
Abstract
This study aimed to investigate the impact of beliefs about breathlessness on health-related quality of life (HRQoL) among chronic obstructive pulmonary disease (COPD) patients and to explore whether self-efficacy and self-management behaviors mediate this relationship. A cross-sectional study was conducted with 287 Chinese COPD patients. Mediation analysis was performed using structural equation modeling with Amos 24.0. The findings indicated that self-efficacy and self-management behaviors independently mediated the relationship between breathlessness beliefs and HRQoL, accounting for 28.91% and 33.01% of the overall effect, respectively. Additionally, a serial mediating effect of self-efficacy and self-management behaviors was found in the link between breathlessness beliefs and HRQoL, accounting for 6.33% of the total effect. This finding demonstrated that self-efficacy and self-management behaviors served as sequential mediators in the relationship between breathlessness beliefs and HRQoL. Targeted interventions should be developed to address breathlessness beliefs, enhance self-efficacy, and promote self-management behaviors, ultimately improving HRQoL.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the most prevalent chronic diseases in the elderly population. According to the World Health Organization, COPD ranks as the third leading cause of death worldwide (Zhang et al., 2023). In China, the prevalence of COPD has shown an upward trend over recent decades. It is estimated to have surpassed one million cases by 2019, with a significant rise associated with advancing age (Teng et al., 2023). Consequently, the global aging population, coupled with the increasing morbidity and mortality associated with COPD, is anticipated to impose substantial social and economic burdens on national healthcare systems, particularly in developing regions (Chen et al., 2022). Although classified as a non-communicable disorder, many COPD patients experience persistent yet partially reversible airflow restrictions and ongoing respiratory symptoms, such as productive phlegm, dyspnea, wheezing, and chronic cough (Labaki and Rosenberg, 2020), resulting in impaired lung function, reduced physical activity, and diminished health-related quality of life (HRQoL).
HRQoL is defined as a multidimensional self-reported evaluation of health, encompassing physical, psychological, and social domains. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) emphasizes that the hallmark symptoms of COPD lead to significant activity limitations and reduction in HRQoL (Halpin et al., 2021). Evidence suggests that HRQoL is inversely correlated with the disease burden experienced by COPD patients. Miravitlles and Ribera (2017) reviewed the impact of COPD symptoms on disease burden, highlighting that symptoms such as breathlessness, cough, and sputum production have adverse effects on health status and daily functioning, thereby increasing the risk of exacerbations (Miravitlles and Ribera, 2017). Another study investigated factors influencing HRQoL in COPD patients over a 5-year follow-up period. The findings revealed that pulmonary function, exercise capacity, and physical activity levels significantly influence HRQoL, suggesting that targeted interventions could enhance patient health outcomes (Esteban et al., 2020). Furthermore, elevated levels of emotional anxiety and distress perceived by COPD patients are associated with increased uncertainty and life dissatisfaction (Assaf et al., 2022). Collectively, these studies underscore the critical need to implement effective management strategies for COPD patients to promote overall health, reduce exacerbation frequency, manage symptoms, and consequently enhance HRQoL (Feldman, 2013).
Breathlessness, or dyspnea, is a core symptom of COPD, characterized by a sensation of air shortage and difficulty breathing. COPD patients’ beliefs about breathlessness, known as breathlessness beliefs or dyspnea-related fear of movement, are frequently associated with anxiety and fear. These beliefs can exacerbate the sensation of breathlessness and result in activity avoidance (Saka et al., 2021). According to the cognitive-behavioral model, an individual’s beliefs about their symptoms significantly influence their emotional and behavioral responses (Leonidou and Panayiotou, 2018). In the context of COPD, negative perceptions of breathlessness can heighten anxiety, discourage physical activity, and ultimately lead to a decline in HRQoL (Vaske et al., 2017). Studies suggest that breathlessness beliefs contribute to decreased physical activity levels among COPD patients, thereby initiating a vicious cycle of anxiety, depression, helplessness, and diminished HRQoL (De Peuter et al., 2011). Another research found that COPD patients with more negative beliefs about their breathlessness experienced greater HRQoL impairments, underscoring the necessity of addressing cognitive factors such as breathlessness beliefs in COPD care (Cappa et al., 2019). Recent findings indicate that breathlessness beliefs adversely impact the HRQoL of male COPD patients, particularly through impairing physical functioning (Bayraktar et al., 2023). However, the mechanisms underlying the relationship between breathlessness beliefs and HRQoL in COPD patients remain largely unexplored.
Self-efficacy refers to an individual’s belief in their ability to effectively manage symptoms, adhere to treatment regimens, and address the physical and mental challenges associated with chronic illness (Chalfont et al., 2021). Higher levels of self-efficacy are associated with proactive health behaviors and improved disease outcomes, as outlined in Albert Bandura’s Social Cognitive Theory (Bandura, 2004). In COPD management, self-efficacy is a critical determinant of participation in exercise training, medication adherence, and symptom monitoring during pulmonary rehabilitation (Selzler et al., 2020). Evidence indicates that COPD patients with higher self-efficacy levels exhibit greater adherence to self-care activities, resulting in improved HRQoL (Clari et al., 2017). Andenæs et al. (2014) identified self-efficacy as a strong predictor of the mental health component of HRQoL in COPD patients (Andenæs et al., 2014). Furthermore, research indicates that COPD patients with stronger breathlessness beliefs are less physically active, as such negative beliefs can undermine self-efficacy and hinder participation in beneficial activities (Wang et al., 2023). These findings suggest that individuals with less negative breathlessness beliefs may better regulate their emotions, enhance their confidence, and facilitate adherence to long-term rehabilitation programs, thereby improving overall physical and mental well-being. Consequently, we hypothesized that self-efficacy mediated the relationship between breathlessness beliefs and HRQoL.
Effective behavioral adjustments and enhanced management skills are pivotal components of pulmonary rehabilitation in COPD management (Cameron-Tucker et al., 2014). Self-management involves the essential abilities and skills individuals require to foster health-related behaviors and manage their conditions within the context of their lives (Monninkhof et al., 2003). COPD-specific self-management programs currently encounter significant challenges and limitations that impede the promotion of patients’ HRQoL and health outcomes in clinical settings (Schrijver et al., 2022). Bringsvor et al. (2019) highlighted that critical self-management domains, such as constructive attitudes and emotional distress, were significantly associated with HRQoL, suggesting that addressing these areas can enhance patients’ HRQoL (Bringsvor et al., 2019). Clinical research has demonstrated the efficacy of self-management interventions in improving HRQoL and decreasing respiratory-related hospital admissions among COPD patients (Schrijver et al., 2022). Furthermore, COPD patients who participate in pulmonary rehabilitation are more likely to develop a deeper understanding of their breathlessness, leading to improved self-management strategies. This underscores the importance of addressing patients’ beliefs about breathlessness to enhance self-management practices (Gysels and Higginson, 2009). A meta-analysis further suggested that patients’ perceptions of breathlessness significantly influenced their self-management strategies (Clari et al., 2017). Therefore, we proposed the intermediary role of self-management in mediating the relationship between breathlessness beliefs and HRQoL.
