
Abstract
Residential childcare workers face stressors such as violence and heavy workloads, leading to stress. This scoping review aimed to synthesise research on stress in residential childcare workers and identify research gaps. APA PsycInfo, CINAHL, MEDLINE, SCOPUS and Social Work Abstracts were searched in January 2024 for papers on residential childcare worker stress. Of 3810 papers identified, 18 met the inclusion criteria. While a lot of research has focussed on predictors of burnout, there has been less research into predictors of perceived stress, hair cortisol, indirect trauma and post-traumatic symptoms. Largely, appraisals and coping have been omitted. Few findings have successful replications. Residential childcare workers face numerous stressors predicting high burnout and indirect trauma. However, there is a need to explore appraisals and coping in finer detail and replicate many of the existing findings.
Introduction
Residential childcare workers support young people living in out-of-home residential settings. They manage group dynamics, facilitating interventions, and more (Jones et al., 2007; Smith et al., 2021). These workers, whilst describing the role as rewarding (Potts et al., 1995; Vashchenko et al., 2010), are often faced with challenges that increase their risk of stress and trauma, such as client violence (Smith et al., 2021) and high workloads (Lee et al., 2017). Workplace stress has been linked to several negative physical (Goh et al., 2015) and mental health problems (Raskin et al., 2015; Smith et al., 2021), highlighting the potential importance of understanding stress in this workforce. An overview of the current state of the literature is needed, which will help guide future research by providing a more thorough understanding of stress in this population.
Youth residential settings and residential childcare workers
Definitions of youth residential settings and residential childcare workers vary internationally. As such, we adopted the following broad definition for inclusiveness. Youth residential settings include services for young people in short- and long-term out-of-home residential accommodation whilst the young person is unable to live with family, such as due to child abuse or neglect (Davidson-Arad, 2005). They also include purpose-built living environments that incorporate treatment, education, socialisation, support and protection for young people with severe emotional, behavioural or mental health concerns who do not require hospitalisation (Johnson et al., 2017; Whittaker et al., 2016).
In the present study, the term residential childcare worker has been adopted. However, they are also known as youth care workers, residential youth workers and more. These workers are defined as people who supervise, treat, and protect youth living in youth residential settings 24 hours a day when the youth are not engaged with other professionals. Residential childcare workers facilitate entertainment, prepare meals, provide behavioural management, and more (Smith et al., 2021). Many residential childcare workers report working with young people as enjoyable, particularly when they see the young people enjoying themselves or feel they are improving the quality of the young people’s lives. Additionally, residential childcare workers have reported changing from past careers due to perceiving residential childcare as socially meaningful or meeting a moral duty (Moses, 2000; Vashchenko et al., 2010). However, this work also has challenges (Potts et al., 1995).
Residential childcare workers must balance their responsibilities of supporting the young people whilst maintaining appropriate boundaries. Some workers report feeling like surrogate parents; however, their professional responsibilities change the relationship dynamics (Fowler, 2015). The young people in residential care come from diverse backgrounds, often with emotional and behavioural problems, and histories of neglect, abuse and domestic violence (Hejtmanek, 2016; Leloux-Opmeer et al., 2016). Residential childcare workers are, therefore, exposed to the aftermath of the trauma experienced by young people, placing the workers at higher risk for developing secondary traumatic stress (Ireland and Huxley, 2018). Additionally, workers must intervene when there is a risk of harm, which can result in harm against the worker (Smith et al., 2021; Smith and Colletta, 2019). Moreover, long hours, low pay, high workload (Dillenburger, 2004; Lee et al., 2017), and intensive oversight (Smith and Colletta, 2019) also potentially increase the likelihood of the workers experiencing stress.
