
Abstract
This study aimed to identify factors influencing cervical cancer screening participation among women aged 30–65, focusing on HPV knowledge, cancer screening perception, health anxiety, and behaviors for protection against sexually transmitted diseases (STDs). A total of 1755 women participated, with a cervical cancer screening rate of 56.2%. Logistic regression analysis revealed several significant predictors of screening participation, including higher health anxiety, history of STDs, chronic diseases, increased HPV knowledge, positive behaviors for STDs prevention, increasing age, being married or divorced, light physical activity, healthier dietary habits, and living in the Mediterranean region. These findings highlight the interplay of demographic, psychological, and health-related factors in cervical cancer screening decisions. To improve screening rates, public health initiatives should enhance HPV knowledge, address health anxiety, and promote STDs prevention behaviors while considering regional and demographic differences. Further research should comprehensively explore how these factors interact in various settings.
Keywords
Introduction
Human papillomavirus (HPV) is the leading preventable cause of infection-related cancers in women and a major public health threat, especially due to its association with cervical cancer (de Martel et al., 2020). HPV types 16 and 18 account for ~70% of cervical cancers (World Health Organization, 2024b). It is primarily transmitted through sexual contact, though non-sexual transmission reported (Tchouaket et al., 2023). Key risk factors for HPV include multiple sexual partners, HIV infection, and young age. The progression to cervical cancer is further influenced by smoking, oral contraceptive use, high parity, immunosuppression, and co-infection with other sexually transmitted diseases (STDs; Ezechi et al., 2023; Tchouaket et al., 2023; World Health Organization, 2024c). In 2022, World Health Organization (WHO) estimated that 660,000 women were diagnosed with cervical cancer globally, with 350,000 deaths (IA for R on C World Health Organization, 2024). Early detection and treatment make cervical cancer highly treatable (Asthana et al., 2020). The Papanicolaou (Pap) Smear (PS) and HPV-DNA analysis are used for screening, with HPV-DNA testing providing reliable results (Ali et al., 2024). Despite high HPV prevalence in young women, two out of three women aged 30–49 have never undergone screening (Bruni et al., 2022). WHO recommends the HPV vaccine and regular HPV-DNA screening every 5–10 years starting at age 30 (World Health Organization, 2021, 2024c). Screening reduces cervical cancer incidence and mortality (Partridge et al., 2014). Barriers to cervical cancer screening vary regionally and socio-culturally, but the literature identifies factors such as shame related to gynecological exams, low knowledge about cervical cancer/HPV infection, the gender of healthcare providers, concerns about privacy during the examination, the misconception of feeling healthy, fear of the procedure, fear of pain, stigma, fear of a cancer diagnosis, difficulty accessing healthcare, low health literacy, low education levels, negative lifestyle habits, and low perceived awareness and risk perception (Ahadinezhad et al., 2024; Ahmed et al., 2024; Shrestha et al., 2022). Organization for Economic Co-operation and Development (OECD) data show that cervical cancer screening rates vary, with a 53.4% screening rate for women aged 20–69 in the past 3 years (Organisation for Economic Co-operation and Development, 2023), and 47% in the European Union (EU) countries (Eurostat, 2020). WHO reports that cervical cancer incidence and mortality are highest in low- and middle-income countries due to limited access to vaccines, screening, and treatment services (World Health Organization, 2024a, 2024d). Inadequate screening programs in these countries still contribute to a significant burden of cervical cancer (Smith et al., 2023). Studies show that women with limited HPV and cervical cancer knowledge are less likely to undergo screening (Ahmed et al., 2024; Derbie et al., 2021; Yirsaw et al., 2024). STDs are a risk factor for HPV, which can lead to cervical cancer. Increasing protective behaviors and cancer awareness may improve screening participation rates (Kawata and Koga, 2020; United States National Cancer Institute, 2024).
Although some studies in Türkiye have investigated factors affecting cervical cancer screening participation, there remains a need for comprehensive research that simultaneously evaluates psychosocial factors such as health anxiety, HPV knowledge, cancer screening perception, and behaviors protecting against STDs. The distinctive socio-cultural characteristics of Türkiye, along with regional variability in healthcare access, variations in health literacy, and prevailing cultural views on women’s health, underscore the need for further research to accurately comprehend cervical cancer screening behaviors.
Previous studies in Türkiye have primarily focused on demographic and knowledge-based determinants (Dost and Ozdemir, 2024; Sozmen et al., 2016), while the complex interplay of psychological factors and protective health behaviors has not been sufficiently addressed. Additionally, regional differences within Türkiye significantly affect the utilization of health services, yet these have not been thoroughly examined (Sozmen et al., 2016).
Although cervical cancer screening rates in Türkiye remain below the OECD average (Organisation for Economic Co-operation and Development, 2023), psychosocial factors such as the country’s unique socio-cultural structure, regional disparities in access to healthcare services, and women’s health perceptions significantly influence screening participation. Therefore, a comprehensive and simultaneous evaluation of these factors specific to Türkiye is critical for the development of effective public health policies.
Based on the assumption that knowledge and attitudes influence individuals’ practices or behaviors by altering risk perception (Leval et al., 2011), this study aims to examine the impact of knowledge levels about HPV and cervical cancer, perceptions of cancer screening, health anxiety levels, and behaviors related to protection against STDs on the decision to undergo cervical cancer screening tests (Pap Smear and HPV-DNA analysis) among women aged 30–65 in Türkiye.
