
Abstract
This study examines reactions to the Covid-19 pandemic, focusing on routine and behavioral changes. It analyzes how vulnerability influenced behavior using microdata from 26 countries, targeting respondents over 50 from the eighth wave of the Survey of Health, Ageing and Retirement in Europe (SHARE), interrupted in March 2020, and the SHARE Corona Survey conducted via telephone in June–July 2020 and a year later. SHARE data integrates with macro-data to incorporate country-level indicators alongside individual characteristics. Findings reveal that vulnerability significantly affected precautionary behaviors. Older respondents were more likely to adopt protective measures, adjusting for demographic factors. Employment status also influenced behaviors, with employed individuals showing increased vigilance. Vaccination reduced the tendency for high precautionary behavior. Moreover, health vulnerability heightened the likelihood of precautionary measures. These insights highlight the interplay between individual and contextual factors in shaping pandemic-related behaviors, emphasizing vulnerability and demographic variables’ roles in precautionary actions.
Introduction
The new coronavirus was first identified in China in December 2019 and rapidly spread across continents, officially reaching pandemic status in March 2020. Over time, the virus has mutated, giving rise to variants that are more transmissible and/or exhibit greater resistance to vaccines. By November 2023, global reports indicated over 770 million confirmed COVID-19 cases and more than 6.9 million deaths. Europe has been among the regions most severely affected, with over 220 million cases and more than 1.8 million fatalities (World Health Organization (WHO), 2020).
The new disease posed a major policy dilemma, which was felt keenly in all countries. It was a virulent and highly transmissible disease with, at least initially, no known efficacious treatment or possibility of vaccination. The magnitude of the societal threat was illustrated painfully in early experience in places such as Bergamo in Italy (Perico et al., 2021). The lesson learned early on was that the only containment strategy was social distancing to an extent previously unimagined. The imposition of social distancing essentially meant that the course of the disease relied on the reactions of individuals in their effort to protect themselves. In any case, this necessary strategy entailed considerable collateral costs, both on an individual and a societal basis.
This study examines individuals’ responses to the pandemic, focusing on how they adapted their routines and behaviors during this period. The primary goal is to analyze the impact of vulnerability on respondents’ behavior using microdata from European countries participating in the Survey of Health, Ageing, and Retirement in Europe (SHARE). By utilizing data from two time points—the first COVID-19 wave in 2020 and the second in 2021—we aim to identify behavioral changes among vulnerable individuals aged 50 and older during the pandemic. Moreover, the longitudinal dimension of the dataset allows us to capture the effect of vaccination on respondents’ decisions regarding precautionary behavior. We address the following questions: Did preexisting difficult economic situations and health frailty have an impact at the individual level on implementing self-protection? If so, did it have a cumulative effect? Additionally, which factors led to behavioral change between the first and the second wave of the pandemic?
During the COVID-19 pandemic, numerous countries adopted preventive measures, including “stay-at-home” policies, community restrictions, and physical distancing. These measures also involved canceling mass gatherings and closing schools, workplaces, and public spaces (Rapid Risk Assessment, 2020). The widespread impact of COVID-19 significantly disrupted access to healthcare services, leading to reduced activities among healthcare professionals and the rescheduling or cancelation of planned medical treatments. According to a WHO survey, health service disruptions were widespread: 53% of countries experienced partial or complete disruption in hypertension treatment, 49% in diabetes care, 42% in cancer treatment, and 31% in cardiovascular emergency services. Rehabilitation services, critical for recovery after severe COVID-19 cases, were disrupted in nearly two-thirds (63%) of surveyed countries (WHO, 2020). Furthermore, the OECD/European Union (2022) highlighted that continental and northern European countries managed to minimize disruptions across most healthcare services. In contrast, greater disruptions were observed in southern European countries as well as in central and eastern European nations.
The treatment of non-COVID-19 diseases often fell victim to the intense focus on tackling the pandemic, while the decline in the availability of public transport posed a challenge for many to get to their planned appointments. A study by Moynihan et al. (2021) found a median reduction of 37% of health services overall, which was highest for doctor visits (42%) and slightly lower for admissions (28%), diagnostics (31%) and therapeutics (30%). In the same vein, Palmer et al. (2020) explain that the pandemic drove healthcare units to postpone and scale down because of a pre-existing shortage of skilled healthcare workers. This combination could affect the welfare state generally and vulnerable groups in particular. Such were the older adults and infirm or individuals with multiple or more severe conditions that required regular monitoring and adjustment of complex medication regimes. In the words of European Centre for Disease Prevention and Control (ECDC, 2020) “people who are medically vulnerable to COVID-19 and people who are socially vulnerable are much more vulnerable than the rest of the population. (. . .) These overlapping vulnerabilities highlight the importance of ensuring coherent policy responses that recognise both the particular challenges faced by each vulnerable population, and that also include more comprehensive approaches that respond to shared needs and challenges.”
During the initial stage of the pandemic, before vaccines became available, the aforementioned non-pharmaceutical interventions effectively curbed the virus’s spread in certain countries, though their impact was less pronounced in others. Despite the crucial role of precautionary measures, numerous anti-mask protests took place globally, particularly in the US, Canada, Europe, and Australia, occasionally escalating into violent incidents. Variability in individuals’ adoption of preventive behaviors may have been influenced by psychological traits and cognitive processes, lifestyle adjustments (Gallè et al., 2021), and personal perceptions regarding their capability to practice preventive measures (Rogers, 1975). An earlier study by Rosenstock (1974) proposed that engaging in protective behavior is shaped by perceived severity and vulnerability, perceived benefits, and susceptibility. This conceptual model, known as the Health Belief Model (HBM), suggests that stronger perceptions of the severity of negative health outcomes motivate individuals to take actions to avoid such outcomes. Zewdie et al. (2022) identified self-efficacy as a key predictor of COVID-19-related behaviors, ranking it as the second most commonly associated HBM construct with pandemic-related actions. Similarly, Shahnazi et al. (2020) found that individuals with high self-efficacy were more likely to adopt preventive measures against COVID-19.
The pandemic also highlighted and exacerbated existing economic and social inequalities, particularly in health and wealth domains (Alsan et al., 2021; Aspachs et al., 2021). From a health perspective, individuals in poor health prior to the pandemic faced medical appointment cancelations at more than twice the rate of those in good health, deepening the disparity between those requiring urgent care and those in better condition. People with pre-existing health issues also reported reduced physical contact during the pandemic, suggesting that lockdown measures and physical isolation may have worsened mental health challenges (Eurofound, 2023). Regarding wealth, the pandemic resulted in income reductions, increased poverty, and shifts in personal expenditure patterns (Arnault et al., 2022). Using the “COVID-19 economic vulnerability index,” the European Investment Bank (EIB) identified a positive correlation between income levels and vulnerability, revealing that 50% of low-income countries and approximately 25% of middle-income countries faced the highest risks associated with COVID-19 (Davradakis et al., 2020).
The theoretical background for research on responding to pandemics is primarily based on theories of risk perception, such as the Health Belief Model (HBM). The HBM is one of the models most extensively used in health behavior research (Skinner et al., 2015). According to the HBM, individuals’ behavior is shaped by their perceptions of four aspects: (1) perceived susceptibility to a health threat (i.e. the perceived probability of contracting the disease/infection); (2) the severity of the mentioned threat; (3) the likelihood of reducing the threat by implementing health-related behaviors; and (4) perceived barriers associated with recommendations regarding preventive actions. Several studies used this theoretical framework to predict agents’ responses regarding health threats. For example, Fall et al. (2018) predict vaccination intentions for seasonal influenza, while Jose et al. (2021) examined individuals’ perceptions and behavioral responses related to COVID-19 and its control measures. Similarly, Bressington et al. (2020) reported that perceived severity and susceptibility were significant predictors of a Hong Kong population’s compliance with mask-wearing and social distancing.
Additionally, theories that explore the factors influencing behaviors, particularly in how fear can affect thoughts and health behaviors, have been extensively applied as a model to anticipate protective actions. Among them, Protection Motivation Theory (PMT; Prentice-Dunn and Rogers, 1986), has been used as a theoretical framework. At the heart of the theory is the belief that a significant threat appraisal paired with a strong coping appraisal leads to proactive engagement in protective behavior (Balla and Hagger, 2025). Recent studies have highlighted self-efficacy and response efficacy as key drivers of compliance with protective measures during the COVID-19 pandemic. For example, Fullerton et al. (2022) conclude that the adoption of protective behavior depends on individuals’ beliefs regarding their ability to perform it. Also, emotional factors, government reliability and cultural norms can drive effects (Liu and Jiang, 2023). PMT was also used to examine vaccination uptake among adolescents in Los Angeles, revealing that self-efficacy was a significant predictor of vaccination status (Unger et al., 2023), while Elazab et al. (2024) examined how the COVID-19 diagnoses of close contacts influence individuals’ adherence to protective measures behavior.
