
Abstract
Sexual health is integral to physical and mental wellbeing. Yet, sexual health literacy (SHL) is understudied and there is a dearth of reliable and valid SHL measures. To address this gap in the literature, we used Robinson’s Sexual Health Model to guide this qualitative study of sexual health experts’ perspectives of SHL as part of a larger project to inform SHL scale development. Participants were eight cisgender women professionals with sexual health expertise. Participants completed an hour-long semi-structured virtual interview, which was transcribed and then analyzed using thematic analysis. Results provide insight into perceived gaps in, facilitators and barriers to promoting, and considerations for assessing SHL. Findings offer insight into sexual health promotion among diverse populations and will be used to guide development of a SHL scale.
Introduction
Sexual health is defined as “ …a state of physical, emotional, mental and social well-being in relation to sexuality” (World Health Organization [WHO], 2017) and contributes to increased employment and educational opportunities, economic stability, the fulfillment of life goals, improved relationships, life satisfaction, and longevity (Becasen et al., 2015; Hogben et al., 2015; Mustanski et al., 2015; Satcher, 2001). Necessary for attaining optimal physical and mental health, sexual health is considered a basic human right (Office of the UN High Commissioner for Human Rights (OHCHR), n.d.). It is therefore critical to ensure people are literate about sexual health to prevent diseases and promote positive health outcomes.
Sexual health literacy
Defined as “the degree to which individuals have the ability to find, understand, and use information and services to inform health-related decisions and actions for themselves and others” (Brach and Harris, 2021; United States Office of Disease Prevention and Health Promotion, n.d.), health literacy contributes to optimal health in several ways. For example, health literacy helps people navigate and meaningfully participate in their healthcare (DeMarco and Nystrom, 2010; Van Den Broucke, 2014) and improves healthcare communication between providers and patients (Ishikawa and Kiuchi, 2010; Lambert and Keogh, 2014). Compared to other forms of health literacy, relatively little attention is paid to sexual health literacy (SHL), despite its importance for promoting positive sexual health. SHL can help empower people to respect and take responsibility for their sexual needs and lives (Carter et al., 2021). SHL also can help prevent or minimize negative outcomes and sexual health disparities (Batterham et al., 2016), such as sexually transmitted infections (STIs) and unintended pregnancies, which disproportionately affect people of color and sexual and gender minorities (Feldstein Ewing and Bryan, 2020; Parks and Peipert, 2016; Steele et al., 2009).
Expanding on general health literacy definitions, SHL can be defined as the ability to find, use, and understand information and services to inform sexual health-related decisions and actions. Recognizing that complex and interacting systems influence SHL, McDaid et al. (2021) offer a comprehensive framework for understanding SHL that incorporates sexual health information (content and delivery); skills (e.g. to find, understand, evaluate, and discuss sexual health information); information users (e.g. sexual partners or networks, peers, communities); information providers (e.g. healthcare workers, community-based organizations); and systems (i.e. social and structural drivers). Although many measures of general health literacy (e.g. Rapid Estimate of Adult Health Literacy in Medicine, Davis et al., 1991) and disease-specific health literacy (e.g. Brief Estimate of Knowledge and Action-HIV, Osborn et al., 2010) exist, a recent systematic review (Chenneville et al., under review) revealed very few measures that specifically assess SHL.