Self-efficacy is theoretically regarded as a critical element of chronic disease management, enabling patients to acquire the skills necessary for effectively managing COPD in clinical settings (Yi et al., 2021). Prior literature has demonstrated that COPD-related symptoms, including fatigue, dyspnea, and emotional distress, can significantly diminish self-efficacy levels. Conversely, patients with high levels of self-efficacy are more likely to engage in behaviors that manage symptoms and enhance health outcomes (Giezeman et al., 2022). In other words, enhancing patients’ self-efficacy improves their confidence in managing their condition and facilitates behavioral modifications to achieve greater self-management competence (Simpson and Jones, 2013). In COPD management, elevated self-efficacy is associated with improved adherence to self-management practices, such as medication compliance, regular exercise, and symptom monitoring. A randomized controlled trial demonstrated that COPD patients who underwent motivational-interview-based self-management interventions exhibited significant improvements in self-efficacy compared to those receiving usual care. These findings suggest that targeted interventions can effectively enhance self-efficacy, leading to better self-management outcomes (Karaçar and Demirkıran, 2024). Consequently, enhanced self-confidence and a positive attitude toward disease recovery can aid in improving the self-management behaviors of COPD patients during their daily pulmonary rehabilitation. We proposed that self-efficacy and self-management serve as sequential mediators between dyspnea-related fear of movement and HRQoL in COPD patients.
Although evidence indicates that breathlessness beliefs contribute to reduced HRQoL, little is known about the mediating effects of self-efficacy and self-management behaviors in the relationship between breathlessness beliefs and HRQoL. To address these gaps, this study aimed to establish independent and chain mediation models to investigate the impact of breathlessness beliefs on HRQoL in COPD patients, specifically exploring the mediating roles of self-efficacy and self-management behaviors. In this framework (Figure 1), breathlessness beliefs were treated as the independent variable, HRQoL as the dependent variable, and self-efficacy and self-management behaviors as mediators. This study sought to provide valuable insights into developing tailored interventions for COPD patients. The following hypotheses were proposed:
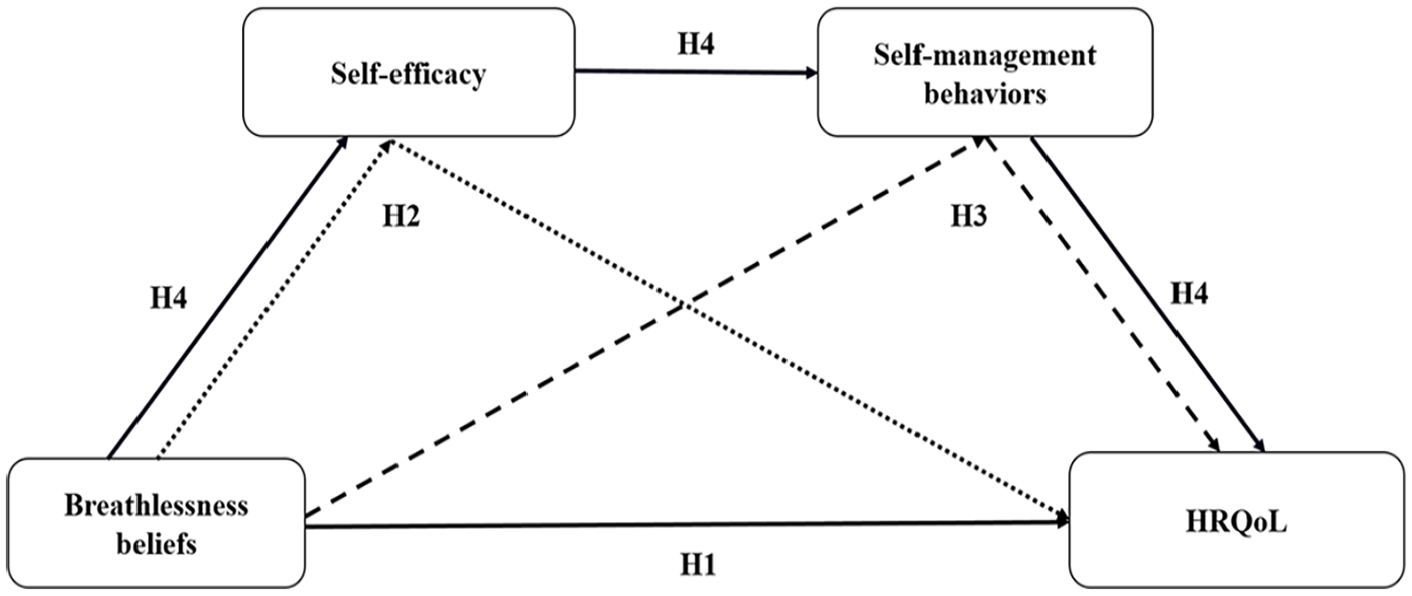
Theoretical mediation model for COPD patients. Abbreviations: COPD, chronic obstructive pulmonary disease; HRQoL, health-related quality of life. H, Hypothesis.
Methods
Procedure and participants
This cross-sectional study recruited a convenience sample of 310 COPD patients from three tertiary hospitals affiliated to the First Hospital of China Medical University in Shenyang, China, between December 25, 2022 and November 10, 2023. The inclusion criteria were: (1) diagnosed with COPD according to the GOLD guidelines (Vestbo et al., 2013); (2) aged at least 18 years; (3) in stable condition without COPD exacerbation for more than one month; (4) clear consciousness and proficiency in reading, speaking, and writing in Chinese to complete the survey; (5) voluntary participation in this study and provision of informed consent. The exclusion criteria were: (1) having life-threatening diseases such as liver, heart, or kidney injury, or malignant tumors; (2) severe mental disorders or cognitive impairment; (3) pregnancy or lactation; (4) co-occurrence of other chronic respiratory disorders such as asthma, bronchiectasis, and tuberculosis.
Sample size
The minimum sample size required for this study was calculated as 5 to 10 times the number of variables (Zimmer et al., 2023). Considering 14 demographic and clinical factors and nine dimensions of measurement instruments included in this study, the minimum required sample size was determined to be 144, accounting for a 20% dropout rate. Ultimately, 310 eligible participants were recruited, and 287 successfully completed the survey, yielding a valid response rate of 92.58% (Figure 2).
