
Abstract
Irritable bowel syndrome (IBS) is a chronic gastrointestinal disorder that imposes significant life impairment. Smoking is an addictive and potentially exacerbating behavior that may be important to IBS, but the psychological factors linking IBS and smoking remain underexplored. This study aims to investigate gastrointestinal-specific anxiety (GI-specific anxiety) in relation to smoking processes among adults with IBS who smoke. The sample consisted of 263 adults who met the criteria for IBS and reported smoking at least 5 cigarettes per day for the past year (Mean age = 44.1 years, SD = 12.71, 52.1% female). Hierarchical regression results indicated that higher GI-specific anxiety was statistically significantly associated with greater perceived barriers for smoking cessation, increased negative affect reduction smoking expectancies, and stronger urges to smoke for relief of negative affect. The present investigation found that GI-specific anxiety is an important construct informing smoking among individuals with IBS. Future research considerations are explored.
Keywords
Irritable bowel syndrome (IBS) is a chronic gastrointestinal (GI) disorder characterized by abdominal pain and altered bowel habits (e.g. constipation or diarrhea) without any identifiable biomarker (Drossman and Hasler, 2016). IBS affects 10%–15% of the global population, with significant variability in symptom presentation and severity (Ford et al., 2017). The severity of GI symptoms prompts many more severely-affected individuals with IBS to seek medical care (Ford et al., 2018). The impact of IBS is profound from a public health perspective, leading to reduced quality of life, increased psychological distress, and substantial economic costs (Buono et al., 2017; Canavan et al., 2014). The medical management of IBS is challenging due to the lack of a satisfactory medical therapy, often resulting in a chronic course of illness (Camilleri, 2021; Simrén et al., 2017).
Lifestyle and health behaviors are implicated in the etiology and progression of IBS (Jha et al., 2013). Although diet and physical activity have been among the most studied health behaviors in terms of IBS (Ho et al., 2024), there is a growing recognition that addictive behaviors may also influence the course of illness (Bakhshaie et al., 2024). Combustible cigarette smoking (hereafter smoking) is a prevalent addictive behavior that may be important to IBS (Al Saadi et al., 2016; Başpınar and Basat, 2022; Burns, 1986; Farzaneh et al., 2013). Some research indicates that among individuals who smoke, prevalence of cigarette dependence is higher among those with IBS compared to those without IBS (Başpınar and Basat, 2022). Smoking is also associated with an increased risk of GI symptoms, including those characteristic of IBS (Gudleski et al., 2017; Halpin and Ford, 2012). Furthermore, successful smoking cessation has been linked to a decrease in the severity of IBS symptoms (Başpınar and Basat, 2022). Among health behaviors, smoking has been found to have a particularly strong impact on IBS, as it not only contributes to GI symptom exacerbation but is also uniquely tied to negative reinforcement processes that maintain both smoking and IBS distress (Zvolensky et al., 2017). Although other substances, such as alcohol use and misuse, have been explored in relation to IBS, smoking is particularly relevant due to its acute physiological effects on the gut (e.g. altered motility and inflammation; Chang et al., 2014) and its role as a maladaptive coping mechanism for GI-specific anxiety (Zvolensky et al., 2017). Psychological distress associated with both IBS and smoking can theoretically elicit a forward feedback cycle, whereby smoking is used as a coping mechanism for managing IBS symptoms (in the context of nicotine’s acute analgesic and mood modulating effects; Ditre et al., 2016), but such behavior can exacerbate IBS symptoms over time (Chang et al., 2014). However, there has been highly limited empirical study of individual difference factors related to smoking among persons with IBS.
One individual difference factor that may influence smoking among persons with IBS is GI-specific anxiety. GI-specific anxiety refers to heightened sensitivity and anxiety related to GI sensations (Labus et al., 2004). GI-specific anxiety exacerbates IBS symptoms (Sibelli et al., 2017). For instance, higher levels of GI-specific anxiety are associated with greater IBS symptom severity and poorer quality of life among persons with IBS (Hazlett-Stevens et al., 2003; Lackner et al., 2014). Another line of research implicates GI-specific anxiety as a risk factor for cigarette dependence and abstinence-related worry in the general population via negative reinforcement processes (Zvolensky et al., 2017). However, no work has integrated these two lines of research by evaluating GI-specific anxiety among adults with IBS who smoke. To the extent elevated levels of GI-specific anxiety enhances somatic perturbation among persons with IBS (Farzaei et al., 2016), it may serve as a transdiagnostic mechanism tied to both GI symptoms and emotion regulatory smoking functions (Kauffman et al., 2024). Thus, persons with IBS who smoke with higher levels of GI-specific anxiety may be more likely to perceive greater barriers for quitting, expect smoking to alleviate aversive internal states, and be motivated to smoke for negative affect reduction reasons.