Theoretical framework and purpose of study
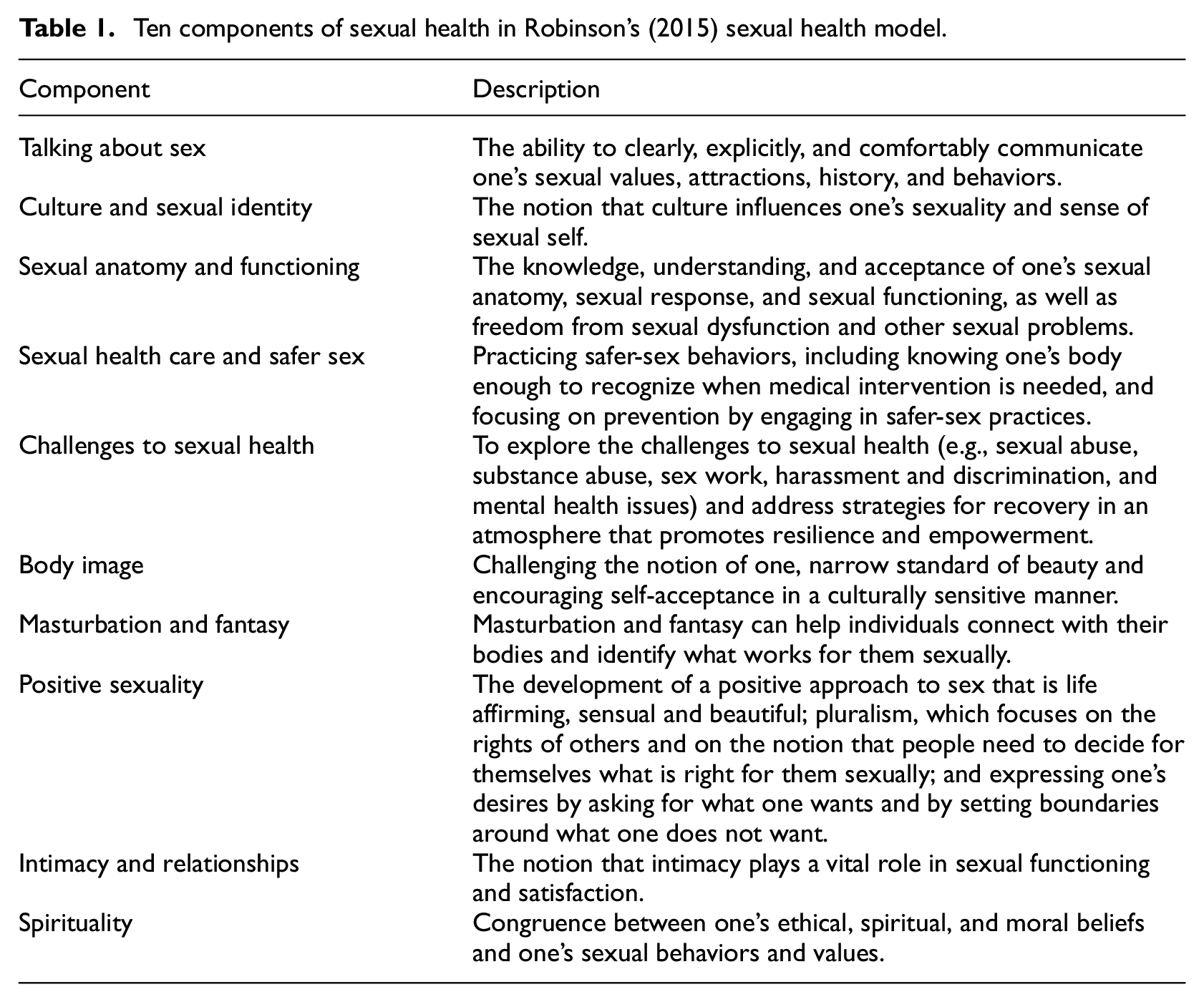
Guided by Robinson’s (2015) Sexual Health Model (SHM), first described in Robinson et al. (2002), this phenomenological qualitative study aimed to gather data from sexual health experts about SHL as part of a larger project to inform SHL scale development. Although other SHMs exist (e.g. Hensel and Fortenberry’s, 2013 multidimensional model), most focus on specific populations or specific sexual health problems. Further, many sexual health frameworks are overly medicalized and narrowly focused on disease prevention, failing to account for the broader social context of diverse sexual identities and practices, sexual rights, and sexual pleasure (Epstein and Mamo, 2017). Addressing many of these concerns, Robinson’s (2015) SHM approaches sexual health holistically, recognizing the importance of not just preventing sexual health problems but also promoting positive sexual health, including sexual satisfaction and pleasure, among diverse populations. This model includes 10 areas considered important for sexual health along the prevention (of negative outcomes) to promotion (of positive outcomes) continuum: talking about sex, culture and sexual identity, sexual anatomy and functioning, sexual healthcare and safer sex, challenges to sexual health, body image, masturbation and fantasy, positive sexuality, intimacy and relationships, and spirituality. See Table 1.
Ten components of sexual health in Robinson’s (2015) sexual health model.
Methods
Study design and approach
We employed a qualitative research design using a phenomenological approach (Creswell and Poth, 2016) to explore sexual health experts’ perceptions of sexual health and SHL.
Participants
Participants were professionals from varied disciplines across health and education sectors across all United States (U.S.) regions with expertise in sexual health. We included professionals identified as having sexual health expertise through personal knowledge, word-of-mouth referrals, literature reviews, and internet searches (i.e. to identify scholars doing work in sexual health). We excluded sexual health professionals whose contact information was not available on the internet.