Methods
Research design and sampling method
This study is cross-sectional in type. The sample size was calculated using a 50% PS participation rate (p = 0.5), a 95% confidence level (Z = 1.96), a 5% margin of error (d = 0.05).
Based on this, the initial sample size was calculated as:
Given that cluster sampling was used, a design effect (DEFF) of 2 was applied to account for the sampling structure:

Accordingly, the minimum sample size required for the study was determined to be 769 participants. However, to enhance the generalizability of the sample to the population and improve the statistical power of the study, a total of 1755 women were included. The Republic of Türkiye Ministry of Health, General Directorate of Public Health, Cancer Department, highlights the necessity of conducting PS and HPV-DNA testing every 5 years for women aged 30–65 as part of the national cervical cancer screening program (Republic of Turkiye Ministry of Health General Directorate of Public Health, 2023). Therefore, women aged 30–65 from across Türkiye were included in the study. In this study, the dependent variable was defined as whether women had undergone a cervical smear test at least once in their lifetime. Inclusion criteria consisted of having at least one sexual partner, being able to express oneself verbally or in writing, being willing to participate, and the ability to read and understand Turkish. Exclusion criteria included women with no sexual experience, those with medical conditions preventing the performance of PS, and those who did not provide consent to participate.
Data collection process
The data collection process was conducted between January 10 and February 10, 2025. During the informed consent process, participants were told that completing the questionnaire would take approximately 15–20 minutes, that no personal information would be included, that the responses would be used solely for scientific research purposes, and that questions could only be answered after consent. In addition to socio-demographic questions, participants were asked about the Human Papillomavirus Knowledge Scale (HPV-KS), Cancer Screening Perception Scale (CSPS), Health Anxiety Inventory (HAI), and STD Behavior Scale (STD-SCS). These questions were provided to participants via a link created through Google Forms. Initially, the survey was distributed through acquaintances and university students from different regions of Türkiye, who were asked to share the link with their networks. Each participant was requested to forward the link via mobile devices and/or social media platforms to their communication networks. This method allowed us to reach a wide range of participants from various geographical regions.
Instruments
Human Papilloma Virus Knowledge Scale
The HPV-KS, developed by Waller et al. (2013), was adapted to Turkish by Demir Bozkurt and Ozdemir and consists of 33 items. The scale has four subdomains: “General HPV knowledge,” “HPV testing knowledge,” “HPV vaccine knowledge,” and “HPV vaccine availability.” The total score ranges from 0 to 33, with higher scores indicating comprehensive knowledge in the four subdomains. The Cronbach’s alpha for the full scale is 0.96, indicating high internal consistency, and the Turkish version is reported as valid and reliable (Demir Bozkurt and Ozdemir, 2023).
Cancer Screening Perception Scale
The CSPS, developed by Mahmood et al. (2018), was adapted to Turkish by Kıran et al. (2024). The scale consists of 26 items and five subdomains: “Perceived severity,” “Perceived susceptibility,” “Perceived benefits,” “Perceived barriers,” and “Cues for action.” It is a Likert-type scale ranging from 1 (Strongly disagree) to 6 (Strongly agree). As the average response approaches 6, cancer screening perception increases, and as it approaches 1, perception decreases. The “perceived susceptibility” subdomain is reverse-coded. The general Cronbach’s alpha of the scale is 0.849, indicating that the Turkish version is valid and reliable (Kıran et al., 2024).
Health Anxiety Inventory
The HAI, developed by Salkovskis et al. (2002), was adapted into Turkish by Aydemir et al. (2013) The 18-item scale includes 14 items assessing mental state with four response options, while four items focus on evaluating mental state under the assumption of a serious illness. Each item is scored from 0 to 3; higher scores indicate higher levels of health anxiety. The Cronbach’s alpha for internal consistency of the scale is 0.918, indicating that the Turkish version is valid and reliable (Aydemir et al., 2013).
Scale of behaviors for protection from sexually transmitted diseases
The STD-SCS, developed by Kılavuz and Yiğit, consists of 21 items and uses a five-point Likert scale. It includes two subscales: knowledge and protection, and attitudes. Each item is scored as 1–2–3–4–5, with 10 items being reverse-coded. The highest possible score on the scale is 105, and the lowest score is 21. Higher scores indicate an increase in positive behaviors for the protection against STDs. The overall Cronbach’s alpha coefficient of the scale is 0.911, indicating that it is valid and reliable (Kılavuz and Yigit, 2023).
Statistical analysis
Categorical variables (nominal and ordinal) were expressed as frequency counts and percentages, while numeric variables were summarized using means and standard deviations. To evaluate the effects of categorical independent variables on the outcome variable, a chi-square test was conducted. The Kolmogorov–Smirnov test was applied to assess the normality of data distribution, and the results confirmed a normal distribution. An independent samples t-test was used to examine the relationship between numeric independent variables and the dependent variable. Finally, binary logistic regression (LR) was performed to investigate the combined effects of all variables on the outcome. All analyses were conducted using SPSS 28.0, and a p-value of ⩽0.05 was considered statistically significant.
Results
An overview of the demographic characteristics of our sample is provided in Table 1.
Participants’ descriptives and the effects of these variables on the frequency of undergoing cervical cancer screening tests.
