
Abstract
Spiritual wellbeing correlates with improved pain perception. We hypothesize that pain catastrophizing, which correlates with worsened pain, partially explains this relationship. In this cross-sectional, human laboratory-based study, 120 US Americans with chronic pain completed self-report measures of spiritual wellbeing, pain catastrophizing, and their subconstructs. A cold pressor task measured pain perception (i.e. pain sensitivity and pain tolerance). Multiple regressions evaluated the relationship between spiritual wellbeing (and its subconstructs) and pain perception with and without the inclusion of pain catastrophizing (and its subconstructs). No direct relationships were found between spiritual wellbeing or its subconstructs and pain sensitivity, although helplessness significantly altered regression coefficients. Spiritual wellbeing, meaning, and peace associated less strongly with pain tolerance controlling for pain catastrophizing, helplessness, and (for peace) magnification. This shows that many of the links between spiritual wellbeing and pain perception are indirect, through pain catastrophizing and especially helplessness.
Introduction
Chronic pain
Chronic pain, pain lasting three or more consecutive months (Treede et al., 2015) impacts 51.6 million US Americans (Rikard et al., 2023) and costs $560–$636 billion annually (Gaskin and Richard, 2012). Individuals with chronic pain report interference to mood (Craig et al., 2013), employment (Breivik et al., 2006), physical functioning (Wilson and Palermo, 2012), cognitive functioning (Higgins et al., 2018), energy (Craig et al., 2013), relationships (Ojega et al., 2014), and quality of life (Hadi et al., 2019; Husky et al., 2018). Furthermore, 6.9% of US citizens report substantially restricted functioning due to chronic pain (Rikard et al., 2023).
In addition to the physical processes of pain sensations, some variance in pain perception results from biopsychosocial-spiritual factors and behaviors (Edwards et al., 2016). Cognitive and emotional factors that underlie chronic pain such as pain catastrophizing have been examined repeatedly. Despite their importance in the biopsychosocial-spiritual model, spiritual factors, however, are frequently overlooked. The combination of these factors within this study therefore offers a more holistic evaluation of pain etiology.
Spiritual wellbeing
Spiritual wellbeing is defined as “the degree to which [one’s] spirituality can help them make sense of their lives and feel whole, hopeful and peaceful even in the midst of a serious illness” (Lewis et al., 2014). Often this includes three subconstructs: peace, a sense of tranquility; meaning, a perception of purpose; and faith, a feeling of strength in connectedness to one’s beliefs (Haugan, 2015; Peterman et al., 2002).
Spirituality, which is closely connected to spiritual wellbeing, negatively correlates with pain intensity (Ferreira-Valente et al., 2019; Siddall et al., 2017). Spirituality also negatively relates to pain’s interference on activities, socialization, and life enjoyment (Bai et al., 2018; Ferreira-Valente et al., 2019). Research also supports spiritual meditation as more beneficial for pain tolerance than secular meditation (Wachholtz and Pargament, 2008).
Spiritual wellbeing is linked with moderate to large increases in quality of life in pain populations (Ferreira-Valente et al., 2019), which is negatively correlated with pain intensity and interference (Bai et al., 2018). Spirituality is associated with greater pain self-efficacy (Wachholtz and Pargament, 2008) and increased use of positive pain coping skills including task persistence, positive self-statements, and ignoring pain (Ferreira-Valente et al., 2020). Additionally, spiritual wellbeing is negatively associated with distress, fatigue, depression, and anxiety (Kandasamy et al., 2011).
One way to conceptualize the impact of spiritual wellbeing on pain and pain-related constructs is through Gray’s Reinforcement Sensitivity Theory which posits that one’s interactions are influenced primarily by the behavioral activation system (BAS), which rewards approach and action, and the behavioral inhibition system (BIS), which punishes behavior and encourages avoidance (Gray, 1990). Spiritual wellbeing functions in line with the BAS as it appears to encourage the use of several positive coping strategies. Inversely, pain catastrophizing has been positively linked to elevated BIS sensitivity in tests and may lead to avoidance behaviors and inactivity in response to pain (Sánchez-Rodríguez et al., 2020). This is another reason why pain catastrophizing is of particular interest in this study—it provides a more holistic examination of how different systems combine to shape the chronic pain experience.
Pain catastrophizing
Pain catastrophizing refers to the negative thoughts and beliefs resulting from the experience or anticipation of pain (Quartana et al., 2009). Like spiritual wellbeing, this construct is typically comprised of three subdomains: magnification, an exaggeration of pain consequences; rumination, a focus on pain; and helplessness, a perception of pain as unstoppable (Sullivan et al., 1995). In chronic pain populations, pain catastrophizing is associated with depression, anxiety, anger (Hirsh et al., 2007), and fear of pain (Sullivan et al., 2004). Pain catastrophizing is associated with greater pain interference and disability as well as increased illness behaviors including repeated healthcare visits (Sullivan et al., 2001). This link between pain catastrophizing and disability is significant controlling for disease and pain severity, depression, anxiety, and neuroticism (Sullivan et al., 2001).
Pain catastrophizing also appears to impact pain perception directly. High pain catastrophizing prior to surgery, for example, is associated with more intense post-surgery pain (Pavlin et al., 2005), longer recovery times (Kendell et al., 2001), and less treatment satisfaction (Kendell et al., 2001). In the chronic pain population, pain catastrophizing is significantly correlated with higher pain intensity as well (Sullivan et al., 2004). In fact, when studying various psychological responses to pain, Sorbi et al. (2006) found pain catastrophizing to be the largest predictor of pain intensity.