Relevant models and outcomes of stress
Stress is a pressure, demand, or force, internal or external to the individual, requiring them to respond (Ursin and Eriksen, 2004). Stressors (the source of stress) can be physical, such as illness; life changes, such as a loved one’s death; environmental, such as temperature; or daily hassles, such as arguing (Ursin and Eriksen, 2004). According to both the Transactional Model of Stress and the Cognitive Activation Theory of Stress, when presented with a stressor, we engage in a stress response comprising a stressor appraisal (e.g. will this stressor benefit or harm me and can I cope with the stressor); a response that may involve behavioural (e.g. engaging in self-care), emotional (e.g. re-framing thoughts) or physiological (e.g. increased heart rate or release of cortisol); and a feedback mechanism (Folkman et al., 1986; Ursin and Eriksen, 2004). The feedback mechanism determines whether our coping addresses the situation, if our appraisals or coping needs to change, and if the stressor has subsided (Folkman et al., 1986). Acute stress is typically considered an adaptive response. However, prolonged stress (e.g. chronic stress) or beyond the capability of the individual to manage can result in physiological, psychological and behavioural impairments (Eriksen and Ursin, 2004).
Moreover, stressful work roles requiring frequent empathy and trauma exposure, like residential childcare workers, are more likely to experience empathetic stress (for a review, see: Rauvola et al., 2019). Empathetic stress can present as vicarious traumatisation, secondary traumatic stress, and compassion fatigue. All of these are argued to result in burnout. Vicarious traumatisation specifically refers to the accumulation of physical, neurological, emotional, mental, cognitive, sexual and spiritual changes experienced by an individual from repeated exposure to other people’s trauma and is typically long-term (Branson, 2019; McCann and Pearlman, 1990). Secondary traumatic stress, on the other hand, is the experience of symptoms of post-traumatic stress disorder (e.g. avoidance, intrusive mental imagery, sensitivity to trauma-related material) that an individual may display following exposure to another person’s trauma (Figley, 1983). Secondary traumatic stress is normally an acute and shorter-term response to the initial exposure, as opposed to vicarious trauma, which captures the longer-term and repeated nature of trauma exposure (Jenkins and Baird, 2002). The term compassion fatigue was a later relabelling of secondary traumatic stress to reduce the stigma associated with the term (Figley, 1995). However, the term compassion fatigue has appeared in other relevant literature with different conceptualisations. For example, some define compassion fatigue as emotional exhaustion or the cost of caring rather than a response to trauma exposure (Ledoux, 2015). Burnout is conceptualised as the response of an individual to chronic interpersonal stressors at work, which some argue presents as a syndrome of emotional exhaustion, depersonalisation (personal detachment from work) and lack of personal accomplishment (Maslach and Leiter, 2016).
Given that there is evidence that youth workers experience high workplace stress, coupled with evidence that stress has physical and emotional consequences, there is impetus to explore stress in this population further to understand the stress response in detail so that approaches to minimising the potential negative outcomes associated with this stress can be generated. To the author’s knowledge, there is only one previous systematic review by Seti (2008) which focussed on the causes and treatment of burnout in residential childcare workers but did not focus on stress more broadly. As such, there remains a need for a body of work that synthesises all the current research on stress more broadly. Therefore, this review aims to synthesise the current literature on stress in residential childcare workers. The breadth of the literature and the quality of the research will be examined to provide a comprehensive understanding of the current state of the research. Furthermore, this scoping review aims to identify areas where further research is needed regarding this population.
Method
Search strategy and inclusion criteria
The databases APA PsycInfo, CINAHL Complete, MEDLINE Complete, SCOPUS and Social Work Abstracts were searched in January 2024 due to their comprehensive coverage of the research area. Search terms were searched in titles, abstracts, and keywords where possible. The search structure involved four groups of keywords describing stress, client age, setting, and worker. The complete search terms were: (*stress* OR burnout OR fatigue OR tension OR strain OR distress* OR anxi* OR worr* OR apprais* OR coping OR ‘vicarious stress’ OR ‘vicarious trauma’ OR ‘secondary stress’ OR ‘secondary trauma’ OR ‘occupational stress’) AND (teenager* OR adolescen* OR child OR juvenile OR minor OR youth OR childcare OR p?ediat*) AND (‘care home’ OR ‘in care’ OR ‘group home’ OR ‘youth care’ OR ‘youth residential care’ OR ‘residential facility’ OR ‘residential treatment’ OR ‘child residential care’) AND (‘Staff member’ OR ‘caregiver’ OR ‘support worker’ OR ‘youth worker’ OR ‘childcare worker’ OR ‘frontline worker’ OR ‘care worker’ OR ‘child care staff’ OR ‘staff’ OR ‘welfare worker’).
