
Abstract
This study identified the control factors of inappropriate supplement intake to support public agencies in preventing health problems. We used an exploratory sequential mixed-method design with the integrated behavioral model (IBM). Control factors in the IBM were identified with 95 participants. The highest impact behavioral change was established for the following two out of 19 control factors: “I trust others’ blogs as a source of information when they post the bad as well as the good” (r = −0.324, p < 0.001) and “I can control any health problems by adjusting the amount and frequency of my supplement intake” (r = −0.308, p < 0.001). The findings suggest that when providing safety information on supplement use, it is important to: (1) disseminate information to online communities of supplement users who share knowledge based on real experiences and (2) effectively demonstrate the risks associated with continued supplementation.
Introduction
The use of dietary supplements has a long history, evolving from traditional herbal remedies used in ancient civilizations to modern use aimed at enhancing health. In recent years, the prevalence of supplement intake has increased worldwide, including in Japan. As of 2019, approximately 30%–40% of Japanese people use supplements (Ministry of Health Labour and Welfare, 2020b), which has remained relatively stable (Yano Research Institute, 2023). This trend reflects a broader global pattern, with the United States leading the supplement sector (Future Market Insights, 2024), where one-third–one-half of the population uses dietary supplements.
The global dietary supplement market has experienced significant growth in recent years. In 2023, the market was valued at approximately USD 176.89 billion and is projected to reach USD 348.27 billion by 2032 (Research and Markets, 2023). In Japan, the supplement market was valued at approximately 900 million yen in 2023, with an estimation of the growth to 950 million yen by 2028 (Yano Research Institute, 2023). This growth is partly driven by the post-COVID-19 increase in outdoor activities and a rising interest in supplements with potential beauty benefits (Tomar et al., 2023). As product choices in health and beauty become more diverse, supplements have become a key way to meet consumer needs.
However, the rise in dietary supplement use has also brought attention to several problematic categories, particularly in the United States. The issues have arisen around supplements for sexual enhancement, weight loss, and bodybuilding (Brown, 2017). Geller et al. (2015) reported that weight loss or energy products accounted for 71.8% of all supplement-related emergency department visits in the United States (Geller et al., 2015). The U.S. Food and Drug Administration (FDA) has issued multiple warnings about the dangers of weight loss supplements, particularly those containing sibutramine, which can significantly increase blood pressure and is not approved by the FDA (FDA, 2021). The global reach of the Internet has made it easy for Japanese people to purchase supplements from overseas, extending the issue of unsafe weight loss supplements to Japan. Adverse events were reported in Japan after foreign-manufactured weight loss jellies containing sibutramine were consumed in 2022 (Ministry of Health Labour and Welfare, 2022); the issue of the use of weight loss supplements is not limited to the United States. In addition to supplement-related adverse events based on quality issues, recent events in Japan have drawn attention to the safety of the ingredients themselves. Many health problems are caused by the intake of a supplement containing Pueraria mirifica used for weight loss or beauty. In June 2020, the Food Sanitation Law (Law No. 233 of 1947), was amended to the Law Partially Amending the Food Sanitation Law (Law No. 46 of 2008) (Ministry of Health Labour and Welfare, 2020a). Following this revision of the law, Pueraria mirifica was designated an “ingredient requiring special attention to prevent the occurrence of food sanitation problems, as designated by the Minister of Health, Labour and Welfare after hearing opinions from the Pharmaceutical Affairs and Food Sanitation Council.”
As health and beauty consciousness grows, providing consumers with accurate and relevant health information has become increasingly important. Given these global and local concerns, it is crucial for public health agencies to effectively disseminate health information to prevent supplement-related health problems. Despite existing warnings about the use of supplements, only 5.5% of supplement users made a decision to discontinue supplement use after being informed of the risks (Chiba, 2023). This highlights the need for targeted interventions aimed at the most vulnerable populations of supplement users.
This study aims to identify the factors influencing risk-taking behavior related to supplement use for weight loss or beauty, despite health risks. The clarification of these factors can develop more effective communication strategies to mitigate health problems caused by inappropriate supplement use.
