
Abstract
This research aimed to assess the spiritual well-being and quality of life (QOL) among patients with chronic kidney disease who are undergoing hemodialysis in Jordan. A cross-sectional, descriptive correlational study was employed. A convenience sample of 238 Jordanian adult patients with chronic kidney disease undergoing hemodialysis in governmental hospitals was selected. Findings revealed that the response rate was 93.7%. and the participants had moderate spiritual well-being and low QOL. A significant positive correlation was shown between QOL and spiritual well-being, educational level, marital status, and monthly income (p < 0.001), while a negative correlation was shown with age (p < 0.001). Spiritual well-being, educational level, and monthly income were predictors of QOL. Thus, patients with chronic kidney disease undergoing hemodialysis need to enhance their spiritual well-being and improve their QOL. Counseling programs should be provided to patients with chronic kidney disease undergoing hemodialysis to promote spiritual well-being and improve their QOL.
Introduction
Patients with chronic kidney disease (CKD) depend on renal replacement therapies, such as dialysis or kidney transplantation, for survival (Jardine et al., 2020; Webster et al., 2017). Globally, an estimated 5.3 to 10.5 million individuals require these treatments; however, many face barriers to access due to limited resources or financial constraints (Gonzalez-Bedat et al., 2020; Himmelfarb et al., 2020; International Society of Nephrology, 2020). Hemodialysis is the most commonly used dialysis modality (Lee et al., 2021; Murdeshwar and Anjum, 2023; Queeley and Campbell, 2018), typically performed multiple times per week (Adwan et al., 2023; McConnachie et al., 2021), and is utilized by approximately 89% of CKD patients worldwide (Bello et al., 2022).
During hemodialysis, patients often experience declines in their physical, mental, and social well-being. Chronic pain is common (Ishtawi et al., 2023; Masià-Plana et al., 2022), along with psychological challenges such as depression and anxiety, and social isolation due to the burdensome nature of ongoing treatment (Gadia et al., 2020; Gerogianni et al., 2019; Santini et al., 2020). Additionally, these patients frequently report reduced levels of quality of life (QOL) and spiritual well-being (Aini and Cahyaning Wahyu, 2020; Alshogran et al., 2021). The World Health Organization, Quality of Life Group (1996) defines QOL as an individual’s perception of their position in life in relation to their goals, expectations, and concerns, within the context of their culture and value system (Iqbal et al., 2020). QOL encompasses a comprehensive assessment of physical, psychological, social, and environmental well-being. For patients undergoing hemodialysis, QOL is often significantly diminished due to treatment demands, strict dietary restrictions, physical impairments, and emotional stress (Megari, 2013). Studies consistently show that the QOL of hemodialysis patients is substantially lower than that of the general population (Al Salmi et al., 2021; Legrand et al., 2020), as hemodialysis imposes considerable physical, emotional, and social limitations on nearly every aspect of daily life (Benjamin and Lappin, 2021). Factors influencing QOL in this population include disease stage, comorbidities, and the availability of psychosocial support.
Similarly, spirituality is defined as an individual’s sense of connection to the essence of life, encompassing a search for meaning through relationships with oneself, others, nature, and the sacred (Doumit et al., 2019). Alongside physical, mental, and social dimensions, spirituality is recognized as one of the four core components of human health. A person’s health can be significantly influenced by their spiritual or religious beliefs, practices, and experiences (Pilger et al., 2017). In Muslim societies, spirituality is deeply integrated into daily life and health-related beliefs. Spiritual well-being consists of two key aspects: existential well-being, which pertains to a sense of meaning, purpose, inner peace, and emotional strength, and religious well-being, which reflects one’s relationship with God (Rabitti et al., 2020). Research indicates that individuals with CKD undergoing hemodialysis often report moderate levels of spiritual well-being (Fradelos et al., 2021; Musa et al., 2018; Rayani et al., 2025; Saedi et al., 2024). Those with higher spiritual well-being tend to experience a better QOL and lower psychological distress (Senmar et al., 2020). Spirituality frequently serves as a vital coping mechanism, offering strength, peace, comfort, support, and satisfaction, all of which can significantly enhance QOL (Musa et al., 2023) and overall well-being (Moons et al., 2019). Furthermore, studies demonstrate that spirituality positively influences the physical, mental, and social health of individuals with chronic illnesses (Fanoodi et al., 2021; Lima et al., 2020; Najafi et al., 2022), underscoring that optimal QOL cannot be achieved without addressing this essential component (Jafaripoorr et al., 2019). Early research also shows that spiritual well-being is positively associated with improved QOL and better psychological outcomes among patients with chronic illnesses, including CKD (Al-Ghabeesh et al., 2018; Musa et al., 2023). Within Muslim populations, practices such as prayer, faith in divine will, and community support provide emotional strength and effective coping mechanisms.
Socio-demographic factors, including marital status, age, gender, educational level, income, and duration of hemodialysis, play a significant role in shaping QOL among patients with CKD undergoing hemodialysis (Alshelleh et al., 2023; Elsodany et al., 2022; Ishtawi et al., 2023; Naseef et al., 2023). Advancing age is often associated with reduced QOL, primarily due to physical and cognitive decline (Rehman et al., 2020). Women generally report lower QOL compared to men (Mohd Shahrin et al., 2019). In contrast, higher educational attainment tends to be linked with better QOL outcomes (Rikos et al., 2023), whereas lower income is correlated with poorer QOL (Abdulqader and Ali, 2023; Rikos et al., 2023). Marital status also influences QOL, with married individuals typically reporting higher QOL than those who are single or divorced (Abdulqader and Ali, 2023). Additionally, longer duration on hemodialysis has been correlated with poorer QOL (Alhajim, 2018; Alshogran et al., 2021).