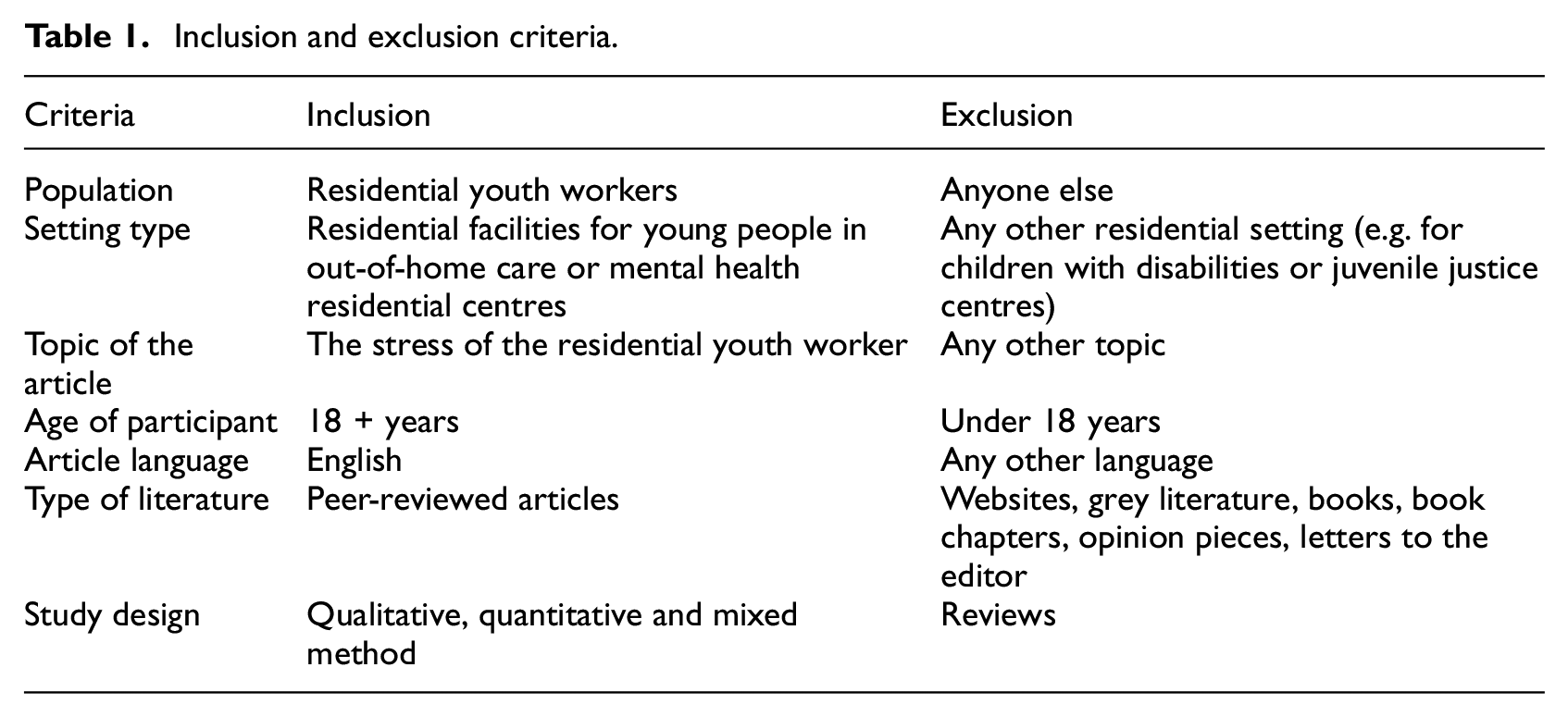
Titles and abstracts were screened against inclusion and exclusion criteria (see Table 1). The full texts of remaining papers were retrieved and screened to arrive at the final list of papers. Backward and forward-hand searching of all included papers was also conducted. The authors manually double-extracted data for each included paper. Any discrepancies in data charting were discussed and resolved between authors. Data were synthesised by the outcome variables in the included papers and interpreted in the context of existing stress models. This facilitated a high-level perspective of the field while cross-examining the findings against existing models. This scoping review was not pre-registered. As a scoping review, there are no human participants in this research and informed consent is not required.
Inclusion and exclusion criteria.
