
Abstract
The present cross-sectional study examined how perceived weight stigma (PWS) and weight-related self-stigma (WRSS) may sequentially mediate the relationship between body mass index (BMI) and quality of life (QoL) among Malaysian young adults. Malaysian university students (n = 1044; mean age = 21.3 years) self-reported their height/weight and completed the Weight Self-Stigma Questionnaire, Perceived Weight Stigma Scale, and World Health Organization Quality of Life–BREF. Sequential mediation analyses assessed direct/indirect effects of BMI on QoL domains (including physical, psychological, social, and environmental) and overall QoL, with PWS and WRSS as mediators. Higher BMI (i) positively related to PWS (r = 0.150, p < 0.01) and WRSS (r = 0.469, p < 0.01); and (ii) negatively related to psychological QoL (r = −0.105, p < 0.01) and general health (r = −0.148, p < 0.01). Sequential mediation analyses showed significantly negative indirect effects of BMI on all QoL domains via PWS and WRSS. Therefore, PWS and WRSS are important factors in the relationship between BMI and QoL among Malaysian young adults.
Introduction
The growing prevalence of obesity and being overweight among Malaysian adults has emerged as a major public health concern. According to the National Health and Morbidity Survey 2023, the prevalence of being overweight among adults (aged ≥18 years) increased from 29.4% in 2011 to 32.6% in 2024, while the prevalence of obesity rose from 15.1% to 21.8% over the same period (Institute for Public Health (IPH), 2024). Moreover, 39.4% of Malaysian young adults aged 18–29 years are overweight and/or have obesity (IPH, 2024). These statistics are of concern because excess weight is associated with impaired quality of life (QoL) among young adults (Stephenson et al., 2021). The World Health Organization (WHO) defines QoL as “individuals’ perceptions of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns,” encompassing various dimensions, including physical health, psychological health, social relationships, and environmental health (The WHOQOL Group, 1998). Given that more than one-third of Malaysian young adults are affected by overweight and obesity, understanding the impact of body weight on QoL is crucial for guiding interventions and improving health outcomes.
The relationship between body mass index (BMI) and QoL remains complex and inconsistent across studies (Apple et al., 2018). A recent systematic review reported an inverse relationship between higher weight status and lower QoL, particularly among individuals with obesity, where physical and psychological functioning, mental health, body image, and overall well-being were negatively impacted (Okolo et al., 2024). While obesity is generally associated with reduced QoL (Luah et al., 2024; Ward et al., 2024), even after controlling for comorbidities (Apple et al., 2018; McClintock et al., 2025), some studies suggest that individuals with higher BMI may report better mental QoL (Ul-Haq et al., 2013; Zhu et al., 2015).
In Malaysia, findings have also been mixed. Some studies have shown negative associations between obesity and QoL, for example, lower physical, social, and overall health functioning among children (Abdullah et al., 2024), diminished physical health among men, and reduced psychological health among women (Mohd-Sidik et al., 2021). In contrast, other studies have found no significant relationship between BMI and QoL among older adults (e.g. Mohd Noor et al., 2023). These inconsistencies may arise from variations in study populations and differences in the measurement instruments used to assess QoL. These conflicting findings highlight the need for further research to better understand the impact of BMI on different dimensions of QoL, which is essential for developing effective prevention and weight management strategies.
Young adulthood is a critical period for establishing identity, self-esteem, self-perception and long-term health behaviors, making this demographic particularly vulnerable to stigma, which can significantly impact their mental and emotional well-being (Emmer et al., 2020). Researchers have proposed that stigma among those who are overweight or have obesity can be broadly categorized into perceived weight stigma (PWS) and weight-related self-stigma (WRSS; Papadopoulos and Brennan, 2015). PWS refers to the negative attitudes, beliefs, and stereotypes that individuals believe others view about them due to their body weight or size, and can often lead to feelings of shame and embarrassment (Alimoradi et al., 2022). On the other hand, WRSS involves the internalization of negative attitudes and beliefs about being overweight or having obesity, where individuals apply societal stereotypes to themselves, leading to self-devaluation and diminished self-worth (Wott and Carels, 2010). Addressing these forms of stigma is essential to improving QoL of young adults affected by weight issues.
Previous studies have shown that both PWS and WRSS are significantly associated with BMI (Gan et al., 2022; Khodari et al., 2021; Lin et al., 2023) and QoL (Alimoradi et al., 2022; Fan et al., 2021; Khodari et al., 2021; Lin et al., 2024), indicating these factors may potentially act as sequential mediators in this relationship. Guardabassi et al. (2018) proposed a mediation model examining the relationship between weight status, stigma, and QoL among children aged 8–11 years in Italy, showing that weight-related stigma, rather than weight status, was negatively associated with QoL. Similarly, Fan et al. (2021) found that WRSS was associated with QoL among children aged 8–12 years in Hong Kong, with different effects on child-reported and parent-reported QoL. More specifically, PWS and WRSS were found to significantly mediate the relationship between body weight and children’s QoL (Fan et al., 2021). However, most of these studies focused on children or Western populations, with limited exploration of the mediating mechanisms among young adults in non-Western contexts.