While the positive impact of spiritual well-being on QOL is well established, there remains a lack of research exploring this relationship within specific cultural, religious, or regional contexts, particularly among Muslim patients. This study aimed to address this gap by providing context-sensitive, patient-centered insights. By examining the role of spirituality in this population, the findings may inform the development of more holistic and culturally appropriate care strategies that extend beyond medical treatment to support the whole person.
Situation in Jordan
In 2020, the total number of Jordanian patients diagnosed with CKD was 7290. Of these, 3318 (45.5%) received treatment in Ministry of Health hospitals, 2357 (32.3%) in private sector hospitals, 1424 (19.5%) in Royal Medical Services hospitals, and 191 (2.6%) in a university hospital (Ministry of Health, 2020). The majority of Jordanians are Muslims, and many draw on their faith, spiritual beliefs, and religious practices as vital sources of comfort and resilience during illness and adversity. Even amid significant suffering, spiritual and religious values can provide individuals with hope, a sense of purpose, and inner peace (Al-Ghabeesh et al., 2018; Musa et al., 2023).
Despite the recognized importance of spiritual well-being and QOL in chronic illness management, limited research has explored these factors among patients with CKD undergoing hemodialysis in Jordan. For instance, Alshraifeen et al. (2022) examined only QOL in this population and found that hemodialysis negatively impacted patients’ overall QOL, with the social domain being the most affected and the physical domain the least. Similarly, Musa et al. (2023) investigated the relationship between spiritual well-being and QOL but did not account for the influence of socio-demographic factors. Their study reported moderate levels of spiritual well-being and poor QOL among patients, with a significant positive correlation between the two variables.
However, no previous research in Jordan has examined the combined influence of QOL, spiritual well-being, and demographic characteristics among Muslim patients with CKD undergoing hemodialysis. Therefore, it is essential for healthcare professionals—particularly nurses and social workers—to provide comprehensive, holistic care that addresses not only the physical health of these patients but also their spiritual and psychosocial needs. Accordingly, this study aimed to assess QOL and its association with spiritual well-being among patients with CKD undergoing hemodialysis in Jordan. Specifically, the study was guided by the following research questions:
What are the levels of spiritual well-being and QOL among the participants?
What is the association between spiritual well-being, socio-demographic factors (e.g. age, gender, duration on hemodialysis, educational level, monthly income, and marital status), and QOL among the participants?
What are the predictors of QOL among the participants?
Framework of the study
This study is closely aligned with Puchalski’s Model of Spiritual Care (Puchalski et al., 2009), which emphasizes spiritual well-being as a core dimension of health that can significantly influence—or even predict—individuals’ perceptions of QOL. In Islamic culture, spirituality is expressed through practices such as prayer, trust in God’s will, and active engagement with the religious community. These elements are deeply embedded in the coping strategies, sense of hope, and search for meaning among patients living with chronic illnesses.
By applying Puchalski’s model, spirituality is conceptualized not as a secondary or supplementary factor, but as an essential, measurable, and clinically relevant component of patient care—particularly in the management of long-term conditions such as CKD. The model offers a meaningful framework for integrating spirituality into healthcare, especially in cultural contexts like Jordan, where religious and spiritual beliefs are closely tied to health perceptions and the healing process. Furthermore, the model underscores that spiritual care is not an isolated domain but is interwoven into all aspects of a patient’s well-being. This approach aligns with holistic nursing and medical practices that aim to treat the whole person—body, mind, and spirit.
This study examined spiritual well-being as the primary independent variable, hypothesizing its correlation with QOL and its potential role as a key predictor. Its inclusion allows for an exploration of how religious and cultural factors shape patient experiences within the Jordanian Muslim context, in alignment with Puchalski’s model of spiritual care. QOL, the dependent variable, serves as a critical measure for evaluating whether spiritual well-being functions as a protective or enhancing factor for patients managing the complex demands of hemodialysis in a socio-religious environment.
The inclusion of socio-demographic variables enables subgroup analysis and helps control for potential confounding factors that may influence the relationship between spiritual well-being and QOL. Additionally, clinical variables, such as duration on hemodialysis, provide important context for interpreting QOL outcomes and allow for the assessment of whether spiritual well-being exerts a buffering effect, regardless of clinical severity. Based on this framework, the following hypotheses were proposed:
1- There is a positive relationship between spiritual well-being and QOL among participants.
2- There is a relationship between socio-demographic characteristics and QOL among participants.
Methods
Design, setting, sampling, and sample
This study employed a cross-sectional, descriptive correlational design. Data were collected from hemodialysis units in Ministry of Health hospitals between April and July 2024. Four hospitals located in Jordan’s largest cities—Amman, Zarqa, Irbid, and Karak—were selected based on their size, patient volume, and accessibility to a broad and diverse population. These hospitals were chosen for their well-established hemodialysis units, advanced infrastructure, available resources, and multidisciplinary care teams, all of which contributed to the reliability and generalizability of the study findings.
A convenience sampling method was employed for participant recruitment. The required sample size was determined using G*Power software version 3.1.9.7, with a significance level (p-value) of 0.05, statistical power of 0.90, an effect size of 0.09, and seven predictors included in the regression model (Faul et al., 2009). Based on these parameters, the minimum required sample size was calculated to be 211 participants. To account for potential incomplete or missing data, an additional 20% was added, resulting in a target recruitment sample of 254 participants.
Inclusion criteria were as follows: Muslim patients aged 18–60 years, undergoing hemodialysis for at least 6 months, able to read, with no history of kidney transplantation, and willing to participate. Exclusion criteria included patients with documented mental or cognitive disorders in their medical records, as well as those with altered levels of consciousness.