Procedures
The University of South Florida Institutional Review Board reviewed and determined this study [STUDY004861] exempt given that the data collected contained no identifying information. The research team generated a list of 26 potential participants across the U.S. including two from the Northwest, four from the Northeast, three from the Midwest, four from the Southwest, and 13 from the Southeast (where the study originated, resulting in greater familiarity with sexual health experts in the region). To ensure geographic representation across regions, we staggered recruitment. The lead investigator emailed an invitation to participate in the study to the first potential participant from each of the five major U.S. regions. Participants who responded were referred to another research team member who scheduled a 1-hour virtual interview. Two weeks after the initial request, the lead investigator sent a follow-up email to potential participants who did not reply with a response deadline. Once we recruited initial participants from each region, we used the same procedure to recruit additional participants from each U.S. region until we reached data saturation, defined here as the point at which no new information was emerging from the interviews (Saunders et al., 2018), determined through discussions among the research team.
To address budget constraints and logistical issues prohibiting face-to-face data collection, we conducted and recorded virtual interviews via Microsoft Teams, which offers end-to-end encryption. Interviewers were two members of the research team (see Author Positionality section below for a description of the team) assigned based on scheduling availability. Following a brief introduction, the assigned interviewer obtained verbal consent using a script and conducted a semi-structured interview using questions the research team developed to elicit information about how sexual health experts define sexual health and SHL; SHL aspirations for patients/clients/students/community members (depending on professional role) along the prevention to promotion continuum; perceptions of SHL facilitators and barriers; the potential utility of a SHL measure; and desired components of, and how to incorporate diversity, in a SHL measure (see Supplemental File 1 for a complete list of interview questions). Participants then received a Qualtrics link to an anonymous demographic survey. Upon completion, participants received $50USD via a mobile banking app. Using the transcription feature, Microsoft Teams automatically transcribed recordings at the end of each interview. The interviewer reviewed the transcript to ensure it contained no identifying information and saved it onto a university-sponsored secure cloud-based file management platform only accessible to the research team. Interviewers then deleted recordings. Aggregate anonymous demographic survey results were accessed after data collection ended.
Data analysis
Our analysis drew on principles of reflexive thematic analysis (RTA; Braun and Clarke, 2006; Clarke and Braun, 2016), particularly its emphasis on flexibility, inductive coding, and iterative theme development. However, we incorporated structured elements more akin to template analysis (Brooks et al., 2015), including the development of a codebook to enhance analytic transparency and consistency. While RTA typically does not employ a structured coding framework, we used the codebook as an organizational tool rather than a rigid coding structure. Additionally, we engaged in negotiated agreement to refine codes and themes while remaining mindful of RTA’s focus on researcher reflexivity in the interpretative process. This blended approach allowed us to balance an inductive, phenomenologically-informed meaning-making process with structured analytic practices, ensuring both depth and coherence in theme development.
First, two independent coders familiarized themselves with the data by reading an entire transcript and making memos in the margins. They then reviewed the transcript again to identify and assign codes to meaningful units (i.e. quotes). After establishing codes, the data analysis team (i.e. two coders and a mediator) met to discuss and finalize codes using negotiated agreement. Subsequently, the team created a codebook using Microsoft Excel, a simple, cost-effective, and acceptable manual coding approach (Bree and Gallagher, 2016; Ose, 2016). Using the codebook, the coders repeated the familiarization and coding process for each transcript. Afterward, the research team met to finalize codes and determine if new codes should be added. After coding all transcripts, the coders met to condense codes into initial themes and subthemes, ensuring that preliminary themes matched the original data and determining if any themes could be subsumed under an existing theme. After shifting focus back to the original data and revising themes as needed, coders finalized themes/subthemes, which the research team reviewed/confirmed.
Author positionality
Author positionality is a term used to describe how authors’ intersecting identities can influence their interpretations of qualitative data and present potential bias (Bourke, 2014; Massoud, 2022) and contributes to the broader concept of trustworthiness in qualitative research (Adler, 2022). All authors are White/European American heterosexual cisgender women affiliated with the same large urban, Carnegie classified R1 university in the Southeastern U.S. One author has a doctoral degree in psychology and is a licensed psychologist. Three authors have Master’s degrees in psychological sciences, with one enrolled in a doctoral psychology program. All authors have sexual health research experience.