Moreover, inconsistencies in the relationship between BMI and QoL in the literature may be explained by variations in the assessment of weight stigma and the role of cultural influences. Cultural factors such as societal attitudes toward body image and weight, and the importance of food in social interactions, are likely to influence how weight stigma is perceived and experienced, potentially shaping its impact on QoL in ways that differ from Western contexts (Pimenta et al., 2015). While Western cultures often emphasize thinness as the ideal body type, Malaysian culture presents a more complex relationship with body image, where larger sizes may symbolize health, and prosperity, resulting in mixed messages about body ideals (Yunus et al., 2022). The cultural significance of food, particularly in fostering social interactions through communal eating, further complicates perceptions of body weight, and stigma (Benton et al., 2025). Yunus et al. (2022) found that Malaysians who have obesity often experience weight discrimination and negative emotions associated with societal expectations, which exacerbate their mental health challenges and create barriers to self-acceptance and effective weight management.
Given these cultural and methodological differences, it is important to conduct research that considers the local context when examining the relationship between BMI and QoL. To address this inconsistency, the present study focused on young adults in Malaysia, and used the WHOQOL-BREF, a validated multidimensional measure of QoL. Most research has focused on the direct relationship between BMI and QoL, overlooking the potential mediating roles of factors such as PWS and WRSS (Apple et al., 2018; Luah et al., 2024; Okolo et al., 2024; Ward et al., 2024). By incorporating PWS and WRSS as mediators, the present study aimed to clarify how BMI is associated with QoL through stigma-related processes, offering a more nuanced understanding of this complex relationship. To date, no studies have explored whether the impact of BMI on QoL among Malaysian young adults is mechanistically explained by stigma processes. Therefore, the present study addressed this gap by examining the mediating roles of PWS and WRSS in the relationship between BMI and QoL among young adults in Malaysia. It was hypothesized that: (i) higher BMI would be positively correlated with both PWS and WRSS; (ii) higher BMI would be correlated with lower QoL across all domains (physical, psychological, social, environmental), as well as lower overall QoL and lower general health; (iii) higher PWS and WRSS would be negatively associated with all domains of QoL (physical, psychological, social, and environmental), as well as overall QoL and general health; and (iv) PWS and WRSS would sequentially mediate the relationship between BMI and all domains of QoL (physical, psychological, social, and environmental), as well as overall QoL and general health, with age and sex as covariates. By examining these sequential mediators, the study sought to provide a deeper understanding of how body weight affects QoL and to inform interventions to reduce stigma and improve the physical and mental well-being of young adults facing weight-related challenges.
Methods
Participants and data collection procedure
The present cross-sectional study was conducted among university students in Malaysia. University students were recruited through convenience sampling between March and August 2024, using Google Forms distributed through emails and WhatsApp. Study criteria included: (i) being Malaysian; (ii) being aged 19 years and above; (iii) currently studying in a university in Malaysia; and (iv) having access to the internet. The information sheet and informed consent form appeared on the first page of the survey on Google Forms. Students who agreed to participate in the study were required to click the “I agree to participate in the study” button, after which they could proceed to complete the online survey. Google Forms was programed to prompt participants if any item was left unanswered. Consequently, the survey could not be submitted unless all questions were completed. Therefore, there were no missing data. Additionally, participants who completed the online survey were provided with a small remuneration of RM15 (~3.4 USD). Ethical approval for the study protocol was obtained from the Ethics Committee for Research Involving Human Subject of Universiti Putra Malaysia (JKEUPM; reference number: JKEUPM-2023-1324) prior to the data collection of the study.
Measures
Weight Self-Stigma Questionnaire (WSSQ)
The WSSQ is a self-report instrument assessing WRSS (Lillis et al., 2010). It comprises the self-devaluation subscale (Items 1–6) and the fear of enacted stigma subscale (Items 7–12). An example item in the self-devaluation subscale is “I caused my weight problems.” An example item in the fear of enacted stigma subscale is “I feel insecure about others’ opinions of me.” All 12 items are scored using a 5-point Likert scale (1 = completely disagree to 5 = completely agree), with a higher score indicating a greater experience of shame related to the individual’s weight (i.e. WRSS). The internal consistency of the scale in previous studies, including research on a Malaysian sample, was high (α = 0.88; Gan et al., 2022; Lillis et al., 2010). The Cronbach’s α for the WSSQ in the present sample was 0.94.
The Perceived Weight Stigma Scale (PWSS)
The PWSS is a self-report instrument assessing individual’s perceived weight stigma (PWS; Lin et al., 2020). It consists of 10 items, each evaluated using a dichotomous scale where responses are either “yes” (1) or “no” (0). An example item in the PWSS is “You faced discrimination in a host of social settings (e.g. university).” A previous study reported good internal consistency for the PWSS among Malaysians (α = 0.83; Gan et al., 2022). The Cronbach’s α for the PWSS in the present sample was 0.82.