This work contributes to the existing literature about behavioral responses to a pandemic by focusing on older people, a group consistently shown to be at higher risk for severe outcomes from COVID-19 and other infectious diseases (Sand and Bristle, 2024b). Older adults’ attitudes and behaviors regarding precautionary measures and vaccinations are of particularly importance owing to their relative vulnerability to COVID-19 and other vaccine-preventable diseases. Although previous research has explored overall predictors of precautionary behavior through frameworks such as Protection Motivation Theory (Hinssen and Dohle, 2023; Li et al., 2023), there has been less focus on how factors like vulnerability, perceptions of age-related risk, and vaccination status affect behavior over time among older individuals. Nevertheless, much of this research has focused on cross-sectional data or general populations, with little emphasis on the dynamic aspects of behavior in older cohorts and how vaccination status can influence risk perceptions and protective measures (Domínguez et al., 2023). Given the panel nature of SHARE data, combined with the large sample size we can isolate the time variation of precautionary behavior. Finally, through an analysis of regional differences across Europe we can estimate the effect of implemented policies and speculate about the importance of cultural and social aspects. Moreover, the panel nature of the data allows us to compare the individuals’ preventive behaviors before and after they got vaccinated. From a behavioral perspective, this process could indicate the impact that a solution such as vaccination may have on the rapid abandonment of precautionary behaviors.
Data and methods
Selection process
This research examines panel data from the Survey of Health, Ageing, and Retirement in Europe (SHARE), a comprehensive database initiated in 2004 to explore the economic, health, and social pathways of Europeans aged 50 and above. The survey offers in-depth insights into respondents’ demographics, household expenditures, health conditions, cognitive functions, income, and access to healthcare (Börsch-Supan et al., 2013). The SHARE study is ethically approved by the Ethics Council. The 2020 SHARE Wave 8 was approximately two-thirds complete in March 2020 when it was interrupted due to the enforcement of social distancing measures during the pandemic. To compensate, a special telephone-based pandemic survey (SHARE COVID-19) was introduced. This ad hoc survey focused on the pandemic’s impact and was conducted twice: first in June–July 2020, during the initial wave of the pandemic (Wave 1), and again a year later (Wave 2), following the second wave and several months after the first vaccines became available.
Our analysis focused on individuals aged 50 and above who participated in both waves of the SHARE COVID-19 survey. To obtain comprehensive individual-level characteristics, including pre-pandemic behaviors and health status, we integrated data from the SHARE Corona Survey with SHARE Waves 8 and 7. The final sample included 33,248 individuals with complete data, covering 26 countries: Scandinavian countries (Sweden, Denmark, Finland), Western countries (Germany, Netherlands, Switzerland, Belgium, Luxembourg, France), Southern countries (Spain, Italy, Greece, Portugal, Cyprus, Malta), Central and Eastern European countries (Poland, Estonia, Lithuania, Slovenia, Czech Republic, Hungary, Latvia, Romania, Slovakia, Bulgaria, Croatia), and Israel. To clarify the structure of our research design, a conceptual framework summarizing the key components of the analysis is provided (Figure 3, Appendix 1). It illustrates the flow from data sources through the creation of vulnerability and behavior indicators, the inclusion of individual and contextual covariates, and the modeling strategy used to examine changes in precautionary behavior.
Measuring vulnerability
Participants in SHARE answer a list of household related questions; among them the ability to make ends meet. The question states: “Thinking of your household’s total monthly income, would you say that your household is able to make ends meet. . .?” The answer scale was composed of four categories ranging from “with great difficulty” to “easily.” According to Litwin and Sapir (2009) this question is a sufficiently robust indicator of perceived income able to provide useful information in both survey questionnaires and intake inventories. Moreover, it can provide information about the subject’s living conditions allowing for comparison between countries regardless of cultural norms (Fahey, 2007).
To capture pre-pandemic health vulnerability, the self-perceived health question posed in wave 8 or 7 was used. It is an indicator of “subjective health” that integrates various aspects of respondents’ well-being, including physical functioning in daily life, lifestyle factors, specific disease characteristics (such as severity and prognosis), and cultural background (Jylhä, 2009; Verropoulou, 2012). Despite the subjective nature of this question, indicators of perceived health have proved an important predictor in explaining mortality and future health (Palladino et al., 2016; Wels, 2020). Self-perceived health is significantly associated with lifestyle habits, such as exercise, smoking, and rest adding more capturing a broader range of individuals actual health condition (Maniscalco et al., 2020). Additionally, we account for major developments following the first covid wave, making use of the following question “Did your health
Vulnerability index.
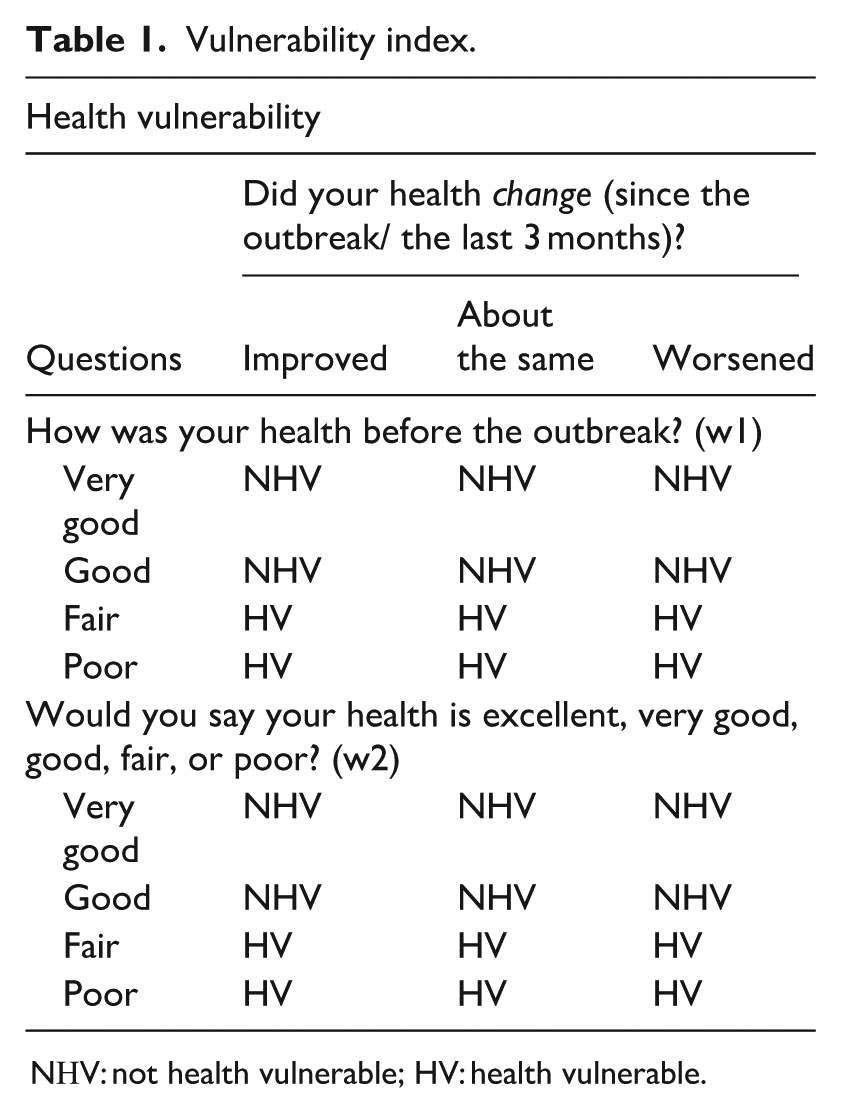
NΗV: not health vulnerable; HV: health vulnerable.
