Cundiff and Matthews, 2017). Traditional SES indicators, such as employment and income, can be vulnerable to fluctuation during times of economic uncertainty, such as the COVID-19 pandemic. During the pandemic, income or job loss might not have precisely reflected an individual’s actual status. Conversely, SSS accounts for historical and anticipated changes in one’s social status and may offer more reliability as a measure of status (Destin et al., 2017). For these reasons, the current study incorporates both SES and SSS measures.
The present study
The primary objective of the present study was to build upon prior research and explore the intervening role of psychological distress in explaining the relationships between SES and SSS and engagement in health behaviors following the onset of the COVID-19 pandemic. Guided by the reserve capacity model, we hypothesized that greater psychological distress would mediate the association between low SES and SSS, and less healthy self-reported behaviors (i.e. sleep quality, alcohol consumption, and physical activity). Additionally, we expected greater psychological distress to be related to perceptions of worsened behavior changes since the start of the pandemic, including perceptions of sleep quality change, alcohol consumption change, and physical activity change.
Method
Sample and procedure
Data were collected between April 24 and June 30, 2020. Participants were 479 adults between ages 18 and 85 recruited online across social media sites (e.g. Facebook, Twitter) and emails advertised across universities. To be eligible for participation, respondents were required to (1) be at least 18 years of age, (2) reside in the US, and (3) speak and read English. Participants completed consent followed by an online battery of questionnaires, covering a variety of psychosocial and health surveys. Only variables central to the scope of this study were used in the present reporting. Those who took part in the study were entered into a raffle for the chance to win one of ten $50 electronic gift cards. The study was approved by the university’s institutional review board. The model and analysis plan were pre-registered and are publicly available (https://aspredicted.org/be9t9.pdf). For the present analyses, participants were additionally excluded if they completed the study in less than 5 minutes and demonstrated inattention such as selecting one answer response for all survey questions (n = 41) or did not complete the surveys corresponding to any of the health behavior outcomes (n = 26). The final sample consisted of 412 adults (298 females, 93 males, 3 nonbinary, 18 missing).
Measures
Education
Participants reported their highest completed degree of education ranging from 1 (no school/some grade school) to 7 (Professional degree [PhD, MD, EdD, DDS., etc.]).
Income
Annual pre-tax household income, including all forms of potential income (e.g. government assistance) from 2019 was self-reported on a scale from 1 (less than $5,000) to 14 (more than $150,000). Income from 2019 is likely to be a more stable reflection of individuals’ financial status compared to reports from 2020 that were likely impacted by the COVID-19 pandemic.
Employment status
Participants reported their current employment status which included categories of working full-time, working part-time, student, retired, homemaker, disabled, and unemployed. These were further categorized into 3 (full-time), 2 (part-time), and 1 (unemployed). Despite their qualitative differences, those who reported being a student, a homemaker, retired, or disabled were placed in the unemployed category in line with the United States Census Bureau (2019) definition of employment (i.e. those working and receiving payment).
The three manifest variables of education, income, and employment status were specified as indicators of the SES latent variable (ω = 0.645, 95% CI [0.535, 0.759]) as modeled in previous work (Senn et al., 2014).
Subjective social status (SSS)
Using the MacArthur Scale of Subjective Social Status (Adler et al., 2000), participants were shown a picture of a 10-rung ladder and told to think of each rung as an economic standing in the US with the top rung reflecting the highest standing and the bottom rung reflecting the lowest standing. Considering money, education, and jobs, they were asked to select the rung they stand on at this time in their life relative to other people in the US. Higher scores reflected higher relative SSS, which was incorporated as an exogenous manifest variable in the model.
Psychological distress
Three latent variables, perceived stress, depressive affect, and depressive cognition were loaded onto one overarching latent factor, psychological distress, to create a second-order model (ω = 0.825, 95% CI [0.810, 0.837]).
Perceived stress
The 4-item Perceived Stress Scale (Cohen et al., 1983) was used to assess stress appraisals of recent situations. Participants responded to items inquiring about controlling the important things in life, handling personal problems, overcoming difficulties, and feeling that things were going their way. Participants reported how often these occurred in the past 2 weeks (1 = never, 5 = very often) where higher values indicate more perceived stress (ω = 0.765, 95% CI [0.717, 0.800]).