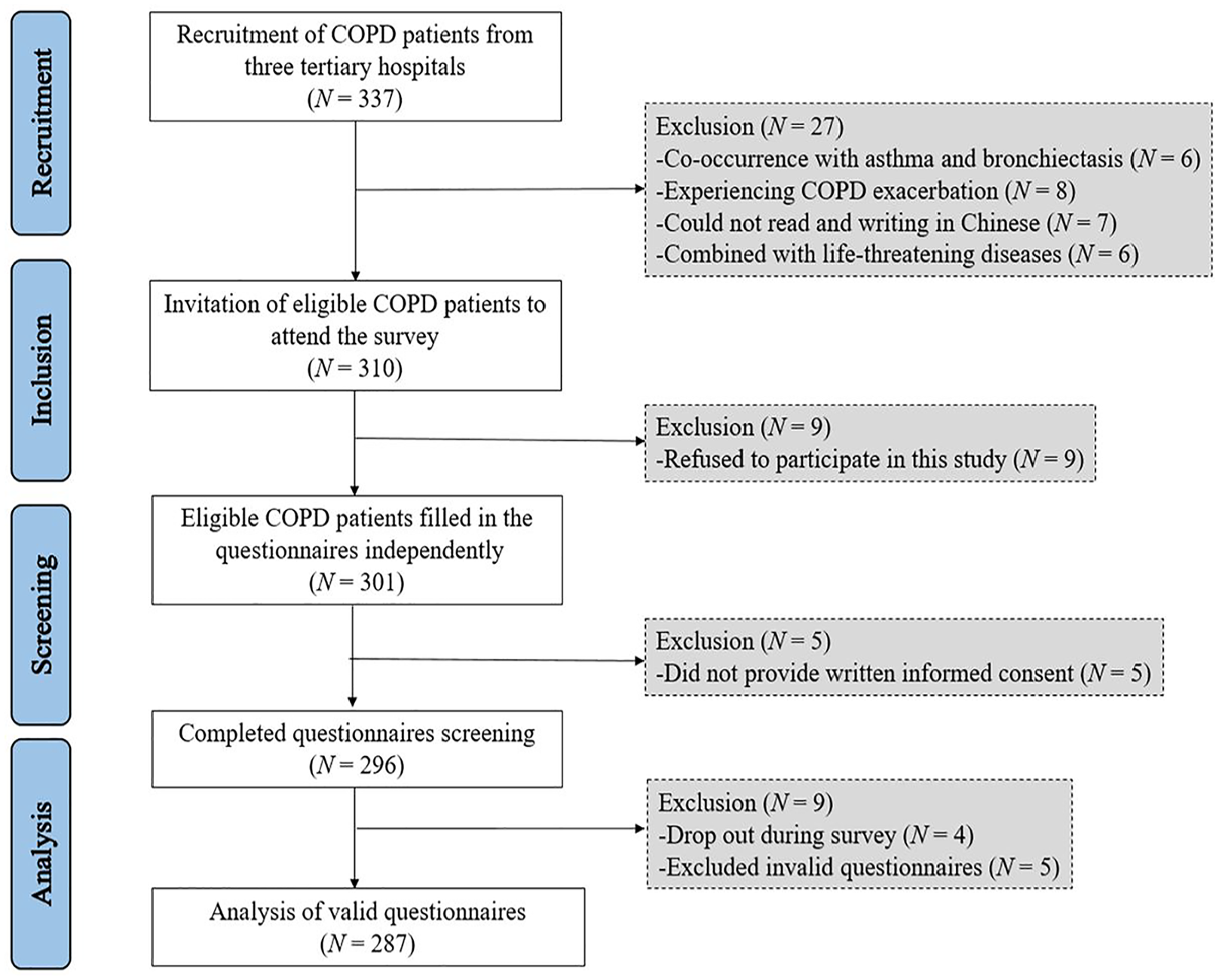
Flow diagram of the participants. Abbreviations: COPD, chronic obstructive pulmonary disease.
Data collection
Prior to the survey, investigators underwent training on standardized instruction protocols. Eligible participants were invited to a private room within the Respiratory Outpatient Department. Before the study, participants were briefed on the study’s objective and the informed consent procedures. After providing the written consent form, participants independently completed the self-reported questionnaires. During the survey, if participants encountered difficulties with the questionnaire, investigators provided assistance in understanding each item but ensured that no suggestive input was given. Participants took an average of 30 min to complete the survey. Completed questionnaires were collected immediately on-site and promptly reviewed by investigators to ensure completeness. Data handling strictly adhered to principles of confidentiality and anonymization.
Measurement
Demographic data
Socio-demographic and clinical characteristics were collected using a self-reported questionnaire, which included variables such as age, gender, body mass index (BMI), residence, educational level, marital status, employment status, smoking status, disease duration, severity of dyspnea, GOLD stage, hypertension, coronary heart disease, and diabetes.
Modified medical research council (mMRC) scale
The severity of dyspnea among COPD patients was assessed using the Modified Medical Research Council (mMRC) Scale, which is widely used in Chinese research to evaluate the impact of breathlessness on patients’ daily activities. The mMRC is a one-dimensional scale with five grades, ranging from 0 (no breathlessness) to 4 (severe breathlessness). An mMRC score ≥ 2 indicates persistent breathlessness (Lu et al., 2022).
Breathlessness belief questionnaire (BBQ)
The Chinese version of the Breathlessness Belief Questionnaire (BBQ), derived from the Tampa Scale for Kinesiophobia, was used to evaluate beliefs regarding breathlessness among COPD patients (Wu et al., 2018). The BBQ comprises 11 items and 2 dimensions: activity avoidance (6 items) and fear of dyspnea (5 items). Each item is rated on a 5-point Likert scale, ranging from 1 (totally disagree) to 5 (totally agree). The total score ranges from 11 to 55 point, with higher scores indicating stronger fear of dyspnea. In this study, the Cronbach’s α coefficient for the BBQ was 0.914.
General self-efficacy scale (GSES)
The General Self-Efficacy Scale (GSES) was employed to assess individuals’ self-efficacy. The Chinese version of the GSES, recognized for its good validity and reliability, has been widely adopted in Chinese populations (Wang et al., 2001). It comprises 10 items designed to evaluate individuals’ beliefs about their competence in coping with challenges, using a 4-point Likert scale. Each item is rated from 1 (totally wrong) to 4 (totally correct), with a total score of 10-40. Higher total scores indicate greater self-efficacy, with scores of 10-20 indicating low self-efficacy; 21-30 indicating medium self-efficacy; and 31-40 indicating high self-efficacy. In this study, the Cronbach’s α coefficient for the GSES was 0.866.
Self-management scale (SMS)
Self-management behaviors were assessed using the Self-Management Scale (SMS) derived from the Stanford Chronic Disease Self-Management Program (Lorig et al., 1999). The SMS consists of 15 items and is divided into 3 dimensions: exercise frequency in the last week (6 items), communication with doctors about their conditions (3 items), and cognitive management of disease-related physical discomfort (6 items). Exercise frequency is rated on a 5-point Likert scale, ranging from 0 (never) to 4 (>3 h), while communication with doctors and cognitive disease management is rated on a 6-point Likert scale, from 0 (never) to 5 (always). The total score ranges from 0 to 69, with higher scores indicating better self-management behaviors. The Chinese version has demonstrated good reliability and validity among Chinese patients with chronic disorders (Lan et al., 2022). In this study, the overall Cronbach’s α coefficient for the SMS was 0.921.
COPD assessment test (CAT)
The COPD Assessment Test (CAT), developed by Jones et al. (Jones et al., 2009), was used to measure the impact of COPD on disease-specific HRQoL. The unidimensional CAT includes 8 items assessing cough, sputum, chest tightness, sleep, energy, mood, exercise endurance, and daily activities. Each item is scored on a scale from 0 (best) to 5 (worst). The total score ranges from 0 to 40, with 0–10 indicating minor impacts, 11–20 indicating moderate impacts, 21–30 indicating severe impacts, and 31–40 indicating very severe impacts. A higher CAT score indicates poorer health status. The CAT has shown satisfactory reliability and validity among Chinese populations (Liu et al., 2023). In this study, the Cronbach’s α coefficient for the CAT was 0.860.