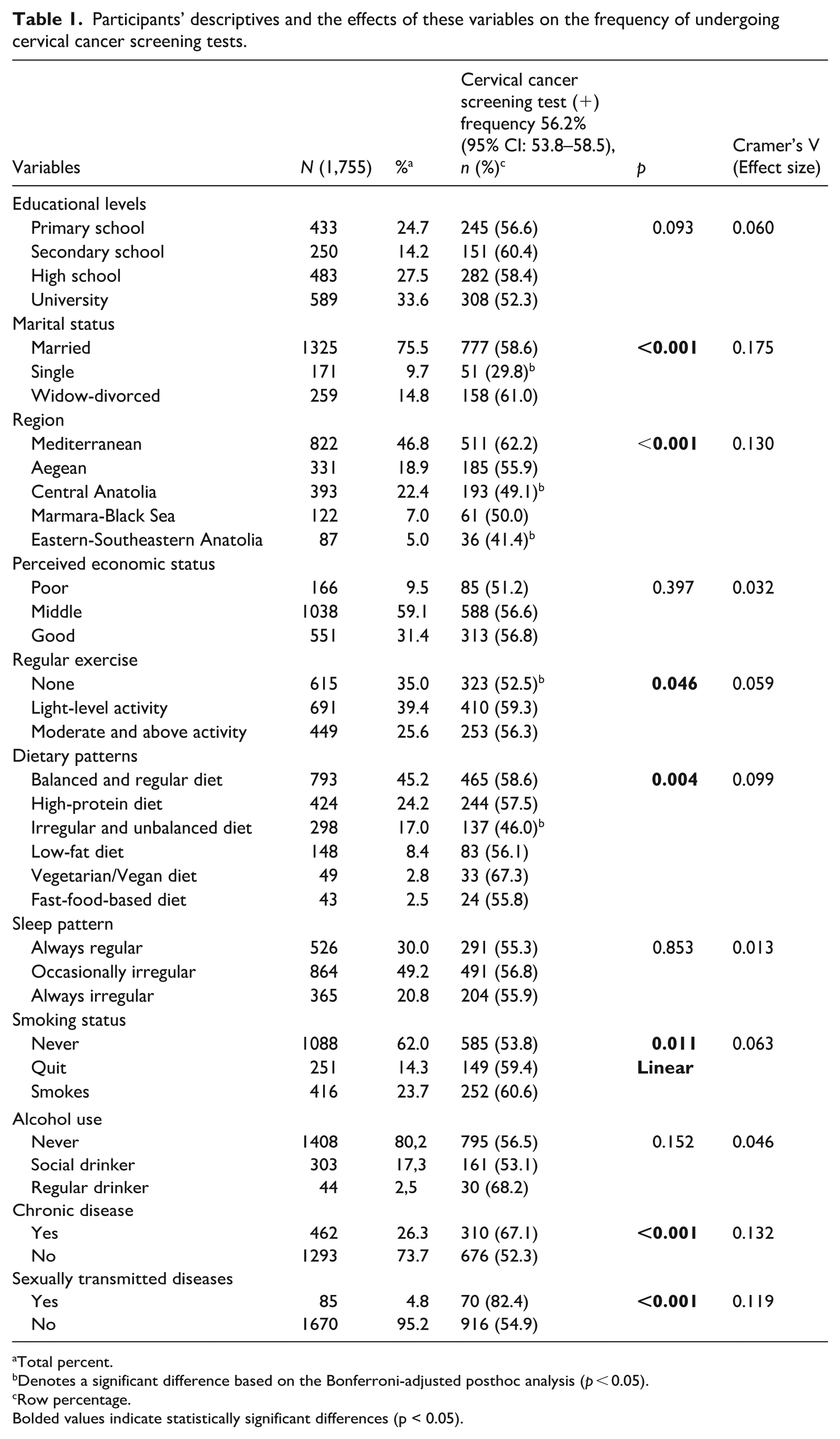
Total percent.
Denotes a significant difference based on the Bonferroni-adjusted posthoc analysis (p < 0.05).
Row percentage.
Bolded values indicate statistically significant differences (p < 0.05).
In this study, the cervical cancer screening rate was 56.2% (95% CI: 53.8–58.5). Screening was lower among unmarried participants and those living in Eastern-Southeastern Anatolia and Central Anatolia. Women with irregular diets or low physical activity were less likely to be screened, whereas screening was more common among those with chronic diseases, a history of STDs, or who smoked. Education level, perceived economic status, sleep patterns, and alcohol use did not affect screening frequency (Table 1).
Participants who had been screened were older, with a mean age of 46.71 years compared to 44.55 years for those who had not been screened (p < 0.001, Cohen’s d = 0.21). Additionally, those who underwent screening had a higher mean number of children (2.02 vs 1.76, p < 0.001, d = 0.23). No significant difference was observed in body mass index (BMI) between the two groups (p = 0.251, d = 0.05).