Results
Participant demographics
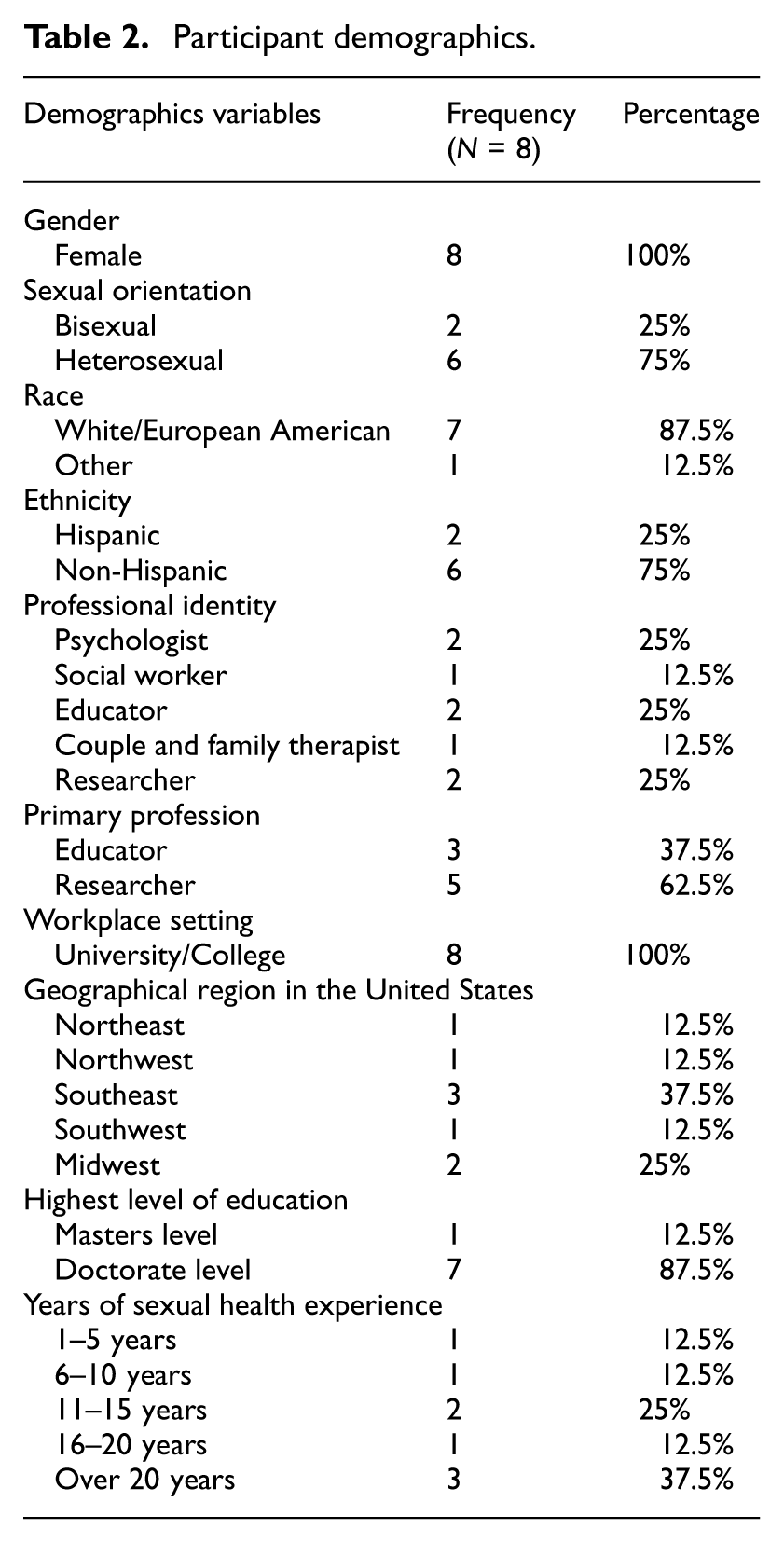
Participants were eight cisgender women aged 33–62 (M = 45.7, SD = 9.9) with sexual health expertise. Most participants identified their racial identity as White/European American (n = 7), ethnic identity as non-Hispanic (n = 6), and sexual orientation as heterosexual (n = 6). In terms of professional identity, two participants identified as psychologists, two as educators, two as researchers, one as a social worker, and one as a couples/family therapist. Over half (n = 5) described their current role as that of a researcher, while others (n = 3) described their current role as that of an educator. All participants (n = 8) worked in a university or college setting in mostly urban (n = 7) areas across U.S. regions - Southeast (n = 3), Midwest (n = 2), Northeast (n = 1), Northwest (n = 1), and Southwest (n = 1). Most (n = 7) had doctorates. One had a master’s degree. Three had over 20 years of sexual health experience, two had 11–15 years, one had 16–20 years, one had 6–10 years, and one had 1–5 years. See Table 2.
Participant demographics.
Categories and themes
We used the following categories to organize themes based on the interview data: observed gaps in SHL, facilitators to promoting SHL, barriers to promoting SHL, and considerations for assessing SHL. Themes and subthemes within each category are summarized below. See Supplemental File 2 for a table containing a complete list of categories, themes, subthemes, and representative quotes using pseudonyms as well as corresponding components of Robinson’s (2015) SHM.