Depression
Depressive symptoms were measured using a shortened version of the Center for Epidemiological Studies Depression scale (CES-D; Andresen et al., 1994) which contained 10- items that captured how often depressive symptoms were experienced in the past week. Each item was reported on a scale from 1 (rarely or none of the time) to 4 (most or all of the time). One item (i.e. “My sleep was restless.”) was not used in the present analyses as it would have conflated with the sleep outcomes. Two items (i.e. happy and hopeful) were reversed so that higher scores represented greater depressed affect. Items were separated into factors modeled from Radloff (1977) to capture the multifaceted nature of depressive symptoms. Five manifest items indicated a latent variable representing depressive affect and emotions (ω = 0.805, 95% CI [0.772, 0.834]) and four manifest items were loaded onto a second latent construct pertaining to depressive cognitions and activity (ω = 0.805, 95% CI [0.768, 0.834]).
Health behaviors
Three behaviors associated with health were measured: sleep quality, physical activity, and alcohol consumption. Sleep quality was assessed using one item from the shortened version of the Pittsburgh Sleep Quality Index (Famodu et al., 2018). Participants reported the quality of sleep over the past 2 weeks (1 = very bad, 4 = very good). Physical activity was recorded as the self-reported number of times per week within the past month that participants engaged in at least 30 minutes of exercise enough to raise their breathing rate not including housework or activities part of work (Milton et al., 2011). Response options ranged from 1 (not at all) to 5 (every day). Finally, one item of alcohol use was adapted from Cohen et al. (1993), “Since the COVID-19 pandemic began, how many days per week have you been drinking alcohol?” on a scale from 1 (never drink) to 9 (usually drink 7 days). Alcohol consumption was Blom-transformed to adjust the positive skew of responses on this item. These three health behavior variables were included as manifest outcomes in the model.
Perceived health behavior change
Following each health behavior item, participants were asked to think back before the COVID-19 pandemic began and report how they perceived each behavior to have changed. Sleep quality was recorded on a 5-point scale from 1 (a lot worse) to 5 (a lot better). Physical activity and alcohol consumption were recorded on a 5-point scale from 1 (decreased a lot) to 5 (increased a lot). This approach has been adopted in previous investigations of behavior change during COVID-19 (e.g. Beck et al., 2021; Gao and Scullin, 2020; Stanton et al., 2020). These three variables were represented as manifest outcomes in the model.
Covariates
Covariates including age, race, and gender were selected according to their associations with health behaviors reported in prior research (e.g. Mezick et al., 2008). For analytical purposes, race was dummy coded as White/Caucasian (0) versus all others (1) and gender as male (0) versus female (1).
Two variables were also included to control for any specific effect that COVID-19 had on participants’ environment and their worry about virus contraction. First, the participant-reported zip code and the survey completion date were used to determine whether the participant was under a shelter-in-place ordinance (i.e. lockdown; no (0), yes (1)). The shelter-in-place regulations at the time of survey completion were assessed at the county level within each state through executive orders located on state or county government websites. A single item (i.e. “How worried have you been about contracting COVID-19?”) was used to assess COVID-19-related worry. This item was recorded on a 5-point scale from 1 (not at all) to 5 (very worried).
Analysis plan
Data preparation and bivariate correlations were conducted in SPSS, and internal consistency estimates and structural equation modeling (SEM) were implemented in Mplus (version 8.1, Muthén and Muthen 1998–2017) using maximum likelihood estimation. First, measurement models for SES and psychological distress were specified to examine how well the indicators loaded onto these latent factors. Next, direct and indirect effects of SES and SSS on health behaviors (i.e. sleep quality, physical activity, alcohol consumption, and their respective self-reported change variables) through psychological distress were computed. Omega was used to compute model-based internal consistency reliability of the latent factors (McDonald, 1999). This approach does not assume tau equivalence; that is, this model does not assume that each item equally identifies the factor. Thus, omega is preferred over Cronbach’s alpha in the presence of complex or multidimensional factors (Reise et al., 2013). Bias-corrected confidence intervals were generated from 5000 bootstrap resamples. Data contained 2.8% missing values. Missing data were handled with full information maximum likelihood.