Women in the screened group scored slightly higher on the total CSPS (115.70 vs 113.57, p = 0.036, d = 0.10). Among its subscales, significant differences were found in perceived benefits (23.12 vs 23.55, p = 0.006, d = 0.07), perceived barriers (20.43 vs 20.82, p = 0.014, d = 0.13), and cues for action (27.15 vs 27.59, p = 0.014, d = 0.06). However, no significant differences were found in perceived severity (p = 0.732, d = 0.01) or perceived susceptibility (p = 0.926, d < 0.01). The screened group also exhibited significantly higher levels of health anxiety, as indicated by HAI scores (20.28 vs 19.00, p = 0.004, d = 0.14). With respect to STD-related protective behaviors, participants who had undergone screening had higher total STD-SCS scores (73.51 vs 71.90, p = 0.001, d = 0.16). This difference was significant both in the knowledge and protection subscale (49.26 vs 49.86, p = 0.007, d = 0.12) and the attitude subscale (22.64 vs 22.94, p < 0.001, d = 0.20). Participants who had been screened also showed higher total HPV knowledge, with mean HPV-KS scores of 17.69 versus 16.18 (p < 0.001, d = 0.42). Subscale analysis revealed significant differences in general HPV knowledge (6.92 vs 7.59, p < 0.001, d = 0.22) and HPV vaccine availability (2.19 vs 2.33, p < 0.001, d = 0.17). No significant group differences were observed in HPV testing knowledge (p = 0.382, d = 0.03) or HPV vaccine knowledge (p = 0.622, d = 0.01; Table 2).
Comparison of variables in cervical cancer screening test participation status.
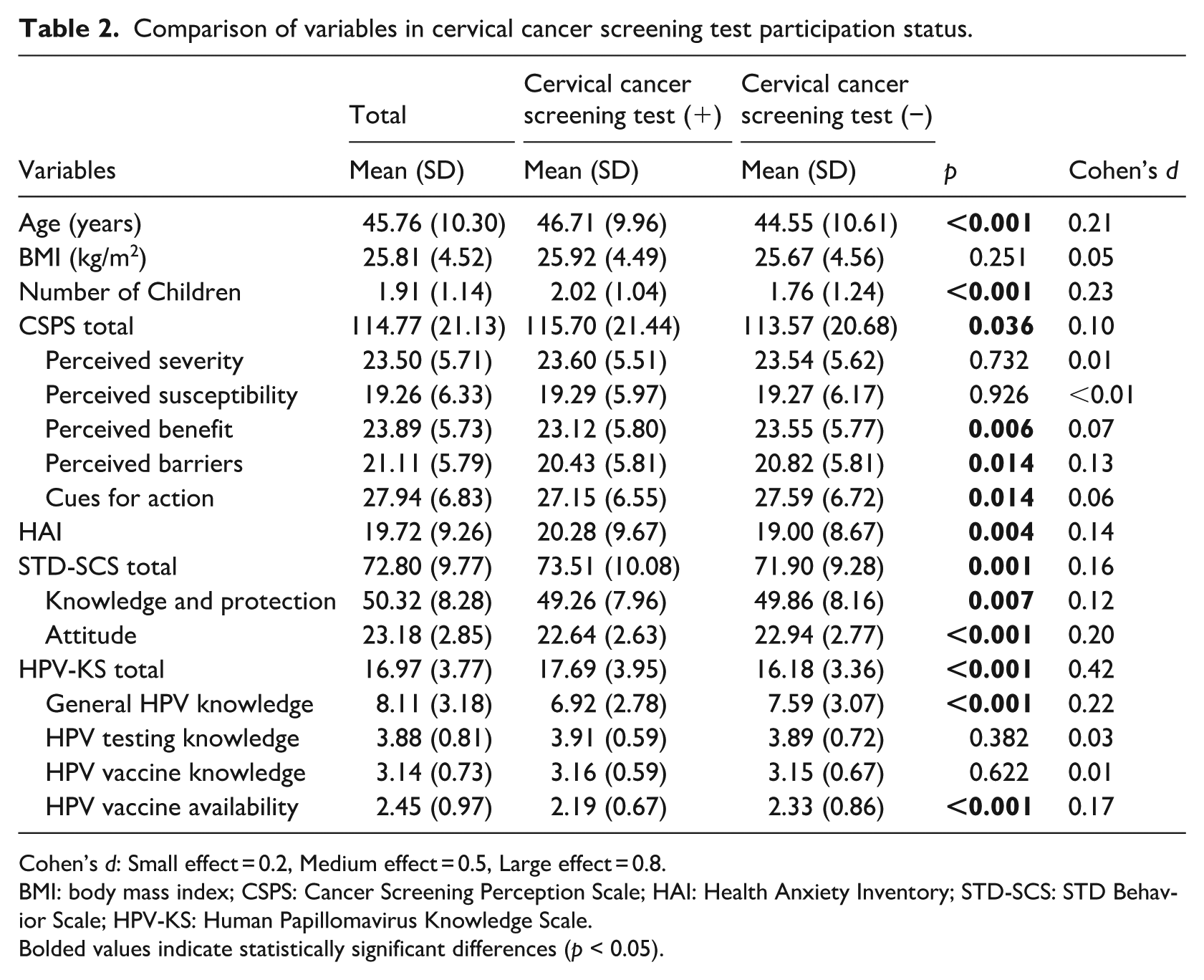
Cohen’s d: Small effect = 0.2, Medium effect = 0.5, Large effect = 0.8.
BMI: body mass index; CSPS: Cancer Screening Perception Scale; HAI: Health Anxiety Inventory; STD-SCS: STD Behavior Scale; HPV-KS: Human Papillomavirus Knowledge Scale.
Bolded values indicate statistically significant differences (p < 0.05).