The present study examined GI-specific anxiety in terms of several clinically significant processes among adults with IBS who smoke. Specifically, it was hypothesized that GI-specific anxiety would be associated with expectancies for negative affect reduction, perceived barriers for smoking cessation, and urge to smoke related to reduction of negative affect. Each of these smoking constructs is related to the maintenance and relapse of smoking and involve negative reinforcement processes (Farris et al., 2014; Milcarz et al., 2019; Robinson et al., 2012). The hypothesized effects were expected in adjusted models that accounted for the variance explained by cigarette dependence (Başpınar and Basat, 2022), sex (Smith et al., 2016), education (Tenn et al., 2010), and depressive symptoms (Mendelsohn, 2012).
Method
Procedure
A nationally representative sample was recruited from across the United States using Qualtrics Panels, an online survey management system. The study name and inclusion/exclusion criteria were listed in the Qualtrics Panels Management system and adults were able to self-select into the study if they believed they may be eligible. Participants who self-selected into the study first completed a brief eligibility screener survey. Participants deemed eligible were asked to provide informed consent and were directed to the study survey. Participants could opt to receive the equivalent of $10.75 in compensation via cash-based incentives (i.e. gift cards), reward miles, or reward points. To ensure quality responses, a speeding check (i.e. one-half the median survey completion time) was included and IP addresses were recorded to prevent multiple attempts to complete the survey by the same respondent. The study was approved by the Institutional Review Board of the university where the study took place.
A total of 2858 individuals responded to the study advertisement, of whom 2141 were excluded because they did not meet self-reported Rome IV criteria for IBS (Palsson et al., 2016), 181 were excluded because they reported smoking less than five cigarettes per day, 84 were excluded because they did not meet the age criteria, and 189 were excluded because they did not pass data quality checks.
Participants
A total of 263 (52.1% female; mean age =44.1 years, SD = 12.71) adults who met criteria for IBS and reported smoking at least 5 cigarettes per day were included. Inclusion criteria was as follows: (1) being between the ages of 18 and 75, (2) endorsing current daily smoking (≥5 cigarettes per day), (3) meeting criteria for IBS based on self-reported symptoms on the Rome IV Diagnostic Questionnaire for IBS (i.e. recurrent abdominal pain occurring at least weekly; at least two of the following at least 30% of occasions: pain related to defecation, pain associated with a change in frequency of stool, pain associated with a change in the appearance of stool; and symptom onset at least 6 months ago; Drossman and Hasler, 2016), and (4) having access to a computer or mobile device (to ensure ability to complete the study survey). Exclusion criteria included: (1) an inability to complete self-report surveys, (2) lack of proficiency in English (to ensure comprehension of survey items), and (3) an inability to provide voluntary informed consent.
Measures
Demographics
Demographic information collected included sex, age, sexual orientation, gender, race, ethnicity, annual income, and highest level of education. Sex and age were included as covariates.
Chronic pain conditions
The Chronic Overlapping Pain Conditions Screener (COPCS; Schrepf et al., 2024) is designed to identify the presence of nociplastic pain conditions that frequently co-occur in an individual. Respondents are presented with a body map and asked to indicate areas in which they experience chronic pain. Based on the indicated area(s), they respond to a series of diagnostic questions corresponding to a relevant pain condition (i.e. if an individual marks jaw pain on the body map, they will be presented with questions corresponding to the criteria for temporomandibular disorder [TMD]). As the COPCS provides a comprehensive assessment of 10 different chronic pain conditions, it was used in this study to describe the sample in terms of reporting prevalence of specific pain conditions, including but not limited to TMD, IBS, and fibromyalgia (FM).
Smoking history
The Smoking History Questionnaire (SHQ; Brown et al., 2002) is used to measure history of smoking, including age of onset, products used, quit attempts. In the current study, the SHQ was used to describe smoking history.
Cigarette dependence
The Fagerström Test for Cigarette Dependence-Revised (FTCD-R; Korte et al., 2013) is a 6-item self-report measure of cigarette dependence. Items on the FTCD-R vary in scale and grading (e.g. “What cigarette would you most hate to give up? 1 = first in the morning, 0 = all others” and “How soon after you wake up do you have your first cigarette? 3 = within 5 minutes, 2 = 6–30 minutes, 1 = 21–30 minutes, 0 = after 60 minutes”). All items are summed for a total score and higher scores indicate a greater degree of cigarette dependence. In the current study, the FTCD-R was utilized in descriptive analyses and as a covariate in primary analyses (Cronbach’s alpha = 0.51), indicating low internal consistency, which is expected given the scale’s focus on descriptive smoking behavior rather than a unidimensional construct (Berlin et al., 2016).