The World Health Organization Quality of Life—BREF (WHOQOL-BREF)
The WHOQOL-BREF is a self-report instrument assessing an individual’s quality of life (QoL; The WHOQOL Group, 1998). The WHOQOL-BREF consists of 26 items, assessing overall QoL, general health condition and four QoL domains: physical health, psychological health, social relationship, and environment. The two questions for assessing general condition are “How would you rate your quality of life?” and “How satisfied are you with your health?.” These two items are treated independently and are not included in the domain scores. In the present study, they were analyzed separately as indicators of “overall QoL” and “general health,” consistent with the WHOQOL-BREF scoring guidelines. Seven questions assess the physical QoL (e.g. “How satisfied are you with your ability to perform your daily living activities?”). Six questions assess psychological QoL (e.g. “How well are you able to concentrate?”). Three questions assess social QoL (e.g. “Do you feel respected by others?”). Eight questions assess environmental QoL (e.g. “How satisfied are you with your access to health services?”). All 26 items are scored using a 5-point Likert (1 = not at all to 5 = completely). A higher score indicates a better QoL. Previous studies, including research with a Malaysian sample, have reported good internal consistency for the WHOQOL-BREF, with Cronbach’s α values ranging between 0.66 and 0.84 (Seok et al., 2023; The WHOQOL Group, 1998). The Cronbach’s α values for WHOQOL-BREF in the present sample were 0.72 (physical QoL), 0.80 (psychological QoL), 0.63 (social QoL), and 0.84 (environmental QoL).
Self-reported body weight and height
BMI was calculated from participants self-reporting their current body weight and height. While self-report can introduce measurement error (Lynggaard et al., 2022), the use of self-reported BMI is consistent with similar research involving university student populations (Sai et al., 2018). Additionally, previous research has shown that self-reported anthropometric measurements are generally consistent with directly measured values (Davies et al., 2020).