Measuring precautionary behavior
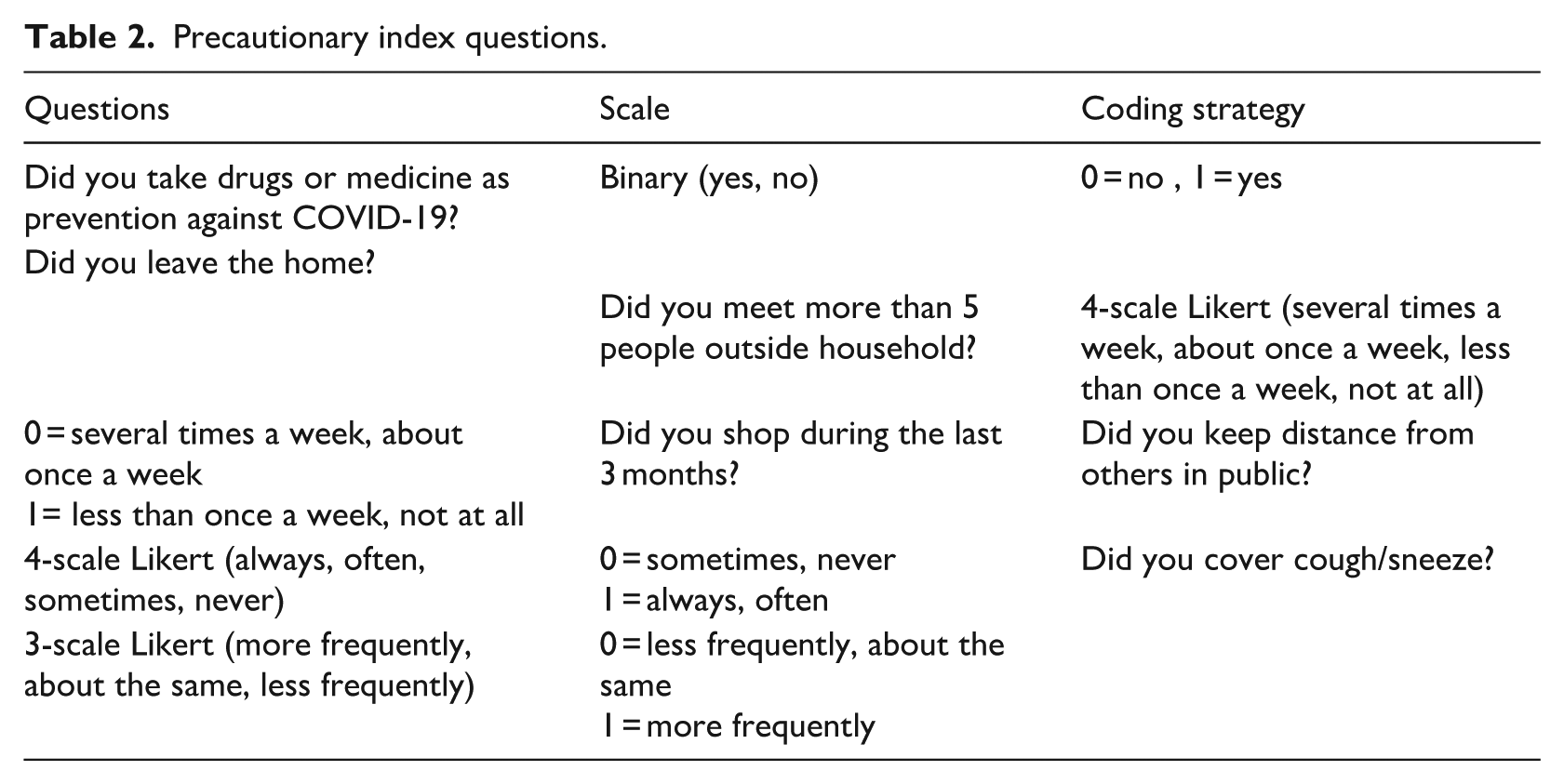
The SHARE Covid questionnaires (CATI1 and CATI2) include six common questions related to protective measures (cover cough and sneeze, took drugs against COVID-19) and maintaining social distance (left home, keep distance in public, meet more than 5 people). Respondent’s answers were coded using the following strategy. Questions with a binary scale coded as yes (1) and no (0). For variables with ordered-response categories the answers “always,” “often” was coded as yes (1) while the options “sometimes” and “never” were coded as no (0). Additionally, participants were asked three more questions regarding their daily activities outside the household, with responses recoded as 0 or 1, following the same approach as before (Table 2). The total score ranged from 0 (no self-protective measures) to 6 (fully self-protective). The proposed scale demonstrated strong reliability for both the first (Cronbach’s alpha (α) = 0.81) and the second questionnaire (Cronbach’s alpha (α) = 0.89).
Precautionary index questions.
Vigilance is defined according to local prevalence, rather than in absolute terms. A respondent was classified as “highly vigilant” if the total score of the above-mentioned behaviors is equal or greater to the mean value of the precautionary behaviors of his country. Otherwise, he/she was classified as “low precautionary.” The reason behind the use of the mean value for each country as a reference can be found in the theory of herding behavior: impulsive mental activity in individuals responding to signals from the behavior of others. Thus, individuals tend to adopt a given behavior based on the behavior of other people, whose observed behaviors and they mimic. In the case of the covid pandemic, telling people that “the majority of the people in your neighbouring city or province are following the social distancing/stay-at-home policy” may increase adherence to social distancing policy (Soofi et al., 2020).
Micro and macro level covariates
The adoption of precautionary measures is affected in complex ways by individuals’ micro-characteristics as well as by country, macro-level contexts. To consider the socioeconomic position of the respondents, two indicators were used in the analysis: education level and economic vulnerability. Education level was measured according to the highest obtained degree using the International Standard Classification of Education (ISCED-1997). Economic vulnerability was measured using households’ ability to make ends meet as described in the previous section. Furthermore, we control for an indicator for closeness and exposure to COVID-19, asking whether a respondent is exposed or knows someone in their social network with symptoms, tested positive, hospitalized, has died. Following Sand and Bristle (2024a), we categorize the first two indicators as “mildly exposed” and the last two as “severely exposed.”
Additionally, respondents’ intentions to vaccinate were used to classify them as vaccinated or not vaccinated. Vaccination may influence the adoption of precautionary behaviors, prompting individuals to reassess their actions. Research on other vaccination programs suggests that receiving a vaccine can lead to a potential increase in risk-taking behavior (Brewer et al., 2007; Denford et al., 2021). On the other hand, empirical evidence suggests that the spread of vaccination does not threaten the effectiveness of the behavioral recommendations (Desrichard et al., 2022). A cross-sectional analysis about changes in behavior following COVID-19 vaccination shows an increased compliance in precautionary measures such as handwashing, face mask wearing and social distancing (Littleboy, 2021). This process allows us to capture the effect of economic and health vulnerability while we control for education and income measures.
Additionally, based on guidelines from ECDC (2020), a health risk factor index was calculated for each individual including the following diseases: hypertension, chronic lung disease, cardiovascular disease, diabetes, and obesity. If a respondent has at least one of the five underlying medical conditions is classified as risky, otherwise as non-risky.
At the community level, we examined the influence of country-specific measures on respondents’ behavior by utilizing cumulative health indexes from the onset of COVID-19 until May 31, 2020. This date was selected as the cut-off point because the field survey commenced in June 2020, with a second wave of data collected 1 year later. To measure government responses, we used the Containment and Health Index (CHI), a stringency index provided by the Oxford COVID-19 Government Response Tracker (OxCGRT) project. The CHI comprises nine indicators of containment and health responses, calculated as the average score of these metrics, each ranging from 0 to 100, where higher values indicate stricter measures (Hale et al., 2020). Additionally, we employed the Universal Health Coverage (UHC) index to assess access to essential health services, including care for infectious and non-communicable diseases, as well as service capacity. The UHC index ranges from 0 (lowest) to 100 (highest). To evaluate the severity of the pandemic’s impact, we incorporated data on morbidity (number of cases per 100,000 population) and mortality (number of deaths per 100,000 population).
The models
The analysis started with a descriptive examination of the study variables. In the next step we performed logistic regressions on the dependent variable—change in precautionary behavior—to examine the probability of implementing a less protective behavior. Given the binary nature of the primary dependent variable logistic regression is suitable, as it estimates the probability of categorical events. This method effectively analyzes differences in protective behaviors over time and allows for the estimation of marginal effects associated with individual-level predictors. The probability is derived from the following equation:
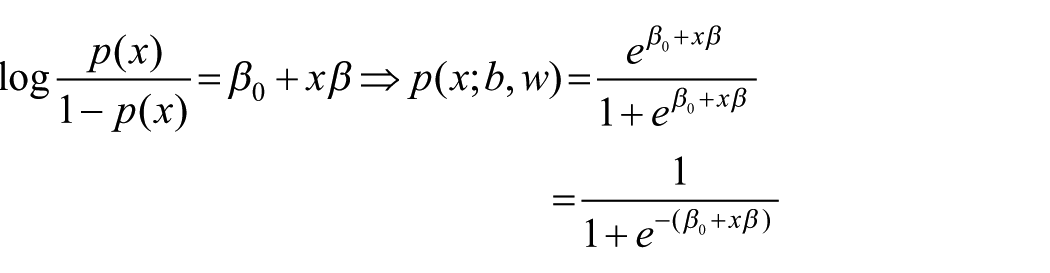
The equation models the probability
Three models were evaluated. In the first model, self-protective behavior was analyzed in relation to demographic variables, employment status, and network-exposure severity. The second model expanded on this by incorporating economic and health vulnerability. The last model includes the macro-level characteristics related to the pandemic, aiming to capture the effect of the implemented policies. Thus, starting from a micro level where only individual-level characteristics are included, we gradually add more information regarding the effect of social networks as a channel of influence, reflecting the interpersonal environment in which people are embedded and interact. The inclusion of policy responses to the pandemic aims to evaluate country differences based on national conditions. At the same time, individuals’ response to the pandemic reflects the propensity for irrational beliefs and the process of evaluating information. For example, we may assume that people scoring low on the perceived severity from its network may follow a less protective behavior in the law of small numbers—incorrect belief that small samples are likely to be highly representative of the populations. The availability of vaccinations was also added as a cofactor to explain respondents’ protective behavior.