There is evidence of directionality in this relationship as well. Elevated pain catastrophizing scores in early-to-mid portions of studies predict elevated pain intensity in the mid-to-late portions, but not vice versa (Campbell et al., 2010). In interventions that focus on reducing pain catastrophizing, researchers have found that decreased pain intensity, disability, and negative affect are likely to persist at least 6–12 months following pain catastrophizing treatment completion (Jensen et al., 2001).
Three-step model of pain perception and the current study
Explicit links have been found between spiritual wellbeing and pain catastrophizing. Increased spiritual distress correlates with greater pain catastrophizing (Ferreira-Valente et al., 2019). Pain catastrophizing also appears to mediate the relationship between spiritual wellbeing and depression (Shaygan and Shayegan, 2019).
Theoretical pathways proposed by Wachholtz et al. (2007) to explain spirituality’s impact on pain perception also parallel the domains of pain catastrophizing. The first three of these pathways relate to appraisals of pain as something with which one can cope, increased feelings of pain self-efficacy, and the use of spiritual or religious techniques as distraction. These pathways largely represent the inverse of magnification, helplessness, and rumination, respectively. As such, spiritual wellbeing and pain catastrophizing may be incompatible.
Despite the established interrelation between spiritual wellbeing and pain catastrophizing, there is a dearth of studies analyzing spiritual wellbeing, pain catastrophizing, and pain perception altogether. As many pain management programs have begun targeting spiritual wellbeing (Steinhorn et al., 2017) and pain catastrophizing (Jensen et al., 2001) as mechanisms of treatment, it is especially important to understand how these factors jointly impact the perception of pain. This understanding may inform the focus of treatment, how treatments are presented, or even which components of spiritual wellbeing or pain catastrophizing should be measured.
Better understanding how protective factors such as spiritual wellbeing relate to pain through reactions such as pain catastrophizing may also help improve understanding of the methods of action underlying individual differences in pain perception (Dezutter et al., 2015). This improves the comprehensive understanding of individuals with chronic pain necessary for both research and treatment of pain.
Two specific measures of pain perception—pain sensitivity and pain tolerance—were selected for the current study due to their respective natures as primary and secondary appraisals as relevant to the Lazarus Folkman transactional model of stress and coping (1984). According to this model, one’s evaluation of stressors depends on primary appraisals of the severity of threats and secondary appraisals of one’s abilities to cope with said threats (Lazarus and Folkman, 1984). Pain is commonly conceptualized as a threat signal (Dysvik et al., 2005). Through this model then, pain sensitivity—the threshold of a stimulus necessary to elicit pain—can be considered to operate based on primary appraisals of a stimuli as painful (i.e. threatening). Pain tolerance—the quantity of acute pain one feels they can tolerate—also involves appraisals of stimuli as painful and adds a secondary appraisal of one’s ability to withstand the pain.
The current study’s purpose, therefore, is to evaluate the ways spiritual wellbeing and pain catastrophizing together may relate to one’s perception of pain and their perceived ability to cope as exemplified through pain sensitivity and tolerance.
Hypotheses
We hypothesize that:
Pain catastrophizing partially explains the relationships between spiritual wellbeing and both measures of pain perception (i.e. pain sensitivity and pain tolerance) as measured through a significant reduction in the strength of the correlation between spiritual wellbeing and pain perception when pain catastrophizing is added to the analysis. Specifically, we propose that high spiritual wellbeing is associated with low pain sensitivity and high pain tolerance and that a portion of this relationship is explained by pain catastrophizing.
The subconstructs of pain catastrophizing (i.e. magnification, rumination, and helplessness) partially explain the relationship between the subconstructs of spiritual wellbeing (i.e. peace, meaning, and faith) and measures of pain perception (i.e. pain sensitivity and pain tolerance) as measured through a reduction in the strength of the correlation between spiritual wellbeing’s subconstructs and the measures of pain perception when pain catastrophizing or its subconstructs are added to the model.
Method
Procedures
The current project is a secondary data analysis of a distinct human laboratory-based study conducted by Amy Wachholtz, PhD, MDiv, MS and colleagues. Recruitment targeted adults with chronic pain in the New England area. The original study examined differences between participants with various opioid use histories including some (i.e. half) currently undergoing opioid replacement therapy for opioid use disorder, so recruitment was conducted at addiction treatment clinics as well as through public advertisements. Opioid histories were not examined in the current study; instead, these groups were collapsed to represent the diverse experiences of individuals with chronic pain. Inclusion criteria included current pain lasting six or more consecutive months and age between 18 and 65. Exclusion criteria included psychosis, suicidal ideation, current hospitalization, and conditions or substance use that may impact pain perception.
After passing a screener to determine eligibility and providing informed, written consent, participants underwent a 12-panel urine drug screening to verify abstinence from substances. They then completed self-report measures related to pain, spiritual wellbeing, and pain catastrophizing. The cold-pressor task, an established means of safely evaluating pain sensitivity and tolerance through simulating acute pain or pain flares, was then used to assess pain perception. Participants were instructed to inform researchers when they experienced pain (pain sensitivity) and when that pain became unbearable (pain tolerance).
In total, the study lasted approximately 1 hour, for which participants were compensated $20. All procedures were approved as ethical by the IRB of a large academic medical institute. This manuscript contains no information that can be linked to any specific, individual participant.
Participants
Participants included 120 adults with chronic, non-malignant pain. The mean participant age was approximately 42.0 years (SD = 11.44). Participants self-identified predominantly as female (60.8%), White (85.8%), and non-Hispanic (82.5%). Participants identified with various religious orientations, and catholic participants represented the largest religious group within the sample (47.1%).
Musculoskeletal pain was reported by 100% of participants with 20% also endorsing neuropathic pain. A total of 90 patients reported a history of opioid dependence, while the remaining 30 were opioid naïve, which was defined as having taken opioids for less than 2 weeks cumulatively across their lifespan. A flowchart of participant enrollment is illustrated in Figure 1. A full list of patient demographic factors is detailed in Table 1.