Experimental methods
The current study’s theoretical framework is based on Fishbein and Ajzen’s integrated behavioral model (IBM) (Fishbein, 2008; Fishbein and Ajzen, 2009; Institute of Medicine US Committee on Communication for Behavior Change in the 21st Century, 2002), which originated in Fishbein’s (1967) theory of reasoned action (Fishbein, 1967) and Ajzen’s (1991) theory of planned behavior (Ajzen, 1991). IBM has three categories of control factors (attitude, perceived norms, and personal agency) that influence behavioral intentions (Supplemental Figure 1).
This study employed an exploratory sequential mixed-methods design. We conducted a preliminary qualitative survey to identify candidate control factors for each of the three IBM categories (attitudes, perceived norms, and personal agency) for risk-taking behavioral intentions. We then conducted an online quantitative survey to target risk-taking users and identify the factors controlling their risk-taking behavioral intentions.
Preliminary qualitative survey
Study sample and selection process
We contracted with a research company (MD, Inc.) in Japan to provide an online environment for screening participants and conducting a 30-minute interview survey. Since the recommended sample size in surveys based on interpretive phenomenology is six (Sandelowski, 2013), the target number of participants was set at six for each gender. Eligible participants were screened through an online presurvey of a large consumer panel provided by MD, Inc. The study sample consisted of 12 consumers in their 20–50s who were supplement users with diet/beauty goals. The principal investigator conducted the screening, explained the study to the participants, and obtained participant consent prior to the interview. The survey was conducted between July 9 and August 18, 2022.
Questionnaire
No personal information was obtained from participants during the interviews. The questionnaire elicited background information such as age, gender, education level, job, partner, health status, current status of supplement use, and control factors (attitudes, perceived norms, and personal agency) regarding the intake of supplements.
Analysis
In the interviews, we described the themes identified for each of the candidate control factors (attitudes, perceived norms, and personal agency). We also interpreted the narrative by paying attention to patterns, inconsistencies, and contradictions according to the hermeneutic phenomenological approach (Benner, 1994).
Main online quantitative survey
Study sample and selection process
For the main online quantitative survey, we contracted with another research company in Japan (NEO MARKETING, INC.) that provided a large consumer panel from which the eligible participants were initially recruited. Assuming a 50% response rate, a 10% tolerance interval, and a 95% confidence level, the required sample size was 96. After considering potential dropouts, the total number of participants was set to 100. Eligible Japanese participants aged 18–49 years were included after screening through an online pre-survey. The screening questions on the first page of the online survey, conducted from October 3 to October 4, 2022, referred to the following inclusion criteria: (1) Do you currently use supplements for weight loss or beauty? (Yes) (2) Have you ever had health problems after taking supplements? (Yes). A description of the study objectives and design was provided on the survey webpage to facilitate the participants’ understanding. Completing the survey was regarded as providing voluntary consent based on the ethical standards guidelines published in Japan.
Questionnaire
The questionnaire items elicited background information including age, gender, education level, status (medical/nutritional specialist or non-specialist), prescribed drug use (yes/no), and history and current status of supplement use. Additionally, certain items required participants to rate candidate control factors based on the preliminary qualitative survey on a scale of 1–5 (1 = totally disagree to 5 = fully agree). The survey also included the following question: “Are there health problems addressed by the safety information that make you want to discontinue supplement use?” (yes/no).
Main outcome of the study
The main outcome of this study was the estimation of behavioral intentions using the Hornik score (Hornik et al., 2018; Hornik and Woolf, 1999).
Analysis
We analyzed eligible Japanese participants with no missing data and summarized their background data. Frequencies and proportions were calculated for categorical variables for each questionnaire item, and summary statistics were calculated for continuous variables.
The estimated effects were calculated for each candidate control factor. The correlation between risk-taking behavioral intentions and candidate control factors was analyzed using Spearman’s rank correlation coefficient.
The Hornik score is the estimation effect calculated by examining differences in the percentage of those participants who “did not intend to discontinue supplement use in any situation” and those who responded “somewhat agree” or “fully agree” for each of the candidate control factors clarified in the preliminary qualitative study.