Demographic information
Participants were asked to self-report their age (in years), sex (male or female), ethnicity (Malay, Chinese, Indian, or other), study program level (undergraduate or postgraduate), current year of study (year 1, year 2, year 3, year 4, or year 5 or above for undergraduate; year 1, year 2, or year 3 or above for postgraduate), and marital status (single or married).
Data analysis
Descriptive analysis (e.g. means and standard deviations) was used to analyze the characteristics of the participants. Pearson’s correlations were used to evaluate the associations between all studied variables (i.e. BMI, PWSS score, WSSQ score, WHOQOL-BREF scores in physical, psychological, social, and environment domains, the first two question scores in WHOQOL-BREF, age, and sex). To evaluate the assumptions of normality, linear regression analyses were conducted corresponding to the mediation model. Variance Inflation Factor (VIF) values were all below 2. Durbin-Watson values ranged from 1.786 to 2.073, suggesting independence of residuals. Values of skewness and kurtosis were acceptable (see Supplemental Table 1). Six sequential mediation analyses (see Figure 1) were then conducted to evaluate the effects of BMI on all domains of QoL (i.e. physical QoL, psychological QoL, social QoL, environmental QoL) and the first two WHOQOL-BREF questions (i.e. overall QoL and general health) through PWSS score and WSSQ score, with covariates including age and sex. All data analyses were conducted using SPSS Statistics 22. The sequential mediation analyses were performed using Model 6 in Hayes’ PROCESS macro in SPSS. Building on findings of Lin et al. (2023), which suggested that PWS often precedes and contributes to WRSS, this model was selected to test a theoretically grounded pathway, incorporating a hypothesized causal chain in which PWS was expected to influence WRSS, which then impacts QoL.
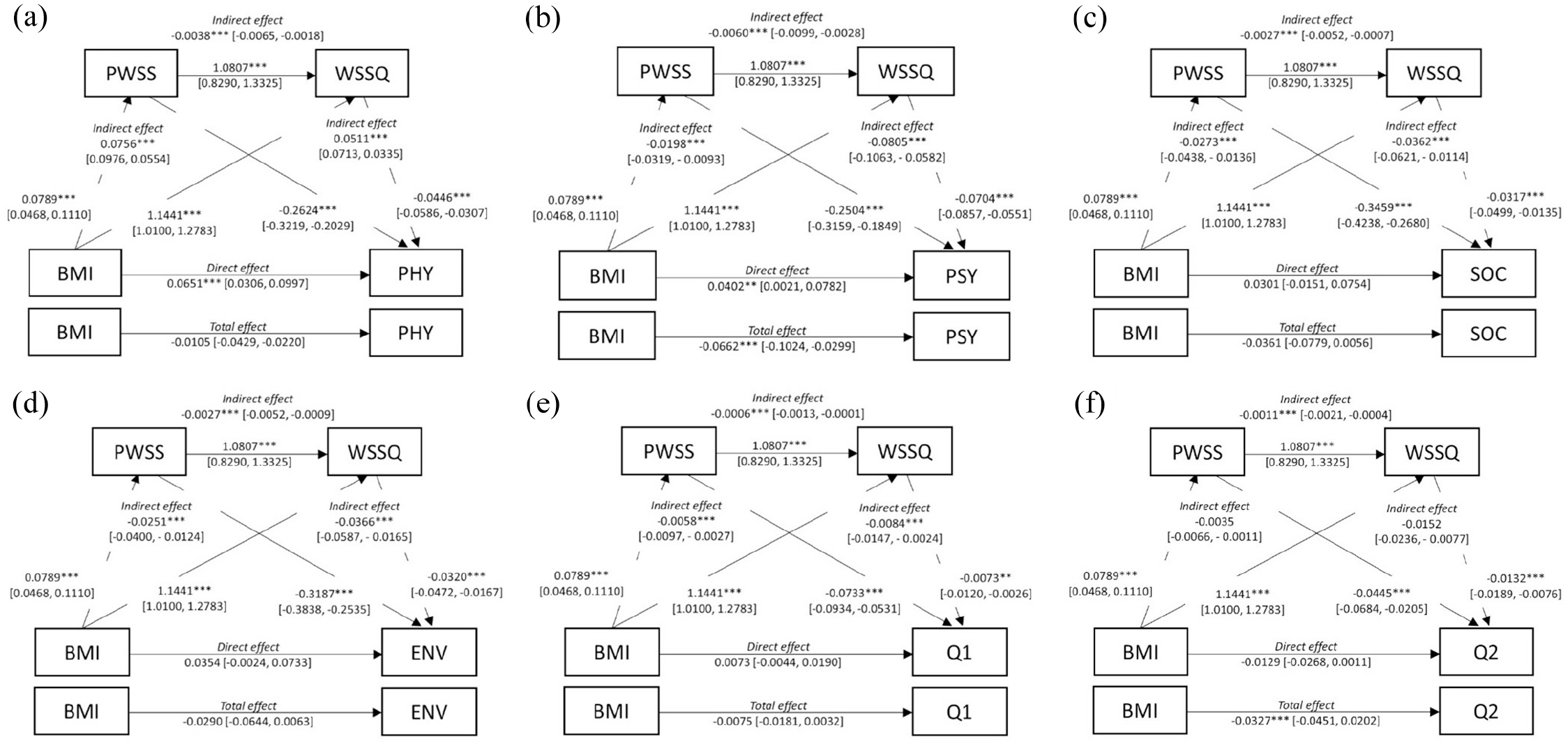