IBS symptom severity
The IBS Symptom Severity Scale (IBS-SSS; Francis et al., 1997) was utilized to assess the degree to which individuals experience gastrointestinal symptoms (0–500 scale, ≥300 = Severe). This 5-item scale evaluates pain, distension, bowel dysfunction, dissatisfaction with bowel habits, and interference with quality of life, classifying respondents’ symptoms as mild, moderate, or severe. In the current study, IBS symptom severity was used in descriptive analyses to characterize the sample (Cronbach’s alpha = 0.82), indicating good internal consistency.
Depressive symptoms
The Overall Depression Symptom and Impairment Scale (ODSIS) is a 5-item self-report measure assessing symptoms and functional impairment associated with depressive symptoms (Bentley et al., 2014). Items of the ODSIS are summed to create total score ranging from 0 to 25; higher scores indicate more severe symptoms and impairment. The ODSIS has shown strong convergent and discriminant validity across both clinical and non-clinical samples and demonstrates measurement invariance across diverse samples (Ito et al., 2015). The ODSIS total score was utilized to identify individuals in the sample who met criteria for likely depression. The ODSIS evidenced excellent internal reliability in the current sample (Cronbach’s alpha = 0.95).
GI-specific anxiety
The Visceral Sensitivity Index (VSI; Labus et al., 2004) is a 15-item measure of GI-specific anxiety, or anxiety centered around GI symptoms and the contexts in which they occur. Items are rated on a 6-point Likert scale (1 = “strongly agree” to 6 = “strongly disagree”). In the current analyses, the VSI were reverse coded, then summed to create a total score such that higher scores indicate more severe IBS-related anxiety. The VSI total score was used in the primary analyses as a predictor variable (Cronbach’s alpha = 0.95), demonstrating excellent internal consistency.
Barriers for cessation
The Barriers for Cessation Scale (BCS; Macnee and Talsma, 1995) is a 19-item self-report questionnaire that measures perceived barriers for smoking cessation. Responses are provided using a 4-point Likert scale (0 = “not a barrier” to 3 = “large barrier”) and items are summed to create a total score such that higher scores represent more severe perceived barriers for quitting smoking. The BCS has strong psychometric properties (Garey et al., 2017). In the current study, the total score was used as a criterion variable (Cronbach’s alpha = 0.95), indicating excellent internal reliability.
Smoking consequences
The Short-Form Smoking Consequences Questionnaire (S-SCQ; Myers et al., 2003) is a 21-item self-report measure that assesses individuals’ beliefs about the outcomes of smoking behavior. Items are rated on a scale from 0 (completely unlikely) to 9 (completely likely). This study uses a negative reinforcement subscale (SCQ-NR), which refers to individuals’ beliefs that cigarette use will help them cope with uncomfortable moods or sensations. The mean SCQ-NR score was computed, with a higher score indicating higher negative reinforcement expectancies; the mean score was utilized as a criterion variable and demonstrated excellent internal consistency (Cronbach’s alpha = 0.95).
Smoking urgency
The Questionnaire on Smoking Urges-Brief (QSU-Brief; Toll et al., 2006) is a 5-item measure of smoking urges. The QSU-Brief has 2 factors, which capture distinct categories of smoking urges: (1) intention/desire to smoke (2 items) and (2) relief of negative affect and urgent desire to smoke (3 items). Items of the QSU-Brief are rated on a scale from 0 (“strongly disagree”) to 100 (“strongly agree”). Items that load onto each factor are summed to create two scores, such that higher scores indicated stronger smoking urges. The second factor (relief of negative affect; QSU-NR) was utilized as a criterion variable in the primary analyses (Cronbach’s alpha = 0.88), indicating good internal reliability.