Study instruments
A self-reported questionnaire was used, consisting of three sections: (1) socio-demographic data (age, gender, duration on hemodialysis, educational level, monthly income, and marital status); (2) the Spiritual Well-Being Scale (SWBS); and (3) the World Health Organization Quality of Life–BREF scale (WHOQOL-BREF).
The SWBS, developed by Paloutzian and Ellison (1982), was used to assess overall spiritual well-being. It consists of 20 items: 10 odd-numbered items measuring Religious Well-Being and 10 even-numbered items measuring Existential Well-Being. Responses are rated on a 6-point Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree). Total scores range from 20 to 120, with higher scores indicating greater spiritual well-being. Nine negatively worded items are reverse-scored before calculating the total score. Based on established cut-off points, scores were categorized as low (20–40), moderate (41–99), and high (100–120) (Ebrahimi et al., 2015). The SWBS has demonstrated strong validity and reliability, with a reported Cronbach’s alpha of 0.82 (Ebrahimi et al., 2015). The Arabic version used in this study also showed good construct validity and reliability, with Cronbach’s alpha values ranging from 0.82 to 0.87 (Musa and Pevalin, 2012). In the current study, the SWBS demonstrated excellent internal consistency, with a Cronbach’s alpha of 0.91.
The WHOQOL-BREF was used to assess QOL. This 26-item instrument includes four domains: physical health (7 items), psychological well-being (6 items), social relationships (3 items), and environment (8 items), along with two items assessing overall health and general QOL (WHOQOL Group, 1998). Each item is rated on a 5-point Likert scale ranging from 1 (very dissatisfied/very poor) to 5 (very satisfied/very good). Domain scores were calculated in accordance with the WHOQOL-BREF manual, yielding scores from 4 to 20, with higher scores indicating better functioning in the respective domain (WHOQOL Group, 1998). Overall QOL was interpreted using the mean domain scores, where a score below 48.00 indicated low QOL, and a score above 48.00 indicated high QOL. The WHOQOL-BREF has demonstrated strong psychometric properties, with a Cronbach’s alpha of 0.89 reported in previous studies (Krägeloh et al., 2011). The Arabic version used in this study also demonstrated high validity and reliability, with a Cronbach’s alpha of 0.91 (Almarabheh et al., 2023). In the current study, internal consistency was excellent, with a Cronbach’s alpha of 0.94.
Ethical considerations
Ethical approval was obtained from the Institutional Review Board (IRB) of the Jordanian Ministry of Health (Reference No. 198/2024). Participants were asked to provide written informed consent and were informed of their right to decline participation or withdraw from the study at any time without any consequences. To ensure confidentiality, all data were handled securely, and no personal identifiers were disclosed.
Data collection procedures
Following approval from the selected hospitals, meetings were conducted with the head nurses of the hemodialysis units to explain the purpose and significance of the study. Eligible participants were then informed about the study, and paper questionnaires were distributed and collected by the researchers prior to their dialysis sessions. To accommodate any potential discomfort during treatment, participants were given the option to choose a convenient time to complete the questionnaires.
Data analysis
Data analysis was conducted using the Statistical Package for the Social Sciences (SPSS) version 26.0. The normality of the data was assessed using the Kolmogorov–Smirnov test, which indicated that the data were normally distributed and free from outliers (p > 0.05). Descriptive statistics, including frequency, percentage, mean, and standard deviation, were used to summarize the study variables. Correlation analyses were performed using Pearson’s correlation coefficient (r) and the point-biserial correlation coefficient (p.b.r). Pearson’s correlation was used to examine associations between continuous variables, while p.b.r was applied to assess relationships between continuous and dichotomous or categorical variables.
Linear multivariate regression analysis was employed to identify significant predictors of QOL. Prior to the regression analysis, relevant variables were converted into dichotomous categories. Multicollinearity was assessed using tolerance values and the Variance Inflation Factor (VIF), in line with the guidelines of Hair (2019). According to Warner (2008), multicollinearity is considered problematic when tolerance falls below 0.1 or when VIF exceeds 10. In this study, all values were within acceptable ranges, with VIF values ranging from 1.214 to 2.981 and tolerance values between 0.218 and 0.967. The Durbin–Watson statistic was used to check for autocorrelation, yielding a value of 1.634, which is considered acceptable based on Hair’s (2019) criteria.
To further explore the identified predictors, independent samples t-tests were conducted (Flanagan et al., 2025). One-way analysis of variance (ANOVA) and independent t-tests were used to examine whether significant differences in the dependent variable existed across the levels of the independent variables. When significant differences were found, Scheffé’s post hoc test was used for pairwise comparisons.
Effect sizes were calculated to complement statistical significance testing. For comparisons between two groups, Cohen’s d was used, with interpretation as follows: 0.10–0.29 = small effect, 0.30–0.49 = moderate effect, and 0.50–1.00 = large effect (Lakens, 2013). For comparisons involving more than two groups, Eta squared (η2) was used, with values interpreted as: <0.01 = no effect, 0.01–0.06 = small effect, 0.061–0.14 = moderate effect, and >0.14 = large effect (Lakens, 2013). A p-value less than 0.05 was considered statistically significant throughout the analysis.
Results
Socio-demographic characteristics of the participants
Out of 254 distributed questionnaires, 238 were completed and returned, yielding a response rate of 93.7%. Among the participants, 58.8% were male and 41.2% female. Approximately 67.2% were married, and 70.6% had completed secondary education or less. The mean age was 52.4 years (SD ± 15.5), and the average monthly income was 420 JOD (SD ± 380), consistent with the national average in Jordan. Participants had been on hemodialysis for an average of 6.5 years (SD ± 5.3; see Table 1).