(a) Sequential mediation model with Perceived Weight Stigma Scale (PWSS) and Weight Self-Stigma Questionnaire (WSSQ) as mediators between body mass index (BMI) and physical health domain of WHOQOL-BREF (PHY). (b) Sequential mediation model with PWSS and WSSQ as mediators between BMI and psychological domain of WHOQOL-BREF (PSY). (c) Sequential mediation model with PWSS and WSSQ as mediators between BMI and social relationships domain of WHOQOL-BREF (SOC). (d) Sequential mediation model with PWSS and WSSQ as mediators between BMI and environment domain of WHOQOL-BREF (ENV). (e) Sequential mediation model with PWSS and WSSQ as mediators between Body Mass Index and question 1 (overall QoL) of WHOQOL-BREF (Q1). (f) Sequential mediation model with PWSS and WSSQ as mediators between BMI and question 2 (general health) of WHOQOL-BREF (Q2).
Results
Among 1044 students (mean age = 21.27 ± 2.54 years) who participated in the present study, 727 were female (69.6%) and 317 were male (30.4%). The majority were Chinese (53.5%), followed by Malay (31.3%) and Indian (8.2%). Participants were predominantly undergraduates (90.4%). Regarding the anthropometry of the participants, the mean weight was 58.40 kg (±14.50), the mean height was 162.80 cm (±8.80), and the mean BMI was 21.92 kg/m2 (±4.55). The mean PWSS score was 1.84 out of 10 (±2.37), and the mean WSSQ score was 29.29 out of 60 (±11.41; Table 1).
Participant characteristics (n = 1044).
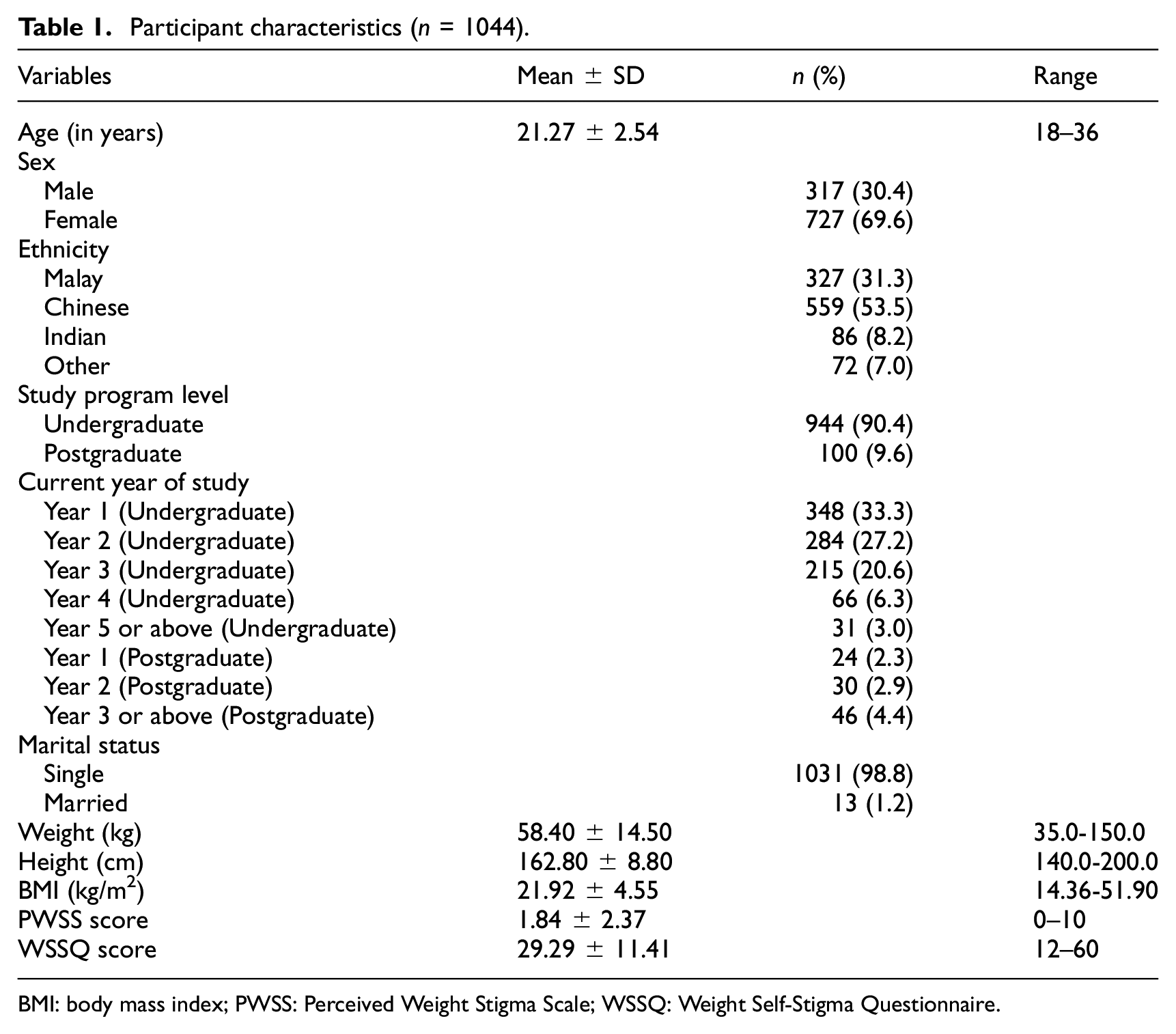
BMI: body mass index; PWSS: Perceived Weight Stigma Scale; WSSQ: Weight Self-Stigma Questionnaire.
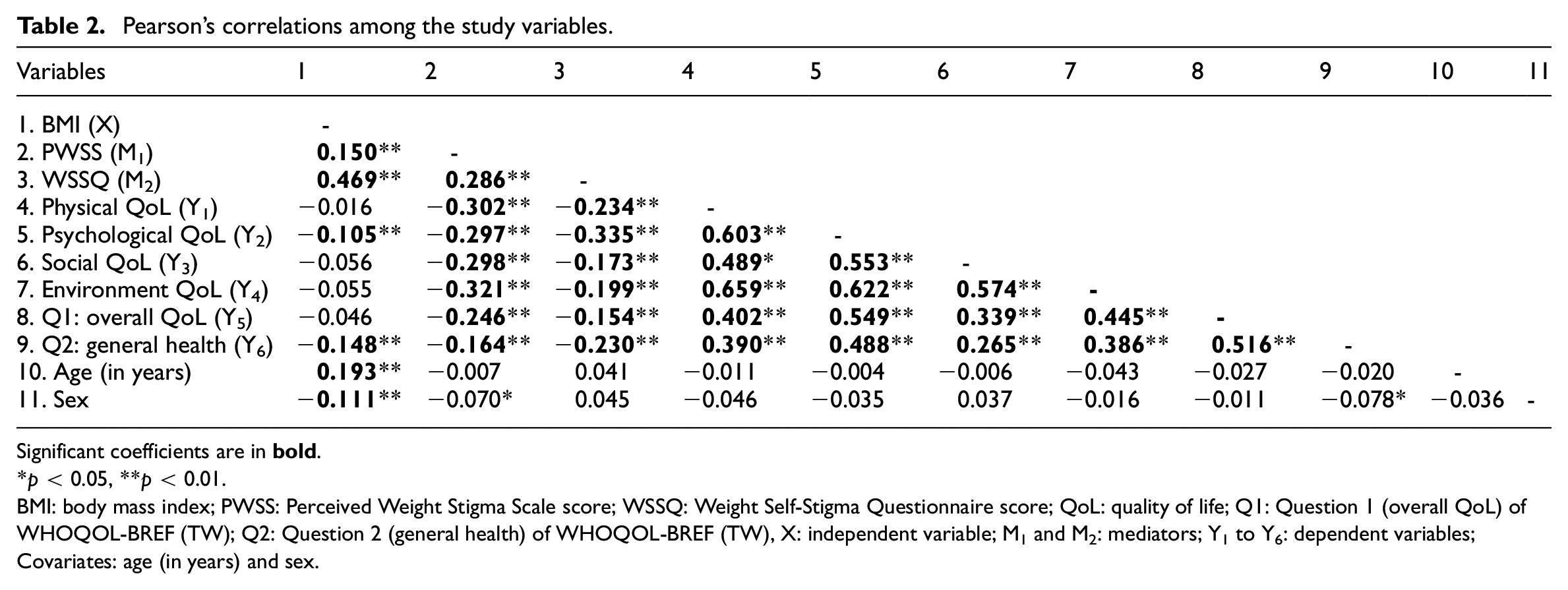
Pearson correlation analysis showed that BMI was positively correlated with the PWS, WRSS, and age (r = 0.150 to 0.469, p < 0.01), and negatively correlated with the psychological domain of QoL (r = −0.105, p < 0.01). PWS had correlations with WRSS (r = 0.286, p < 0.01), all QoL domain scores (r = −0.297 to −0.321; p < 0.01), the two general QoL questions (r = −0.246 with overall QoL (p < 0.01), and r = −0.164 with general health (p < 0.01)). WRSS was also negatively correlated with all QoL domain scores (r = −0.173 to −0.335, p < 0.01) and the two general QoL questions (r = −0.154 with overall QoL (p < 0.01); and r = −0.230 with general health (p < 0.01); Table 2).