Ethical considerations
Ethics approval was granted by the Ethics Committee of the First Hospital of China Medical University (No. EC-2022-HS-262; date: December 20, 2022), and this study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Statistical analysis
All statistical analyses were conducted using SPSS software version 23.0. Continuous data with a normal distribution were expressed as mean ± standard deviation (SD), while categorical variables were described as frequency (%). Independent sample t-test and one-way ANOVA were performed to assess differences in basic characteristics among COPD patients concerning HRQoL scores. Pearson correlation analysis was employed to evaluate the relationships between variables. Hierarchical regression analysis was performed to identify predictive factors associated with HRQoL. Multicollinearity among variables was assessed using variance inflation factor (VIF) values (<10) and tolerance values (>0.2) (Al-Ashkar et al., 2021). Amos software version 24.0 was used to construct the structural equation model (SEM), and the Bootstrap method with 5000 samples was employed to test the mediating effect. A 95% confidence interval (CI) that excluded zero was considered statistically significant. The confirmatory factor analysis (CFA) of SEM demonstrated good construct validity if χ2/df < 5, Comparative Fit Index (CFI) ≥ 0.90, Incremental Fit Index (IFI) ≥ 0.90, Tucker Lewis Index (TLI) ≥ 0.90, Root Mean Square Error of Approximation (RMSEA) < 0.08, and Standardized Root Mean Square Residual (SRMR) < 0.08 (Hu and Bentler, 1999). Significant independent variables identified in the univariate analysis were included as covariates. A p-value < 0.05 (two-tailed) was considered statistically significant.
Results
Common method bias test
This study might be subject to common method bias due to the use of self-reported questionnaires for data collection. Harman’s single-factor test was applied to assess the presence of common method bias. The results revealed 5 factors with eigenvalues exceeding 1, with the first factor explaining 31.38% of the variance, which was below the 40% threshold. These findings suggested that the data analysis in this study was unlikely to be substantially affected by common method bias.
Demographic analysis
The sample consisted of 287 participants, with 166 (57.84%) males and 121 (42.16%) females. The mean age was 55.65 ± 7.74 years, ranging from 37 to 71 years. Further demographic and clinical details were presented in Table 1. Significant associations were observed between higher CAT scores and various demographic and clinical variables, including gender (p = 0.026), age (p = 0.014), advanced GOLD stage (p = 0.001), COPD duration (p = 0.008), severe dyspnea symptom (p = 0.001), and hypertension (p = 0.006) (Table 1). Therefore, these variables were incorporated as covariates in the subsequent regression and SEM analyses.
Demographic statistics and the influence on HRQoL (N = 287).
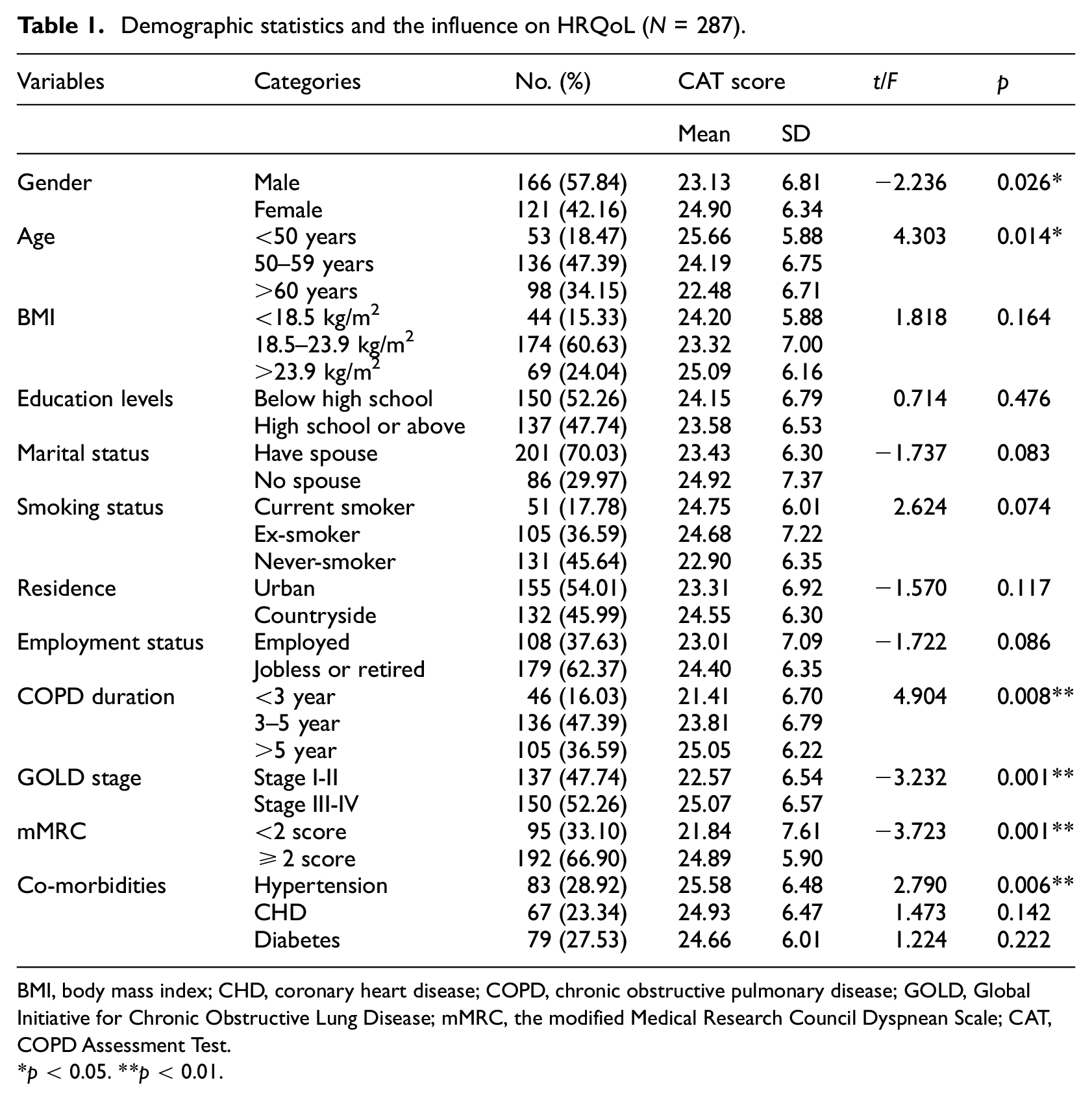
BMI, body mass index; CHD, coronary heart disease; COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; mMRC, the modified Medical Research Council Dyspnean Scale; CAT, COPD Assessment Test.
*p < 0.05. **p < 0.01.
Pearson correlation analysis
Table 2 presented the mean scores for breathlessness beliefs (31.04 ± 9.05), self-efficacy (23.76 ± 6.19), self-management behaviors (27.68 ± 14.04), and CAT (23.88 ± 6.66). Furthermore, the Pearson correlation analysis revealed that breathlessness beliefs were significantly negatively correlated with self-efficacy (r = −0.287, p < 0.01) and self-management behaviors (r = −0.325, p < 0.01), but positively correlated with CAT (r = 0.471, p < 0.01). In addition, CAT demonstrated significant negative associations with self-efficacy (r = −0.546, p < 0.01) and self-management behaviors (r = −0.540, p < 0.01). Moreover, a significant positive correlation was observed between self-efficacy and self-management behaviors (r = 0.353, p < 0.01) (Table 2).
Descriptive statistics and correlation analysis of variables (N = 287).