All statistical analyses were performed using EZR software, which is a modified version of R Commander that adds statistical functions frequently used in biostatistics. Statistical significance was indicated by p-values <0.05 (two-sided).
Informed consent
The principal investigator screened the participants, explained the study to them, and obtained their consent before the preliminary qualitative survey interviews. A description of the study design and objectives was provided on the survey webpage to facilitate participants’ understanding of the main survey. Completion of the survey was regarded as voluntary consent based on the ethical standards guidelines published in Japan.
Ethics statement
The preliminary qualitative survey was approved on June 21, 2022 (no. 250), and the main survey was approved on September 2, 2022 (no. 409), by the Ethics Committee. The surveys were conducted in accordance with the 1964 Declaration of Helsinki and its subsequent amendments.
Results
Preliminary qualitative survey
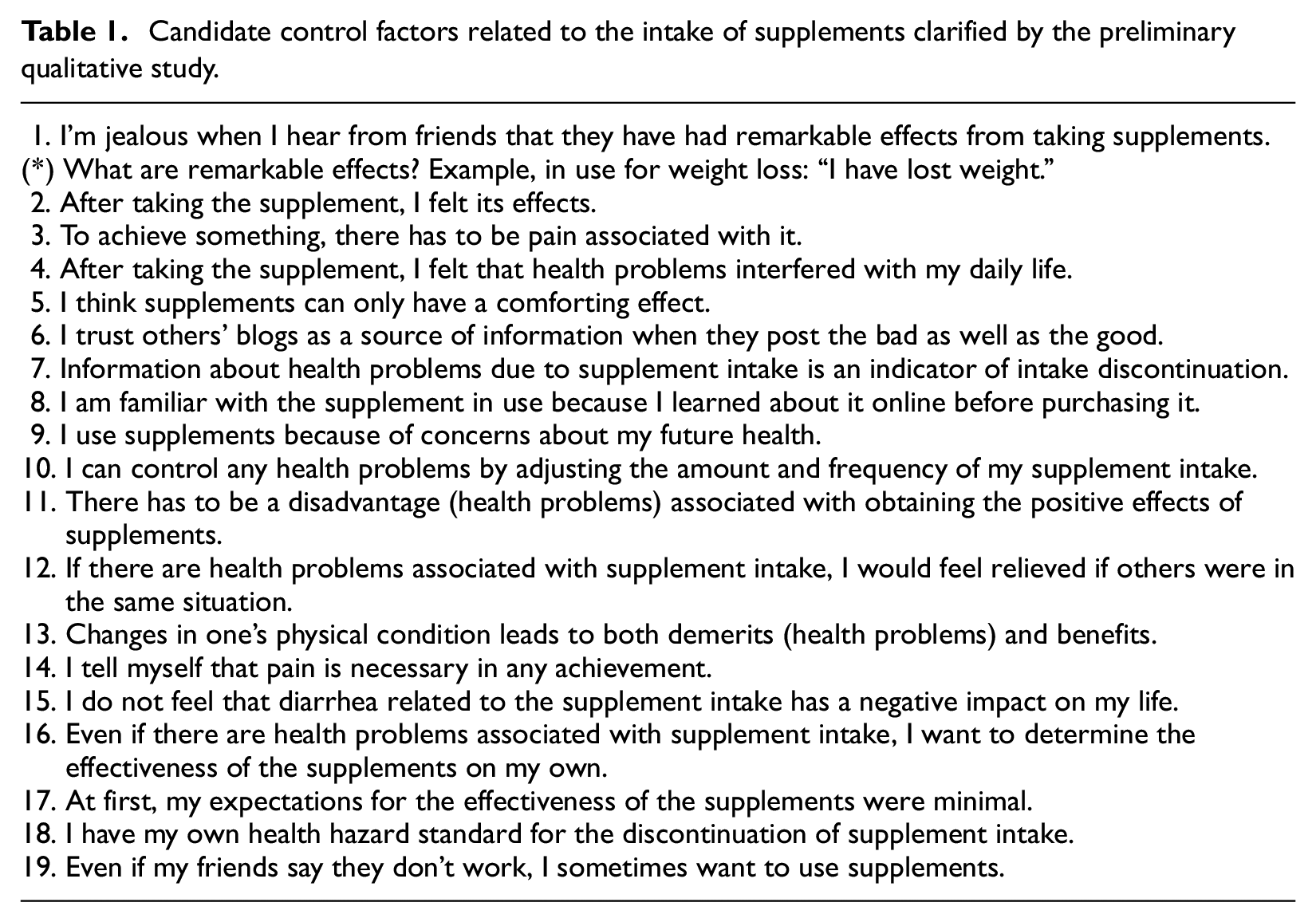
An eligible male participant in his 20s could not be found during the limited study period; therefore, the total number of participants was 11 (Supplemental Table 1). All the participants had higher education levels, and four were continuously taking supplements. All the participants were healthy and had partners. After conducting the qualitative content analysis, we described 19 candidate control factors of risk-taking behavioral intentions: six in relation to attitudes (items 2, 4–6, 8, and 17), four in relation to perceived norms (items 1, 9, 12, and 19), and nine related to personal agency (items 3, 7, 10–11, 13–16, and 18) (Table 1).