Observed gaps in sexual health literacy
Participants’ discussions about perceived gaps in SHL among the people they serve revealed three themes cutting across six components of Robinson’s (2015) SHM. See Supplemental File 2. The first theme, limited knowledge about holistic sexual health across the lifespan, captures participants’ perceptions that many people have a limited understanding of anatomy and physiology and do not know how to engage in appropriate physical and emotional self-care including what to do when facing developmental sexual health concerns (e.g. men experiencing erectile dysfunction or women experiencing menopause). For example, one participant (Sam) said, “I don’t think people know how to take care of themselves physically and probably not to take care of themselves spiritually, emotionally, and socially, not, not as a whole.” This theme highlights the challenges associated with failing to situate sexual health within the context of overall health.
The second theme, difficulty communicating about sex, captures the discomfort many people feel talking about sex. To illustrate, one participant (Alex) gave the example of how many people might be uncomfortable using terms such as “penis” and how uncomfortable many parents are talking about sex with their children. Another participant (Gloria) described how difficult it is for some people to discuss sex with their partners: “if you don’t know your bodies and what feels good, it’s harder to then also, to know what, is not feeling good. And to be really articulate about that and kind of what you want.” This theme highlights the challenges to sexual health that communication barriers pose and how being able to talk about what one knows and what one does not know about sex is important for sexual health.
The third theme, lack of understanding about the importance of sexual agency, captures the need for people to connect with and take control over decisions affecting their bodies and highlights how doing so relates to sexual experiences and overall sexual health. For example, one participant (Alex) described how she tells her patients, “. …you have to be empowered, you have to have a sense of autonomy, and you have to know that you sometimes may have to lead those conversations…if you don’t, you’re not gonna get what you want out of that experience or that interaction… ” Another participant (Barbara) encouraged giving young patients “information that they deserve [about] bodily autonomy, what that might mean for them, and how that reflects. [This information] should support their ability to make decisions and access services that are best for them. Not a partner, not a parent, but centering their needs and desires.” This participant also explained that her team “push[es] for providers and parents to allow teens to have time alone with the provider. It’s not just about the confidentiality of that time, it’s also about the skill building of being an advocate for one’s own.”
Facilitators to promoting sexual health literacy
We identified two themes illustrating facilitators to promoting SHL cutting across five components of Robinson’s (2015) SHM. See Supplemental File 2. The first theme, sexual health education, captures the need for widespread education about sexual health. Within this theme, there were several subthemes. The first subtheme, public messaging to increase awareness of sexual health, captures how media and public health campaigns can be useful for educating the public about sexual health matters. For example, one participant (Sally) talked about the importance of having “champions…personalities that are trusted by communities” to deliver sexual health messages. This subtheme highlights the need for varied educational outreach strategies tailored to the intended audience. The second subtheme, normalizing sexual health as a topic of conversation, captures the importance of providing developmentally appropriate sexual health education from an early age and highlights the importance of creating a society where exploring sexual health matters is not taboo. For example, one participant (Taylor) talked about the importance of becoming “a society that, you know, openly gives permission and accepts, you know, the exploration and accepts, you know, the exploration and questions and, and understanding of sexual health.” Building on this, the third subtheme, training sexual health educators, captures the importance of standardized training for sexual health educators. One participant (Alex) described regulation to ensure the credibility of information, noting that the lack of regulation “makes it hard to figure out who you can trust” and can result in people claiming to be sexual health experts “spewing nonsense to people.”
The second theme, diverse representation and inclusivity, captures participants’ perceptions that attention to diversity and inclusivity is important for promoting SHL as sensitivity to cultural differences makes sexual health information more accessible and relatable, helps reduce stigma, and challenges misinformation and stereotypes. For example, one participant (Bethany) talked about “having providers ask about pronouns” as an example of “inclusive care.” Participants also discussed societal shifts in understanding gender and sexuality with increased media representation of diverse identities. For example, one participant (Sam) said, “I love the fact you can go on Netflix and there is an LGBTQ genre.” This theme highlights that promoting SHL requires a recognition of diverse sexual and gender identities.
Barriers to promoting sexual health literacy
We identified four themes illustrating barriers to promoting SHL cutting across eight components of Robinson’s (2015) SHM. See Supplemental File 2. The first theme, laws and policies that limit sexual and reproductive education and rights, captures the impact of legislation and political factors on the promotion of SHL. For example, participants described “government systems” (Sally) that limit access to contraception and abortion or that eliminate “funding” (Rebecca) for comprehensive sexuality education as systematic barriers to SHL. As one participant (Gloria) explained, “I think more broadly it’s just also people understanding the connection of like, if you start restricting access to like abortion care, that that does actually relate to restrictions on contraceptive care and these are all kind of related and access will shrink for everything.” This theme highlights the role the local and federal government plays in sexual health.