Variables found to be significant in the univariate analysis were included in the multiple logistic regression model, which was conducted using the backward elimination method. The logistic regression results demonstrated that the model was statistically significant (Omnibus test: χ² = 229.738, p < 0.001). The model’s fit to the data was supported by a −2 Log Likelihood (−2LL) value of 2176.309, and the Hosmer-Lemeshow test (χ² = 6.904, p = 0.547) confirmed adequate goodness-of-fit, indicating consistency between predicted and observed outcomes. The Cox & Snell R² (0.123) and Nagelkerke R² (0.164) values indicate that the model explains approximately 12.3% and 16.4% of the variance in the dependent variable, respectively. Multiple logistic regression analysis identified several factors influencing cervical cancer screening test participation. Women from the Mediterranean region were significantly more likely to participate compared to those from Eastern-Southeastern Anatolia (Exp(B) = 1.914, p = 0.009). Marital status was a strong predictor, with married (Exp(B) = 3.340, p < 0.001) and widow/divorced women (Exp(B) = 3.495, p < 0.001) having higher odds of participation than single women. The presence of chronic disease (Exp(B) = 1.700, p < 0.001) and a history of STDs (Exp(B) = 4.000, p < 0.001) were also associated with increased participation. Dietary habits played a role, as those following a vegetarian/vegan diet (Exp(B) = 2.379, p = 0.014) or a high-protein diet (Exp(B) = 1.568, p = 0.007) had higher odds of participation compared to those with an irregular and unbalanced diet. Regular exercise at a light level was positively associated (Exp(B) = 1.442, p = 0.003), while moderate level exercise showed no significant effect. Additionally, increasing age (Exp(B) = 1.011, p = 0.037), higher HAI scores (Exp(B) = 1.017, p = 0.004), greater STD-SCS scores (Exp(B) = 1.012, p = 0.012), and higher HPV knowledge scores (Exp(B) = 1.107, p < 0.001) were all significant predictors of screening participation (Table 3).
Multiple logistic regression results of factors influencing cervical cancer screening test participation.
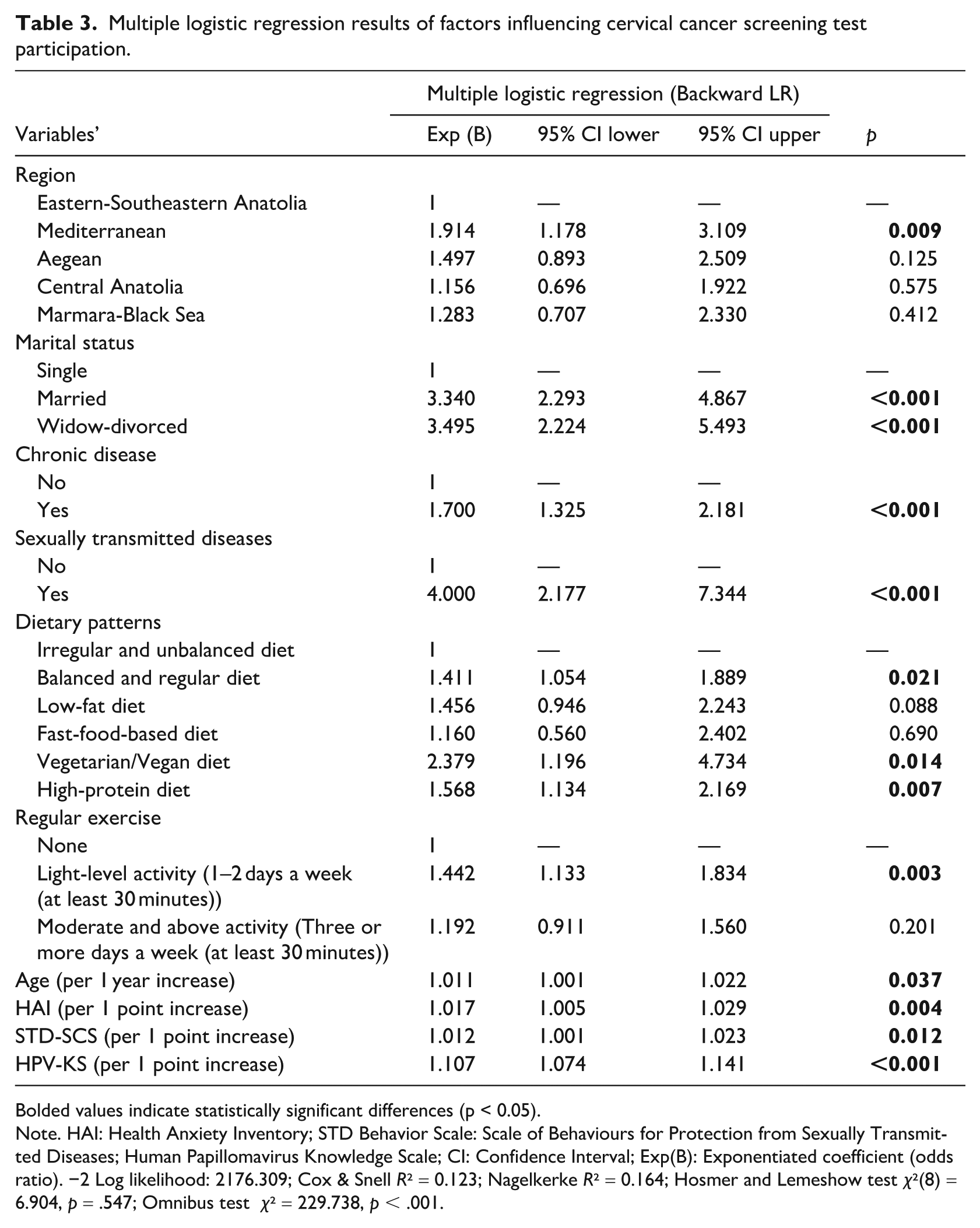
Bolded values indicate statistically significant differences (p < 0.05).