Pearson’s correlations among the study variables.
Significant coefficients are in
p < 0.05, **p < 0.01.
BMI: body mass index; PWSS: Perceived Weight Stigma Scale score; WSSQ: Weight Self-Stigma Questionnaire score; QoL: quality of life; Q1: Question 1 (overall QoL) of WHOQOL-BREF (TW); Q2: Question 2 (general health) of WHOQOL-BREF (TW), X: independent variable; M1 and M2: mediators; Y1 to Y6: dependent variables; Covariates: age (in years) and sex.
Six mediation models were used to examine the mediating effects of PWS and WRSS in the relationship between BMI and various QoL domains (Figure 1 and Table 3). Model A showed a positive and statistically significant direct effect of BMI on physical QoL (β = 0.0651, p < 0.001), while the indirect effect from BMI to physical QoL via PWS and WRSS was statistically significant and negative (β = −0.0038, p < 0.001). Model B showed a positive and statistically significant direct effect of BMI on psychological QoL (β = 0.0402, p < 0.01), with a statistically significant and negative indirect effect via PWS and WRSS (β = −0.0060, p < 0.001). Model C showed that the direct effect of BMI on social QoL was positive but not statistically significant (β = 0.0301, p = 0.1919), while the indirect effect from BMI to social QoL via PWS and WRSS was statistically significant and negative (β = −0.0027, p < 0.001). Model D showed a positive, but not statistically significant, direct effect of BMI on environmental QoL (β = 0.0354, p = 0.0665), with a significant and negative indirect effect from BMI to environmental QoL via PWS and WRSS (β = −0.0027, p < 0.001). Model E showed a positive but non-significant direct effect of BMI on the overall QoL (β = 0.0073, p = 0.2201), while the indirect effect from BMI to overall QoL via PWS and WRSS was statistically significant and negative (β = −0.0006, p < 0.001). Finally, Model F showed a negative but non-significant direct effect of BMI on general health (β = −0.0129, p = 0.0703), with a statistically significant and negative indirect effect from BMI to general health via PWS and WRSS (β = −0.0011, p < 0.001). Full regression results are presented in Supplemental Table 1.
Mediation models assessing mediated effects of perceived weight stigma and weight-related self-stigma from body mass index (BMI) to quality of life (QoL).
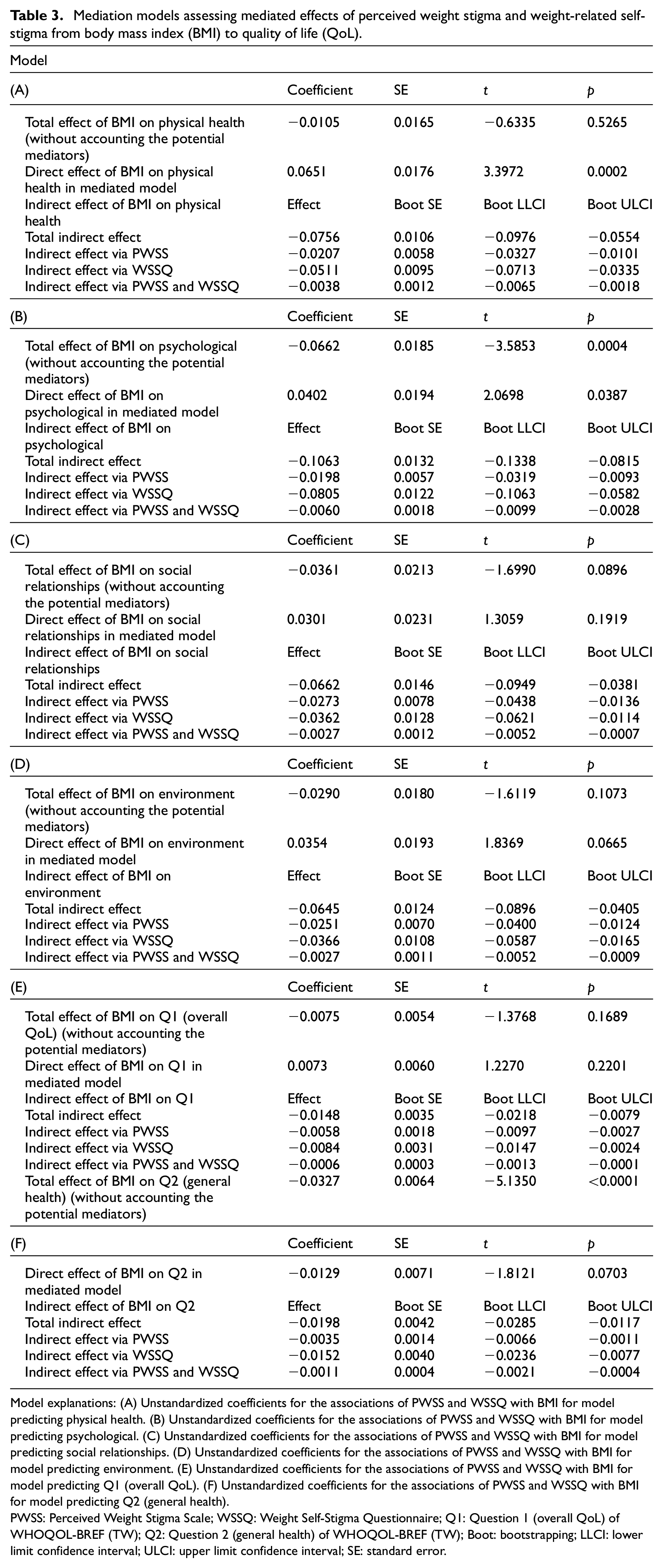
Model explanations: (A) Unstandardized coefficients for the associations of PWSS and WSSQ with BMI for model predicting physical health. (B) Unstandardized coefficients for the associations of PWSS and WSSQ with BMI for model predicting psychological. (C) Unstandardized coefficients for the associations of PWSS and WSSQ with BMI for model predicting social relationships. (D) Unstandardized coefficients for the associations of PWSS and WSSQ with BMI for model predicting environment. (E) Unstandardized coefficients for the associations of PWSS and WSSQ with BMI for model predicting Q1 (overall QoL). (F) Unstandardized coefficients for the associations of PWSS and WSSQ with BMI for model predicting Q2 (general health).