The covariates in the model were determined by examining bivariate correlations with endogenous variables. Gender, age, race, shelter-in-place, and COVID-19-related worry were associated with psychological distress and were subsequently specified in the model as covariates for this endogenous mediator. Covariates specified for each of the health behaviors were as follows: age, shelter-in-place, and COVID-19 worry for sleep quality; age, race, and shelter-in-place for alcohol use; race for physical activity and change in alcohol consumption; age and COVID-19 worry for change in sleep quality. No covariates were correlated with change in physical activity; thus, none were specified for this outcome. SES and SSS were correlated as shown in previous work (Cundiff and Matthews, 2017). Error terms among the health behaviors were allowed to freely covary. Similarly, covariates were allowed to covary with each other.
Model fit was assessed using the root mean square error of approximation (RMSEA) and the comparative fit index (CFI). RMSEA values no larger than 0.06 suggest good fit (Hu and Bentler, 1999) and values 0.08 and lower indicate reasonable fit (Browne and Cudeck, 1992). CFI scores nearer to 1 indicate better fit, with a preference for values 0.95 or higher (Hu and Bentler, 1999). The chi-square test was not used to assess model fit as it is directly influenced by sample size and biased in large samples (Bentler and Bonett, 1980); however, it is included to maintain consistency and transparency across model fit reporting standards.
Model adjustments
The pre-registered model contained a fourth health behavior: smoking frequency. However, as only 3.3% of the sample reported being smokers, this outcome was excluded. Additionally, perceived stress was the pre-registered intermediary variable of interest with depressive symptoms included as a covariate. In the present model, perceived stress and depressive symptoms were combined into a latent factor of psychological distress as the items were moderately associated, contributed to improved model fit, and remained in line with the conceptual underpinning of the theoretical model.
Results