Data analytic approach
SPSS version 29.0 was used. First, zero-order correlations were examined among study variables along with descriptive analyses. Then, three separate two-step hierarchical regression analyses were conducted for the following continuous criterion variables: (1) perceived barriers for smoking cessation, (2) negative affect reduction smoking expectancies, and (3) relief of negative affect smoking urge. In the first step, covariates, including cigarette dependence (FTCD-R; Başpınar and Basat, 2022), sex (Smith et al., 2016), education (Tenn et al., 2010), and depressive symptoms (ODSIS; Mendelsohn, 2012), were entered into the model (See footnote) Sex was coded as follows: 0 = male, 1 = female. Education was treated as a continuous variable and was coded as follows: 1 = less than high school, 2 = some high school, 3 = completed high school or equivalent, 4 = some college, 5 = associate’s degree, 6 = bachelor’s degree, 7 = master’s degree, 8 = doctoral degree. In the second step, GI-specific anxiety was added to the model. For each model, the F statistic was utilized to measure model fit and squared semi-partial correlations (sr2) were utilized as an indicator of effect size, with effects of 0.01, 0.09, and 0.25 indicating small, medium, and large effect size (Cohen et al., 2013), respectively.
Results
Descriptive analyses
Detailed descriptive information for the sample is presented in Table 1. The largest self-identified racial/ethnic group in the sample was White and non-Hispanic/Latino (N = 183 69.6%), followed by Hispanic/Latino White (N = 25; 11.0%) and non-Hispanic/Latino Black (9.5%). Most participants completed high school or higher (95.8%) and approximately half (49.0%) of the sample completed a bachelor’s degree or higher. About one-third of participants (30.8%) reported earning an income of $100,000 or higher.
Demographic information for the sample (N = 263).
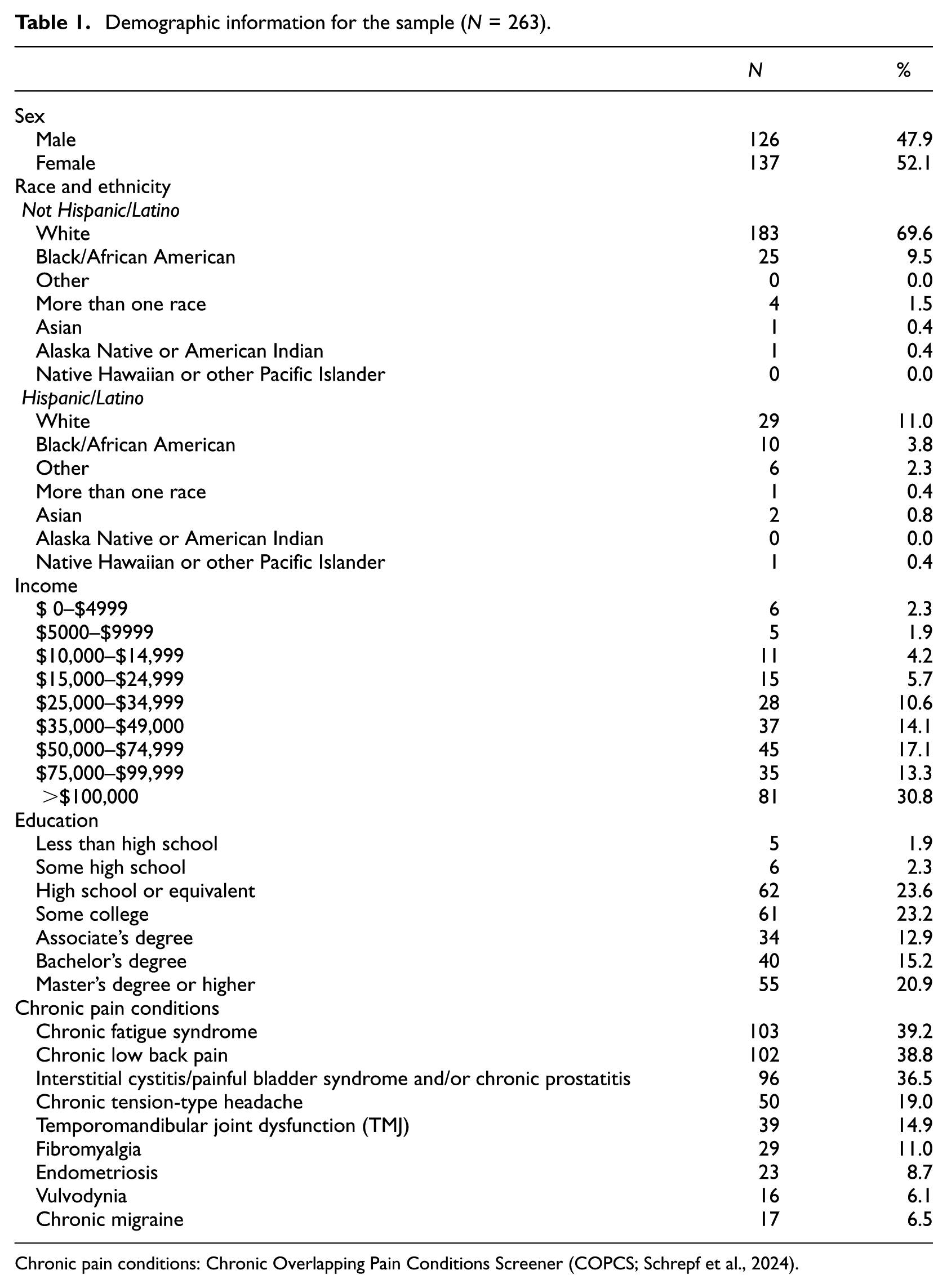
Chronic pain conditions: Chronic Overlapping Pain Conditions Screener (COPCS; Schrepf et al., 2024).