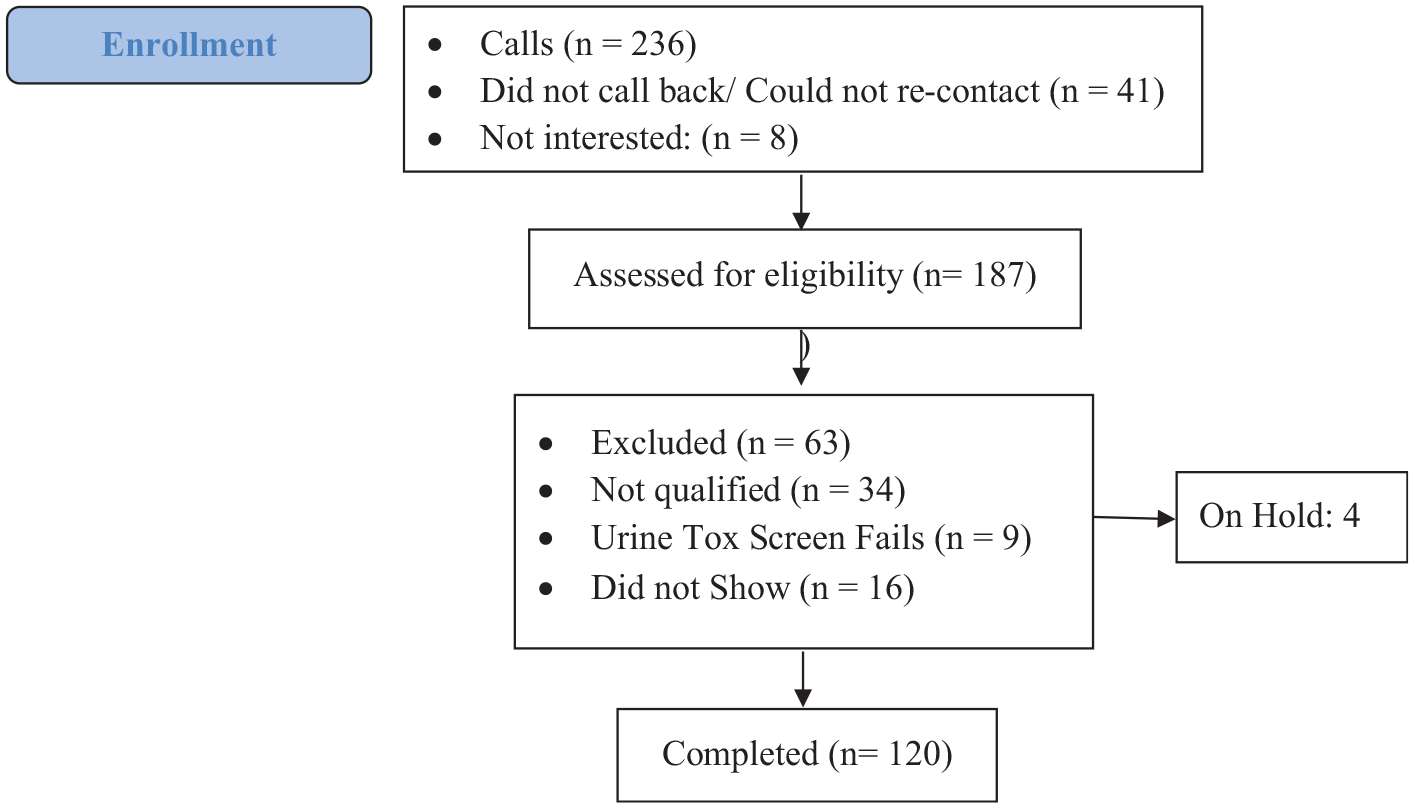
STROBE flow diagram.a
Participant demographic characteristics. a
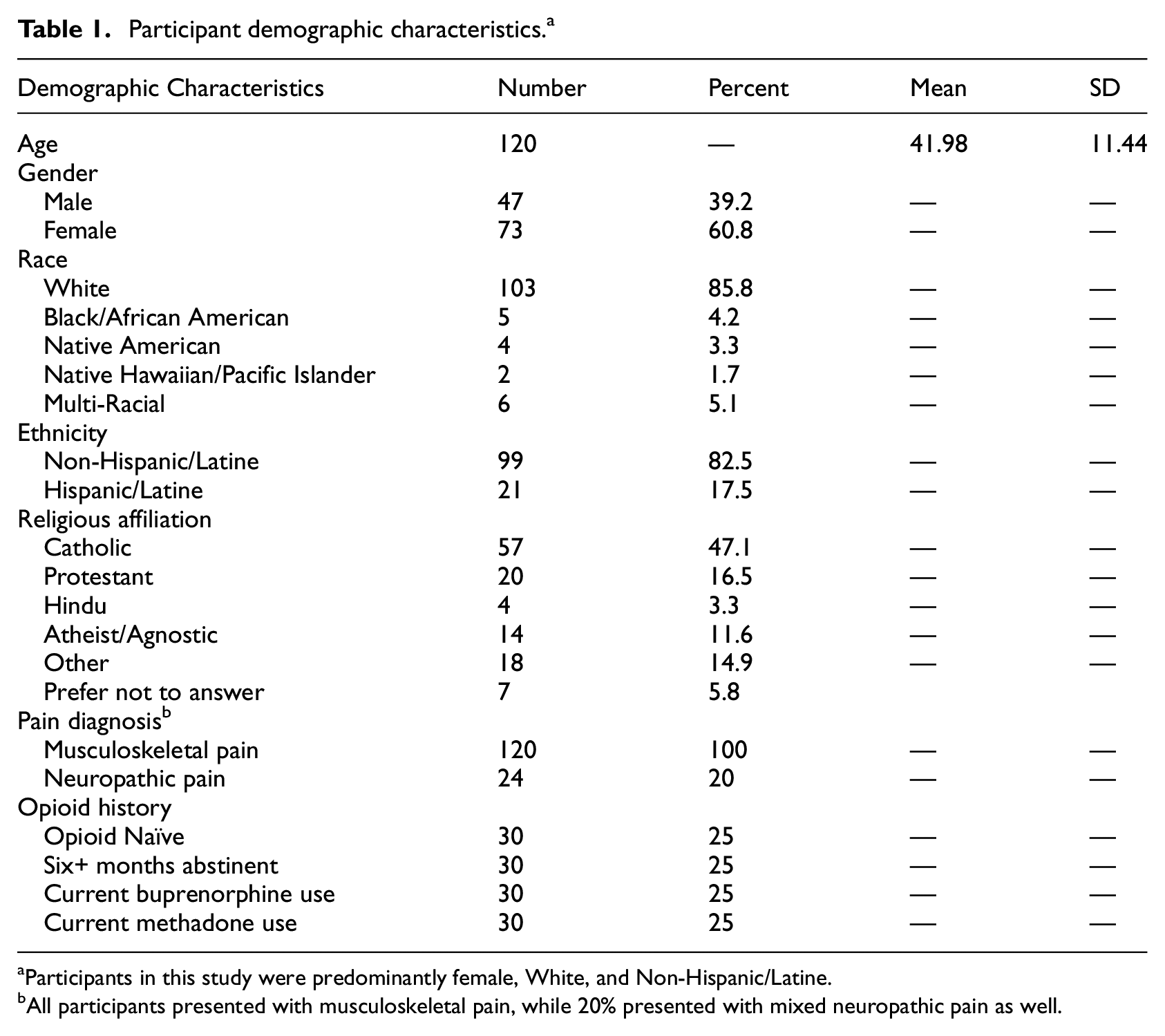
Participants in this study were predominantly female, White, and Non-Hispanic/Latine.
All participants presented with musculoskeletal pain, while 20% presented with mixed neuropathic pain as well.
Measures
Spiritual wellbeing
Spiritual wellbeing was assessed using the Functional Assessment of Chronic Illness Therapy-Spiritual Well-being (FACIT-Sp) scale (Peterman et al., 2002). This 12-item self-report measure of respondents’ perceived feelings of tranquility (i.e. peace), purpose in life (i.e. meaning), and strength from their spiritual beliefs (i.e. faith). Items relating to each include “I feel peaceful,” “I have a reason for living,” and “I find comfort in my faith or spiritual beliefs” respectively (Peterman et al., 2002). Factor analyses confirmed a three-factor model containing peace, meaning, and faith (Haugan, 2015). Each item is scored from 0 to 4 for a total score range from 0 to 48, with higher scores representing greater spiritual wellbeing.
In previous research, the aggregate FACIT-Sp score displayed appropriate convergent and divergent validity and adequate internal consistency (Cronbach’s α= 0.76; Haugan, 2015). Within this study, the FACIT-Sp displayed appropriate internal consistency as demonstrated by Cronbach’s alpha (α= 0.750). Total scores ranged from 1 to 44 (M = 6.93, SD = 7.69).
Pain catastrophizing
Pain catastrophizing was measured by the Pain Catastrophizing Scale (PCS; Sullivan et al., 1995). This 13-item self-report measure examines common beliefs and cognitions that occur in response to pain including overemphasizing the impacts of pain (i.e. magnification), perseverating over pain (i.e. rumination), and feeling there is no way to combat pain (i.e. helplessness; Sullivan et al., 1995). Items related to each of these subconstructs include, “I become afraid