Quality assessment
Two quality assessments were conducted, one for quantitative and one for qualitative research. As study designs were heterogeneous, assessment tools were created from a combination of Joanna Briggs Institute Critical Appraisal tools. As not all criteria were applied to all study designs, study quality was defined as the percentage of criteria that were met that applied to that study design.
Results
Of the 3715 papers identified, 18 met inclusion criteria (see Supplemental Figure 1). Table 2 summarises findings from individual studies. Most studies were conducted in the USA (n = 6), then Switzerland (n = 3), Canada (n = 3) and one study, respectively, in Australia, Hong Kong, Norway, Scotland, Spain and Sweden. Eleven were cross-sectional, three were longitudinal, and four were qualitative. All studies met almost all relevant quantitative quality criteria. However, only 14% included an a priori power calculation and only 7% included confound variables in analyses (mean quality score = 86%, range: 75%–100%, see Supplemental Table 1). Similarly, almost all relevant qualitative criteria were met for all studies. However, only 50% included a researcher positioning statement or the inclusion of evidence of ethical approval and only 25% included a statement regarding the researcher’s theoretical background (mean quality score = 82.5%, range: 70%–100%, see Supplemental Table 2).
Summary of included papers. Significant and non-significant results are grouped by outcome.

n.s.: not significant (p > 0.05).
Included studies explored stress levels (n = 3), secondary traumatic stress or compassion fatigue (n = 3), post-traumatic stress symptoms (n = 1), and burnout (n = 10). Of the 211 distinct associations across 73 predictors and 12 outcomes, 59 (28%) of these were explored in more than two studies, of which only 8 (4%) produced significant associations across the majority of studies, 18 (9%) associations had inconclusive evidence, and 33 (16%) demonstrated non-significant associations across the majority of studies exploring those associations (see Supplemental Table 3).
Outcome 1: Stress level
Qualitative (Bickle, 2021; Heron and Chakrabarti, 2002; McLean, 2015; Steinkopf et al., 2022) research highlighted that workplace stress is related to perceived difficulties in the work environment, difficulties in caring for the youth, and workplace events reminiscent of personal trauma. One quantitative study found that subjectively perceived stress levels were higher for those with higher levels of education and in non-full-time employment (del Valle et al., 2007).
Outcome 2: Reactions to stress
Two quantitative studies have examined hair cortisol levels, an objective marker of a physiological reaction to stress (Bürgin et al., 2020; Kind et al., 2018). The research aligns with the above findings’ theme that challenging work environments (e.g. aggressive clients) correlated with increased cortisol levels (Kind et al., 2018). However, a greater sense of workplace coherence, using self-care and implementing trauma-informed care (Kind et al., 2018) were associated with lower cortisol levels. Gender produced mixed results, with one study finding females had higher cortisol (Bürgin et al., 2020) and another finding no difference (Kind et al., 2018).
Two cross-sectional quantitative studies reported behavioural reactions in residential childcare worker stress (Mann-Feder and Savicki, 2003; Stapleton et al., 2016). Stapleton et al. (2016) found that increased emotion-focussed coping was associated with greater compassion satisfaction, compassion fatigue, and secondary traumatic stress. In this same study, increased problem-focussed coping was associated with greater compassion satisfaction. However, it was unrelated to compassion fatigue and secondary traumatic stress. Mann-Feder and Savicki (2003) highlighted that the association of coping with burnout differed between Anglophone and Francophone Canadian workers. No study examined emotional reactions to stress.
Outcome 3: Secondary traumatic stress and compassion fatigue
Three quantitative studies explored secondary traumatic stress and compassion fatigue (Eastwood and Ecklund, 2008; Stapleton et al., 2016; Steinlin et al., 2017). Males (Stapleton et al., 2016) with lower socio-economic status (Eastwood and Ecklund, 2008) reported the highest levels of indirect trauma. Like perceived stress levels, indirect trauma was higher in those with lower workplace coherence, poorer work environments in terms of interpersonal support and resourcing (Steinlin et al., 2017), and greater burnout (Eastwood and Ecklund, 2008).
Outcome 4: Post-traumatic stress symptoms
One study examined participants’ levels of PTSD symptomology following traumatic work events. This study found that a higher sense of coherence, greater work-related self-care, more enjoyment of work, having no children and being male predicted lower levels of post-traumatic stress symptoms (Steinlin et al., 2017).