The most common nociplastic pain condition in the sample was chronic fatigue syndrome (N = 103; 39.2%), followed by chronic low back pain (N = 102; 38.8%). In terms of IBS symptom severity (IBS-SSS), approximately two-fifths of the sample (N = 107; 40.7%) met criteria for severe IBS symptoms, 36.1% (N = 95) had moderate symptoms, 17.5% (N = 46) had mild symptoms, and 5.7% (N = 15) had very mild symptoms.
On average, participants reported smoking 18.49 (SD = 16.42) cigarettes per day and starting daily cigarette smoking at age 17.8 years (SD = 6.93). The average level of cigarette dependence in the sample was in the moderate range (mean = 5.54; SD = 2.01). In addition to smoking combustible cigarettes, approximately one quarter (24.3%) of the sample reported daily use of electronic cigarettes. Additionally, from a lifetime perspective, 51.0% reported cigar use, 38.4% reported smokeless tobacco use, and 30.0% reported pipe tobacco use; the frequency of use for these products was not assessed.
Bivariate correlations
Bivariate correlations are presented in Table 2. GI-specific anxiety was statistically significantly and positively correlated with cigarette dependence, depressive symptoms, perceived barriers for quitting smoking, negative affect smoking expectancies, and relief of negative affect smoking urge. The three criterion variables were statistically significantly and positively correlated with one another.
Correlations among study variables (N = 263).
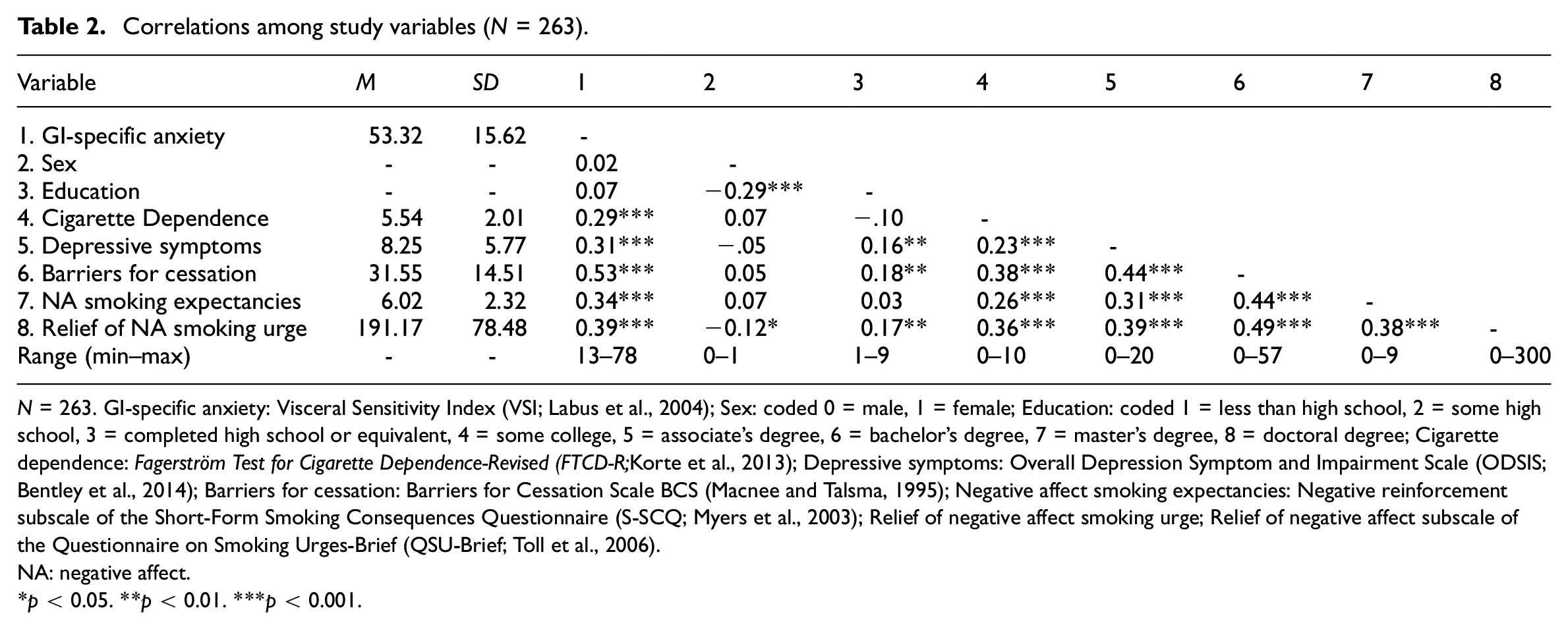
N = 263. GI-specific anxiety: Visceral Sensitivity Index (VSI; Labus et al., 2004); Sex: coded 0 = male, 1 = female; Education: coded 1 = less than high school, 2 = some high school, 3 = completed high school or equivalent, 4 = some college, 5 = associate’s degree, 6 = bachelor’s