Demographic characteristics of the participants (N = 238).
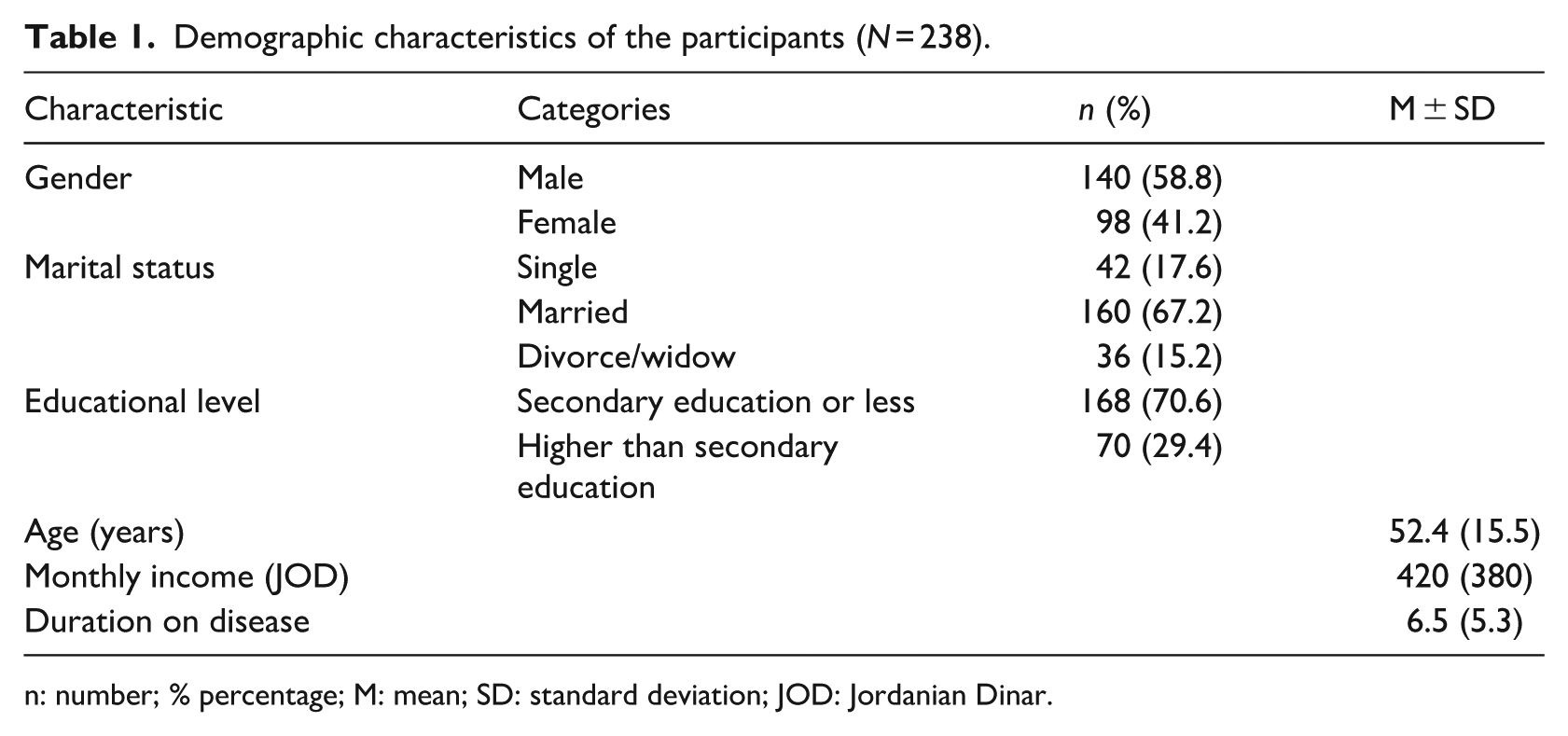
n: number; % percentage; M: mean; SD: standard deviation; JOD: Jordanian Dinar.
Levels of spiritual well-being and QOL
The analysis revealed that participants had a moderate level of spiritual well-being, with a mean score of 92.6 (SD ± 13.3) out of 120. Specifically, the religious well-being subscale showed a high mean score of 51.5 (SD ± 7.9) out of 60, while the existential well-being subscale reflected a moderate mean score of 41.1 (SD ± 7.8) out of 60. Regarding QOL, the overall mean score was 47.2 (SD ± 8.35), indicating a low level of QOL. Among the four QOL domains, the physical health domain had the lowest mean score at 11.1 (SD ± 2.95) out of 20, whereas the social relationships domain scored the highest, with a mean of 13.2 (SD ± 3.42) out of 20 (see Table 2).
Levels of spiritual well-being and QOL among participants (N = 238).