The characteristics of the sample and bivariate associations among all the study variables are displayed in Table 1. Among the perceived health behavior change outcomes, 31% of the sample reported no change in physical activity levels, 40% reported a decrease, and 29% reported an increase. For alcohol use, 60% reported no change, 28% reported an increase, and 12% reported a decrease in consumption. For sleep quality, 42% reported no change in sleep quality since the pandemic began, 44% reported worse sleep, and 14% reported better sleep.
Bivariate correlations among study variables.
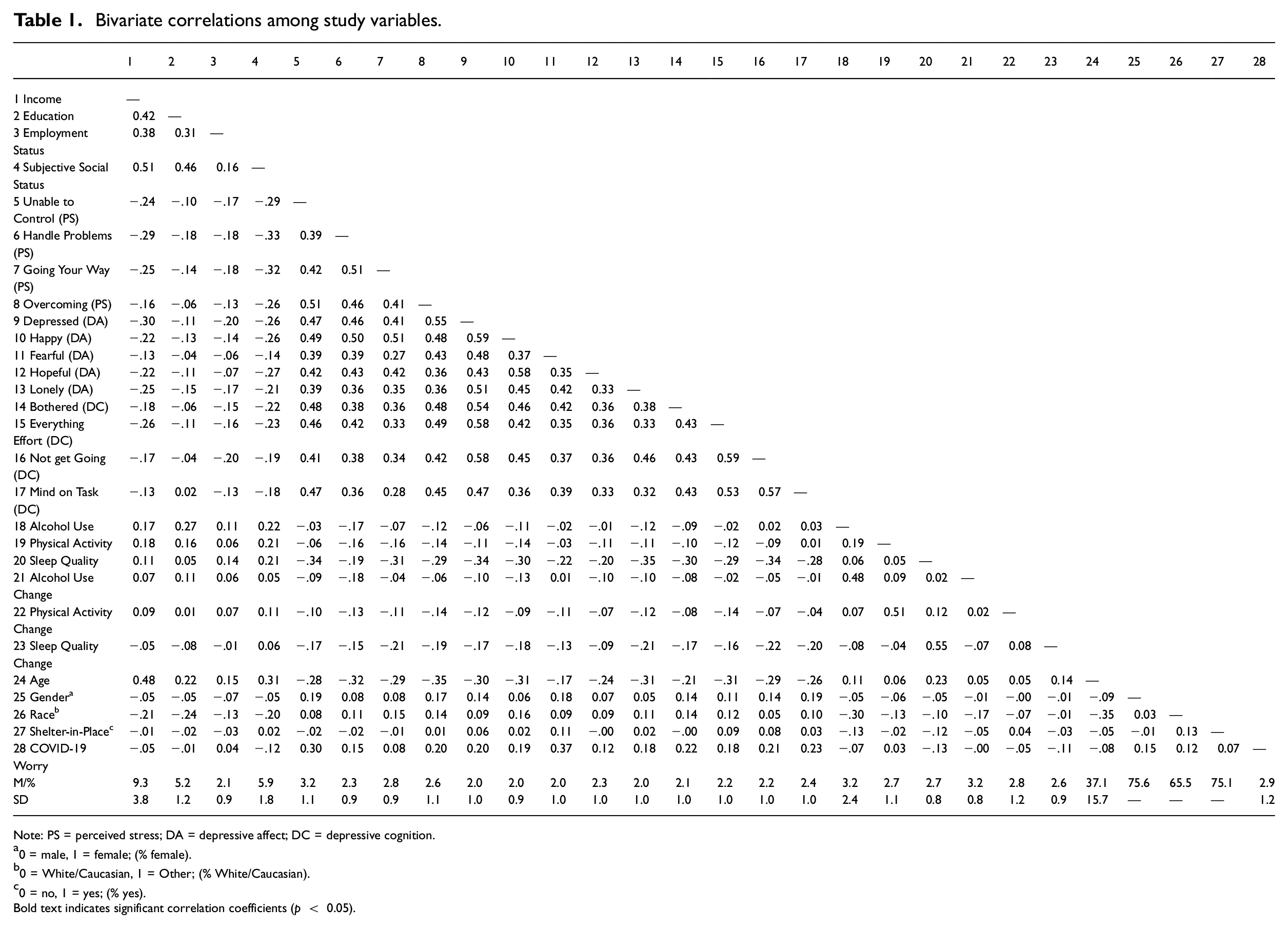
Note: PS = perceived stress; DA = depressive affect; DC = depressive cognition.
0 = male, 1 = female; (% female).
0 = White/Caucasian, 1 = Other; (% White/Caucasian).
0 = no, 1 = yes; (% yes).
Bold text indicates significant correlation coefficients (p < 0.05).
Measurement models for SES and psychological distress
The confirmatory factor analysis revealed significant factor loadings for income (β = 0.720, p < 0.001), education (β = 0.585, p < 0.001), and employment status (β = 0.529, p < 0.001) indicating SES; however, this model was saturated (χ2(0) = 0.000, p < 0.001, RMSEA = 0.000, CFI = 1.000). The amount of observed information available was equal to the number of estimated parameters limiting the interpretation of the fit indices. 1
The second-order latent factor of psychological distress demonstrated reasonable fit (χ 2(62) =176.312, p < 0.001, RMSEA = 0.067, 90% CI [0.055, 0.079], CFI = 0.940) and was well-defined by perceived stress (β = 0.956, p < 0.001), depressed affect, (β = 0.973, p < 0.001), and depressed cognition (β = 0.898, p < 0.001).
Direct associations to psychological distress
Overall model fit of the hypothesized structural model was adequate (χ2(298) = 684.320, p < 0.001, RMSEA = 0.056, 90% CI [0.051, 0.062], CFI = 0.885).
Direct pathways among the study variables are presented in Figure 1. There was a significant direct inverse association between SSS, but not SES, and psychological distress such that lower SSS was associated with greater psychological distress. Being younger, female, and worrying more about COVID-19 contraction were associated with greater psychological distress. Shelter-in-place and race were unrelated to psychological distress. The total model explained 27.8% of the variance in psychological distress.