the pain will get worse,” “I keep thinking of how much it hurts,” and “I feel I can’t go on” respectively (Sullivan et al., 1995). Factor analysis confirmed a three-factor model of magnification, rumination, and helplessness (Osman et al., 1997). Each item is scored from 0 to 4 for a total score range from 0 to 52, with higher scores representing worse pain catastrophizing.
The PCS has shown appropriate construct, convergent, divergent, and criteria validity (Osman et al., 1997). Within this study, the PCS was shown to have appropriate internal consistency (Cronbach’s α= 0.947). PCS scores within this study ranged from 0 to 50 (M = 22.59, SD = 13.38).
Pain perception
Acute pain was induced using a cold pressor task in which participants were asked to submerge their dominant hand up to the wrist in cold water (2°C). The cold pressor task permits the objective observation of several aspects of subjective pain perception including pain sensitivity and pain tolerance. In this study, pain sensitivity was defined as the time (in seconds) between when participants submerged their hand to when they first endorsed feeling pain. Greater pain sensitivity was operationalized as a shorter time to pain report. Pain tolerance was measured as the amount of time (in seconds) each participant kept their hand submerged until they determined that the pain was too intense to endure further. Greater pain tolerance was operationalized as a longer time with one’s hand submerged. Participants who reached 300 seconds were instructed to remove their hands as a safety precaution.
The cold pressor task is well established throughout the literature and has high test-retest reliability (Koenig et al., 2014). Within this study, submersion time until reporting pain (i.e. pain sensitivity) ranged from 0 to 295 seconds (M = 31.26, SD = 37.35), and submersion time until hand was removed (i.e. pain tolerance) ranged from 15 to 300 seconds (M = 76.69, SD = 76.08).