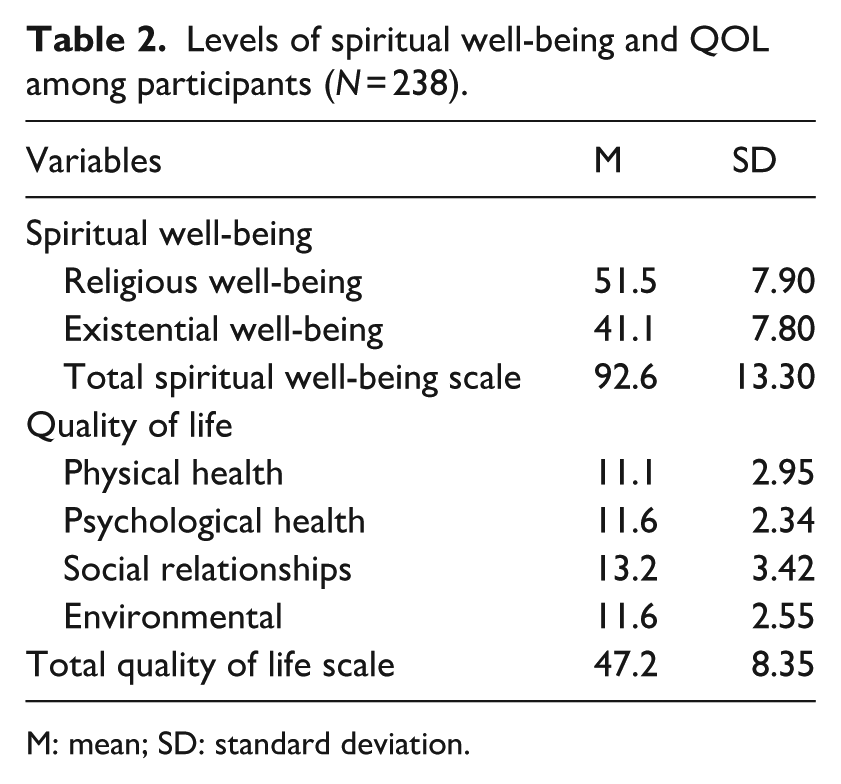
M: mean; SD: standard deviation.
Association between spiritual well-being, socio-demographics (e.g. age, gender, duration on hemodialysis, educational level, income/month, and marital status), and QOL
The results indicated a significant positive correlation between QOL and several factors: spiritual well-being (r = 0.412, p < 0.001), monthly income (r = 0.186, p < 0.001), marital status (p.b.r = 0.232, p < 0.001), and educational level (p.b.r = 0.253, p < 0.001). In contrast, QOL was negatively correlated with age (r = −0.174, p < 0.01; Table 3).
Correlations between QOL, spiritual well-being, and socio-demographic characteristics.
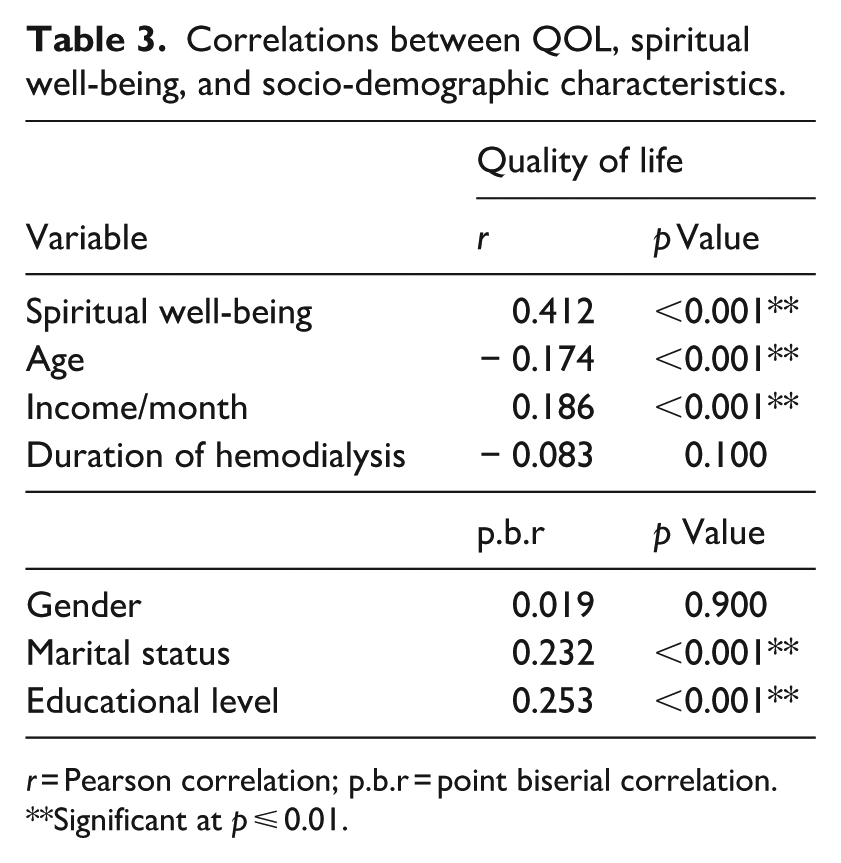
r = Pearson correlation; p.b.r = point biserial correlation.
**Significant at p ⩽ 0.01.
Predictors of QOL
Table 4 presents the results of the multiple linear regression analysis. The model was statistically significant (F = 30.93, p < 0.001), with all independent variables collectively accounting for approximately 29.3% of the variance in QOL scores. The analysis identified spiritual well-being (β = 0.392, p < 0.01), educational level (β = 0.247, p < 0.01), and monthly income (β = 0.120, p < 0.05) as significant predictors of QOL. Specifically, for every one-point increase in spiritual well-being, educational level, and monthly income, QOL increased by 39.2%, 24.7%, and 12.0%, respectively.
Predictors of quality of life among participants.