Then, using the panel nature of the data, we use a fixed effect regression model to estimate the number of precautionary measures individuals implemented during the covid pandemic. The estimated function of the used model is the following:

where
Results
A sample of 33,248 individuals (42.1% male) with a median age of 73 years was included in the analysis. Country-specific weights were used at country level to make the analysis sample representative of the population aged 50 years and over. The following graph presents the distribution of the precautionary index in two time periods, 2020 and 2021. The scale range varies from 0 (absence of self-protective measures) to 6 (fully self-protective), though the largest share of participants took 4 precautionary measures (53%) during the first wave and 3 precautionary measures (45%) during the second wave. While in the first period respondents were more conservative—almost 40% followed up to 3 measures—a year after the percent doubled (75.9%). Only 5% and 3.8% chose to strictly follow the rules scoring at least 5 out of 6 in the first and second year, respectively (Figure 1).
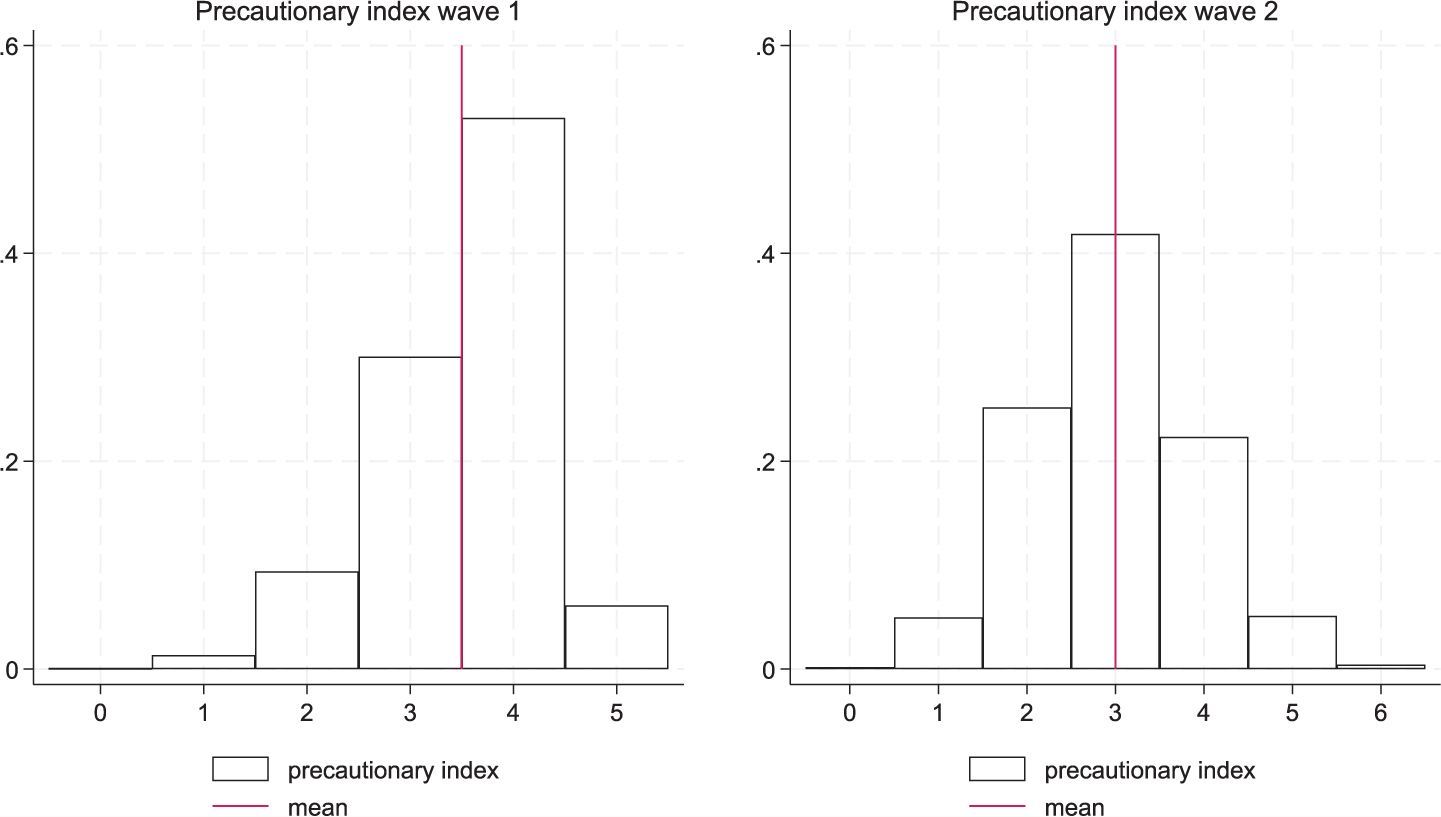
Precautionary Index distribution.
Variations on the extent of precautionary measures can be noted in different counties and between waves; Three quarters of the respondents from Western countries adopted most of the measures while Central and Eastern counties score was lower, about 65%. Remarkably, Netherlands and Malta recorded the greatest reduction in precautionary measures between the two waves (Figure 4, Appendix 1).
Descriptive statistics of variables for both waves I and II are exhibited in Table 3. It can be seen that 10,882 respondents (32.7%) followed a low precautionary behavior relative to the norm at the time during the first year of the pandemic while slightly fewer individuals followed the same behavior in the following year (29.5%). During the first year of the examined period, the proportion of respondents who reported they experienced health vulnerability is lower among those who followed a low precautionary behavior (32.6%) compared to those who took more self-protection measures (33.0%). This trend remains the same in both waves. Furthermore, the higher the risk factors the more precautionary measures tend to be followed. 75.2% of those implementing high precautionary measures were classified as “high risk.”
Sample description—percentages of subsample by type of precautions.
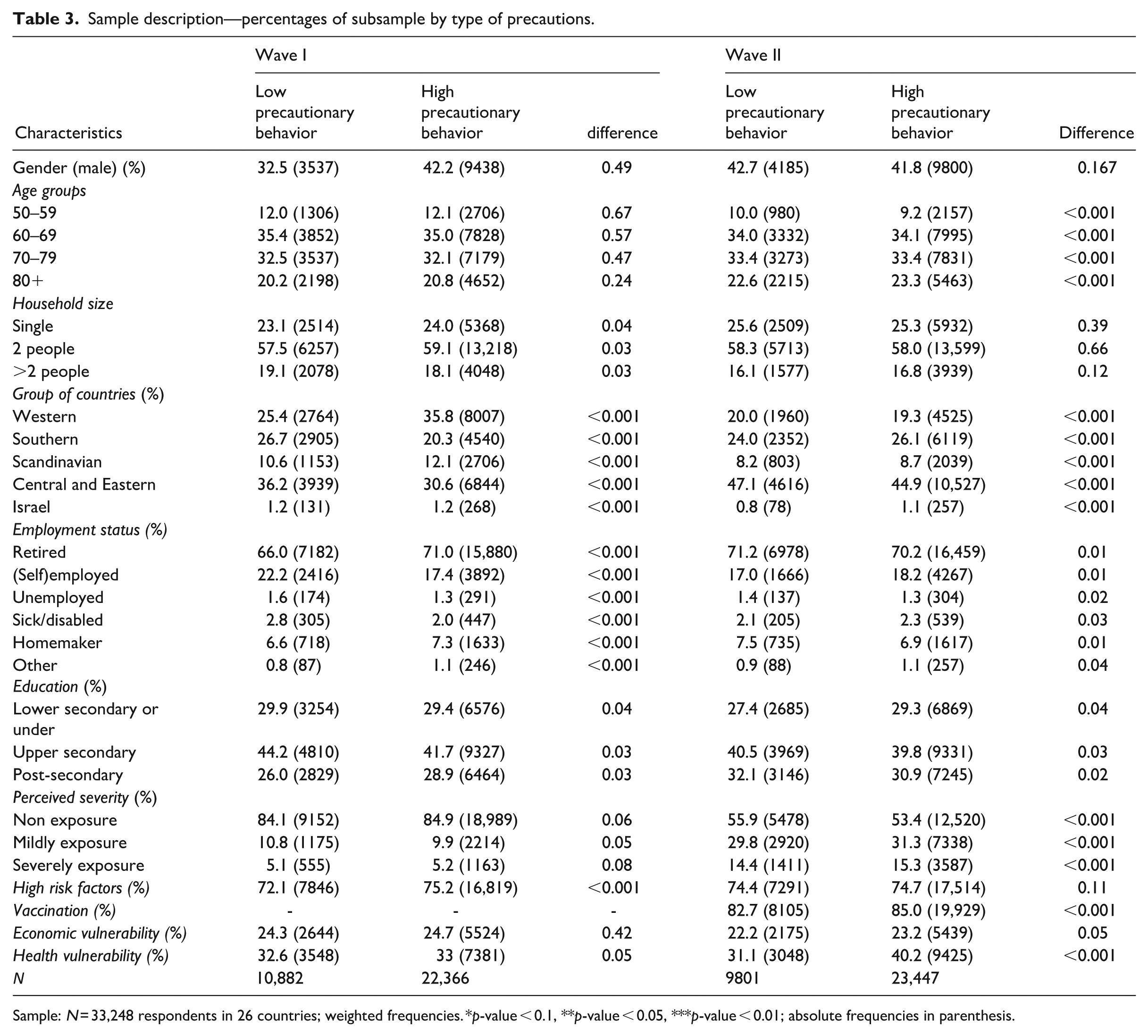
Sample: N = 33,248 respondents in 26 countries; weighted frequencies. *p-value < 0.1, **p-value < 0.05, ***p-value < 0.01; absolute frequencies in parenthesis.