Data analysis
We used linear regression analyses to evaluate the relationship between spiritual wellbeing and pain perception with no other variables included in the model. These results were then compared to the results of a multiple regression analysis which regarded the relationship between spiritual wellbeing and pain perception controlling for the effect of pain catastrophizing. A significantly smaller regression coefficient in the complex model (as determined by bootstrapping analyses with 95% confidence intervals) would denote that a significant portion of the relationship between spiritual wellbeing and these measures of pain perception was explained by pain catastrophizing. These processes were then repeated for subconstructs of spiritual wellbeing and pain catastrophizing.
For ease of reading, the relationship between spiritual wellbeing and pain perception with no other included variables in the analysis will hence be referred to as the “simple relationship” and the relationship between spiritual wellbeing and pain perception controlling for the impact of pain catastrophizing will be referred to as the “controlled relationship.”
Statistical power
Statistical power analyses were conducted through G-Power, with the statistical power level set to 0.80 and the significance level set to α= 0.05 as align with standard practice (Mazen et al., 1987). Results of these analyses indicate that with 120 participants, analyses had 80% power to detect relationships with an effect size of f2 = 0.08 or greater. The current sample of 120 participants should, therefore, ensure that analyses were adequately powered to detect able to detect medium effects (f2 = 0.15–0.34) and even most small effects (f2 = 0.02–0.14; Chuan and Penyelidikan, 2006).
No studies were identified which evaluate spiritual wellbeing, pain catastrophizing, and acute pain perception directly. However, previous studies have found spiritual wellbeing and its subconstructs to display moderate-strength correlations with pain intensity (r2 =−0.10 to 0.21; Siddall et al., 2017) and mostly moderate to strong correlations with pain interference (r2 =−0.04 to 0.29; Bai et al., 2018). Pain catastrophizing also exhibits a moderate correlation with pain intensity (β= 0.37; Sorbi et al., 2006), and mediation studies have found pain catastrophizing to mediate the links between positive traits similar to spiritual wellbeing (i.e. hope and optimism) and pain perception at predominantly moderate strengths (total effects = r2 =−0.05 to 0.14; direct total effects = r2 =−0.03 to 0.13; Pulvers and Hood, 2013). Although some of these ranges dip into the “small” effect range at their lower ends, these are less frequent and still within the level supported by current power analyses (Pulvers and Hood, 2013). Based on this literature, a sample size of 120 participants was therefore deemed to be adequate to measure the expected effects.
Results
Statistical analyses assumptions
Current data met all standard assumptions of linear analyses. Visual evaluation of simple linear regressions confirmed linearity in relationships between each set of variables, and visual inspection of histograms confirmed normality. Homoscedasticity was confirmed through visual analysis of plotted residuals. Independence of participants was established through research procedures as participants were collected independently across several locations and data were collected cross-sectionally at one time-point. Finally, multicollinearity was affirmed as no variables shared in any multiple regression analyses exhibited VIF values of greater than 1.1 which is well below the established cutoff of 10 used in multicollinearity analyses across the literature (Thompson et al., 2017). No missing data were identified.
Initial correlation analyses
Bivariate correlation analyses did not support faith as associated with pain catastrophizing or any of its subconstructs, so it was removed from further analyses. Likewise, magnification was not correlated with spiritual wellbeing, meaning, or pain sensitivity. Therefore, it was only included as a variable in the multiple regression analysis of the relationship between peace and pain tolerance.
Models testing construct-level simple and controlled relationships
At the α= 0.05 level, the simple relationship (β = 0.30, p = 0.50) and controlled relationship (β = 0.09, p = 0.84) between spiritual wellbeing and pain sensitivity were not significant. The reduction in effect size between these relationships was also nonsignificant (β =−0.20, 95% CI =−0.63 to 0.00).
Neither the simple relationship (β = 1.11, p = 0.22) nor the controlled relationship (β = 0.60, p = 0.50) between spiritual wellbeing and pain tolerance were significant. Interestingly, however, the reduction in effect size between these models when pain catastrophizing was added was significant (β = 0.51, 95% CI = 0.03–1.33).
These analyses provide partial support for Hypothesis 1. Spiritual wellbeing did not relate to pain sensitivity or tolerance in the manner predicted. However, the effect size reduced significantly with the addition of pain catastrophizing in the model as predicted indicating an indirect relationship between spiritual wellbeing and pain tolerance.
Models testing subconstruct-level simple and controlled relationships
Spiritual wellbeing
The results of the model testing the relationship between spiritual wellbeing and pain sensitivity did not change with the inclusion of rumination (β =−0.18, 95% CI =−0.59 to 0.02). Controlling for helplessness, however, resulted in a significantly weaker relationship (β =−0.22, 95% CI =−0.65 to −0.01).
Likewise, controlling for rumination (β = 0.36, 95% CI =−0.01 to 1.08) had no impact on the spiritual wellbeing-pain tolerance relationship, but controlling for helplessness significantly reduced the regression coefficient (β = 0.58, 95% CI = 0.08–1.34).
Meaning
The simple relationship between meaning and pain sensitivity was not significant (β =−2.41, p = 0.06) nor was the change in the relationship when controlling for pain catastrophizing (β =−0.51, 95% CI =−1.74 to 0.01) or rumination (β =−0.43, 95% CI =−1.51 to 0.06). Including helplessness, however, resulted in a significant reduction in regression coefficient in the complex model of meaning and pain sensitivity (β =−0.63, 95% CI =−1.79 to −0.04).
The simple relationship between meaning and pain tolerance was 6.72 which is significant at the 0.05 level (p = 0.01). Controlling for pain catastrophizing reduced the effect size significantly (β = 1.30, 95% CI = 0.10–3.54), yet the controlled relationship in the complex model remained significant (β = 5.42, p = 0.04). Adding rumination to the model instead, however, resulted in no significant change compared to the simple model (β = 0.87, 95% CI =−0.14 to 2.76). The controlled relationship including rumination remained significant (β = 5.86, p = 0.02). The controlled relationship which removed the influence of helplessness from the model was also significant (β = 5.08, p = 0.05) as was the reduction in effect size between the simple relationship and the relationship adjusting for helplessness (β = 1.64, 95% CI = 0.29–3.96).