degree, 7 = master’s degree, 8 = doctoral degree; Cigarette dependence: Fagerström Test for Cigarette Dependence-Revised (FTCD-R; Korte et al., 2013); Depressive symptoms: Overall Depression Symptom and Impairment Scale (ODSIS; Bentley et al., 2014); Barriers for cessation: Barriers for Cessation Scale BCS (Macnee and Talsma, 1995); Negative affect smoking expectancies: Negative reinforcement subscale of the Short-Form Smoking Consequences Questionnaire (S-SCQ; Myers et al., 2003); Relief of negative affect smoking urge; Relief of negative affect subscale of the Questionnaire on Smoking Urges-Brief (QSU-Brief; Toll et al., 2006).
NA: negative affect.
p < 0.05. **p < 0.01. ***p < 0.001.
Multiple regression analyses
Hierarchical regression results are presented in Table 3. For barriers for cessation, step 1 of the model with covariates was statistically significant (R2 = 0.30, F(4, 258) = 28.21, p < .001). Education, cigarette dependence, and depressive symptoms emerged as statistically significant predictors. At step 2 (ΔR2 = 0.11, ΔF[1, 257] = 49.04, p < 0.001) a statistically significant main effect emerged for GI specific anxiety (b = 0.24, SE = 0.04, p < 0.001).
Hierarchical regression results.
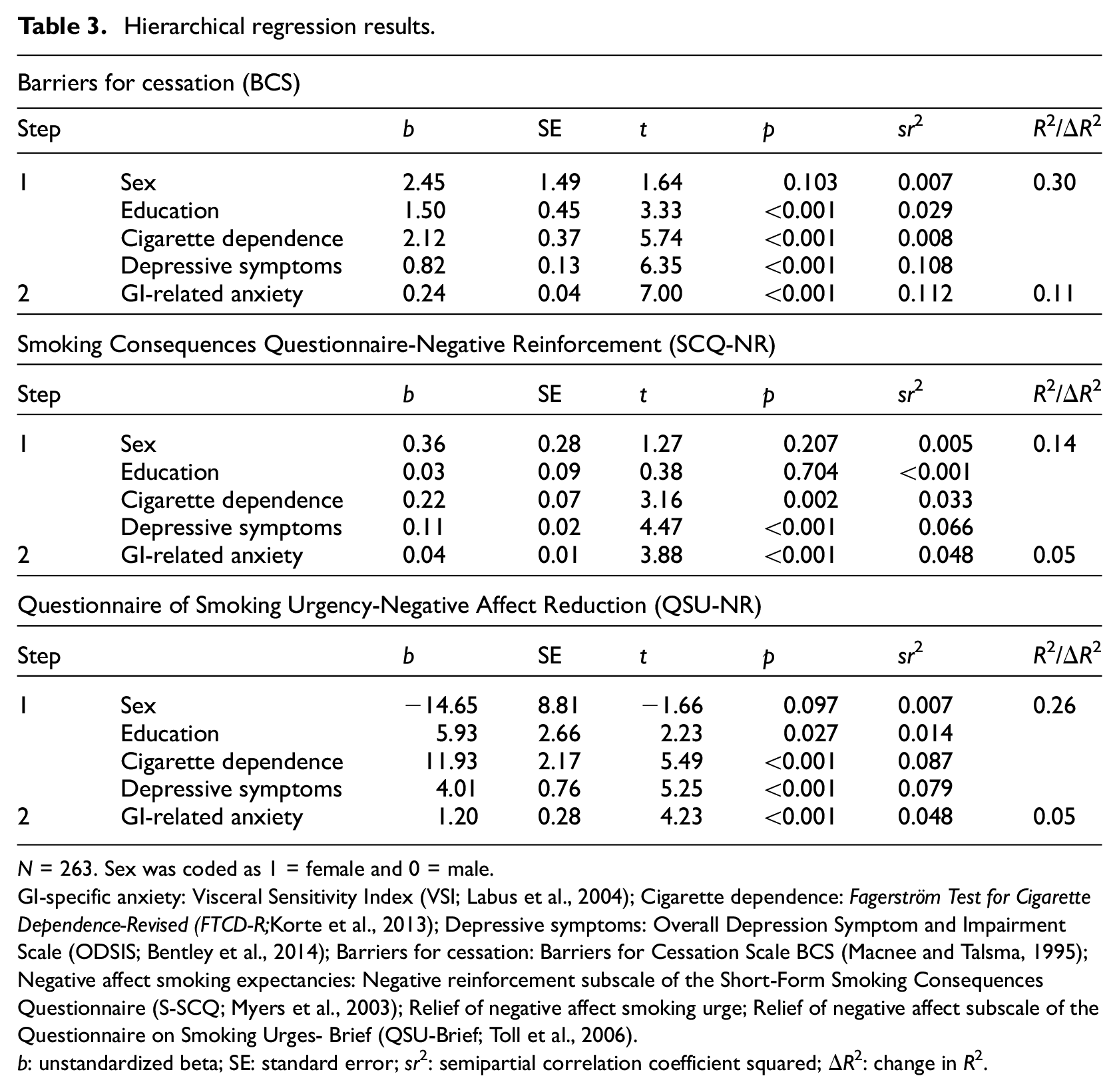
N = 263. Sex was coded as 1 = female and 0 = male.
GI-specific anxiety: Visceral Sensitivity Index (VSI; Labus et al., 2004); Cigarette dependence: Fagerström Test for Cigarette Dependence-Revised (FTCD-R; Korte et al., 2013); Depressive symptoms: Overall Depression Symptom and Impairment Scale (ODSIS; Bentley et al., 2014); Barriers for cessation: Barriers for Cessation Scale BCS (Macnee and Talsma, 1995); Negative affect smoking expectancies: Negative reinforcement subscale of the Short-Form Smoking Consequences Questionnaire (S-SCQ; Myers et al., 2003); Relief of negative affect smoking urge; Relief of negative affect subscale of the Questionnaire on Smoking Urges- Brief (QSU-Brief; Toll et al., 2006).