Descriptive information on the macro-level variables is provided in Table 4. A clear pattern is drawn between groups of countries. The highest average stringency index is reported in Southern countries (60.1) and the lowest in Scandinavian countries (49.6) while the second year reported higher values of CHI index but with the same trend. The highest coverage of essential health services reported in Central & Eastern (83.4) and Western countries (83.3). A clear increase in the stringency index is noted between the two waves; Greece reported the highest value (83.6) followed by Italy (80.3) while Latvia (50.1) and Finland (53.7) the lowest (Appendix 1).
Sample description (macrolevel).
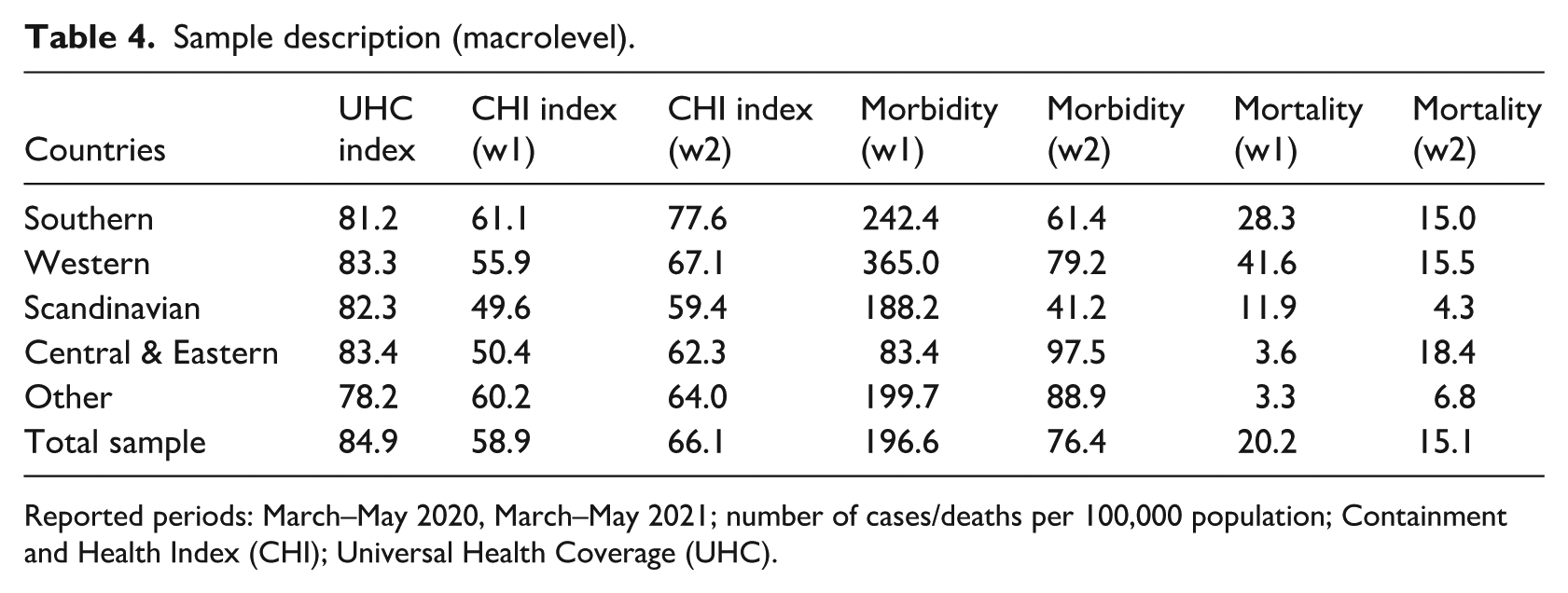
Reported periods: March–May 2020, March–May 2021; number of cases/deaths per 100,000 population; Containment and Health Index (CHI); Universal Health Coverage (UHC).
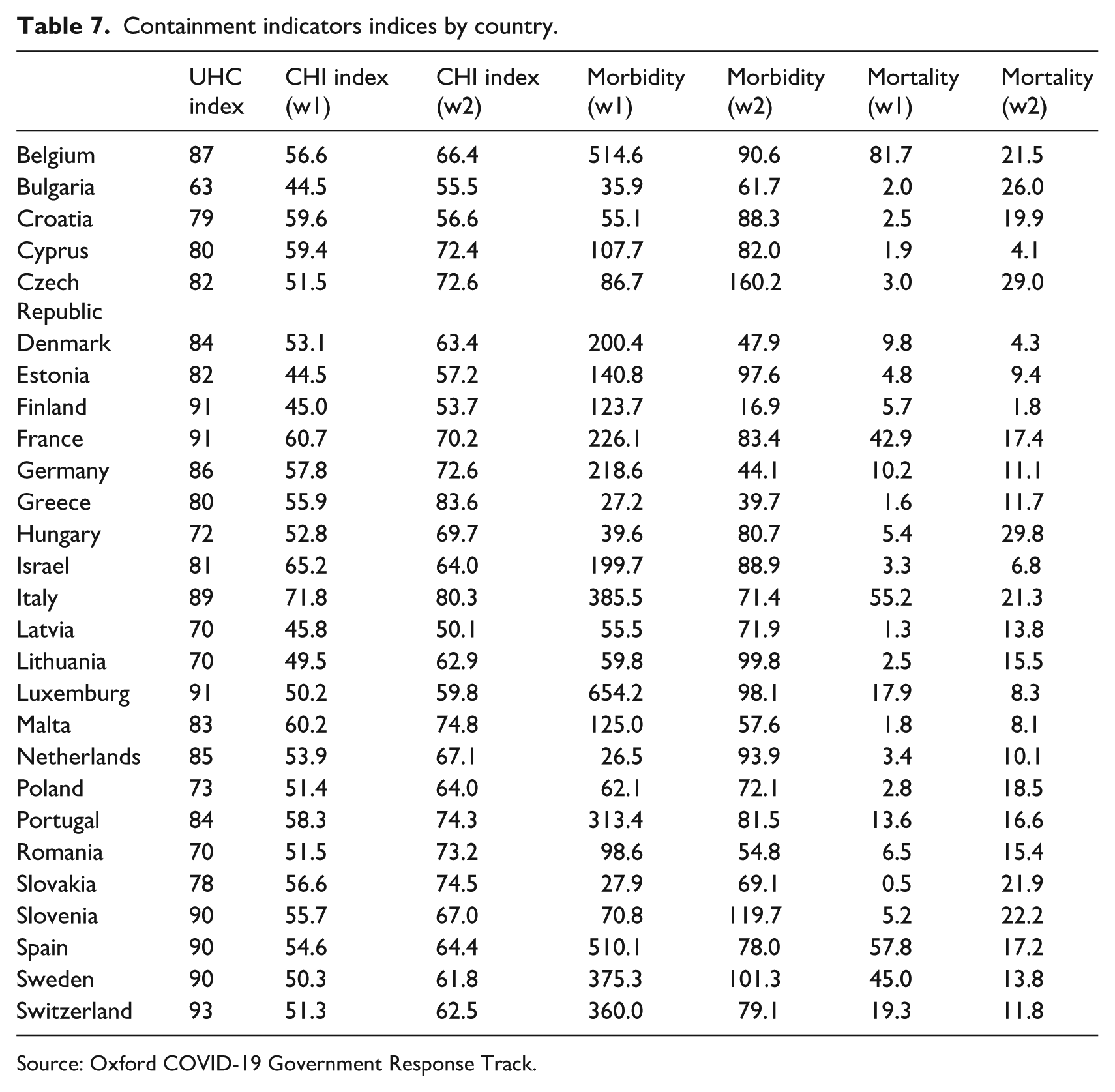
The variation of government responses against the number of COVID-19 cases can be seen in Figure 2. Notably, Bulgaria and Estonia reported the lower score (44.5), indicating a delay in implementing stringent measures. On the contrary, Italy has the highest value meaning an extended lockdown as a result of the devastating wave of infection hit the county. Table 7 on the Appendix 1 provides additional insights on a country level. Nonetheless, the stringency index—despite its completeness—fails to capture subnational variation for almost all countries, except for adding a flag denoting whether the restriction is national or subnational where this is meaningful (Conteduca, 2021).