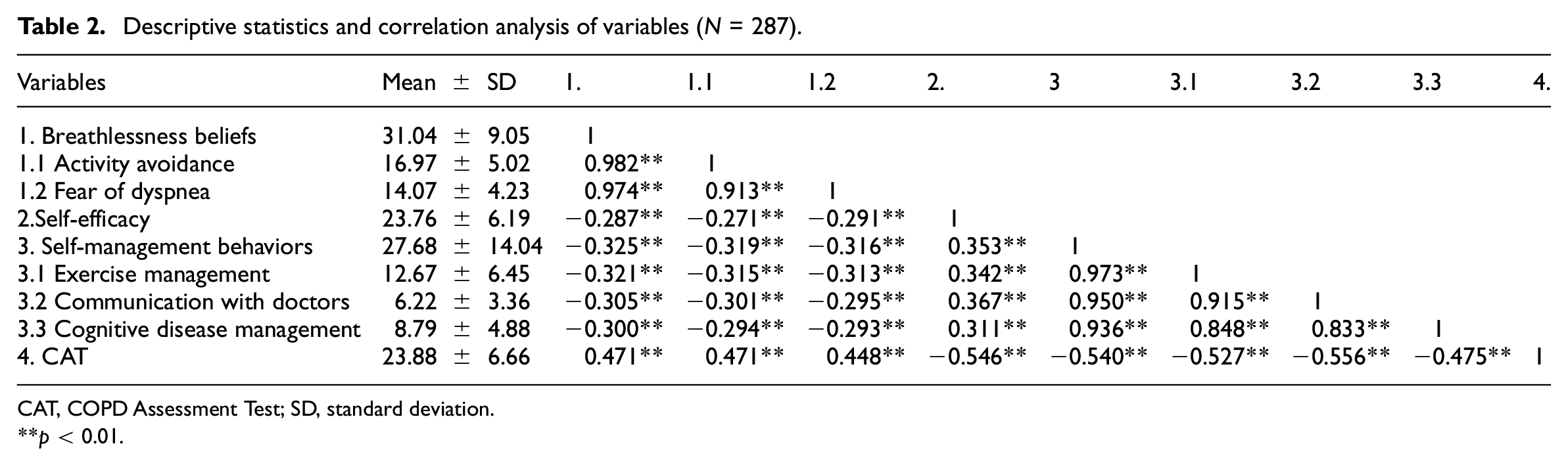
CAT, COPD Assessment Test; SD, standard deviation.
**p < 0.01.
Hierarchical multiple regression analysis
To identify predictive factors for HRQoL, a hierarchical multiple regression analysis was performed using the CAT score as the dependent variable. No multicollinearity issues were identified, as indicated by the VIF values (ranging from 1.005 to 1.243, all < 10) and tolerance values (ranging from 0.805 to 0.995, all > 0.2). As shown in Table 3, after adjustment for covariates (gender, age, COPD duration, GOLD stage, mMRC, and hypertension), Model 1 showed that these covariates explained 13.10% of the variance in CAT. When incorporating breathlessness beliefs into Model 2, breathlessness beliefs emerged as a significant positive predictor of CAT (β = 0.406, p < 0.001) and explained an additional 15.60% of the variance in CAT (△R2 = 0.156, F = 17.484, p < 0.001, Table 3). When incorporating self-efficacy into Model 3, the effect of breathlessness beliefs on CAT diminished from 0.406 to 0.291 and explained an additional 16.50% of the variance in CAT (△R2 = 0.165, F = 30.814, p < 0.001, Table 3). Additionally, when adding self-management behaviors into Model 4, self-management behaviors had a significant negative impact on CAT (β = −0.309, p < 0.001), and the final Model 4 explained 53.20% of the variance in CAT (△R2 = 0.077, F = 37.115, p < 0.001, Table 3). Moreover, the predictive effects of breathlessness beliefs and self-efficacy on CAT decreased from 0.291 to 0.222 and from −0.433 to −0.348, respectively (Table 3), indicating that self-efficacy and self-management might serve as potential mediators between breathlessness beliefs and HRQoL.
Multivariate linear regression analysis of influencing factors of CAT in COPD patients (N = 287).
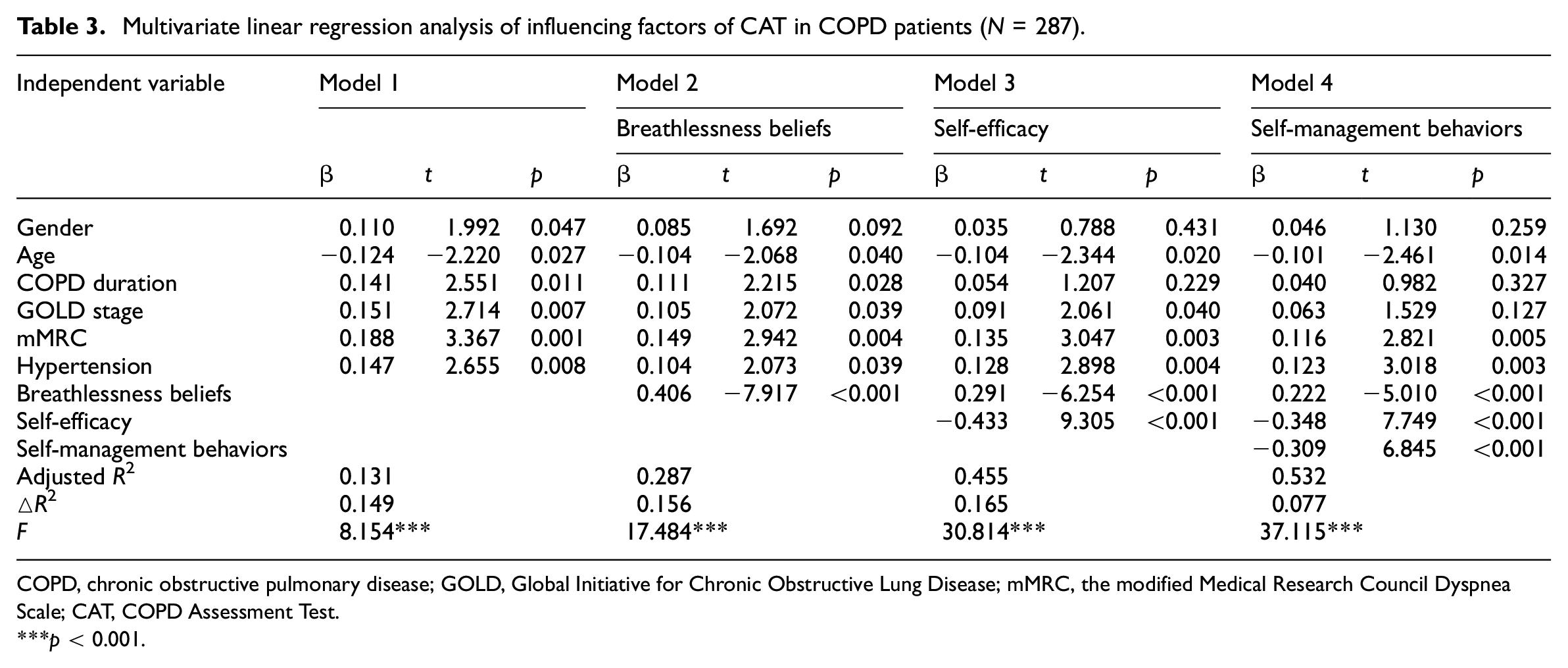
COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; mMRC, the modified Medical Research Council Dyspnea Scale; CAT, COPD Assessment Test.
***p < 0.001.
Mediation analyses
Next, SEM models were conducted using Amos 24.0 to evaluate the independent and chain–mediating effects of self-efficacy and self-management behaviors in the relationship between breathlessness beliefs and HRQoL. The model fit indices for the three mediation models fell within the acceptable ranges, indicating a good model fit (Supplemental Table S1).