Note. HAI: Health Anxiety Inventory; STD Behavior Scale: Scale of Behaviours for Protection from Sexually Transmitted Diseases; Human Papillomavirus Knowledge Scale; CI: Confidence Interval; Exp(B): Exponentiated coefficient (odds ratio). −2 Log likelihood: 2176.309; Cox & Snell R² = 0.123; Nagelkerke R² = 0.164; Hosmer and Lemeshow test χ²(8) = 6.904, p = .547; Omnibus test χ² = 229.738, p < .001.
Discussion
This study aimed to investigate the key factors influencing cervical cancer screening participation among Turkish women aged 30–65, focusing on psychosocial variables such as HPV knowledge, cancer screening perception, health anxiety, and protective behaviors against sexually transmitted diseases. The findings revealed a screening rate of 56.2%, with significant predictors including increased health anxiety, history of STDs, chronic illnesses, higher HPV knowledge, positive preventive behaviors, demographic factors, and regional differences.
Frequency of participation in cervical cancer screening
In this study, approximately half of the participants underwent cervical cancer screening. Compared to international literature, our findings show some differences. According to OECD data, Türkiye’s rate is 32.5%, below the OECD average of 53.4% (Organisation for Economic Co-operation and Development, 2023). However, Türkiye’s cervical cancer screening rates are similar to the European average of 46% (Eurostat, 2020) and higher than many developing countries such as those in Africa (27.2%) and Arab countries (18.2%) (Ahmed et al., 2024; Nwabichie et al., 2018). Türkiye’s cervical cancer screening rates are similar to the European average but lower than in developed countries. However, they are higher than in many developing nations in Africa, the Arab countries, and South Asia. Higher screening rates in developed countries highlight the importance of strengthening national screening programs, focusing on accessibility, awareness, and effectiveness. Comprehensive strategies such as implementing mobile screening units in rural areas with limited access to healthcare services and subsidizing screening costs can be developed.
Factors increasing participation in cervical cancer screening
Increase in HPV knowledge level
In the univariate analysis, both the total score of the HPV-KS and the subdimensions General HPV Knowledge and HPV Vaccine Availability were significantly higher among women who underwent cervical cancer screening. Furthermore, the HPV-KS total score remained a significant predictor of screening participation in multivariate analysis. The findings of this study show that increasing HPV knowledge enhances cervical cancer screening rates. Supporting this, a study conducted in Türkiye reported that education on HPV screening tests and HPV vaccines positively influenced participants’ perceptions regarding the benefits of undergoing Pap Smear tests (Gul Oztas and Isik, 2025). Our results align with existing research, highlighting the impact of knowledge on screening participation. Previous studies have found that knowledge about HPV and cervical cancer increases participation in screening (Ayenew et al., 2020). In Ethiopia, HIV-positive women with good knowledge about cervical cancer were 3.5 times more likely to be screened (Dessalegn Mekonnen, 2020). Similarly, studies in Arab countries, Nepal, and Sub-Saharan Africa have shown that lack of knowledge is a major barrier, while research in India, Singapore, Spain, Kazakhstan, and Argentina confirms that better knowledge increases screening rates (Ahmed et al., 2024; George, 2021; Huang and Tan, 2024; Issa et al., 2021; McFarland et al., 2016; Paolino and Arrossi, 2011; Puig-Tintoré et al., 2008; Shrestha et al., 2022). In conclusion, knowledge about HPV and cervical cancer plays a crucial role in encouraging the uptake of screening tests (Faradisa et al., 2020). The findings of our study suggest that increasing knowledge about HPV and cervical cancer is one of the key factors in promoting participation in screening tests. In this regard, health policies should include strategies to enhance knowledge and awareness, which is vital for the widespread adoption of cervical cancer screening programs.
Cancer screening perception
In this study, in univariate analyses, the total score of the CSPS and three of its subdimensions—Perceived Benefit, Perceived Barriers, and Cues for Action—were found to be significantly higher among women who underwent screening. However, in the multiple logistic regression analysis, the significance of the CSPS total score included in the model disappeared. This finding aligns with the literature emphasizing the impact of screening perception on participation, yet it also demonstrates that in multivariate analyses, this effect may be diminished by other contextual and individual factors.
Overall, the literature reports that screening perception strongly affects participation. For example, women with high cancer risk awareness are more likely to undergo screening (Dessalegn Mekonnen, 2020). In various contexts, perceived benefits and low barriers increase participation (Aguilar-Pérez et al., 2003; Ahmed et al., 2024), while low awareness and low perceived risk reduce it (George, 2021; McFarland et al., 2016). This study highlights that while screening perception is often emphasized in the literature, its independent effect may be less pronounced in multivariate models due to complex interactions with contextual and individual factors. Future research should model screening perception together with other psychosocial factors.