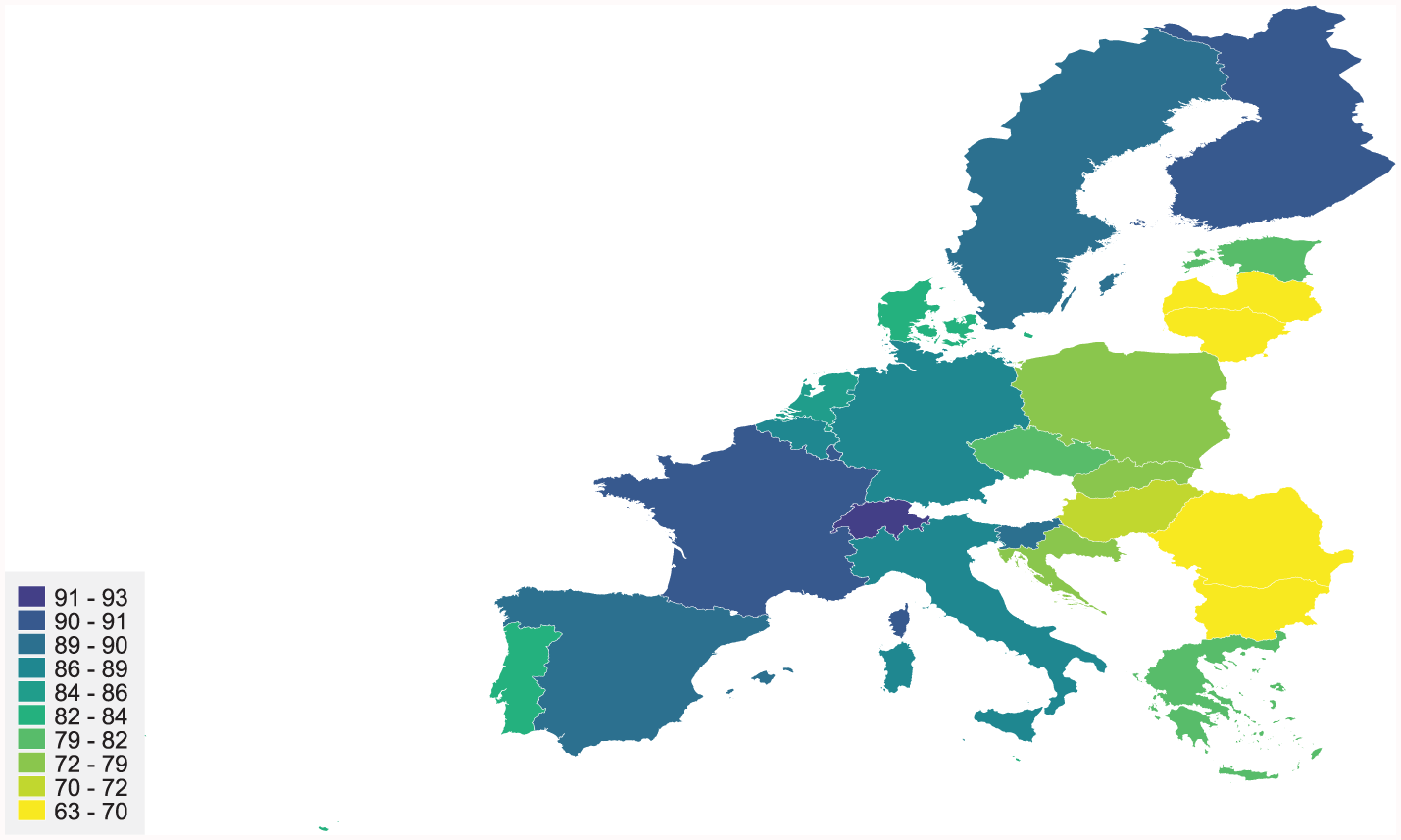
Universal Health Coverage Index.
The following table presents the main findings of the analysis. The odds ratios were estimated for all the factors associated with the dependent variable, precautionary behavior. In total, three different models were computed. The first model controls for the main demographic factors (such as gender, age, education, household size, and employment status) and individuals’ exposure to covid through its network. The second model adds information related to respondents’ vulnerability and vaccination while the third model accounts for macro variables related to health system and countries response against the pandemic. First, we found that employment status affects the implementation of higher protective behavior; self-employed and homemakers tend to implement less precautional behavior compared to pensioners. Examining the macro factors, the coverage of health system, coverage of essential health services and service capacity and access significantly affects individuals’ decision. Furthermore, mortality and morbidity have a positive impact. Southern countries and Central and Eastern countries are less likely to follow a high precautionary behavior.
During the second year of the pandemic where two major changes happened, the availability of vaccinations and the pandemic experience of the previous year. The effect of vaccination seems to be significant increasing 19% on average, the probability of following a less precautionary behavior. Also, the health and the economic vulnerability affects individuals’ behavior as well as the macro variables. We find that older respondents are less likely to follow less protective behavior against covid. More precisely, the odds of implementing strictly anti-covid measures were roughly 10% higher for responders over 80 years old compared to the reference group. Higher educated European tend to follow most of the protective measures, while employed respondents have greater chances of following a less precautionary behavior. Examining the effect of closeness and exposure to Covid-19 we found that the more exposed the individual is, the higher the probability of follow a high precautionary behavior. Interestingly, macro factors related to stringency index and health coverage have a persistent negative impact on the probability of following a less precautionary behavior.
The effect of implemented macro policies against the pandemic has a positive impact on the probability of following stricter anti-covid behavior; each additional measure of the stringency index increases the probabilities by 1 percentage points. Also, the coverage of essential health services is considered as an important factor affecting individuals’ choices. Our set of health-related variables exhibits the expected patterns, with vaccinated Europeans aged 50+ to be 19% more prone to relax their strictly precautionary behavior. The experienced vulnerability during the pandemic has a notable effect on individuals’ behavior; health vulnerable has 24% lower probability of following less of the protective measures. Also, the effect of economic vulnerability seems to follow the same pattern; non-economic vulnerable responders have higher probabilities of following a less protective behavior.
To further evaluate the validity and robustness of the results, we performed a series of diagnostic tests and tested alternative model specifications. Initially, we estimated three nested logistic regression models (Table 5), progressively adding predictors to assess the consistency of key associations. The odds ratios stayed stable, and the Akaike Information Criterion (AIC) decreased from Model I to III, suggesting an improved fit and reinforcing the robustness of our findings.
Effects on the probability of following a less precautionary behavior.
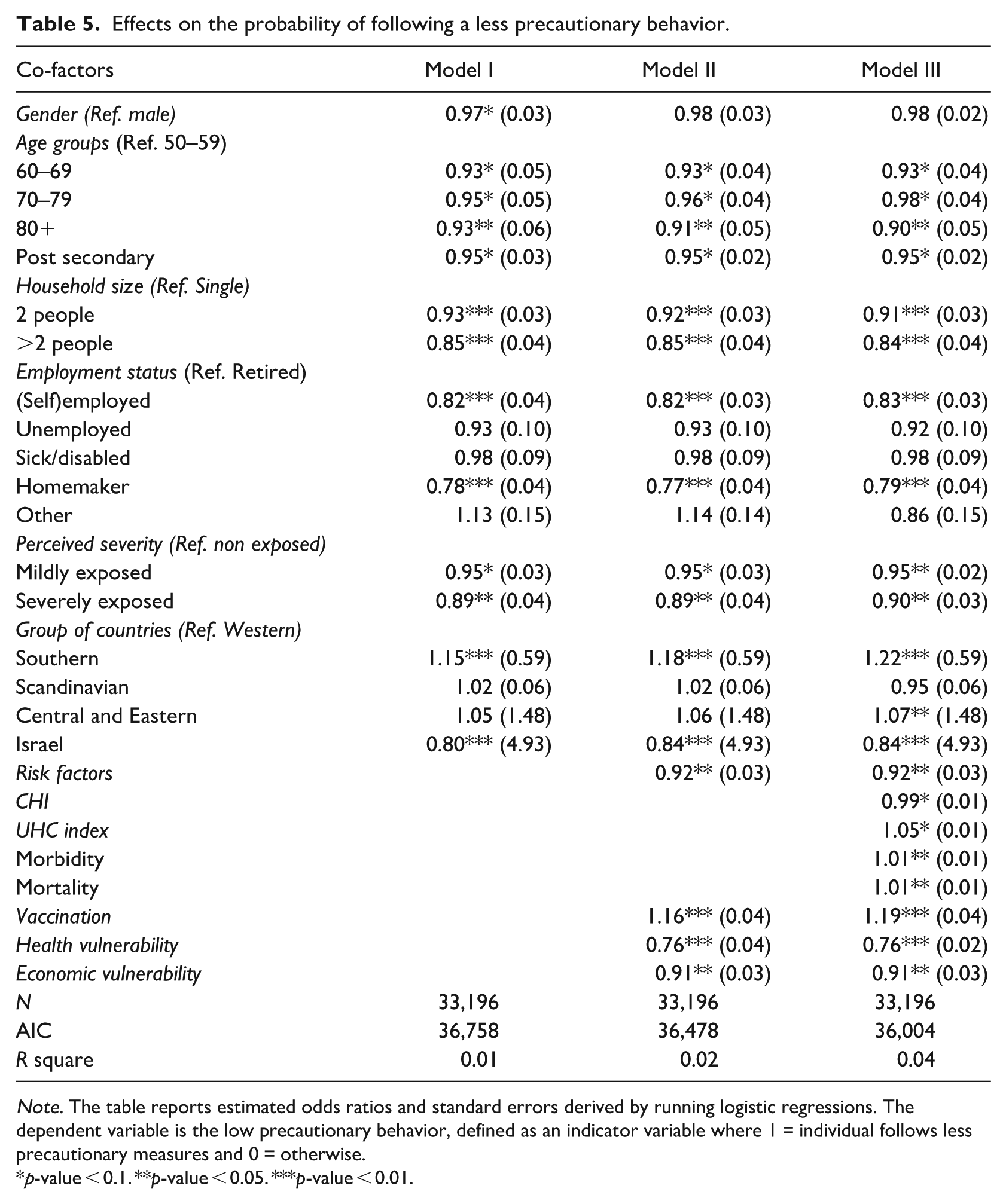
Note. The table reports estimated odds ratios and standard errors derived by running logistic regressions. The dependent variable is the low precautionary behavior, defined as an indicator variable where 1 = individual follows less precautionary measures and 0 = otherwise.