The independent self-efficacy mediation model (Figure 3(a) and Table 4) showed a significant total effect of breathlessness beliefs on HRQoL (Effect size = 0.716, Bootstrap 95% CI = 0.484–0.924, p = 0.001) and self-efficacy was found to be a significant mediator in the relationship between breathlessness beliefs and HRQoL (Effect size = 0.207, Bootstrap 95% CI = 0.109–0.323, p < 0.001), accounting for 28.91% of the total effect. Furthermore, the independent self-management behaviors mediation model (Figure 3(b) and Table 4) also showed a significant total effect of breathlessness beliefs on HRQoL (Effect size = 0.721, Bootstrap 95% CI = 0.497–0.924, p = 0.001) and self-management behaviors were found to be a significant mediator in the relationship between breathlessness beliefs and HRQoL (Effect size = 0.238, Bootstrap 95% CI = 0.160–0.336, p < 0.001), accounting for 33.01% of the total effect. These findings highlighted the distinct independent mediating roles of self-efficacy and self-management behaviors in the relationship between breathlessness beliefs and HRQoL, respectively.
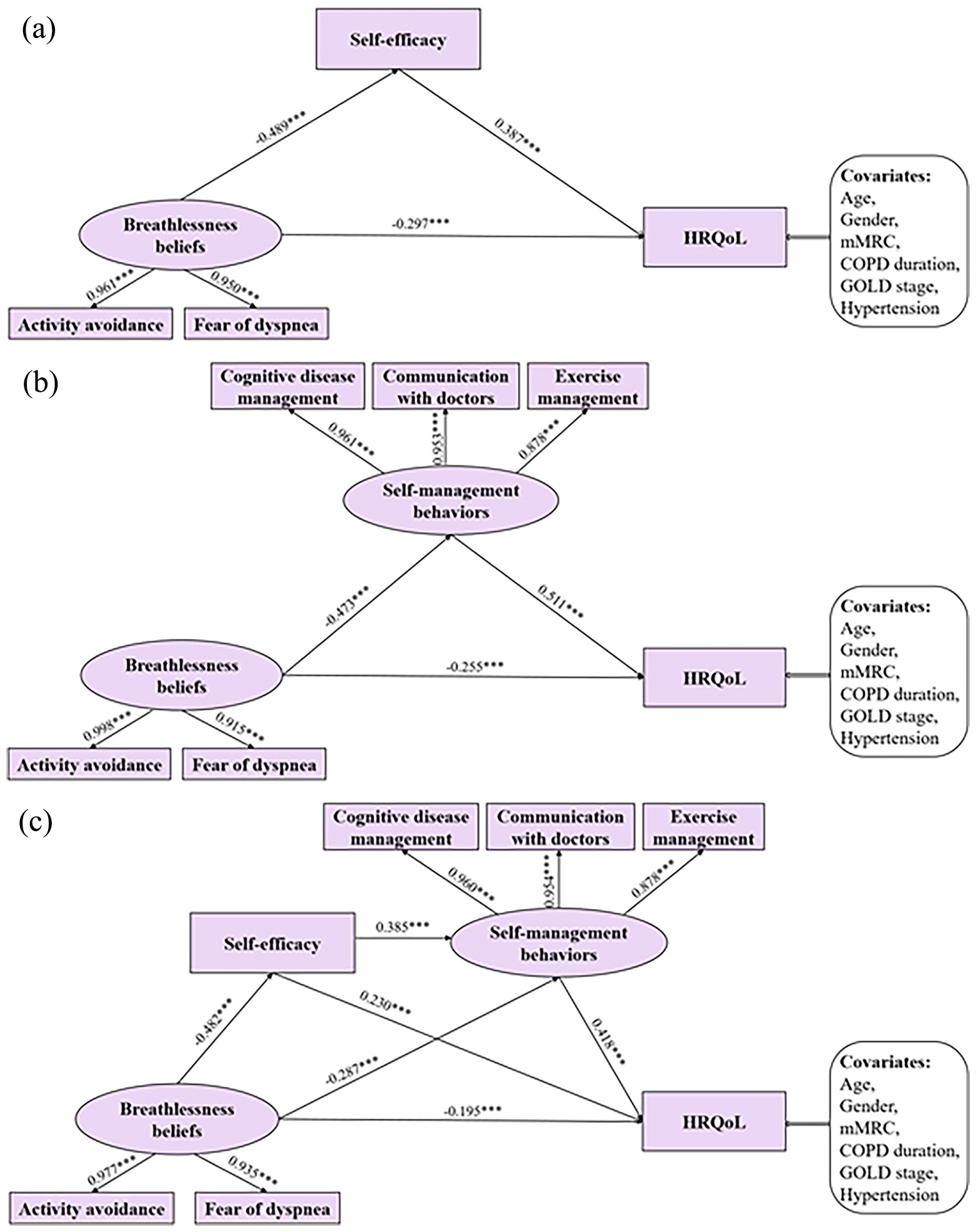
Structural equation model. (a) Independent mediation model of self-efficacy. (b) Independent mediation model of self-management behaviors. (c) Chain mediation model of self-efficacy and self-management behaviors in the relationship between the effects of breathlessness beliefs and HRQoL (N = 287). ***p < 0.001. Abbreviations: COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; mMRC, the modified Medical Research Council Dyspnea Scale; HRQoL, health-related quality of life.
Bootstrap analysis of mediating effect test.
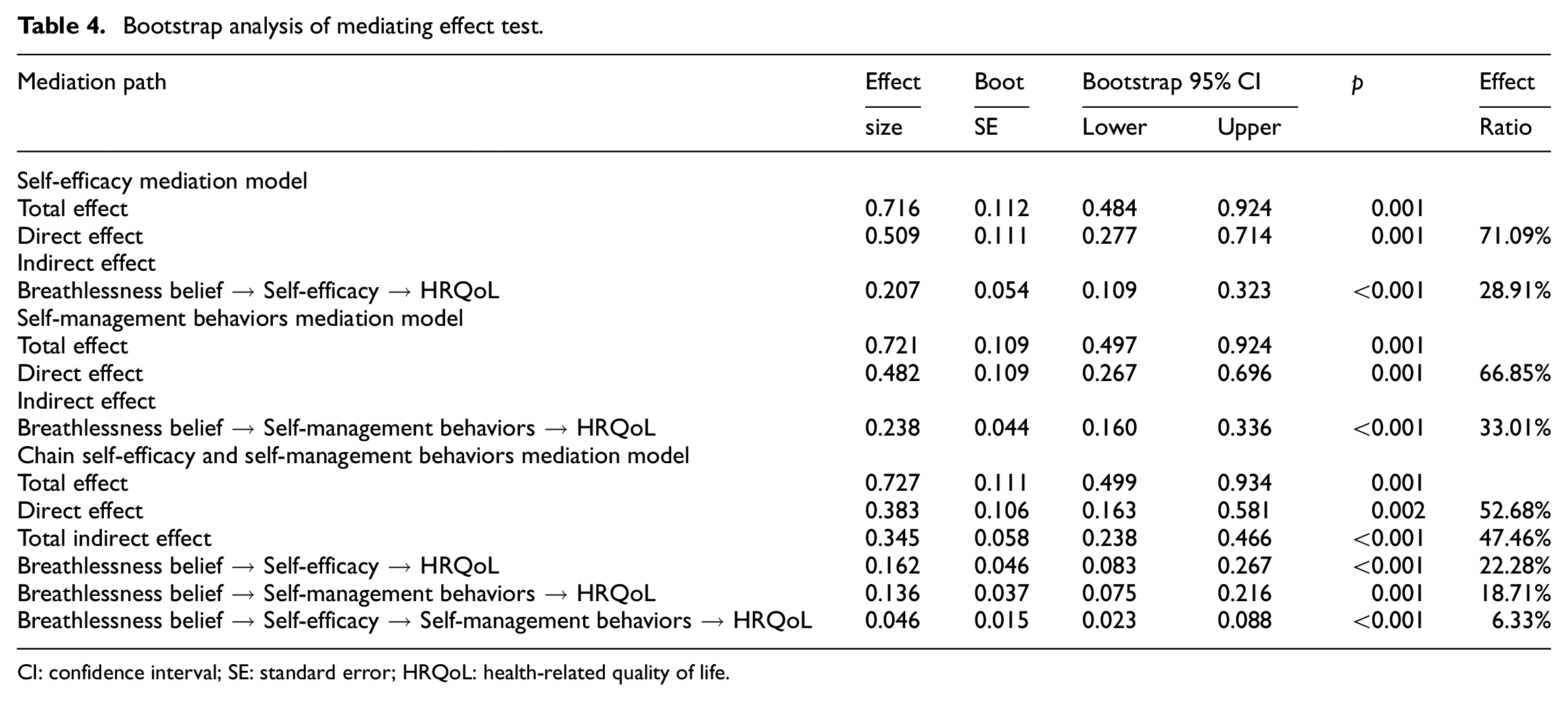
CI: confidence interval; SE: standard error; HRQoL: health-related quality of life.