Increase in health anxiety
In this study, it was found that as health anxiety increased among women, their likelihood of undergoing cervical cancer screening tests also increased. These findings align with previous studies showing that health anxiety influences screening behaviors. Individuals with high health anxiety tend to perceive cancer risk as higher. Meta-analyses have shown that perceived susceptibility to cervical cancer increases the use of screening tests (Ayenew et al., 2020; Puspitasari et al., 2022). A meta-analysis on women of reproductive age found that those who perceived cancer more seriously were 1.61 times more likely to undergo screening (Habibatullah et al., 2021), which supports our findings. The impact of health perception on screening behavior varies across contexts. Studies in Arab countries and Kazakhstan show that individuals who perceive themselves as healthy are less likely to undergo screening (Ahmed et al., 2024; Issa et al., 2021), while research in South India suggests that health anxiety may hinder screening (Dsouza et al., 2022). Systematic reviews indicate that anxiety related to expectations may increase screening rates, while anxiety about the screening procedure may reduce participation (Goodwin et al., 2023). Overall, health anxiety is considered a factor that can both encourage and hinder cervical cancer screening behaviors. Future studies should explore the contextual and individual differences in this relationship to better understand this dynamic.
Positive behaviors for protection against sexually transmitted diseases
This study found that as women engaged in more positive behaviors for STDs prevention, the likelihood of cervical cancer screening increased. It was found that women who scored high on both the Knowledge and Protection and Attitude subdimensions of the STD-SCS had higher rates of undergoing PS tests. This indicates that improved health awareness leads to higher participation in preventive healthcare services. Meta-analyses confirm that risky sexual behaviors (e.g., multiple sexual partners, early sexual initiation) increase cervical cancer risk, yet more research is needed to clarify whether these behaviors directly reduce screening participation (International Collaboration of Epidemiological Studies of Cervical Cancer, 2009). Limited evidence shows that women with risky sexual behaviors or living with HIV have lower screening rates in various settings, including Puerto Rico, Kenya, and other contexts (Frazier et al., 2016; González et al., 2015; Haile et al., 2018). These findings underline the importance of access to healthcare and positive attitudes toward screening. In a randomized controlled study conducted in Türkiye, it was reported that participants’ scores regarding the benefits of undergoing PS tests increased following an educational intervention (Gul Oztas and Isik, 2025). Strengthening access to healthcare and awareness programs is essential for early detection of cervical cancer and STI prevention. Behavioral precautions, such as regular condom use, provide effective protection (Shepherd et al., 2011). In conclusion, the findings of this study suggest that women’s positive behaviors for protection against STDs may increase participation in cervical cancer screening. However, given the limited studies directly addressing this relationship in the literature, more comprehensive research is needed. Encouraging participation in screening tests and increasing sexual health awareness should be a key public health policy goal for the prevention of cervical cancer. Future studies should also explore culturally tailored interventions and community-based educational programs to strengthen women’s knowledge, protective behaviors, and positive attitudes toward screening.
History of sexually transmitted diseases
This study found that women with a history of STDs were four times more likely to undergo cervical cancer screening compared to those without such a history. Similarly, a meta-analysis showed that Ethiopian women with an STI history were more likely to undergo cervical cancer screening (Ayenew et al., 2020). Other studies in Australia and Mexico reported similar trends (Aguilar-Pérez et al., 2003; Smith et al., 2011). However, research in Peru found that having a history of STDs was a barrier to cervical cancer screening (Olaza-Maguiña and De La Cruz-Ramirez, 2019). These differences highlight the influence of cultural and socioeconomic factors on attitudes toward screening. Our findings suggest that a history of STDs and associated protective behaviors may increase participation in cervical cancer screenings. Nevertheless, given the limited number of studies addressing this relationship, further research is needed. Promoting screening participation and increasing sexual health awareness should be a key public health goal for cervical cancer prevention.
Other factors
Increasing age
This study shows that women’s cervical cancer screening participation increases with age. However, findings contrast with some studies, such as one in Ethiopia where participation decreased with age (Yirsaw et al., 2024). Similarly, research in Spain found younger women had higher participation (Puig-Tintoré et al., 2008), while a study in Kazakhstan showed lower participation among younger women (Issa et al., 2021). These differences suggest that factors like healthcare access, cultural influences, and national policies affect screening participation. Future research should explore these age-related differences to improve screening program effectiveness.
Marital status: Married versus divorced
This study shows that married and divorced women have higher cervical cancer screening rates compared to single women, aligning with previous research. A meta-analysis in Arab countries found higher screening rates among married women (Ahmed et al., 2024). Similar findings are reported in Africa (Nwabichie et al., 2018) and Singapore (Huang and Tan, 2024). Married women’s higher participation may be linked to more healthcare interactions, better access to reproductive health services, and healthcare provider guidance. Single women may face lower perceived risk, lack of awareness, or barriers like stigma and access issues. Targeted interventions to address these barriers and improve access are needed to increase screening among single women.
Health-related behaviors (Light physical activity and diet)
This study found that light physical activity and certain diets (Balanced, Vegetarian/Vegan, High-Protein) significantly influence cervical cancer screening participation. Previous studies support this, showing that obesity and low physical activity are associated with screening non-participation (Castañeda et al., 2023), while those with unhealthy diets are less likely to participate in screening (Richard et al., 2015; Venturelli et al., 2019). Individuals with healthier diets may have higher health awareness, leading to greater engagement in preventive services. However, smoking and alcohol use were not directly linked to screening, suggesting that personal health perception and motivation may also play a role. Cultural and demographic differences may affect these behaviors, and further research is needed. Encouraging physical activity and healthy eating habits could increase screening participation, making lifestyle-supporting public health policies crucial for raising screening rates.