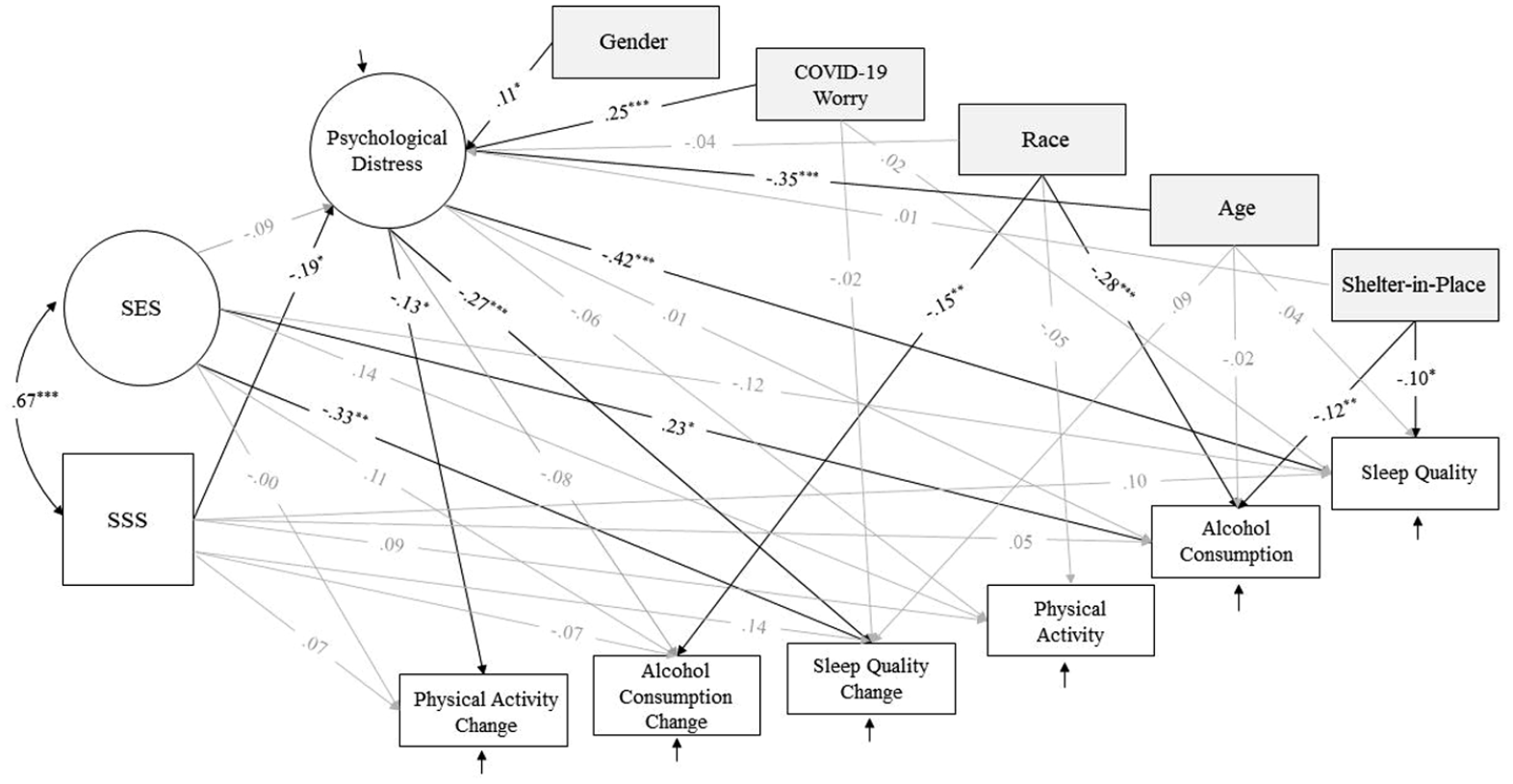
Direct effects path model.
Direct associations to current reported health behaviors
Greater psychological distress was significantly associated with lower reports of sleep quality but was not associated with alcohol consumption or physical activity. Higher SES was directly associated with greater reported alcohol consumption but was not associated with sleep quality or physical activity. SSS was not associated with sleep quality, alcohol consumption, or physical activity. Those under a shelter-in-place ordinance reported worse sleep quality, while COVID-19-related worry and age were not associated with sleep quality. Individuals who identified as White/Caucasian and those not under shelter-in-place orders reported greater alcohol consumption. The model explained 20.7% of the variance in sleep quality, 16.2% in alcohol consumption, and 5.8% in physical activity.
Direct associations to perceived health behavior change
Psychological distress was negatively associated with perceived change in sleep quality and physical activity but was unrelated to perceived change in alcohol consumption. Contrary to expectations, lower SES was associated with higher scores of perceived sleep quality change (i.e. sleep improvements) since the start of the pandemic. SES was not associated with changes in alcohol consumption or physical activity. Associations between SSS and each perceived health behavior change outcomes were nonsignificant. Individuals who identified as White/Caucasian reported higher scores in perceived alcohol consumption change. The model explained 14.8% of the variance in perceived sleep quality change, 3.7% in perceived alcohol consumption change, and 2.5% in perceived physical activity change.