p-value < 0.1. **p-value < 0.05. ***p-value < 0.01.
Next, we applied a fixed effects (FE) panel regression model to leverage the longitudinal structure of the data and control for unobserved, time-invariant individual characteristics. This approach addresses potential endogeneity stemming from stable traits such as risk preferences or baseline health. A Hausman test ( p < 0.05) supported the use of the fixed effects model over the random effects alternative, indicating that unobserved individual heterogeneity is correlated with the regressors. Table 6 presents the estimation results of the FE model. In all models, the coefficients of the vulnerability dummies show a positive sign indicating an increase on the number of implemented protective measures. Furthermore, the effect is still significant adding more cofactors in the model.
Fixed effect model, dependent variables are preventive behavior.
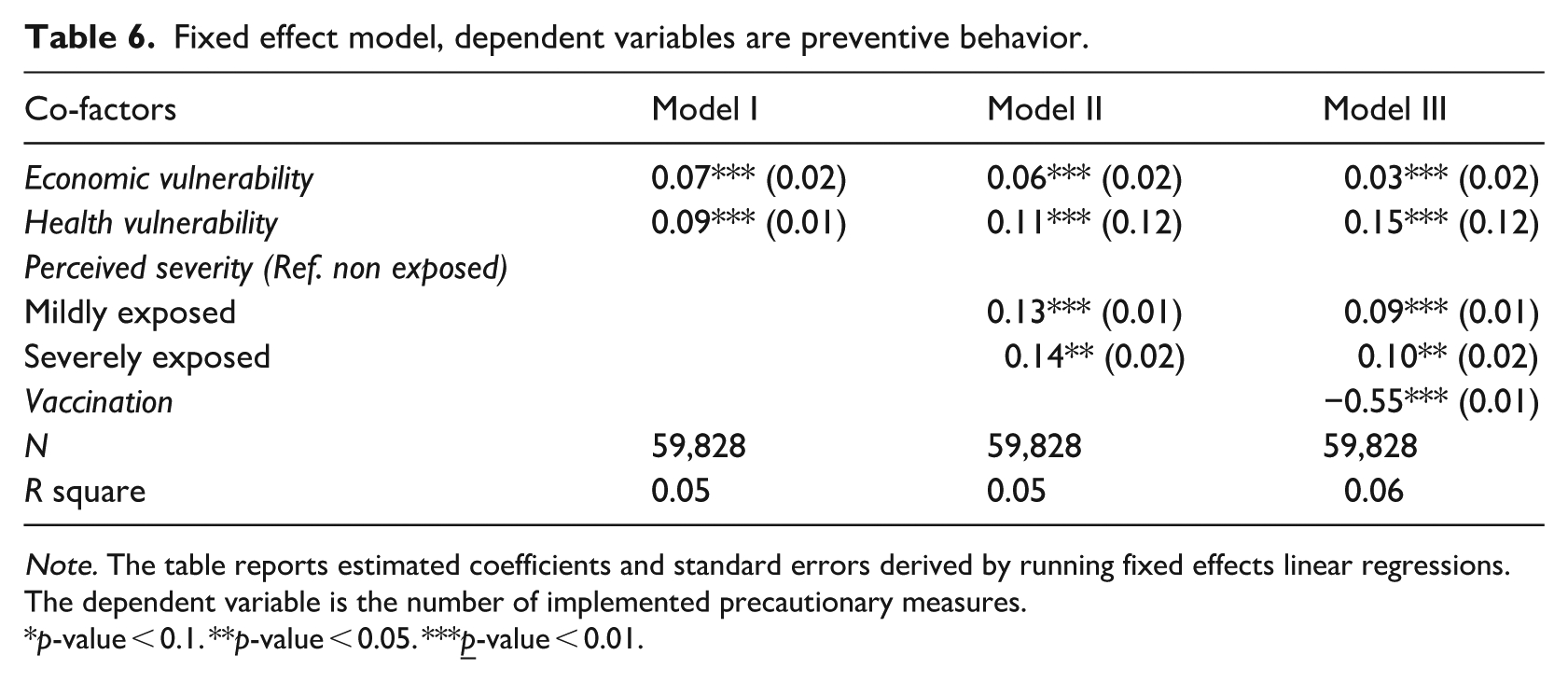
Note. The table reports estimated coefficients and standard errors derived by running fixed effects linear regressions. The dependent variable is the number of implemented precautionary measures.
p-value < 0.1. **p-value < 0.05. ***
The final model (Model III) showed that vulnerable individuals probably will follow a more protective behavior implementing more measures compared to those who are deemed non-vulnerable. Also, the effect of exposure seems to affect the number of implemented protective measures; the more exposure a respondent has experienced, the higher the number of protective measures taken. When covid vaccination is brought in the picture (Model III), results are suggesting a decrease in compliance in precautionary measures among vaccinated individuals. Interestingly, allowing for vaccination accentuates the impact of Health factors and diminishes those of economic factors.
Discussion
This paper aimed to examine how vulnerability influenced precautionary behaviors among older adults in Europe during the COVID-19 pandemic. We studied this effect using two computed measures, one for precautionary behavior as expressed during the pandemic and the other for vulnerability controlling for cross-national differences, features of a country’s health coverage and containment indicators of the pandemic. The analysis focused on individuals who participated in both surveys during the corona period—wave 1 (2020) and wave 2 (2021)—and supplemented these data with previous information from the pre covid period. Moreover, macro level covariates such as the Containment and Health Index and the Universal Health Coverage index were added in the dataset controlling for the effect of different implemented policies.
The main question of this study was the link between self-protective measures and vulnerability, utilizing both cross and panel data dimensions. Vulnerability had a greater impact on most of the countries as societies were not (fully) prepared. Almost half of the examined countries reported lower percent of vulnerable and severely vulnerable individuals. Focusing on the macro-determinants, the stringency index was associated with precautionary behavior. During crises such as pandemics, a decline in public revenue can lead to reduced funding for health services, intensifying the financial strain caused by a surge in patient numbers. Thus, a fragile healthcare system has lower capacities of providing the necessary services to patients, driving them to a more conservative and precautionary behavior.
The preceding analysis explored individuals’ behavior during the pandemic and how that changed between the first phase (2020) and the following year (2021), controlling for sociodemographic factors, intrapersonal characteristics, and macroeconomic variables. In those 2 years, participants were exposed to a new deadly virus for which little was known regarding its transmission or treatment. During the first pandemic year, countries implemented only preventive measures, alongside other community and physical distancing. The following year the introduction of vaccination and the progress of treatment protocols led individuals to change their behavior vis-a-vis taking protective measures. However, this transition was not uniform. In reference to this transition, our major findings are as follows:
Economic and health vulnerability are associated with the implementation of precautionary behavior. While the magnitude of economic and health vulnerability is different, both affect individuals’ attitude toward the precautionary measures.
The availability of vaccination in the context of relaxation of punitive measures decreased compliance in precautionary measures. An explanation could be that respondents may have misunderstood the communication campaigns regarding the benefits of vaccinations. Instead of highlighting that vaccination protects people by creating an immune response without the potentially severe illness, respondents may have perceived a lower risk of contracting the virus when they are vaccinated. This decrease in perceived threat mirrors mechanisms described in Protection Motivation Theory (PMT), where threat appraisal diminishes following perceived successful coping.