To further explore the chain mediating effect of self-efficacy and self-management in the relationship between breathlessness beliefs and HRQoL, a chain SEM was constructed (Figure 3(c) and Table 4). The Bootstrap method revealed that the total effect between breathlessness beliefs and HRQoL was 0.727 (Bootstrap 95% CI: 0.499–0.934, p = 0.001). The total indirect effect was estimated at 0.345 (Bootstrap 95% CI: 0.238–0.466, p < 0.001). Specifically, self-efficacy contributed an indirect effect size of 0.162 (Bootstrap 95% CI: 0.083–0.267, p < 0.001); self-management behaviors contributed 0.136 (Bootstrap 95% CI: 0.075–0.216, p = 0.001); and the combined chain-mediating effect of self-efficacy and self-management behaviors was 0.046 (Bootstrap 95% CI: 0.023−0.088, p < 0.001). These three indirect effects accounted for 22.28%, 18.71%, and 6.33% of the total effect, respectively. Thus, these results confirmed the significant chain mediating roles of self-efficacy and self-management behaviors in the relationship between of breathlessness belief and HRQoL.
Supplementary analysis
Given the equivocal predictive relationship between self-efficacy and self-management behaviors in prior studies, a reverse chain mediating model (breathlessness beliefs → self-management → self-efficacy → HRQoL) was developed to compare with the original hypothesized model (breathlessness beliefs → self-efficacy → self-management → HRQoL). While the two chain SEMs exhibited distinct path coefficients (Figure 3(c) and Supplemental Figure S1), they demonstrated equal goodness-of-fit (Supplemental Table S1), attributed to their identical overall model impact on model fit. To more rigorously investigate the potential mediation directionality between self-efficacy and self-management behaviors, supplementary analyses were conducted using the alternative chain SEM framework. Path analysis confirmed statistically significant effects across all paths (all p < 0.05) (Supplemental Figure S1). Bootstrap analysis indicated that the chain-mediating pathway (self-efficacy → self-management behaviors) demonstrated substantial clinical significance (Supplemental Table S2), providing robust support for its role in mediating the relationship between breathlessness beliefs and HRQoL.
Discussion
This study utilized a cross-sectional design to investigate the mechanisms underlying the association between breathlessness beliefs and HRQoL. To the best of our knowledge, this study is the first to demonstrate the independent and multiple mediating roles of self-efficacy and self-management behaviors in the relationship between breathlessness beliefs and HRQoL in COPD patients. The results indicated that breathlessness beliefs significantly and negatively influenced HRQoL via three primary pathways: (1) the independently mediating effect of self-efficacy, (2) the independent mediating effect of self-management behaviors, and (3) the serial-mediating effect of self-efficacy and self-management behaviors. These findings highlighted the potential of SEM-based strategies and interventions to aid COPD patients in effectively managing dyspnea symptoms and improving their HRQoL.
Reduced breathlessness beliefs significantly predicted better HRQoL
The results revealed a significant and negative effect of breathlessness beliefs on HRQoL among COPD patients (H1 was confirmed). This finding aligned with prior research, which demonstrated that dyspnea-related fear of movement was negatively associated with HRQoL in a study of 70 COPD patients in Turkey (Bayraktar et al., 2023). Research has shown that breathlessness beliefs are prevalent among COPD patients and can affect their emotional state as well as influence their adherence to pulmonary rehabilitation, leading to decreased participation in daily pulmonary rehabilitation programs (Yang et al., 2020). Consequently, decreased physical exercise due to dyspnea-related fear of movement contributes to diminished pulmonary function, delayed disease recovery, prolonged disease duration, and poorer HRQoL (Liang et al., 2023). Targeted rehabilitation programs are recommended to address patients’ breathlessness beliefs during the rehabilitation process. A randomized controlled trial demonstrated that an 8-week inspiratory muscle training program could effectively alleviate COPD patients’ breathlessness beliefs, improve respiratory function, and enhance HRQoL (Saka et al., 2021). Thus, addressing breathlessness beliefs offers a promising strategy for improving health outcomes in COPD patients experiencing poor HRQoL.
Mediating effect of self-efficacy
The present study revealed that self-efficacy mediated the relationship between breathlessness beliefs and HRQoL in COPD patients. Breathlessness beliefs were found to be negatively associated with self-efficacy, whereas self-efficacy positively correlated with HRQoL. This finding confirmed H2. This suggested that COPD patients with strong breathlessness beliefs might face difficulties adhering to pulmonary rehabilitation programs due to a loss of confidence in their ability to exercise, consistent with previous studies (Liu et al., 2021; Zelle et al., 2016). Breathlessness beliefs, including dyspnea-related fear of movement and activity avoidance, influence COPD patients’ perceptions of their ability to manage symptoms. This, in turn, creates doubts about their ability to achieve daily physical activity goals, thereby undermining self-efficacy. Conversely, extensive evidence suggests that individuals with higher preactional self-efficacy are more confident in their ability to achieve positive outcomes, which subsequently motivates them to engage in healthier behaviors (Wechsler et al., 2022). Chronic breathlessness beliefs and stress may reduce self-efficacy and hinder rehabilitation adherence. However, healthcare providers can boost patients’ self-efficacy through strategies such as verbal persuasion, performance achievements, physiological feedback, and observational learning (Bandura, 1977). Recognizing the critical influence of self-efficacy on HRQoL in COPD patients, pulmonary rehabilitation programs that emphasize emotional support and building exercise confidence are recommended to improve patients’ health outcomes (Bamonti et al., 2023).