Candidate control factors related to the intake of supplements clarified by the preliminary qualitative study.
Main online quantitative survey
A total of 100 participants (50 men and 50 women) responded to the survey, using age and gender as allocation factors. After the completion of the survey, five participants who did not meet the eligibility criteria were excluded, resulting in a total sample of 95 participants (49 men and 46 women) (Table 2). The mean age of the participants was 37.8 years; 85.3% had at least a junior college education, and 46.3% were in the category of “heaviest users” of supplements, with a history of at least 1 year of usage. Additionally, 41.4% reported their supplement use to doctors, and 69.5% of participants used multiple supplements.
Characteristics of the study sample in the main online quantitative survey.
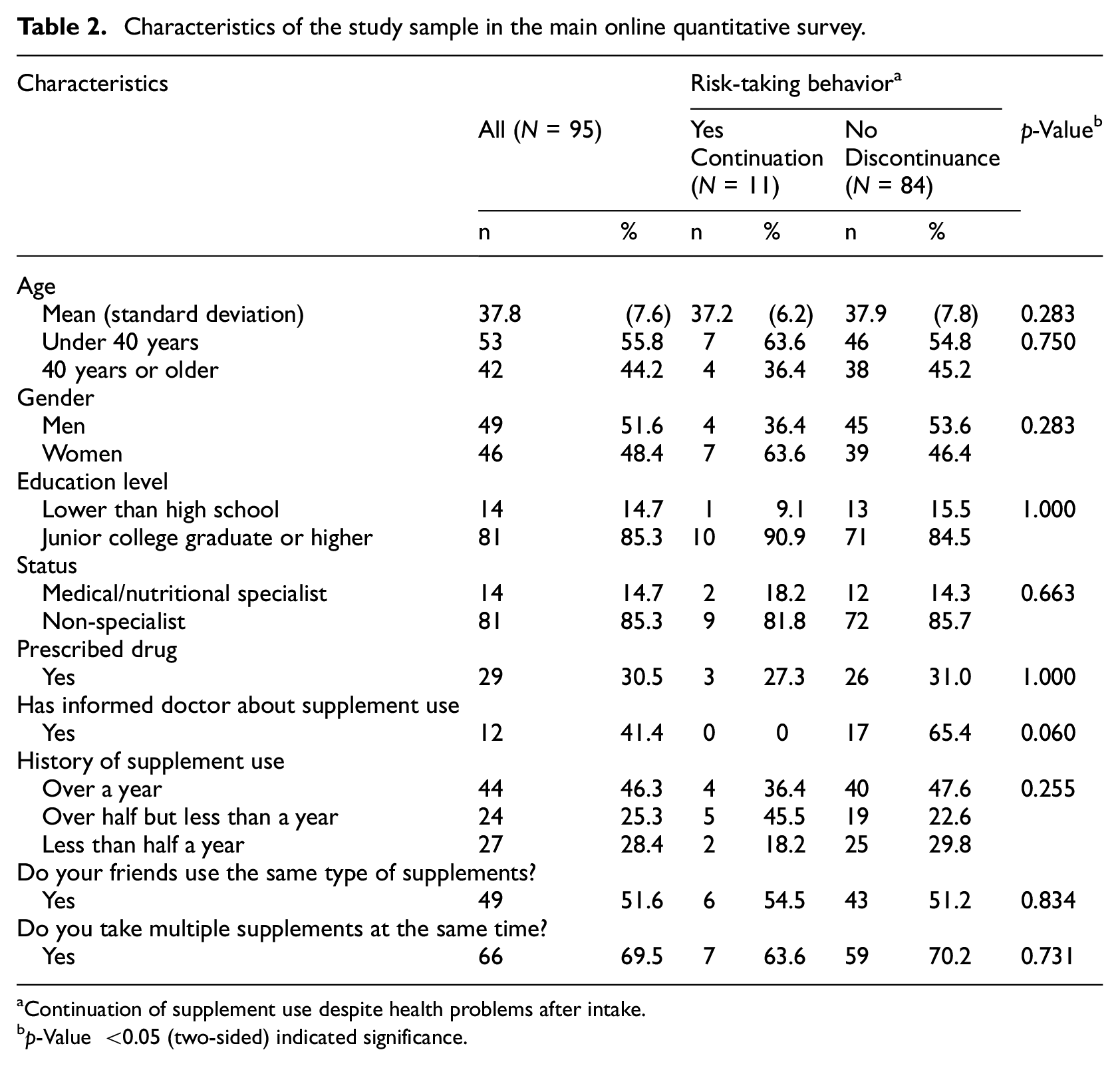
Continuation of supplement use despite health problems after intake.
p-Value <0.05 (two-sided) indicated significance.
Characteristics of eligible Japanese participants
Eleven of the 95 (11.6%) risk-taking users would continue supplementation regardless of health problems. After stratifying the sample by intake continuity, the mean age of the participants who would continue supplement use under any circumstances was 37.2 years; 63.6% were under 40 years of age, 63.6% were women, 90.9% had at least a junior college education, and 45.5% were moderate supplement users, with an intake history of at least 6 months but less than 1 year, so they likely possessed sufficient relevant information about the supplements used. None of them had informed their doctors about their self-administration of the supplements. Furthermore, 63.6% of the participants used multiple supplements (Table 2).
Control factors of risk-taking intentions
In terms of deciding to discontinue intake, the most relevant control factors found were factors 6 (“I trust others’ blogs as a source of information when they post the bad as well as the good”) (r = −0.324, p < 0.001) and 10 (“I can control any health problems by adjusting the amount and frequency of my supplement intake”) (r = −0.308, p < 0.001), with the lowest Hornik score of 9.6% (Supplemental Table 2).
Future high impact of behavior change predicted by control factors among risk-taking users
We found that 11.6% of the participants continued to take inappropriate supplements in spite of the normal health message alerts. When analyzing control factors 6 and 10, we predicted a decrease in the number of participants who inappropriately used supplements by 9.6% based on the Hornik score (Figure 1).