PWSS: Perceived Weight Stigma Scale; WSSQ: Weight Self-Stigma Questionnaire; Q1: Question 1 (overall QoL) of WHOQOL-BREF (TW); Q2: Question 2 (general health) of WHOQOL-BREF (TW); Boot: bootstrapping; LLCI: lower limit confidence interval; ULCI: upper limit confidence interval; SE: standard error.
Discussion
The present study is the first to examine the relationship between BMI and QoL among Malaysian young adults, with a focus on the sequential mediating roles of PWS and WRSS. By examining both direct and indirect effects, the present study’s findings provide valuable insights into how weight stigma may mitigate the positive effects of a healthy BMI on QoL.
The present study found that BMI was positively correlated with both PWS and WRSS, suggesting that young Malaysian adults with higher BMI were more likely to experience weight-related stigma. This is consistent with previous research (Lin et al., 2023; Nicolau et al., 2023; Tomiyama et al., 2018), which has shown that individuals with higher BMIs are often targets of weight discrimination and internalized weight stigma. Moreover, the significant negative correlations between BMI and the psychological domain of QoL further support previous findings in the literature, indicating that individuals with higher BMI may experience adverse psychological outcomes, including lower self-esteem, depression, and anxiety (Apple et al., 2018; Luah et al., 2024; Okolo et al., 2024; Ward et al., 2024).
A negative relationship between weight stigma and different domains of QoL was observed in the present study. This finding is consistent with recent research showing that stigma is significantly correlated with increased mental health issues, such as anxiety and depression, thereby reducing QoL (Lin et al., 2024). Young adults are prone to internalizing stigma, which lowers their self-esteem and discourages them from seeking help, thereby exacerbating their mental health problems. Additionally, the developmental stage of young adulthood makes individuals more vulnerable to the negative impact of stigma on their identity and overall well-being (Prizeman et al., 2023). These findings emphasize the need for targeted interventions aimed at addressing stigma and improving the psychological health and QoL of young adults facing these challenges.
The present study also provides insights into the mediating roles of PWS and WRSS in the relationship between BMI and different QoL domains among Malaysian young adults. More specifically, results in the present study showed that the indirect effects of BMI on physical, psychological, social, and environmental QoL domains via PWS and WRSS were consistently negative. This suggests that higher BMI may be associated with increased PWS and WRSS, which in turn, may be associated with poorer QoL. Young adults with higher BMIs may perceive weight-related stigma, which is associated with feelings of shame, and decreased self-esteem (Gan et al., 2022; Lin et al., 2023). This PWS may act as a mediator that is associated with lower QoL. In addition, WRSS may further exacerbate these negative feelings, potentially leading to even worse QoL outcomes. The mediation results were consistent with those observed in a study of children in Hong Kong (Fan et al., 2021). In general, the findings highlight the need for targeted interventions that not only focus on promoting healthy BMI, but also address the stigma associated with higher weight, with the goal of improving the overall well-being and QoL of young adults facing these challenges.
Interestingly, the present study also found a positive direct effect of BMI on psychological QoL, despite the overall negative indirect effect through weight stigma. This suppression effect may reflect the possibility that some individuals with higher BMI have more acceptance of their bodies, especially among cultural subgroups where larger body sizes are more socially acceptable. Moreover, self-selection bias in the survey may have resulted in the inclusion of individuals with higher BMI who already had more positive psychological well-being or greater confidence in their body image, which may have influenced the observed association. Future research is warranted to explore these potential explanations more deeply.