Mediating role of self-management behaviors
The current study demonstrated that self-management behaviors mediated the relationship between breathlessness beliefs and HRQoL in COPD patients. Specifically, COPD patients with stronger breathlessness beliefs are more likely to exhibit inadequate self-management behaviors, subsequently resulting in diminished HRQoL. This observation confirmed H3. COPD-specific self-management practices, such as early recognition of exacerbation, maintaining healthy diets, adhering to medical compliance, quitting smoking, and engaging in regular exercise training, are critical for managing sudden changes in COPD symptoms (Cravo et al., 2022). Previous research indicates that panic, fear, and anxiety induced by dyspnea in COPD patients may lead to procrastination, reduced physical activity, and reluctance to modify health-related behaviors, such as quitting smoking or engaging in rehabilitation programs (Gardiner et al., 2010). Consistent with these findings, our study confirmed a negative correlation between breathlessness beliefs and self-management behaviors in COPD patients. When COPD patients receive appropriate education and acquire necessary self-management skills, they are better equipped to manage dyspnea symptoms, alleviate persistent fear of breathlessness, and address energy deficits associated with disease progression (Sigurgeirsdottir et al., 2019). Furthermore, a recent meta-analysis supports the notion that adequate self-management support reduces dyspnea-related distress and improves HRQoL in COPD patients by bolstering confidence in adhering to physical exercise regimens and managing symptoms effectively (Jolly et al., 2016). Therefore, identifying the specific needs of COPD patients and providing tailored strategies can foster confidence and resilience, empowering individuals to manage their condition more effectively and independently.
Chain mediating role of self-efficacy and self-management behaviors
The study demonstrated that self-efficacy and self-management behaviors acted as sequential mediators in the relationship between breathlessness beliefs and HRQoL among COPD patients, with self-efficacy positively correlating with self-management behaviors. This observation confirmed H4, indicating that enhancing self-efficacy may foster self-management behaviors, ultimately improving HRQoL in this population. These findings aligned with Katch and Mead (Katch and Mead, 2010), who emphasized the critical role of self-efficacy in empowering patients to manage chronic conditions. COPD patients frequently experience elevated levels of anxiety, distress, fatigue, and dyspnea-related fear, contributing to increased exacerbations, hospital readmissions, and diminished confidence in their ability to recover, all of which hinder effective disease management. Consequently, mitigating breathlessness beliefs may enable COPD patients to regain motivation and adopt proactive self-management strategies. This process likely involves targeted education to improve disease-related knowledge, refine self-management skills, and encourage adherence to structured exercise training (Zhou and Li, 2020). Similarly, prior studies have established self-efficacy as a critical determinant of self-management behaviors among patients with chronic diseases (Do et al., 2015; Yao et al., 2019). Importantly, our study also revealed a significant sequential mediating pathway linking self-management behaviors to self-efficacy, highlighting their synergistic roles as critical mediators bridging breathlessness beliefs and HRQoL. To proactively cope with breathlessness-related fear, COPD patients should be supported in engaging with pulmonary rehabilitation programs to develop self-management competencies, thereby fostering intrinsic motivation, self-confidence, and HRQoL. Prior research supports this approach, demonstrating that structured self-management interventions enhance self-efficacy and improve clinical outcomes in chronic disease populations (Schulman-Green et al., 2012). Therefore, multifaceted interventions that integrate self-efficacy enhancement strategies with evidence-based self-management programs warrant prioritization in COPD care frameworks to optimize clinical outcomes.
Practical implications
This study offers valuable insights into strategies aimed at improving HRQoL among COPD patients. Notably, breathlessness beliefs exert a significant direct influence on HRQoL deterioration. Consequently, healthcare practitioners should prioritize mitigating breathlessness-related fear and emotional distress in COPD patients. Integrating psychological counseling and family-based interventions are recommended to provide multidisciplinary support, empowering patients to regulate distressing emotions and reduce dyspnea-associated avoidance behaviors. Given that breathlessness beliefs influence HRQoL through independent and sequential mediation by self-efficacy and self-management behaviors, these variables must be recognized as pivotal determinants of HRQoL outcomes in COPD populations. Implementing integrated interventions that dual-target both self-efficacy and self-management behaviors may amplify synergistic benefits, including improved rehabilitation engagement and sustained self-care practices (Subramanian et al., 2020). For example, clinicians could establish patient-specific rehabilitation goals paired with tailored behavioral strategies, such as motivational interviewing complemented by structured positive reinforcement, to optimize adherence to physical activity regimens (Kivelä et al., 2014). Additionally, clinicians should develop personalized COPD symptom management plans, implement evidence-based educational programs to improve health literacy, and leverage digital health technologies (e.g., mobile applications or telehealth platforms) for real-time symptom and medication adherence tracking. Integrating peer-led support groups and patient-expert collaborations into the care framework may foster experiential knowledge-sharing, reinforce self-efficacy, sustain self-management adherence, and mitigate the detrimental impact of breathlessness beliefs on HRQoL.
Limitations
Several limitations of this study deserve attention. First, the cross-sectional design of this study prevents establishing causal relationships among the variables. Longitudinal studies are needed to elucidate the influence of breathlessness beliefs on HRQoL. Second, participants were recruited solely from Shenyang city in Northeastern China, potentially limiting the generalizability of the findings. Future studies should aim to recruit participants from diverse geographical regions and populations to enhance generalizability. Third, the self-reported questionnaires may introduce measurement error and bias. Incorporating detailed face-to-face interviews to assess both physical and mental status is recommended to enhance the validity of future research. Fourth, this study focused solely on the psychological perceptions of breathlessness in the simple and chain-mediation models. Further studies should incorporate additional crucial pathological variables in COPD, such as the severity of dyspnea, pulmonary function, and COPD stage, to develop more comprehensive mediation models that can more accurately predict HRQoL.
Conclusion
This study demonstrated that breathlessness beliefs significantly and directly predicted poor HRQoL among COPD patients. Self-efficacy and self-management behaviors served as critical mediators in the relationship between breathlessness beliefs and HRQoL, operating through three mediating pathways: the independent mediating effect of self-efficacy, the independent mediating effect of self-management behaviors, and the serial-mediating effect of both. The chain-mediation model established in this study offers robust evidence to support strategies aimed at improving HRQoL in COPD patients experiencing dyspnea-induced fear of movement in clinical settings. Healthcare services are encouraged to adopt tailored interventions to enhance self-efficacy and self-management behaviors, with the objective of improving HRQoL by mitigating dyspnea-related movement fears.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251331940 – Supplemental material for Effect of breathlessness beliefs on quality of life in chronic obstructive pulmonary disease: Chain-mediating role of self-efficacy and self-management behaviors
Supplemental material, sj-docx-1-hpq-10.1177_13591053251331940 for Effect of breathlessness beliefs on quality of life in chronic obstructive pulmonary disease: Chain-mediating role of self-efficacy and self-management behaviors by Lin Wang, Qiuli Li and Naiwen Jiang in Journal of Health Psychology
Footnotes
Acknowledgements
The authors thank all the patients who voluntarily participated in this study.
Authors’ contributions
Lin Wang and Qiuli Li performed conceptualization, methodology, investigation, Software, data collection, and data analysis; Lin Wang was responsible for writing-original draft; Naiwen Jiang performed conceptualization, methodology, supervision, validation, and writing-review & editing. All authors reviewed and approved the final manuscript.
Data availability statement
The data of the study is available from the corresponding author upon reasonable request. The data are not publicly available due to privacy or ethical restrictions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethics approval was obtained from the Ethics Committee of the First Hospital of China Medical University (No. EC-2022-HS-262, Date: December 20, 2022) and in accordance with the Declaration of Helsinki.
Informed consent
Written informed consent was obtained from all participants before the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.