The second theme, limited access to accurate, holistic, and diverse/inclusive sexual health information and resources, captures issues related to misinformation and incomplete information. For example, one participant (Taylor) described how many people have access to the “wrong things” and another participant (Alex) described how teaching young people that “sex is for procreation” fails to acknowledge the reality that many people have sex for pleasure and that pleasure is an important aspect of sexual health. Another participant (Barbara) said, “I wish that we spend less time worrying about which teen’s body parts were rubbing together and more time worried about the quality of those relationships.” This theme highlights the negative impact of narrow definitions of sexual health.
Building on the previous theme, the third theme, views of sex as taboo, captures the problems that arise because of overly conservative ideas about sex. One participant (Bethany) described the impact of a “Puritan notion around sexuality” and the infiltration of “Judeo-Christian roots” on our ability to “talk about sex openly.” This theme highlights the negative impact on SHL that stems from culturally constrained beliefs about sex.
The fourth theme, limited media literacy, captures the problems associated with people turning to the Internet or social media for information about sexual health. For example, one participant (Sally) expressed concern that information accessed on social media “may be actually technically completely off” and another participant (Taylor) described how the Internet may contain “false information or, you know, information presented inappropriately along the lifespan.” This theme highlights the need to teach people how to access credible sources of information on the Internet.
Considerations for assessing sexual health literacy
We identified four themes illustrating participants’ perspectives on assessing SHL cutting across five components of Robinson’s (2015) SHM. See Supplemental File 2. The first theme, potential utility of a SHL scale, captures participants’ thoughts about how a SHL scale might be used. This theme was separated into two subthemes: establishing a baseline and linking assessment with impact and intervention. For example, participants described how a SHL measure could be used to determine where a person stands regarding their understanding of the various aspects of their sexual health. One participant (Alex) noted it would be useful to know where a person is “starting” in terms of their understanding of sexual arousal and pleasure and noted that a SHL scale could be used for pre/post assessment. Participants also described how information gathered from a SHL measure could be used to better understand the impact of sexual health on overall wellbeing, develop tailored interventions, and monitor progress. One participant (Alex) also noted how data gathered from a SHL measure could be used to create “actionable steps” (e.g. a “prevention schedule of how you need to be taking care of your body”). This theme highlights the practical utility of a SHL scale for improving sexual health.
The second theme, promoting equity through diverse and inclusive assessment strategies, captures the importance of creating a scale that is accessible to diverse cultures and members of marginalized communities. For example, one participant (Bethany) cautioned against “making assumptions about partner types” (e.g. misgendering) and the importance of “inclusive examples and inclusive pronouns.” One participant (Rebecca) suggested “using intersectionality as a guiding framework” to scale development, noting the importance of considering “power and social context” and the importance of acknowledging “different religious beliefs or racial and ethnic cultural, beliefs, race and gender identity.” This theme highlights the idea that a SHL measure should be relatable to people from diverse backgrounds.
The third theme, usability, captures the idea that a SHL measure should be designed with ease of use in mind. Participants described brevity as important (e.g. “has to be fairly brief” [Bethany]) and noted that a SHL measure should be “easy to score” (Sam). Participants highlighted the importance of using simple language as well. This theme highlights important considerations for designing a SHL measure that is functional in real world settings.
The fourth theme, accessibility, captures participants’ ideas about how to make a SHL accessible to a wide audience. For example, one participant (Alex) suggested having a SHL measure available to students on a university website might be useful for self-assessment purposes. Another participant (Taylor) indicated an app might be useful for administration purposes. This theme further highlights the need for scale design construction that takes into consideration how the SHL measure will be used.
Discussion
Sexual health is an important aspect of overall health and mental wellbeing and, therefore, is highly relevant within the field of health psychology and the broader discipline of psychology. Although health literacy is increasingly recognized as critical for optimal health, sexual health literacy (SHL) has received relatively little attention and few validated SHL measures exist. Guided by Robinson’s (2015) SHM and using thematic analysis, findings from this qualitative study aimed to address this gap and to inform SHL scale development by providing insight into what sexual health experts perceive to be gaps in SHL and facilitators and barriers to promoting SHL as well as their perspectives on assessing SHL. All 10 components of Robinson’s (2015) SHM were represented in the themes and subthemes we identified in the data. See Table 1.