Indirect and total effects
Indirect effect estimates are reported in Table 2. Contrary to expectations, psychological distress did not indirectly link the association between SES to any of the current or perceived change health behaviors. There was a total effect (i.e. direct effect + indirect effect) between SES and alcohol consumption (b = 0.070, SE = 0.032, 95% CI [0.011, 0.138]) as well as perceived change in sleep quality (b = −0.099, SE = 0.037, 95% CI [−0.180, −0.035]). There were no statistically significant total effects between SES and sleep quality (b = −0.022, SE = 0.027, 95% CI [−0.078, 0.027]), physical activity (b = 0.059, SE = 0.040, 95% CI [−0.016, 0.147]), perceived change in alcohol consumption, (b = 0.034, SE = 0.030, 95% CI [−0.023, 0.094]), or perceived change in physical activity (b = 0.004, SE = 0.042, 95% CI [−0.081, 0.086]).
Indirect effects of predictors on health behaviors via psychological distress.
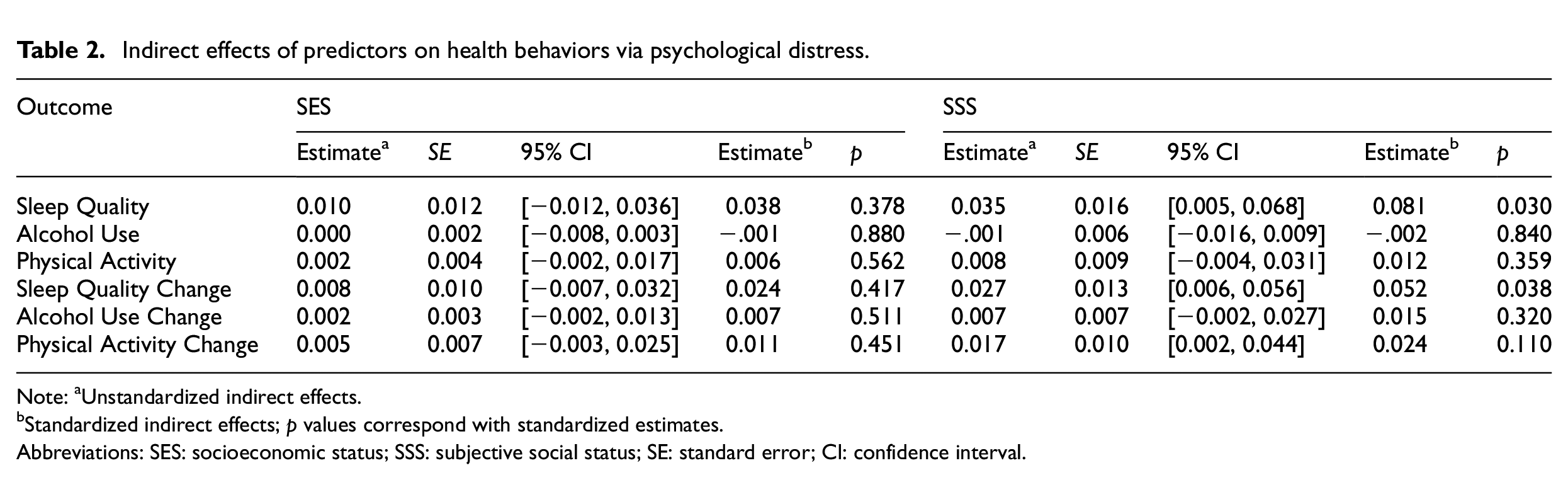
Note: aUnstandardized indirect effects.
Standardized indirect effects; p values correspond with standardized estimates.
Abbreviations: SES: socioeconomic status; SSS: subjective social status; SE: standard error; CI: confidence interval.
There was a significant indirect effect of SSS on current sleep quality, perceived change in sleep quality, and perceived change in physical activity through psychological distress. SSS was not associated with alcohol consumption, physical activity, or perceived change in alcohol consumption via psychological distress. There was a total effect between SSS and sleep quality (b = 0.080, SE = 0.035, 95% CI [0.011, 0.149]) as well as perceived change in sleep quality (b = 0.101, SE = 0.047, 95% CI [0.017, 0.201]) but not for alcohol consumption (b = 0.023, SE = 0.041, 95% CI [−0.062, 0.098]), physical activity (b = 0.066, SE = 0.052, 95% CI [−0.042, 0.165]), perceived change in alcohol consumption (b = −0.025, SE = 0.042, 95% CI [−0.110, 0.053]), or perceived change in physical activity (b = 0.065, SE = 0.056, 95% CI [−0.042, 0.177]).