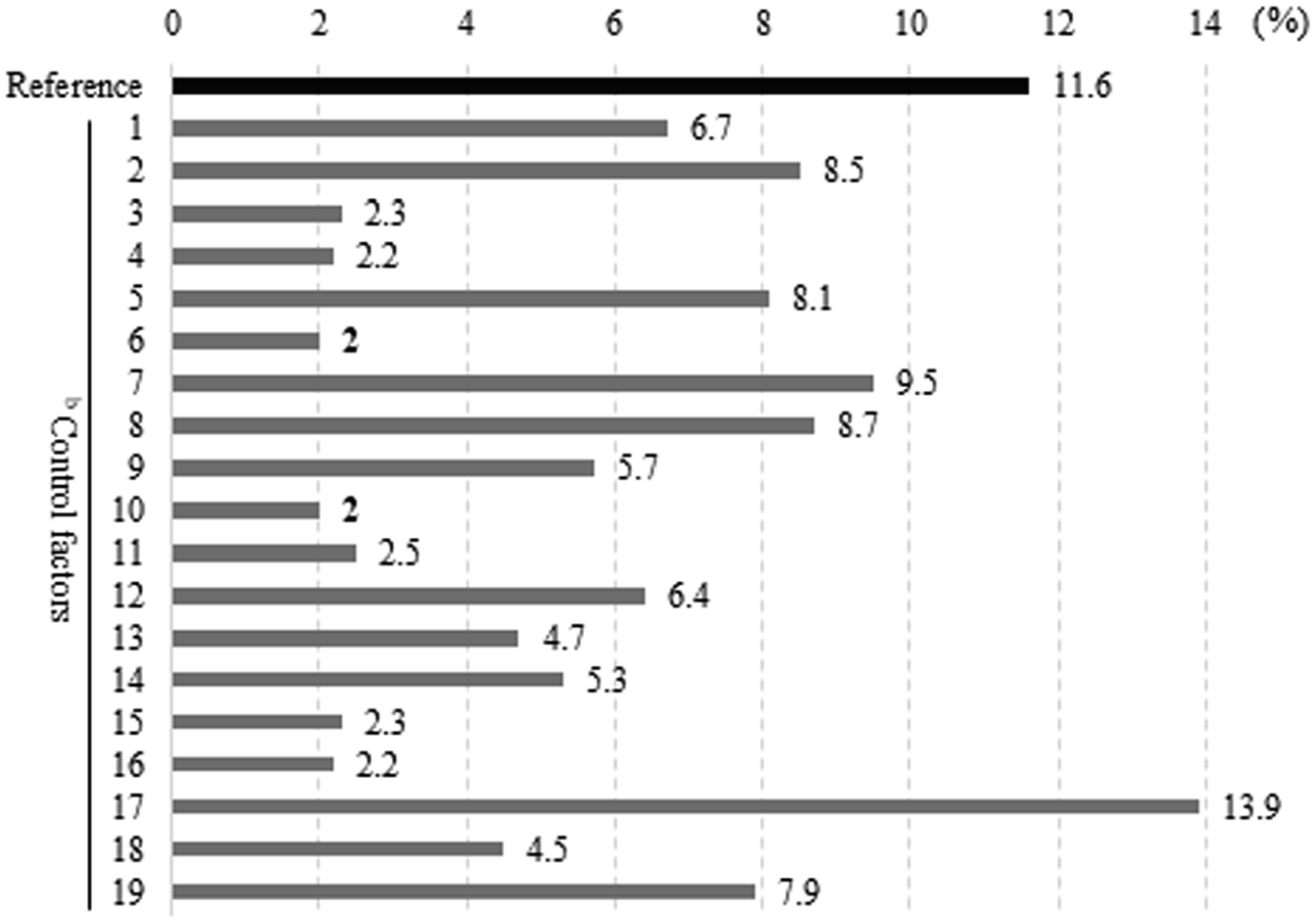
Behavioral change effects by control factors.
Discussion
Control factors of inappropriate supplement intake
Effective presentation of relevant risks to the target population
Of the three control factor categories, personal agency was identified as having a high degree of control over noncompliant behavior. This was expressed by the sentiment that “I can control any health problems by adjusting the amount and frequency of supplement intake.” The consideration of this factor showed that the percentage of those who were unable to appropriately discontinue supplement intake decreased from 11.6% to 2.0% (−9.6%) when health problems occurred.
This factor explains the discrepancy between knowledge and action, whereby people choose noncompliant behavior even when they have acquired the appropriate knowledge (Tanaka et al., 2019). This suggests an underestimation of the impact of the possible undesirable consequences of choosing noncompliant behaviors, which may be due to low risk perception.