Consistent with the WHO’s (2017) definition of sexual health and perspectives of sexuality as a normal part of human development (Crooks et al., 2020), the experts interviewed in this study acknowledged that sexual health is an integral component of overall wellbeing that includes not only physical functioning but also emotional, social, and spiritual functioning. Despite this, experts perceived that many people are unaware of the relationship between sexual health and overall wellbeing, have limited understanding of sexual anatomy, and lack critical information about sexual health across the lifespan, supporting the call for more holistic approaches to understanding sexual health (e.g. moving beyond merely sexual risk avoidance to include sexual positivity; Kantor and Lindberg, 2020). Experts also perceived that many people are limited in their ability to communicate about sex and do not recognize the importance of sexual personal autonomy and control when it comes to decisions affecting sexual health. The idea that sexual agency is central to sexual health aligns with the Guttmacher-Lancet Commission’s (Starrs et al., 2018) report on sexual and reproductive rights. Consistent with Tarasoff’s (2021) call for comprehensive and inclusive sexual and reproductive health education to address the needs of all people including people with disabilities or who identify as LGBTQ+, experts described the importance of diverse, inclusive, factual, and non-stigmatizing information for promoting sexual health, emphasizing the importance of varied strategies across a variety of contexts. Among strategies discussed, experts talked about the importance of public health and media campaigns. In a scoping review of sexual health promotion interventions delivered via digital media, Bailey et al. (2015) found that digital media strategies can, indeed, be effective although issues surrounding technology access, safety, and quality must be addressed when designing digital media interventions. In support of experts’ discussion about the importance of specialized training, research suggests that even medical students in the U.S. lack adequate sexual health knowledge, which may translate to physicians being ill-prepared to address sexual health issues in clinical practice (Warner et al., 2018) and educate patients about sexual health. Sexual health experts identified several barriers to promoting SHL including systemic issues that negatively affect the ability to access sexual health information, resources, and services including laws and policies that limit sexual and reproductive education and rights. Often overlooked in health promotion policy and programing, there is growing recognition that sexual pleasure should be a focus of public health law, policy, and advocacy (Ford et al., 2019). Barriers also included sex shaming attitudes perpetuated by conservative values, including those promoted by religious beliefs. However, research suggests the relationship between religiosity and sexual health may not be straightforward. For example, Watson et al. (2019) found that religiosity was associated with a lower probability of being diagnosed with an existing STI, including HIV, among a sample of 225 Black bisexual men, but not self-disclosure of STIs. As Watson et al. (2019) note, this is a particularly vulnerable group given the impact of double minority stress and potentially increased risk for STIs and HIV. As another example of the complex relationship between religion and sexual health, sex positivity is a hallmark of modern and contemporary Judaism (Epstein-Levi, 2019). Finally, experts offered insight into the potential utility of a SHL scale and offered useful suggestions for SHL development. Experts emphasized the need for a brief measure containing inclusive content that could be used to guide interventions to improve SHL for the purpose of not only preventing negative sexual health outcomes but also promoting positive sexual health outcomes among diverse populations. As noted above, findings from a recent systematic review (Chenneville et al., under review) revealed a dearth of SHL measures. In fact, only nine of the 2378 articles included in the review contained a sexual health scale, subscale, or item(s), only one of which was a true SHL scale. Other scales or items assessed components of SHL (e.g. knowledge, attitudes) and none of the scales addressed all areas of Robinson’s (2015) Sexual Health Model.
Implications for health psychology
Given the link between SHL and sexual and reproductive health (Kilfoyle et al., 2016; Rakhshaee et al., 2020), SHL research is important in the field of health psychology and, more broadly, the psychology discipline. Rohleder and Flowers (2018) highlighted the need for an inclusive and multifaceted approach to sexual health psychology, emphasizing the importance of a holistic understanding of sexual health that extends beyond traditional biomedical models. Current findings contribute to our understanding of how some sexual health experts define SHL and what they perceive to be facilitators and barriers to promoting SHL. The use of current findings to guide the development of a SHL measure will help advance health psychology by providing a tool that can be used by researchers to assess SHL gaps and develop evidence-based interventions, educators to design and monitor the impact of targeted sexual health curricula, and practitioners to tailor interventions that address specific needs and improve sexual health outcomes in diverse populations.
Strengths and limitations
The use of an existing theoretical model to guide this study is a strength in that it provided a structured lens through which to interpret data and helped anchor findings in a broader context. Although overreliance on theoretical frameworks may be problematic (Dodgson, 2019), balanced use of theory can strengthen qualitative approaches (Collins and Stockton, 2018). Our use of Robinson’s (2015) SHM, specifically, may be considered a strength given its holistic approach to preventing sexual health problems and promoting positive sexual health among diverse populations. However, this model is limited given its cursory focus on sexual rights (see Positive Sexuality component of Robinson’s, 2015 SHM). Both the WHO (2024) and the World Association for Sexual Health (2014) describe sexual rights as human rights that are central to the promotion of sexual health.