Overall, experiencing greater psychological distress acted as an intermediate path between lower SSS and worse current reported sleep quality along with the perception that sleep quality worsened and physical activity decreased since the pandemic began.
Discussion
The primary aim of this pre-registered study was to investigate the indirect effect of nonspecific psychological distress on the relationship between SES, SSS, and health behaviors among US adults during the early months of the COVID-19 pandemic. Partially supporting the hypotheses, lower SSS, but not SES, was associated with greater psychological distress. This distress, in turn, was linked to poorer current sleep quality, perceptions of decreased sleep quality, and decreased physical activity since the onset of the pandemic. The model accounted for a greater proportion of variance in the sleep outcomes compared to the physical activity outcome. These findings suggest that psychological distress is a stronger predictor of sleep quality, while factors not included in this study likely have a more significant impact on physical activity. The indirect effects of psychological distress shed light on the role of perceived stress, depressive affect, and depressive cognition in connecting SSS to specific health behaviors. The findings align with previous COVID-19 pandemic studies, which have demonstrated that low SSS is associated with depressive symptoms (Rice et al., 2023) and worsened perceived health (Upenieks et al., 2022).
Despite the moderate association between SSS and SES, they displayed independent associations with distress and health behaviors. SSS was only associated with health behaviors via psychological distress, while, contrary to initial expectations, SES was only directly linked to health behaviors (i.e. higher SES associated with greater alcohol consumption and perceived decreased sleep quality). This finding diverges from previous COVID-19 studies that have demonstrated a link between markers of SES and distress (e.g. Daly and Robinson, 2021). One explanation could be that the present research simultaneously analyzed the effects of SSS and SES on health behaviors, while previous COVID-19 studies considered either SES or SSS but not both. This study demonstrated a robust association between SSS and distress, controlling for the covariation between SSS and SES. Another explanation could be that SSS may serve as a mediator between SES and psychological distress; however, this explanation collides with research showing that SSS and SES have independent, non-overlapping associations with health outcomes (Cundiff and Matthews, 2017; Tan et al., 2020) rather than SSS mediating the link between SES and health. The effects between SES and sleep quality (i.e. decreased sleep quality) were in contrast with the paths found between SSS and sleep quality (i.e. increased sleep quality), supporting the notion that their paths are distinct. Lastly, the unexpected findings between SES and sleep change and alcohol use may indicate that there are additional mechanisms not explored in the present study that may explain this association. For example, past research demonstrates that job stress, specifically high job demand, is more frequently reported among individuals with higher SES (Kunz-Ebrecht et al., 2004) and that job demand is associated with worse sleep quality among full-time workers (Knudsen et al., 2007). The relationship between increased workload and burnout and sleep disruption seems to have persisted during COVID-19 (Costin et al., 2023). However, it is unclear whether the pandemic altered the relationship between SES and job demand. In sum, job-specific demands and workload might have contributed to the association between higher SES and decreased sleep quality.
Overall, our findings seem to confirm that SSS and SES tap into distinct constructs (Tan et al., 2020). Traditional measures of SES, such as income, education, and employment do not fully capture socioeconomic nuances that SSS evaluations may involve including perceptions of financial security, accumulated wealth, earning potential, an imminent retirement, or the prestige of an educational institution. The early months of the COVID-19 pandemic were marked by high economic uncertainty and altered daily routines. During this time, SSS may have additionally captured pandemic-related socioeconomic nuances such as the volatility of one’s financial or employment situation, change in expenses, or fear of unemployment. SSS assessments gage individuals’ perceptions of their status relative to others, which are informed by introspection and changes in context, including uncertainties regarding future identity (Destin et al., 2017). Therefore, it is plausible that the perceptions and social comparison involved in SSS better captured the nuances and fluctuations of financial and social contexts during COVID-19 (Cundiff and Matthews, 2017; Hoebel and Lampert, 2020). Regarding the reserve capacity model (Gallo and Matthews, 2003), the subjective evaluations and social comparison involved in SSS may be more closely related to negative affect and related cognitions compared to SES. This may partially explain why SSS, but not SES, was associated with psychological distress.