Outcome 5: Burnout
Some included studies explored burnout as a whole construct while others measured burnout across three components: emotional exhaustion, depersonalisation, and personal accomplishment. Burnout was the most comprehensively studied outcome. As highlighted in Supplemental Table 3, burnout is the only outcome that produced consistent significant findings across replications. However, there were far more inconsistent than consistent findings across burnout studies. The below summary of findings synthesises across only those associations explored in more than one study (see Table 2 for the results of associations explored in only a single study).
Overall Burnout
While there was no association between overall burnout and gender in one longitudinal (Kind et al., 2018) and one cross-sectional study (Steinlin et al., 2017), there was inconsistent evidence for whether there was a negative association between age and burnout (Kind et al., 2018) or not (Steinlin et al., 2017). Moreover, there was inconsistent evidence as to whether there was a positive association between length of employment and burnout (Kind et al., 2018) or not (Steinlin et al., 2017). These inconsistencies may suggest that some burnout-related associations are only detectable over time. Finally, a greater sense of workplace coherence and self-care correlated with lower burnout (Kind et al., 2018; Steinlin et al., 2017).
Emotional exhaustion
Emotional exhaustion was consistently greater for residential childcare workers who were higher in neuroticism (Barford and Whelton, 2010; Lakin et al., 2008; Leon et al., 2008), work pressure (Barford and Whelton, 2010; Mann-Feder and Savicki, 2003; Savicki and Savicki, 2002) and lower job satisfaction (Lakin et al., 2008; Leon et al., 2008). However, there was no association between task orientation and emotional exhaustion (Mann-Feder and Savicki, 2003; Savicki and Savicki, 2002). There was a lack of consistency in findings between emotional exhaustion and ethnicity (Lakin et al., 2008; Leon et al., 2008), age (Kind et al., 2018; Lakin et al., 2008; Leon et al., 2008), extraversion (Barford and Whelton, 2010; Lakin et al., 2008; Savicki and Savicki, 2002), workplace training (Lakin et al., 2008; Leon et al., 2008) or managerial support (Barford and Whelton, 2010; Lakin et al., 2008; Mann-Feder and Savicki, 2003; Savicki and Savicki, 2002).
Depersonalisation
Only a significant positive association between depersonalisation and neuroticism was replicated across studies (Barford and Whelton, 2010; Lakin et al., 2008; Leon et al., 2008). Culture (Lakin et al., 2008; Leon et al., 2008), age (Barford and Whelton, 2010; del Valle et al., 2007; Kind et al., 2018; Lakin et al., 2008; Leon et al., 2008), agreeableness (Barford and Whelton, 2010; Savicki and Savicki, 2002), task orientation (Mann-Feder and Savicki, 2003; Savicki and Savicki, 2002) and job satisfaction (Lakin et al., 2008; Leon et al., 2008) all had inconsistent findings across studies with depersonalisation.
Personal accomplishment
A positive association between personal accomplishment and extraversion was the only consistently significant finding (Barford and Whelton, 2010; Lakin et al., 2008; Savicki and Savicki, 2002). There was no association between personal accomplishment and peer cohesion (Mann-Feder and Savicki, 2003; Savicki and Savicki, 2002). All other associations produced inconsistent results across studies, specifically for education level (del Valle et al., 2007; Leon et al., 2008), ethnicity (Lakin et al., 2008; Leon et al., 2008), conscientiousness (Barford and Whelton, 2010; Savicki and Savicki, 2002), neuroticism (Barford and Whelton, 2010; Lakin et al., 2008; Leon et al., 2008), length of employment (Barford and Whelton, 2010; del Valle et al., 2007; Leon et al., 2008), task orientation (Mann-Feder and Savicki, 2003; Savicki and Savicki, 2002), job satisfaction (Lakin et al., 2008; Leon et al., 2008) or supervisor support (Mann-Feder and Savicki, 2003; Savicki and Savicki, 2002).
Discussion
This review synthesised all stress research in residential childcare workers. This review found that although a wide range of stress predictors were studied, there were few replication studies, most of which were consistently non-significant or produced inconsistent results. Finally, the review found that key elements of dominant models of the stress response (i.e. appraisals, coping and vicarious trauma) were absent or under-researched in this population.