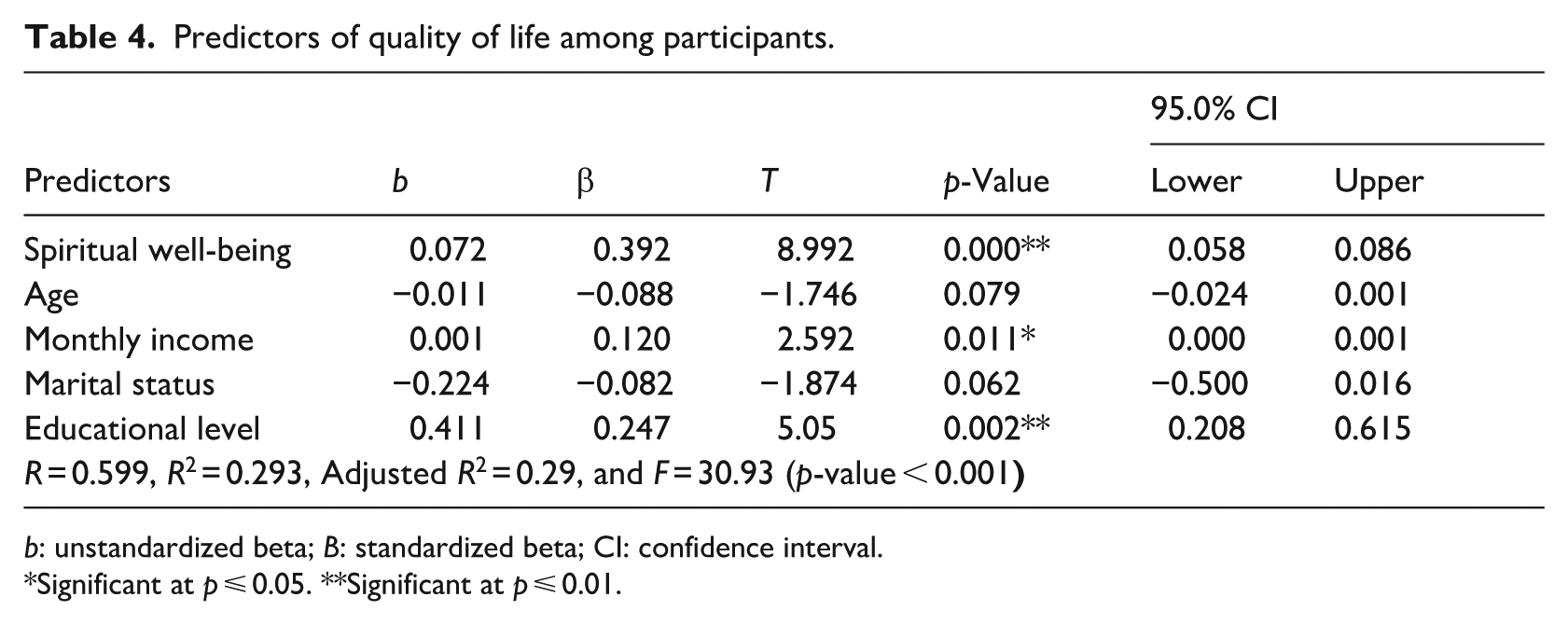
b: unstandardized beta; B: standardized beta; CI: confidence interval.
Significant at p ⩽ 0.05. **Significant at p ⩽ 0.01.
As shown in Table 5, there was no statistically significant difference in QOL based on gender (t = 0.265, p > 0.05), indicating that male and female participants reported similar QOL levels. However, significant differences in QOL were found based on marital status (F = 6.96, p < 0.001) and educational level (t = 1.780, p < 0.001). Further analysis with Scheffé’s test showed that married participants had significantly higher QOL compared to single and divorced/ widowed individuals (p < 0.05). The effect size for gender was Cohen’s d = 0.03, a very small (negligible) effect size, consistent with the p-value (0.798), indicating no meaningful difference between male and female groups. The effect size for educational levels was Cohen’s d = 0.23, considered a small effect size. The effect size for marital status was η2 = 0.056, representing a small to medium effect size.
Differences in the quality of life according to gender, marital status, and educational level.
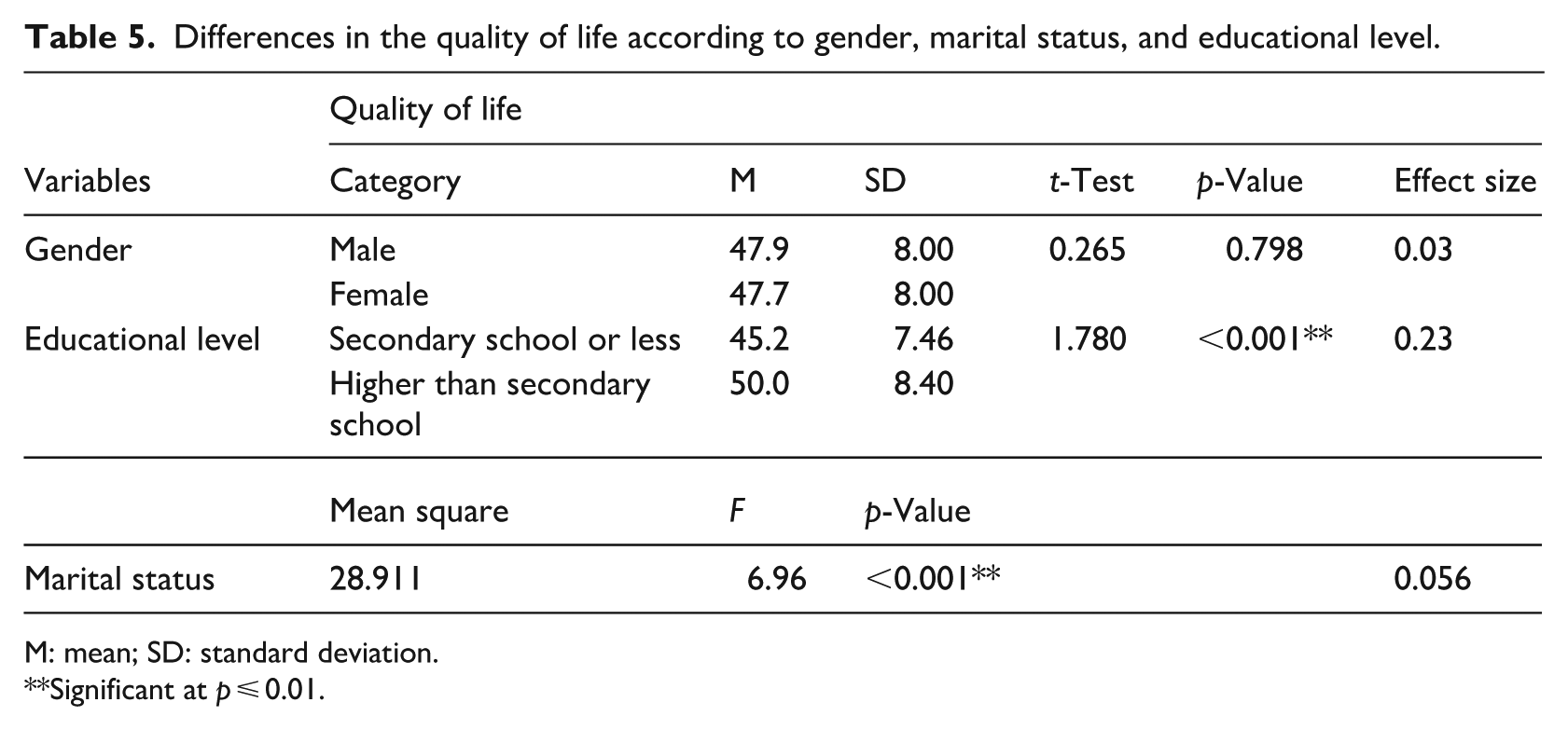
M: mean; SD: standard deviation.
Significant at p ⩽ 0.01.
Discussion
This study explored the relationship between spiritual well-being and QOL among Muslim patients with CKD undergoing hemodialysis. Our findings revealed that participants exhibited moderate levels of spiritual well-being, consistent with previous research (Musa et al., 2018, 2023; Pilger et al., 2017; Rayani et al., 2025). Notably, participants reported high levels of religious well-being alongside moderate levels of existential well-being—findings that contrast with earlier studies where religious well-being was typically moderate and existential well-being was low (Musa et al., 2018, 2023; Pilger et al., 2017). These results suggest that despite the physical and emotional challenges of hemodialysis, participants maintained a strong, positive perception of their relationship with God (Pilger et al., 2017). The relatively high religious well-being observed may be influenced by Islamic beliefs, which often provide a profound source of patience, resilience, and spiritual strength during hardship (Musa et al., 2023). For many Muslim patients, faith not only helps them endure pain and suffering but also serves as a foundation for finding purpose and joy amid adversity. Rooted in the teachings of the Qur’an, this spiritual connection offers comfort and plays a vital role in enhancing overall well-being (Musa et al., 2023).