However, findings of the present study on the direct effects of BMI on social QoL, environmental QoL, and general health were not significant, suggesting that these aspects of QoL may be less directly associated with BMI. The relationship between BMI and social QoL is particularly complex because the extant literature presents mixed results. For instance, a study conducted in Brazil found that individuals who had morbid obesity reported significantly lower social QoL compared to those with normal weight, while in another study, no significant difference was observed between adults who were normal weight and adults who were overweight (Pimenta et al., 2015). This suggests that while having obesity can negatively impact social interactions and relationships, the extent of this effect may differ across various weight categories. Similarly, in the environmental QoL domain, the same study found that individuals with normal weight had better QoL than both individuals with obesity and morbid obesity, with no significant difference between these two groups (Pimenta et al., 2015). This may be due to the mobility and accessibility challenges that individuals in these groups often face, which can limit their ability to fully engage with their environment. These findings suggest that BMI may not be directly associated with specific aspects of QoL, such as social and environmental QoL domains found in the present study. Therefore, interventions should focus on improving psychological support, reducing stigma, and enhancing access to healthy environments, irrespective of BMI.
Interestingly, in several models (e.g. physical QoL, social QoL, environmental QoL, and overall QoL), the total effect of BMI on QoL was not statistically significant, while the indirect effects via PWS and WRSS were. According to mediation theory (Hayes, 2018), a significant total effect is not a necessary condition for mediation to occur. It is possible for significant indirect effects to exist in the absence of a significant total effect (a phenomenon often referred to as indirect-only mediation or suppression). This typically occurs when the direct and indirect effects operate in opposite directions, potentially reducing the total effect. For example, in Model B, although the correlation between BMI and psychological QoL was positive, the effect became negative after accounting for the mediating roles of PWS and WRSS. This suggests that when stigma is not accounted for, higher BMI is associated with higher psychological QoL. However, once stigma is considered, the association between BMI and psychological QoL appears negative. In the present study’s findings, the indirect effects of BMI on QoL outcomes through PWS and WRSS were negative, suggesting that these stigma-related processes may reverse the positive direct effects of BMI on some aspects of QoL. These findings highlight the critical role of stigma-related processes in shaping how body weight influences well-being.
The present study’s findings highlight the importance of addressing weight stigma in improving the QoL of young adults, particularly in Malaysia. Public health interventions should focus on reducing weight stigma, which was found to negatively associated with QoL across multiple domains. Potential interventions include promoting positive body image through university-based psychoeducation programs, providing mental health support for those affected by stigma, and introducing public awareness campaigns that normalize body diversity. Additionally, training healthcare professionals to recognize and reduce weight bias in clinical settings could help to foster more inclusive and supportive care. Integrating these stigma-reduction approaches into weight management programs may enhance their effectiveness. These approaches could improve the well-being of young adults by reducing the psychological effects of weight stigma and promoting more supportive environments, particularly among young people in university settings.
The key strength of the present study was the use of a sequential mediation model, which provided a deeper understanding of the complex relationship between BMI, PWS, WRSS, and QoL. Another strength was the use of a relatively large sample which helped provide a more comprehensive understanding of this relationship in the Malaysian context. However, several limitations of the present study must be acknowledged. The cross-sectional design limits causal inference, making it difficult to determine the directionality of the observed relationships. In addition, the reliance on self-report data for PWS and WRSS might have introduced social desirability bias. Another limitation was the use of convenience sampling, which may limit the generalizability of the findings to the broader population of Malaysian young adults. Therefore, future research should address these limitations by using longitudinal designs to explore causal relationships, incorporating/developing objective measures of weight stigma by quantified stigma (Shrivastava et al., 2013), and using more representative sampling methods to increase the robustness and generalizability of the findings. Moreover, examining the potential moderating effects of ethnicity and cultural factors may also provide valuable insight into the experiences of weight stigma across different demographic groups.
Conclusion
The present study’s findings highlight the sequential mediating effect of both PWS and WRSS in the relationship between BMI and QoL of Malaysian young adults. These results suggest that addressing both PWS and WRSS, alongside enhancing mental health support, may be beneficial components of public health initiatives aiming to improve better physical, and mental well-being in young adults.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251358460 – Supplemental material for Relationship between body mass index and quality of life among Malaysian young adults: Sequential mediated effects of perceived weight stigma and weight-related self-stigma
Supplemental material, sj-docx-1-hpq-10.1177_13591053251358460 for Relationship between body mass index and quality of life among Malaysian young adults: Sequential mediated effects of perceived weight stigma and weight-related self-stigma by Wan Ying Gan, Yu-Ting Huang, Wen-Li Hou, Serene En Hui Tung, Wai Chuen Poon, Yan-Li Siaw, Nadia Bevan, Mark D. Griffiths, Jung-Sheng Chen, I-Ching Lin, Ru-Yi Huang and Chung-Ying Lin in Journal of Health Psychology
Footnotes
Acknowledgements
We thank the participants for their participation in the study.
Author contributions
Data sharing statement
The data that support the present findings are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by (received funding from) the National Science, and Technology Council, Taiwan (NSTC 112-2410-H-006-089-SS2).
Ethics approval
Ethical approval for the study protocol was obtained from the Ethics Committee for Research Involving Human Subject of Universiti Putra Malaysia (JKEUPM; reference number: JKEUPM-2023-1324) prior to the data collection of the study.
Informed consent
The information sheet and informed consent form appeared on the first page of the survey. Participants agree to the study before they proceed to complete the online survey.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.