Peace
The simple relationship between peace and pain sensitivity was not significant (β =−2.15, p = 0.11). Controlling for pain catastrophizing (β =−0.80, 95% CI =−2.37 to 0.02) or rumination (β =−0.67, 95% CI =−2.13 to 0.13) did not significantly impact this model. The addition of helplessness, however, significantly reduced the regression coefficient of the complex model (β =−0.83, 95% CI =−2.22 to −0.06).
The simple relationship between peace and pain tolerance was significant (β = 8.33, p<0.01) as was the controlled relationship accounting for the effect of pain catastrophizing (β = 6.57, p = 0.02). The difference in relationships between these models was significant (β = 1.76, 95% CI = 0.18–4.80). Similarly, magnification significantly reduced the effect size (β = 1.59, 95% CI = 0.24–3.78), yet the controlled relationship remained significant (β = 6.74, p = 0.01). There was no significant change to the relationship between peace and pain tolerance when rumination was included in the model (β = 1.08, 95% CI =−0.55 to 3.26), and the controlled relationship of this model remained significant β = 7.25, p<0.01). Replacing rumination with helplessness, likewise, resulted in a significant controlled relationship (β = 6.38, p = 0.02) but with significant reductions in effect size between models (β = 1.95, 95% CI = 0.35–4.28).
In total, there was mixed evidence supporting Hypotheses 2. Spiritual wellbeing’s subconstructs of meaning and peace and pain catastrophizing’s subconstructs of helplessness and (sometimes) magnification related to pain perception largely as predicted. Table 2 represents the simple and controlled relationships as well as the results of tests of change between models.
Models of pain sensitivity and pain tolerance. a
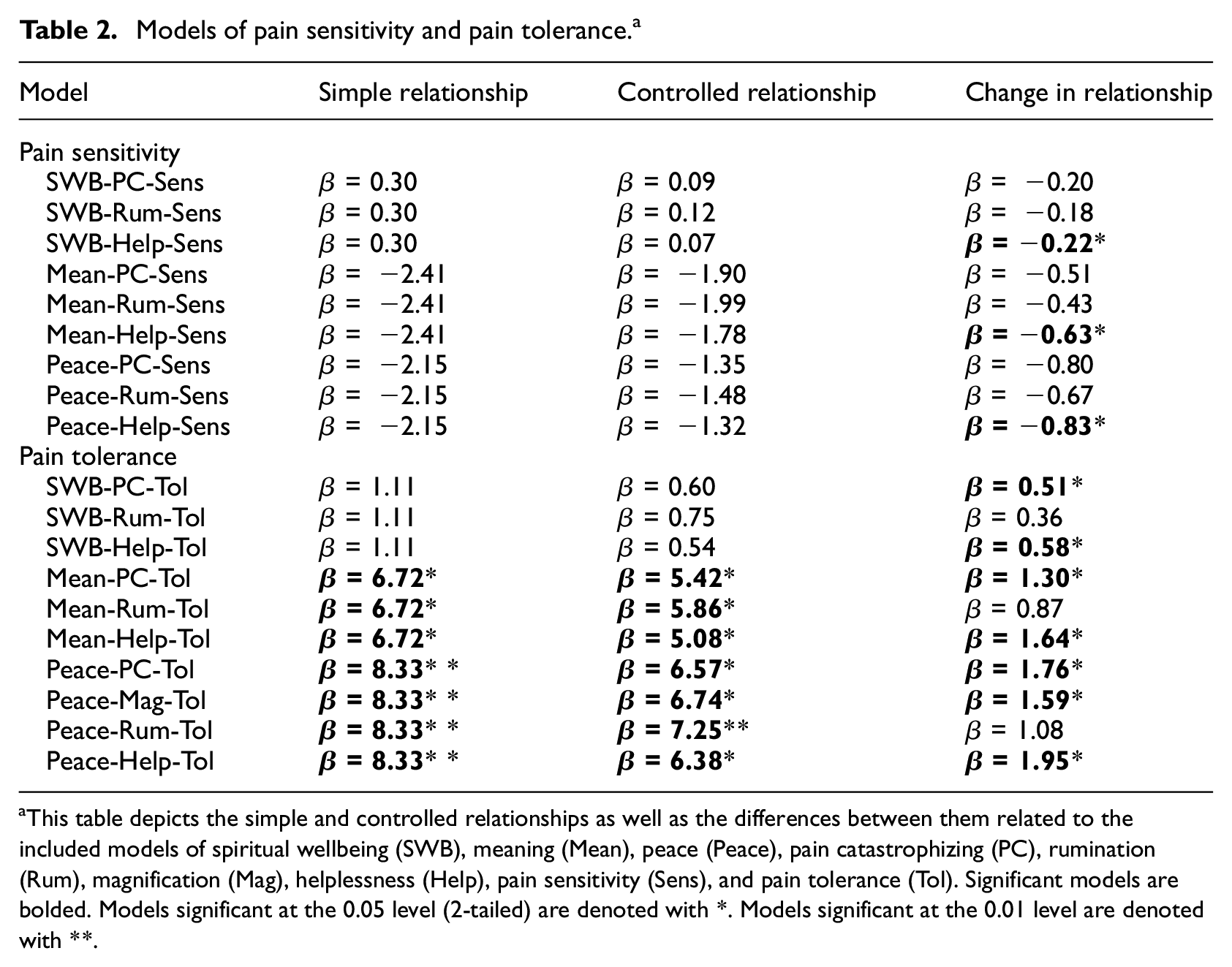
This table depicts the simple and controlled relationships as well as the differences between them related to the included models of spiritual wellbeing (SWB), meaning (Mean), peace (Peace), pain catastrophizing (PC), rumination (Rum), magnification (Mag), helplessness (Help), pain sensitivity (Sens), and pain tolerance (Tol). Significant models are bolded. Models significant at the 0.05 level (2-tailed) are denoted with *. Models significant at the 0.01 level are denoted with **.