This study also found that participants reported poor QOL, consistent with previous research (Abdulqader and Ali, 2023; Alshraifeen et al., 2022; Bakker et al., 2024; Emtair et al., 2021; Ganeshkumar Raja et al., 2023; Gebrie et al., 2023; Kim et al., 2021; Lazarus, 2019; Mollaoglu and Başer, 2021; Musa et al., 2018, 2023; Qaddumi et al., 2020; Ravindran et al., 2020; Rehman et al., 2020). This diminished QOL may stem from the burdens associated with hemodialysis, including limited physical activity, chronic pain, lengthy and frequent treatment sessions, loss of employment, and financial difficulties (Ravindran et al., 2020). Additionally, disease-related factors such as strict dietary restrictions, repeated hospitalizations, loss of independence, sleep disturbances, fatigue, fear of the future, lifestyle adjustments, and reduced energy levels for physical activity further contribute to the decline in QOL among these patients (Mafi et al., 2018; Mollaoglu and Başer, 2021; Qaddumi et al., 2020).
Regarding the QOL domains, our study found that the social relationships domain scored the highest, consistent with previous research (Ganeshkumar Raja et al., 2023). This suggests that participants’ social needs were well-supported through strong family and community connections (Emtair et al., 2021). In Jordan, many patients are part of extended family systems that provide a robust support network, reinforcing social bonds and relationships (Malak et al., 2018). In contrast, the physical health domain recorded the lowest QOL scores, aligning with earlier studies (Krägeloh et al., 2011; Pompey et al., 2019). This is likely due to the physical symptoms associated with hemodialysis and CKD, as well as reduced independence and limitations in daily activities (Gebrie et al., 2023).
This study identified a positive correlation between spiritual well-being and QOL, with spiritual well-being emerging as a significant predictor of QOL, consistent with previous research (Musa et al., 2018, 2023). These findings align with Puchalski’s Model of Spiritual Care, which emphasizes the integration of spirituality into holistic, patient-centered care, recognizing its vital role in enhancing well-being and QOL (Puchalski et al., 2009). As a fundamental dimension of overall health (Vahednasiri and Valadkhani, 2022), spirituality plays a crucial role in maintaining and improving QOL (Pilger et al., 2017). Patients often rely on spirituality as a coping mechanism, drawing strength, peace, fulfillment, and support to navigate the physical and emotional challenges posed by their illness and treatment (Knegtering et al., 2024; Musa et al., 2018, 2023).