b: unstandardized beta; SE: standard error; sr2: semipartial correlation coefficient squared; ΔR2: change in R2.
For negative affect smoking expectancies, step 1 of the model with covariates was statistically significant (R2 = 0.14, F(4, 258) = 10.45, p < .001). Cigarette dependence and depressive symptoms emerged as statistically significant predictors. At step 2 (ΔR2 = 0.05, ΔF[1, 257] = 15.04, p < 0.001), a statistically significant main effect emerged for GI-specific anxiety (b = 0.04, SE = 0.01, p < 0.001).
For relief of negative affect smoking urge, step 1 of the model with covariates was statistically significant (R2 = 0.25, F(4, 258) = 22.38, p < .001). Education, cigarette dependence, and depressive symptoms were statistically significant predictors. In step 2 (ΔR2 = 0.05, ΔF[1, 257] = 17.89, p < 0.001), a statistically significant main effect emerged for GI-specific anxiety (b = 1.20, SE = 0.28, p < 0.001).
Discussion
There is a growing recognition of the importance of investigating addictive behaviors among persons with IBS (Fadgyas-Stanculete et al., 2014). Although extant work is limited in scope, smoking represents one prevalent and deleterious addictive behavior relevant to IBS (Mahmood et al., 2020). For example, smoking could maintain more severe IBS symptoms and impair treatment response (Lackner et al., 2024), and IBS-symptoms or sequalae could maintain smoking behavior (Qin et al., 2014). The current study sought to expand past work on IBS-smoking by exploring a candidate mechanism—GI-specific anxiety—as an individual difference factor relevant to smoking among adults with IBS who smoke.