Discussion
Findings
Spiritual wellbeing, meaning, and peace were found to indirectly, negatively relate to pain sensitivity through feelings of helplessness. Spiritual wellbeing was also found to relate positively to pain tolerance indirectly through pain catastrophizing and helplessness. Meaning related positively to pain tolerance directly, as well as through pain catastrophizing and helplessness. Peace also related positively to pain tolerance directly and indirectly through pain catastrophizing, magnification, and helplessness. In total, there was partial, mixed support for both examined hypotheses.
Interpretations
Indirect relationships
A primary finding of interest in this study relates to instances where adding complexity to a model changed it significantly despite no existing simple relationship between variables. While spiritual wellbeing directly related to neither pain sensitivity nor pain tolerance, including helplessness or, in one case, pain catastrophizing resulted in a significant reduction of effect size. The lack of simple or controlled relationship between spiritual wellbeing and pain perception despite significant reductions in effects with the addition of the pain catastrophizing or its subconstructs could result from limitations related to the relatively small sample size if the simple or controlled relationships were present but too small to observe given the number of participants. However, in many ways, this also parallels recent developments in mediation procedures which no longer require total effects if the predictor and dependent variables relate through a significant indirect effect (Hayes, 2009; Rucker et al., 2011). Spiritual wellbeing and pain perception can be considered to have an indirect relationship through helplessness and, in one case, pain catastrophizing.
Specificity in spiritual wellbeing
This study’s findings also add unique information about the relationships between spiritual wellbeing and pain perception in part due to departures from the literature which frequently supports spirituality as directly impactful to pain perception (Ferreira-Valente et al., 2019; Siddall et al., 2017). While some indirect relationships were supported in this study, no direct relationships were found at the construct level. This may be explained in part by the inclusion of faith-related items which were not associated with pain perception, directly or indirectly.
As exemplified in the measures section above, in the FACIT-Sp, questions related to faith are worded broadly, and variance in participant’s beliefs may greatly impact their interpretation of this item. In previous research, specific spiritual beliefs have been found to affect appraisals and coping strategy use (Bush et al., 1999). Therefore, a strengthening of faith in some participants may inspire maladaptive coping strategy use, while in others, positive coping strategy use may increase (Bush et al., 1999). This study therefore supports the necessity of further specificity when discussing the subconstructs typically grouped together under the umbrella of spiritual wellbeing.
Transactional model of stress and coping
Another departure from theory relates to pain sensitivity. In contrast to the proposed hypotheses, spiritual wellbeing and its subconstructs were not directly associated with pain sensitivity. This may relate to differences in the type of appraisals which underlie pain sensitivity and pain tolerance as discussed in the introduction. As mentioned, while pain sensitivity relates only to primary appraisals of pain (i.e. threat), pain tolerance also relates to secondary appraisals of perceived ability to cope (Lazarus and Folkman, 1984). This distinction is highlighted by study instructions which direct participants to remove their hands when they “feel they are no longer able to withstand the pain.” Both the pain sensitivity and pain tolerance measure thresholds of appraisal such that even though participants continually engage both types of appraisal, pain sensitivity marks the time when their primary appraisal shifts toward threat and pain tolerance marks the time when their secondary appraisal shifts to inability to cope.
Spiritual wellbeing’s relationship with pain tolerance and not sensitivity, therefore, highlights its impact predominantly on secondary appraisals.
The relationship between spiritual wellbeing (or its subconstructs) and pain sensitivity was significant through helplessness. This may relate to the unique role of helplessness within pain catastrophizing. The appraisal model of pain catastrophizing, built directly off the 1984 Lazarus and Folkman transactional model of stress and coping, separates magnification and rumination as primary appraisal processes while helplessness is considered a secondary appraisal (Severijns et al., 2004). This specific role of helplessness as the most frequently significant mediator in these analyses thus reinforces the interpretation of spiritual wellbeing as more strongly tied to one’s secondary appraisals of coping rather than appraisals of threat.
Limitations
The sample size achieved in this study marks one limitation to its interpretation. According to power analyses based on findings in the literature, this study should be adequately powered to observe expected moderate effect sizes and even many small effect sizes (Chuan and Penyelidikan, 2006). However, no studies were identified which evaluated these variables specifically, so an even smaller effect is possible for some of the variables of interest that may not have been observable based on the current sample. Furthermore, small sample sizes did not permit researchers to control for the effects of potential confounds which may better illuminate specifics within these relationships. The current study analysis adds to the literature in exemplifying that relationships exist between many of the variables of interest. Future studies would benefit from increasing sampling to allow for further analysis and the exploration of potential confounding variables.
This study sought to reflect demographic diversity within the general chronic pain population as opposed to evaluating the effects of any particular subgroup. This approach, however, may muddy findings as diversity within this sample may obscure relationships between these variables for specific subpopulations. Furthermore, despite attempting to represent general chronic pain populations, study demographics appear skewed toward White (85.8%) and female (60.8%) participants compared to chronic pain prevalence studies on race/ethnicity (Janevic et al., 2017; Rikard et al., 2023) and sex (Breivik et al., 2006). As individuals in racial minority groups are more likely to report higher intensity of pain (Janevic et al., 2017; Rikard et al., 2023), it is particularly critical for future studies to replicate current analyses with samples centered on ethnic and racial minorities to adequately represent the unique experiences of these populations.