The study’s sample posed both strengths and limitations. Regional representation, the inclusion of participants who identified as ethnic and/or sexual minorities, and the involvement of experts in different professional roles and at different career stages are strengths in terms of increasing the applicability of findings to a diverse range of experiences, cultures, and environments. However, although generalization is not the goal of qualitative research and data saturation was met in this study (Roy et al., 2015), the small sample size may be considered limiting, especially within the context of controversy over how to define and assess data saturation (Fusch and Ness, 2015; Hennink et al., 2017; Saunders et al., 2018).
Another weakness is that the sample was limited to cisgender women who all worked in a university or college setting, and the social and professional identity of the research team was limited to educated White heterosexual women from the U.S. with sexual health research experience. Although similarities in gender, race, ethnicity, and professional background between interviewers and participants may have facilitated rapport building and open dialog, the lack of diversity among the research team and participants creates a limited worldview that likely influenced data collection and interpretation (Berger, 2015). More specifically, gender homogeneity among the research team and sample likely limited the range of perspectives considered, thereby influencing our findings. While the gender composition of the research team and sample likely reflects feminization in health care professions and in science (Marquini et al., 2023), the exclusivity of women as researchers and participants in this study may have narrowed the scope of critical inquiry and reinforced existing gendered narratives in the field. Existing research suggests that gender-diverse teams tend to produce more innovative research outcomes compared to homogeneous teams (Love et al., 2022).
Lastly, some may criticize the use of Microsoft Excel instead of qualitative analysis software to analyze qualitative data due to concerns about bias and inter-rater reliability (McAlister et al., 2017). However, using Microsoft Excel allows for an acceptable, simple, cost-effective, systematic manual approach to coding (Bree and Gallagher, 2016; Ose, 2016).
Conclusion and future directions
Current findings demonstrate experts’ perspectives on SHL including perceived gaps, facilitators and barriers to SHL promotion, and insights into the potential utility of a SHL scale and factors to consider during scale development. Findings align with the holistic components of sexual health outlined in Robinson’s (2015) model. Consistent with findings from a systematic review of SHL measures (Chenneville et al., under review), current findings support the need for a functional and inclusive SHL scale that can be used in clinical, educational, and research settings to promote sexual health among diverse populations along the prevention to promotion continuum. Along with other sexual health research, authors will use this study’s findings to guide the development of a SHL measure. Beyond assessing SHL, future research is needed on effective strategies for promoting sexual health among diverse populations.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251325959 – Supplemental material for Exploring and improving sexual health literacy: Insights from sexual health experts
Supplemental material, sj-docx-1-hpq-10.1177_13591053251325959 for Exploring and improving sexual health literacy: Insights from sexual health experts by Tiffany Chenneville, Serena Wasilewski, Kaitlyn Ligman and Morgan Haskett in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053251325959 – Supplemental material for Exploring and improving sexual health literacy: Insights from sexual health experts
Supplemental material, sj-docx-2-hpq-10.1177_13591053251325959 for Exploring and improving sexual health literacy: Insights from sexual health experts by Tiffany Chenneville, Serena Wasilewski, Kaitlyn Ligman and Morgan Haskett in Journal of Health Psychology
Footnotes
Acknowledgements
We would like to acknowledge Dr. Trevor Hart at Toronto Metropolitan University for his assistance with protocol development. ChatGPT 4.0 was used in the preparation of this manuscript for idea generation and exploration.
Author contribution
Tiffany Chenneville, Ph.D.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, supervision, validation, visualization, writing- original draft, and writing- review & editing. Serena Wasilewski, M.A.: Data curation, formal analysis, investigation, methodology, project administration, validation, visualization, writing- original draft, and writing- review & editing.
Kaitlyn Ligman, M.A.: Data curation, formal analysis, investigation, methodology, validation, visualization, writing- original draft, and writing- review & editing.
Morgan Haskett, M.A.: Data curation, formal analysis, investigation, methodology, validation, visualization, and writing- review & editing.
Data sharing statement
Data are available from the corresponding author, upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of South Florida Creative Scholarship Grant.
Ethics approval
Our study was approved by The University of South Florida Institutional Review Board (Study No. 004861).
Informed consent
All participants provided verbal informed consent prior to enrollment in the study.
Consent for publication
Consent for publication is not applicable as it does not contain any identifiable data.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.