The present research sought to understand how the onset of the pandemic might influence general psychological distress, irrespective of pandemic-centric stressors (e.g. infection, shelter-in-place, adherence to COVID-19 guidelines). The hypotheses and analyses were contextualized for two relevant COVID-19 stressors experienced during the early months of the pandemic, worry about infection and shelter-in-place orders, in addition to controlling for other demographic variables. While the results of the present study occurred during the COVID-19 pandemic, these outcomes have also been observed in the context of other global stressors. For example, many of the features of the pandemic such as job and resource insecurity, economic hardship, and changes to daily routine are shared with the 2007–2009 Great Recession. In addition to similar characteristics, the impacts of these global stressors on individuals are also comparable. Research on health outcomes during the Great Recession consistently reports that symptoms of psychological distress increased in the US and Europe (Margerison-Zilko et al., 2016). Patterns of health behavior change were also coherent between COVID-19 and Great Recession literature with greater sleep issues (Margerison-Zilko et al., 2016) and decreased physical activity (Alam and Bose, 2023). However, evidence for alcohol use is mixed within both literatures with COVID-19 trending toward increased use and the recession trending toward decreased use (Roberts et al., 2021; Sane Schepisi et al., 2021). Finally, evidence suggests that those with fewer years of education and lower socioeconomic positions have a disproportionate risk of experiencing distress and adverse health outcomes resulting from both of these global stressors (Forbes and Krueger, 2019; Sane Schepisi et al., 2021). The present and existing work prompts the need for interventions to address distress during stressful global events, particularly among individuals experiencing financial insecurity.
Limitations and conclusions
The current study had many strengths, including theoretical integration and the simultaneous examination of SES and SSS. While the hypotheses and conceptual underpinnings had a robust theoretical foundation, limitations included the cross-sectional design and non-random recruitment method. This cross-sectional study cannot unambiguously address the directionality or causal chain of the observed associations. Psychological distress impacts health behaviors, but poor health behaviors can also have implications for distress. Further, while participants were diverse in age, race/ethnicity, and US state of residence, the generalizability of the present findings is limited due to the convenience sampling strategy. Another limitation stems from the single-item measurements of the outcome variables, an approach adopted to reduce survey fatigue. Additionally, it is possible that the self-reported nature of both SSS and the outcomes led to conflated and stronger associations (i.e. common method variance) as demonstrated previously between SSS and subjective well-being (Tan et al., 2020). Lastly, behavior change was measured using retrospective accounts. One limitation of this approach is its inability to measure true change and its susceptibility to recall biases (e.g. Gao and Scullin, 2020). Nevertheless, the perception of change offers valuable insight into the psychological impact of the pandemic and informs about participants’ perceptions of their physical well-being.
In conclusion, this study supports the possible intermediate role of psychological distress in linking lower SSS to poorer sleep quality and perceived decrease in physical activity during the initial stages of the COVID-19 pandemic in the US. These findings support SSS and SES as having non-overlapping relationships with health behaviors. Psychosocial and biological explanations have been provided for these independent relationships (Hoebel and Lampert, 2020); however, additional work is needed to empirically examine their underlying causal mechanisms. The present pre-registered study corroborates the reserve capacity model (Gallo and Matthews, 2003) and underscores the importance of addressing distress proneness as a means to mitigate the adverse effects on health behaviors. During global stressors characterized by economic, social, and health uncertainty, deploying electronically mediated professional psychological resources may serve as an effective strategy to mitigate these negative consequences among at-risk populations. Overall, these findings contribute to the growing scientific literature on socioeconomic health disparities during the pandemic and advocate for tailored interventions to address the disproportionate psychological and behavioral health tolls that occur during stressful global events.
Footnotes
Authors’ contributions
JRS: conceptualization, methodology, investigation, formal analyses, visualization, and writing the original draft. TB: conceptualization, methodology, formal analyses, writing – review and editing, and supervision. YJ: formal analyses and writing – review and editing. SZ: conceptualization, methodology, writing – review and editing, and supervision.
Data sharing statement
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ms. Rodriguez -Stanley’s work on this study was supported in part by the NIGMS/NIH grant R25 GM 058905–20.
Ethics approval
This study was approved by the Institutional Review Board at Wayne State University.
Informed consent
All participants provided consent prior to participation.