One strength of this field is the breadth of predictors explored. Across the 18 studies, 73 predictors were explored, such as demographics, personality or workplace attributes. Across these, risk factors (e.g. anxiety, neuroticism, working with clients with complex needs and work pressure) and protective factors (e.g. empathic concern, self-care, sense of coherence, job involvement, and role clarity) were identified across the 12 outcomes.
Another strength of this field of research is the depth in which burnout has been explored. Almost all 73 predictors have been explored in the context of burnout. However, Rauvola et al. (2019) highlight that empathetic stress-related burnout results from experiencing compassion fatigue, secondary traumatic stress and vicarious traumatisation. Unfortunately, only three studies (Eastwood and Ecklund, 2008; Stapleton et al., 2016; Steinlin et al., 2017) have explored compassion fatigue and secondary traumatic stress, with no study examining vicarious trauma, highlighting a need for further research and replication.
Outside of burnout, only gender has been examined in multiple studies, which has produced inconsistent or non-significant findings across replications. This, generally, was also the pattern for burnout, with most replicated associations having either inconsistent or consistently non-significant findings. Given the lack of replicability of these findings, there is impetus to replicate the other associations that have only featured in a single study. Nevertheless, such a volume of non-significant findings favourably suggests that publication bias may not be present.
At the outset of this paper, we outlined the Transactional Model of Stress and the Cognitive Activation Theory of Stress. These paradigms placed the appraisals and responses to stress (behavioural, emotional and physiological) as determinants of individual variations in the experience and outcomes of stress. Unfortunately, no study measured stressor appraisals; only two studies measured coping (behavioural reactions) and two measured hair cortisol levels (physiological reactions). Moreover, there are other indicators of the physiological stress response, such as heart rate variability (Sharma and Gedeon, 2012). As such, the biggest gap in the literature to date is the exploration of appraisals and responses to stress in residential childcare workers.
Limitations of this review
Despite the findings of this review regarding the breadth of associations identified and synthesised and in terms of identifying current gaps for future research, some limitations should be considered. Studies that combined residential childcare workers with other populations were excluded as mixed sampling may have masked unique associations in residential childcare workers. Another limitation was that the quality assessment returned relatively consistent scores, making it difficult to incorporate data from this tool to temper or resolve conflicting findings.
Implications
The current review synthesised all identifiable research on stress experienced by residential childcare workers. Each of the studies included in the review found that residential childcare workers were exposed to a number of stressors and were experiencing stress. However, further replication is needed to help strengthen our understanding of the predictors of stress in residential childcare workers. Future studies should also describe workplace settings, conduct a priori power analyses, and identify and control for confounding variables.
While intervention development is an intuitive implication of this review, more investigation is necessary to promote targeted intervention development. Although extant research has identified issues such as burnout as significant for these workers, other stress outcomes that also have far-reaching effects on health and wellbeing have not been explored. These include emotional reactions and disorders such as depression or anxiety (Folkman et al., 1986) as well as complex psychoneuroendocrinological effects of stress, such as a widespread and potentially lasting change in physiological processes (Juster et al., 2010).
Conclusion
This review is the first to synthesise the current literature on stress in residential childcare workers. Despite the varied methodologies and breadth of associated explored, findings have not been replicated successfully. Nevertheless, the results suggest that the workers’ demographics, personality and work attitudes are important in worker empathetic stress.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251336915 – Supplemental material for A scoping review of stress in residential childcare workers
Supplemental material, sj-docx-1-hpq-10.1177_13591053251336915 for A scoping review of stress in residential childcare workers by Christopher J Kilby, Emma L Horrobin, Courtney Wurth and Kelly Watt-McMahon in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053251336915 – Supplemental material for A scoping review of stress in residential childcare workers
Supplemental material, sj-docx-2-hpq-10.1177_13591053251336915 for A scoping review of stress in residential childcare workers by Christopher J Kilby, Emma L Horrobin, Courtney Wurth and Kelly Watt-McMahon in Journal of Health Psychology
Footnotes
Data sharing statement
All data generated by the authors for this scoping review are included in the paper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
No ethics approval was needed for this review article.
Informed consent
Informed consent was not applicable to this review article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.