Health problems associated with the intake of supplements are often characterized by minor symptoms such as diarrhea (Umegaki, 2015). As a public health measure, the supply of information alone does not necessarily lead to a reduction in risky behaviors, as the provision of risk-related knowledge through mass communication does not influence low-risk behaviors (Cook and Bellis, 2001). Brown (2005) also pointed out that a longer period of practicing risk-taking behaviors decreases risk perception (Brown, 2005). This may reflect the possibility that when the risked loss is small, the psychological impact of incurring it is also small (Harinck et al., 2007), and people may choose to ignore the risk, thinking, “If the damage is small, I don’t care if I suffer a loss.” In short, because greater knowledge increases the sense of control over one’s behavior, one may underestimate the impact of the undesirable consequences associated with noncompliant behaviors. Similarly, prolonged supplement use and acquired knowledge may lead to a low risk perception. Therefore, it is necessary to take measures to effectively present relevant risks to the target population.
Online communities’ provision of information to consumers
As a control factor, attitude was identified as collective decision-making in consumption, expressed as “I trust others’ blogs as a source of information when they post the bad as well as the good.” Varying this factor showed that the percentage of those who were not able to appropriately discontinue supplement intake decreased from 11.6% to 2% (−9.6%) when health problems occurred.
Two considerations are important in relation to this control factor: (1) other people’s blogs are a source of information and (2) the posts include both bad and good information. This raises two points. First, word-of-mouth is an important factor that influences purchasing decisions. Consumers are said to have skeptical attitudes toward sellers because they only provide positive information. By contrast, word-of-mouth information includes facts provided by other consumers who are independent of the seller. Consumers use word-of-mouth as a source of information because it is provided by people who have used the product (Rosen, 2000). Additionally, online communities are places where people gather to provide and filter information suitable for consumers. The existence of such communities is thought to play an important role in decision-making (Miyata, 2006).
Study limitations
This study had three limitations. First, the sample size was small, so the distribution of the Japanese population was not representative. However, we believe that the validity of our survey results was ensured because it was based on sample size calculations prior to the start of the survey. Second, the study results may have been influenced by the fact that the sample of participants had a high education level. However, dietary supplement users tend to have higher education levels and incomes than do non-users (Dickinson and MacKay, 2014). Finally, because the control factors were limited to the target population and supplements can be purchased over the Internet, we believe that the impact of regional bias is small. Thus, because of the differences in control factors related to other consumption safety topics such as tobacco, behavioral analysis is important depending on the social problems to be solved in the target population to ensure effective health communication.
Conclusion
The control factors for risk-taking intentions in this study were attitude and personal agency. In the future, health communication strategies should be based on these control factors to prevent health problems caused by the inappropriate intake of supplements. When providing safety information to risk-taking users, it is important to effectively demonstrate the risk of continuing inappropriate supplement intake with online communities of users.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241296648 – Supplemental material for Key factors for inappropriate supplement intake in risk-taking users: An exploratory sequential mixed-methods pilot study in Japan
Supplemental material, sj-docx-1-hpq-10.1177_13591053241296648 for Key factors for inappropriate supplement intake in risk-taking users: An exploratory sequential mixed-methods pilot study in Japan by Nanae Tanemura in Journal of Health Psychology
Footnotes
Acknowledgements
We are grateful to Editage for providing English language editing of our manuscript.
Author contributions
NT was involved in the study design and data interpretation. NT conducted the data analysis and critically revised the report, commented on drafts of the manuscript, and approved the final report.
Data sharing statement
All relevant data are presented in the paper and supporting information files.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Health and Labour Sciences Research Grant (21KA2002) from the Ministry of Health, Labour and Welfare.
Ethics approval
The preliminary qualitative survey was approved on June 21, 2022 (no. 250) and the main survey was approved on September 2, 2022 (no. 409) by the Ethics Committee of National Institutes of Biomedical Innovation, Health and Nutrition. The surveys were conducted in accordance with the 1964 Declaration of Helsinki and its subsequent amendments.
Informed consent
(1) Preliminary qualitative survey: The principal investigator conducted the screening, explained the study to the participants, and obtained participant consent prior to the interview. (2) Main online quantitative survey: A description of the study objectives and design was provided on the survey webpage to facilitate the participants’ understanding. Completing the survey was regarded as providing voluntary consent based on the ethical standards guidelines published in Japan.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.