Presence of chronic illness
This study found that the presence of chronic illness is a factor that increases participation in cervical cancer screening. Individuals with chronic diseases may have a higher likelihood of participating in screening programs due to more frequent contact with healthcare services. Studies in the United Kingdom and Tanzania similarly show that women with chronic illnesses have higher screening participation rates (Chadwick et al., 2019; Okyere et al., 2024). This suggests that individuals who regularly engage with healthcare services may have increased awareness of screening opportunities and are more likely to be referred by physicians. However, the causality of this relationship remains unclear, and future research should explore these underlying mechanisms in more depth.
Region of residence
This study found that women in Türkiye’s Mediterranean region have higher cervical cancer screening rates compared to other regions. This could be due to better access to healthcare services, awareness levels, and sociocultural factors. Access to healthcare in the Mediterranean region may be better, as indicated by data from the Turkish Statistical Institute (TURKSTAT), which shows that healthcare infrastructure in the region is well-developed (Turkish Statistical Institute, 2024b). Higher education levels in coastal areas (Turkish Statistical Institute, 2024a), may also increase health literacy and encourage participation in screenings. However, awareness of cervical cancer screening may vary regionally. Future research should explore the regional differences in healthcare usage and awareness in greater detail to inform regional health policies.
Practical implications
The findings of this study provide valuable insights for the development of public health policies aimed at increasing cervical cancer screening participation among women aged 30–65 in Türkiye. First, improving HPV knowledge and raising awareness about cervical cancer risks should be considered fundamental strategies for increasing screening rates. In this regard, community-based educational programs and awareness campaigns should focus on addressing knowledge gaps within the target population.
The study also revealed that women with higher levels of health anxiety were more likely to participate in screening tests. Therefore, health communication strategies should be designed to raise cancer awareness while avoiding the creation of unnecessary fear and anxiety.
Additionally, since positive behaviors for the prevention of sexually transmitted diseases (STDs) may support screening behaviors, informative initiatives on safe sexual practices and preventive measures should be strengthened.
Demographic and lifestyle factors should also be taken into account. Special intervention programs should be planned for unmarried women, younger age groups, and regions outside the Mediterranean where screening rates are comparatively lower. Promoting light physical activity and healthy eating habits can increase general health awareness and reinforce preventive health behaviors. Moreover, integrating screening recommendations into routine healthcare for women with chronic illnesses may enhance participation through their more frequent contact with health services.
In conclusion, policymakers should develop targeted, community-based interventions that consider regional and cultural differences, facilitate access to screening services, and ensure that educational programs comprehensively address the psychosocial and behavioral determinants identified in this study. Future research should examine the interaction of these factors over time to contribute to the development of evidence-based and sustainable public health strategies.
Limitations and strengths
This study has several limitations. The cross-sectional design limits the ability to establish causal relationships, and changes in factors influencing screening participation over time could not be observed. Additionally, recall bias may have occurred because participants self-reported their screening history, which could affect data accuracy. The use of a survey may introduce social desirability bias, as it depends on participants’ self-reports. Although the sample is large, it is not fully representative of all regions and socio-economic groups in Türkiye, which may limit the generalizability of the findings. Broader investigation of psychosocial and environmental factors could have provided deeper insights. The online survey method may also limit accessibility, particularly for groups with limited digital access, and might exclude women with low digital literacy or without internet access. Additionally, perceived socioeconomic status was self-reported and participants may have tended to classify themselves as middle-income, which, combined with potentially lower participation from economically disadvantaged groups, could have affected the representation and results related to this variable. Furthermore, other potential determinants, such as healthcare provider attitudes and system-level barriers, were not explored in depth and should be addressed in future studies.
Despite these limitations, the study’s large sample size and geographical diversity across Türkiye enhance its external validity. The research includes both demographic and psychosocial factors, providing a multidisciplinary perspective. Reliable scales (HPV-KS, CSPS, HAI, STD-SCS) were used, ensuring high data quality. The study’s extensive data analysis, using both univariate and multivariate methods, identified key factors influencing cervical cancer screening participation and their interrelationships. The detailed assessment of health behaviors and psychological conditions offers valuable insights for future health policies. In addition, the study fills an important gap by addressing multiple psychosocial and behavioral variables simultaneously, which contributes to a more comprehensive understanding of screening behaviors. The development of recommendations to increase screening participation strengthens the study’s practical applicability, creating a solid foundation for further research.
Conclusion
In this study, the participation rate for cervical cancer screening among women aged 30–65 in Türkiye was determined to be 56.2%. According to multiple logistic regression analysis, the factors that increase participation in cervical cancer screening are as follows: increased health anxiety, a history of STDs, the presence of chronic diseases, higher levels of HPV knowledge, positive behaviors for protection against STDs, increasing age, marital status (married or divorced), physical activity level, dietary habits, and residence in the Mediterranean region. Findings show multiple factors influence screening. Women with STDs or chronic illnesses tend to use health services more. Awareness programs should focus on those with high health anxiety and low sexual health knowledge, and access to services must improve. Future research should explore regional differences for targeted strategies.
Footnotes
Ethical Considerations
Ethics committee approval was obtained from the Sub-Commission of the Health Sciences Ethics Committee of Suleyman Demirel University.
Consent to Participate
All participants provided electronic informed consent before participating in the study. At the start of the online survey, they were presented with an information sheet and a consent form, and only those who agreed were allowed to access and complete the questionnaire.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
Banu Aslan: Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Supervision, Visualization, Writing – original draft and Writing – review and editing.
Özgür Önal: Formal analysis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during this study are available from the corresponding author upon reasonable request.
Manuscript submission statement
This manuscript has not been published elsewhere and is not concurrently under consideration for publication elsewhere.