As hypothesized, higher levels of GI-specific anxiety were associated with increased levels of perceived barriers for quitting smoking, negative affect smoking expectancies, and relief of negative affect smoking urge. Further, the observed effects for GI-specific anxiety ranged from small to medium in adjusted models (Abelson, 1985). These data provide incremental validity support for GI-specific anxiety as a construct of clinical importance among adults with IBS who smoke. Such findings are consistent with past work among the general population (Zvolensky et al., 2017) and align with negative reinforcement models of addiction that emphasize the regulation of aversive interoceptive states as a central process in maintaining addictive behavior (Koob, 2013). Future research is needed to explain the specific mechanisms governing relations between GI-specific anxiety and smoking among persons with IBS. Several conceptually relevant candidates that may mediate or exacerbate this relationship include emotion dysregulation (Zvolensky et al., 2018) and attentional biases for threat (Tayama et al., 2018). For example, individuals with greater GI-specific anxiety may be more likely to experience higher degrees of emotion dysregulation and be more reactive to smoking-related cues due to attentional biases toward threats, reinforcing smoking as a coping mechanism. These processes could tax cognitive-affective systems and engage negative reinforcement and habitual methods of coping (e.g. smoking). Mediation analyses could help clarify the pathways through which GI-specific anxiety influences smoking behavior, while moderation analyses could specify the subpopulations most impacted by these mechanisms, particularly within a longitudinal framework.
Clinically, integrating evidence-based strategies to reduce GI-specific anxiety in treatment programs for IBS patients who smoke could potentially improve smoking cessation outcomes in this population. For instance, smoking cessation interventions could incorporate cognitive-behavioral approaches, such as cognitive restructuring and exposure-based techniques, to help patients develop alternative coping strategies for managing GI-related distress without relying on smoking. Targeting GI-specific anxiety through cognitive-behavioral methods and key therapeutic elements such as interoceptive exposure can help reduce fear reactivity to IBS-related bodily sensations which could intensify during abstinence period (Craske et al., 2011). Additionally, treatment seeking smokers with IBS may benefit from specialized smoking cessation programs that address GI-specific anxiety as a transdiagnostic factor to improve efforts to quit.
This study has several limitations. First, the cross-sectional design limits causal inferences and does not capture the dynamic relationship between GI-specific anxiety and smoking behavior over time. Future research should build on this work by employing longitudinal methodologies to further clarify these relationships and evaluate GI-specific anxiety as a risk factor for smoking cessation. Second, while the sample was large and drawn from across the United States, there was limited racial/ethnic diversity, with approximately 70% of the sample identifying as non-Hispanic White. This limitation may affect the generalizability of the findings. Given that smoking and IBS can be underrecognized and undertreated among racial/ethnic minority groups (Barnes et al., 2021; Sheffer et al., 2022), future research should prioritize recruiting more diverse samples to improve representativeness and ensure broader applicability of findings. Third, daily smoking behavior was an inclusion criterion, but the sample was not treatment-seeking or engaged in a quit attempt for smoking cessation. Future studies could model GI-specific anxiety in relation to quit success among a treatment-seeking sample or those engaged in self-guided quit attempts. Fourth, while this research centered on smoking processes as criterion variables, it is important to recognize the potential bidirectional relationship between smoking and IBS-related processes. Future studies should explore how IBS symptom fluctuations influence smoking behaviors and vice versa, particularly in relation to GI-specific anxiety. A more comprehensive model that integrates both smoking and IBS-related mechanisms could enhance understanding of how these conditions interact and inform tailored intervention strategies. Finally, while we characterized chronic pain conditions in the sample descriptively, we did not conduct specific subgroup analyses based on these conditions, given our study’s primary focus on GI-specific anxiety and smoking processes. Future research should explore how multiple chronic pain conditions interact with GI-specific anxiety and smoking behaviors to better inform targeted interventions.
Overall, the present findings provide novel empirical evidence that GI-specific anxiety among adults with IBS who smoke is associated with several smoking processes implicated in the maintenance and relapse of smoking. These findings highlight the utility in the continued exploration of GI-specific anxiety as a mechanistic target among adults with IBS who smoke in efforts to enhance quit success. Integrating these findings into smoking cessation interventions may improve treatment outcomes by addressing GI-specific anxiety as a modifiable factor contributing to smoking behavior. Future research should further evaluate the effectiveness of such targeted interventions in clinical settings.
Footnotes
Data sharing statement
Data are available from the corresponding author, upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding was obtained through the State of Texas to Dr. Zvolensky and supported by the National Center for Complementary and Integrative Health (1K23AT012364-01), awarded to Dr. Jafar Bakhshaie.
Ethics approval
This project was approved by the University of Houston Institutional Review Board (STUDY00004200).
Informed consent
Informed consent was obtained before participation in the survey.