Although including individuals with various opioid use and histories and opioid addiction statuses may reflect diversity within chronic pain populations, consolidating participants from these backgrounds into one sample may have also clouded study findings. Individuals with different opioid use histories and addiction statuses have been found to perceive pain differently (Wachholtz and Gonzalez, 2014). Opioid abuse treatment frequently targets pain catastrophizing as a method of action (Jensen et al., 2001). It may be possible that opioid use impacts spiritual wellbeing as well. Future studies would benefit from controlling for this as a potential confound.
Religious affiliation may also impact the relationships explored here. Religious affiliations of participants are frequently reported as a demographic variable; however, few, if any, studies have evaluated the impact of specific religious affiliations on either pain catastrophizing or pain perception. Further studies of the relationships between spiritual wellbeing, pain catastrophizing, and pain perception would benefit from increasing representation of various religious groups within their samples and evaluating religious affiliation as a potential confounding variable.
Clinical implications
Understanding the relationships between spiritual wellbeing, pain catastrophizing, and pain perception is important in ensuring treatment is holistic and cognizant of individual factors that may influence treatment progress. Spiritual wellbeing evolves over time, naturally and in response to specific learning opportunities (Pong, 2021), and some pain treatment programs even target spiritual wellbeing as a major component of treatment (Steinhorn et al., 2017). Likewise, reducing pain catastrophizing is a proven and popular mechanism for chronic pain treatment (Jensen et al., 2001).
It is important that treatment facilities are deliberate in how these factors are assessed and treated. This study illustrates that while meaning and peace more directly relate to pain tolerance, spiritual wellbeing itself seems to primarily relate indirectly through helplessness and pain catastrophizing. Programs that wish to target spiritual wellbeing or pain catastrophizing as a mechanism of pain treatment would therefore be best served by expanding treatment to measure or target the other as well to obtain a more complete image of progress. Additionally, it may be more beneficial to focus on subconstructs within these measures to avoid assessments being clouded by potentially divergent relationships within these subconstructs.
Future directions
A future study which focuses on a subset of these relationships would clarify the connections between included variables while more strongly assuring avoidance of type I errors without increasing the likelihood of type II error through a post-hoc correction (Armstrong, 2014). An experiment more closely targeted on these variables would also allow for deeper investigation.
A longitudinal study or randomized control trial which alters spiritual wellbeing or pain catastrophizing may provide greater insight into the directionality within these relationships. This is especially important in guiding treatment programs that seek to target spiritual wellbeing or pain catastrophizing as the current study illustrates that these relationships exist, not that one variable influences another in a causal manner. A longitudinal design would also help account for atypical scores on any of these measures to determine if findings are based on state (short term) or trait (long term) exhibition of any of these constructs.
Another potential future direction relates to the evaluation of these relationships in other pain populations. This study included individuals with musculoskeletal or mixed musculoskeletal and neuropathic pain. This marks a divergence from general pain epidemiology as up to 10% of individuals report neuropathic pain, many without musculoskeletal pain (Van Hecke et al., 2014). Furthermore, this study included no individuals with other types of pain, such as pain related to inflammation or mechanical compressions, and it distinguished between neither the area(s) of the body in which pain is experienced nor the qualitative sensations of pain (e.g. burning vs sharp pain). Future studies may benefit from exploring these differences as separate populations or as confounds.
Many of the biopsychosocial-spiritual factors not examined in this study may also function as potential confounds in these relationships. Traits such as age (Lautenbacher et al., 2017), reactions to pain such as fear of pain (Martinez-Calderon et al., 2019) and pain self-efficacy (Jackson et al., 2002), and mental illnesses such as anxiety (Oktay et al., 2008) have been found to impact pain perception. Now that relationships between spiritual wellbeing, pain catastrophizing, and pain perceptions have been established, future studies would benefit from adjusting for these additional factors to examine if they may explain some of these relationships.
Conclusions
The impacts of pain are complex and far reaching. Understanding factors which relate to pain perception is important in building treatment options to holistically address the experience of chronic pain. In this study, spiritual wellbeing was shown to correlate with pain tolerance indirectly through pain catastrophizing and helplessness. Meaning related to pain tolerance directly as well as through pain catastrophizing and helplessness. Peace also correlated with pain tolerance directly and indirectly through pain catastrophizing, magnification, and helplessness. The links between spiritual wellbeing and pain sensitivity were weaker although spiritual wellbeing, meaning, and peace significantly related to pain sensitivity indirectly through feelings of helplessness. Overall, spiritual wellbeing appeared more strongly related to secondary appraisals of coping over primary appraisals of threat in the context of pain.
Understanding how spiritual wellbeing and pain perception relate is necessary in conducting tests of causality and building treatment options that consider the wide array of factors that impact the experiences of pain and spirituality. While further research is still needed, this study marks an important step to holistically understanding the web of factors that influence every individual’s experience.
Footnotes
Author contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by Dr. Amy Wachholtz. Literature review and data analysis were conducted by Daniel Luedtke. The manuscript was written by Daniel Luedtke with edits and guidance from Dr. Amy Wachholtz. All authors read and approved the final manuscript.
Data availability statement
The data generated during the current study are available upon reasonable request. Please contact the senior author (Amy Wachholtz) to request access to the current data.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a National Institute on Drug Abuse (NIDA) K23 grant (DA030397) to senior author (Amy Wachholtz).
Ethics approval
Methodology resulted in no more than minimal risk to participants and aligned with standard practices in the field. All procedures were approved by the University of Massachusetts Medical School IRB in 2015 (IRB ID: H00009301).
Informed consent
Written, informed consent was obtained from all individual participants included in the study.