Perceived severity had a positive effect on protection, leading respondents to follow a more self-protective behavior. This aligns with the Health Belief Model (HBM), which indicates that people are more inclined to take protective measures if they believe the consequences of infection are serious. In the same spirit as Litwin and Levinsky (2021) we found that the extent of exposure to covid is positively associated with the intensity of one’s own engagement in self-protective behaviors.
A key implication of our findings is that behavioral models like HBM and PMT remain valuable but should be applied flexibly throughout the different stages of a health crisis. While perceived severity and vulnerability significantly influenced behavior early in the pandemic, later phases were affected by emotional fatigue, changing perceptions of measure efficacy, and trust in institutions. This pattern supports the recommendations of Gu et al. (2022) and Fullerton et al. (2022), emphasizing that standard models need to integrate temporal, emotional, and contextual factors.
Furthermore, our application of panel data enhances existing research by tracking behavioral changes over time, a feature often missing in cross-sectional studies (Bressington et al., 2020; Gallè et al., 2021). Focusing specifically on older adults, our study addresses a gap in understanding how persistent vulnerability and risk perception influence long-term adherence to protective measures. Our results also support studies like Balla and Hagger (2025), emphasizing the role of self-efficacy in sustaining precautionary actions, while contrasting with research showing more consistent behavioral responses across different age groups.
The result of the present study may be a helpful tool for public policy decision makers. On a practical level, these insights point to several policy considerations. First, communication strategies during vaccination campaigns must clearly distinguish between protection and immunity. Misinterpretations can lead to premature relaxation of preventive behaviors, undermining broader public health goals. Second, targeted outreach to economically and medically vulnerable populations is essential—not only to encourage protective behaviors but to ensure that individuals have the means (e.g. access to masks, information, and healthcare) to act on public health guidance. Third, our results show that strict national containment policies were effective in shaping individual behavior, suggesting that visible, consistent government action can reinforce personal responsibility during a crisis. Lastly, the variability across countries implies that cultural and systemic differences matter. Therefore, pandemic preparedness plans should not be one-size-fits-all but should adapt to regional health system capacities and population-specific vulnerabilities.
This study both reinforces and expands health behavior models by showing how perceived vulnerability, risk exposure, and contextual support interact over time to influence precautionary actions. Unlike many earlier studies, we emphasize that moving from high-threat situations to post-vaccine contexts can disturb the motivation patterns proposed by models such as the HBM and PMT. Our results indicate that successful health communication must be grounded in theory and adaptable to changing public perceptions, particularly among older groups with different vulnerability levels.
This study enhances our understanding of the psychological and structural influences that affect individual behaviors in a global health crisis. Future research and policy-making need to closely examine how changing risk perceptions and the resilience of health systems interact to either encourage or discourage adherence to precautionary measures.
Concluding thoughts
This study investigated the influence of vulnerability on precautionary behaviors among older adults in Europe during the COVID-19 pandemic, utilizing longitudinal data from the SHARE surveys and controlling for macro-level factors. Our analysis revealed several key outcomes. Firstly, economic and health vulnerability significantly and positively impacted the adoption of precautionary measures, highlighting the importance of individual circumstances in shaping protective behaviors during a health crisis. Secondly, the introduction of vaccination and a relaxation of stringent measures appeared to decrease adherence to precautionary behaviors, potentially due to misinterpretations of vaccination benefits. Finally, perceived severity of the virus positively correlated with the implementation of self-protective actions, aligning with findings on the influence of perceived risk on health behaviors.
These findings offer vital insights for policymakers aiming to optimize public health strategies during pandemics and large-scale crises. Recognizing that economic and health vulnerabilities drive precautionary behaviors highlights the need for tailored support for at-risk populations to enhance adherence to protective measures. Additionally, the drop in precautionary behavior after vaccines and relaxed restrictions underscores the need for clear public health communication. Policymakers should prioritize campaigns that convey vaccination benefits beyond individual protection, emphasizing its role in reducing transmission and safeguarding community health. Future interventions should address potential misinterpretations of evolving health guidelines and focus on sustained public engagement. Ultimately, grasping the interplay between vulnerability, interventions, and individual responses will help policymakers create more effective and equitable strategies for future health crises.
We are aware of the limitations of this paper. The SHARE covid—to the extent of our knowledge—was the first large scale scientific survey examining the effect of the pandemic on the ageing European population. The short time frame for designing and field working may be drove to selection bias. Also, demographic factors such as age as well as health and economic related question may affect the willingness to participate across countries. Nonetheless, no empirical evidence for systematic participation bias and attrition bias has come to our knowledge so far. Another limitation of our study is the usage of a non-standard index for vulnerability. The approach to this multidimensional concept was based solely on the economic and health impact to respondents. While aware of the mentioned limitations, we believe that our findings are useful in revealing how individuals took precautionary decisions, factoring their own circumstances against their perceived overall risk.
Footnotes
Appendix 1
Containment indicators indices by country.
| UHC index | CHI index (w1) | CHI index (w2) | Morbidity (w1) | Morbidity (w2) | Mortality (w1) | Mortality (w2) | |
|---|---|---|---|---|---|---|---|
| Belgium | 87 | 56.6 | 66.4 | 514.6 | 90.6 | 81.7 | 21.5 |
| Bulgaria | 63 | 44.5 | 55.5 | 35.9 | 61.7 | 2.0 | 26.0 |
| Croatia | 79 | 59.6 | 56.6 | 55.1 | 88.3 | 2.5 | 19.9 |
| Cyprus | 80 | 59.4 | 72.4 | 107.7 | 82.0 | 1.9 | 4.1 |
| Czech Republic | 82 | 51.5 | 72.6 | 86.7 | 160.2 | 3.0 | 29.0 |
| Denmark | 84 | 53.1 | 63.4 | 200.4 | 47.9 | 9.8 | 4.3 |
| Estonia | 82 | 44.5 | 57.2 | 140.8 | 97.6 | 4.8 | 9.4 |
| Finland | 91 | 45.0 | 53.7 | 123.7 | 16.9 | 5.7 | 1.8 |
| France | 91 | 60.7 | 70.2 | 226.1 | 83.4 | 42.9 | 17.4 |
| Germany | 86 | 57.8 | 72.6 | 218.6 | 44.1 | 10.2 | 11.1 |
| Greece | 80 | 55.9 | 83.6 | 27.2 | 39.7 | 1.6 | 11.7 |
| Hungary | 72 | 52.8 | 69.7 | 39.6 | 80.7 | 5.4 | 29.8 |
| Israel | 81 | 65.2 | 64.0 | 199.7 | 88.9 | 3.3 | 6.8 |
| Italy | 89 | 71.8 | 80.3 | 385.5 | 71.4 | 55.2 | 21.3 |
| Latvia | 70 | 45.8 | 50.1 | 55.5 | 71.9 | 1.3 | 13.8 |
| Lithuania | 70 | 49.5 | 62.9 | 59.8 | 99.8 | 2.5 | 15.5 |
| Luxemburg | 91 | 50.2 | 59.8 | 654.2 | 98.1 | 17.9 | 8.3 |
| Malta | 83 | 60.2 | 74.8 | 125.0 | 57.6 | 1.8 | 8.1 |
| Netherlands | 85 | 53.9 | 67.1 | 26.5 | 93.9 | 3.4 | 10.1 |
| Poland | 73 | 51.4 | 64.0 | 62.1 | 72.1 | 2.8 | 18.5 |
| Portugal | 84 | 58.3 | 74.3 | 313.4 | 81.5 | 13.6 | 16.6 |
| Romania | 70 | 51.5 | 73.2 | 98.6 | 54.8 | 6.5 | 15.4 |
| Slovakia | 78 | 56.6 | 74.5 | 27.9 | 69.1 | 0.5 | 21.9 |
| Slovenia | 90 | 55.7 | 67.0 | 70.8 | 119.7 | 5.2 | 22.2 |
| Spain | 90 | 54.6 | 64.4 | 510.1 | 78.0 | 57.8 | 17.2 |
| Sweden | 90 | 50.3 | 61.8 | 375.3 | 101.3 | 45.0 | 13.8 |
| Switzerland | 93 | 51.3 | 62.5 | 360.0 | 79.1 | 19.3 | 11.8 |
Source: Oxford COVID-19 Government Response Track.
Ethical considerations
The SHARE study is subject to continuous ethics review. During Waves 1 to 4, SHARE was reviewed and approved by the Ethics Committee of the University of Mannheim. Wave 4 and the continuation of the project were reviewed and approved by the Ethics Council of the Max Planck Society (06/2021). More information is available here: ![]()
Consent to participate
Participants granted their informed consent to participate in the survey after being given comprehensive details regarding the study’s purpose, procedures, data protection measures, and their right to withdraw at any time.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author Contributions
Michail Chouzouris contributed to conceptualization, methodology, formal analysis, data curation, visualization, and writing of the original draft. Platon Tinios contributed to conceptualization, methodology, and writing – review and editing. Both authors approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.