Our study identified a significant correlation between marital status and QOL, with married participants reporting higher QOL compared to those who were single, divorced, or widowed. This finding is consistent with prior research, which indicates that widowed or divorced individuals often experience lower QOL than their married or never-married counterparts (Alshraifeen et al., 2022; Iqbal et al., 2020; Vahednasiri and Valadkhani, 2022). However, a study conducted in Bahrain reported contrasting results, finding no significant association between marital status and QOL (Vahednasiri and Valadkhani, 2022). The discrepancy may be attributed to contextual or cultural differences affecting social support systems. In the present study, the higher QOL observed among married individuals may be explained by the greater psychosocial support they typically receive. Married individuals often benefit from stronger family ties and greater emotional, social, and financial support from their spouses and extended families, which can enhance their capacity to cope with the challenges of chronic illness (Alnaeem et al., 2024; El-Habashi et al., 2020).
In the current study, income demonstrated a positive correlation with QOL and emerged as a significant predictor of QOL. This finding aligns with previous research (Abdulqader and Ali, 2023; Alghamdi et al., 2023; Boukhira et al., 2022; Valsa Jose et al., 2022). Individuals with higher income levels are generally better equipped to access quality healthcare services and meet their daily living needs. Moreover, financial stability contributes to enhanced self-esteem, a stronger sense of fulfillment, and reduced anxiety about the future—all of which are important factors in improving overall QOL (Ng et al., 2021).
Our study also revealed a positive relationship between educational level and QOL, consistent with findings from previous research (Alghamdi et al., 2023; Bakker et al., 2024; Gebrie et al., 2023; Kim et al., 2021; Ravindran et al., 2020). However, this result contrasts with a prior study conducted in Jordan and another investigation, both of which found no significant association between education and QOL (El-Habashi et al., 2020). The current findings may be attributed to the notion that individuals with higher educational attainment are better equipped to understand their illness and its implications. This greater health literacy can facilitate improved self-management, stronger adherence to treatment regimens, and ultimately, a higher QOL (Raghupathi and Raghupathi, 2020; Toole et al., 2020).
This study found a negative correlation between age and QOL, aligning with the findings of previous research (Gebrie et al., 2023; Kim et al., 2021; Ravindran et al., 2020). This relationship may be attributed to age-related declines in physical health, including reduced energy levels, diminished work capacity, and poorer sleep quality—all of which can negatively impact QOL (Amarya et al., 2018). Additionally, older individuals are more likely to experience multiple comorbidities, which can further deteriorate their overall QOL (Naseef et al., 2023).
Limitations of the study
Despite its important findings, this study has several limitations. First, the cross-sectional design limits the ability to draw causal inferences between variables. Second, the reliance on self-reported measures may introduce response bias and affect the accuracy of the data. Additionally, the use of convenience sampling limits the generalizability of the results to the broader population. The study also excluded illiterate patients, which may have led to the underrepresentation of certain demographic groups. Moreover, potentially influential variables such as religious beliefs and spirituality, perceived family support, and duration of time on hemodialysis were not assessed. Future research should consider incorporating these factors to provide a more comprehensive understanding of the determinants of QOL among hemodialysis patients.
Implications for practice
As part of delivering holistic care, healthcare professionals should assess and support all dimensions of patient well-being, including spiritual health. Recognizing QOL as a key outcome measure is essential for evaluating patients with CKD undergoing hemodialysis, monitoring their progress, and determining the effectiveness of treatment plans. This study underscores the significant physical and psychological challenges faced by these patients. Therefore, enhancing QOL should be a central priority for healthcare providers and stakeholders.
Developing and implementing comprehensive therapeutic programs for patients with CKD on hemodialysis is crucial. These programs should prioritize the integration of spiritual well-being to improve patients’ understanding of their disease, treatment options, dietary restrictions, and necessary lifestyle changes—ultimately empowering them to manage their condition more effectively and improve their overall QOL. Additionally, rehabilitation programs are needed to help patients regain independence, enhance physical functioning, and support psychosocial adjustment.
Interdisciplinary collaboration among nephrologists, psychologists, dialysis nurses, and family members is vital to ensure patient-centered care focused on improving QOL. Nursing care guidelines should explicitly address and support both spiritual well-being and QOL. Furthermore, policymakers should allocate additional financial resources to support this population, as such investment can substantially enhance their QOL. Targeted initiatives, training, and programs that demonstrate the benefits of integrating religious or spiritual approaches into care should also be funded and widely implemented.
Conclusion
This study found that participants reported moderate levels of spiritual well-being and poor overall QOL. Several factors, including spiritual well-being, age, income, marital status, and educational level, were significantly correlated with QOL. Among these, spiritual well-being, income, and educational level emerged as significant predictors. These findings underscore the importance of addressing not only the medical but also the spiritual, educational, and financial needs of patients with CKD undergoing hemodialysis in order to improve their overall QOL.
Integrating spiritual care into treatment plans, alongside providing access to counseling services and support groups, may help patients better cope with the physical and emotional challenges of hemodialysis, ultimately enhancing their QOL. Future research should prioritize qualitative studies to explore patients’ lived experiences with hemodialysis and how it affects their QOL, particularly in relation to spirituality. In addition, interventional studies are needed to evaluate the effectiveness of spiritual therapies in improving QOL among this patient population.
Footnotes
Ethical considerations
Approval was obtained in accordance with the Declaration of Helsinki from the Helsinki Committee in Jordan, and the Institutional Review Board (IRB) at the Jordanian Ministry of Health with reference No# 198/2024.
Consent to participate
Participants provided informed written consent. Confidentiality of the data was maintained throughout data collection and analysis.
Consent for publication
Consent for publication is not applicable to this article as no identifiable participant data are included.
Author contributions
M.M. conducted conceptualization. M.M. conducted data curation. M.M. and A.S. respectively conducted the methodology. All authors conducted the writing of the original draft. M.M. and A.S. conducted writing, review, and editing. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data are available from the corresponding author upon reasonable request.