
Abstract
This descriptive qualitative study explored how individuals with cancer perceive their illness across different stages and contexts. Using a reflexive thematic analysis (RTA) framework, the study followed the Standards for Reporting Qualitative Research (SRQR) for transparency. Data were gathered through six semi-structured focus group discussions with 35 patients diagnosed with breast, lung, colorectal, or gastric cancer. Purposive sampling continued until sufficient information was obtained. Analysis yielded four overarching themes: (1) paradox of illness description, (2) paradox of disease causation, (3) paradox of treatment effects, and (4) paradox of life disruption. Participants expressed ambivalent understandings of cancer, some viewing it as a manageable, flu-like condition, while others experienced it as a life-threatening, identity-defining event. Similar tensions emerged regarding perceived causes, treatment responses, and the illness’s broader impact. These paradoxes highlight the complexity of cancer perceptions and the need for individualised, psychosocially informed care across the illness trajectory.
Keywords
Introduction
Cancer profoundly affects patients across physical, psychological, social, and existential domains. Diagnosis and treatment often trigger significant distress and coping difficulties (Mehnert-Theuerkauf et al., 2023; Seiler and Jenewein, 2019), commonly involving stigma, emotional ambivalence, and perceived loss of control linked to illness beliefs and emotional representations (Alaloul et al., 2025; Bashiri-Nejadian et al., 2021). Such distress arises from pain, fear of death, social isolation, debilitating treatments, and uncertainty, frequently persisting across the illness trajectory. Socioeconomic consequences-such as work disruption and financial strain—further compel individuals to reconstruct their sense of identity (Czerw et al., 2020; Wang et al., 2024).
Cancer remains one of the most feared diseases, largely due to its historical association with death (Lester et al., 2006). Quantitative studies show it is perceived as painful, poorly understood, and fatal (Robb et al., 2014). Yet, societal views have evolved: Jensen et al. (2013) noted that survival perceptions vary widely and are shaped by media framing, which can either reinforce or challenge fatalistic beliefs. Parallel to advances in detection and treatment, survival outcomes have improved markedly. Globally, more than 53 million people live at least 5 years post-diagnosis (World Health Organisation (WHO), 2024). In the U.S., mortality rates have declined by over 33% since 1991, resulting in approximately 3.8 million fewer deaths (Siegel et al., 2023).
In recent years, the concept of illness perceptions has been increasingly studied in chronic conditions, such as diabetes, cardiac disease, and cancer, particularly within the framework of Leventhal’s Common-Sense Model (CSM; Hagger et al., 2017; Leventhal et al., 1980). The Common-Sense Model (CSM) conceptualises illness perceptions across five core dimensions-identity, cause, timeline, control, and consequences—each interacting with emotional representations to shape coping and adaptation (Cameron and Leventhal, 2012; Diefenbach and Leventhal, 1996). Research indicates that these perceptions are dynamic, self-regulatory constructs that influence mental health and treatment engagement (Petrie et al., 2008). The CSM thus offers a valuable framework for understanding the subjective, multidimensional experiences of cancer patients. Qualitative studies in other conditions, such as anorexia nervosa, similarly reveal that illness perceptions intertwine with identity and emotional meaning-making (Higbed and Fox, 2010), underscoring the relevance of qualitative approaches to exploring cancer experiences.
As survival improves and cancer increasingly resembles a chronic illness, reframing societal and personal perceptions of cancer has become crucial (The Lancet Oncology, 2016). Recent evidence indicates a gradual shift towards more optimistic public attitudes. For example, 90% of U.S. adults in the Health Information National Trends Survey believed that regular colorectal cancer screening enhances early detection and access to treatment (Agunwamba et al., 2023). Likewise, surveys in Canada, Australia, Scandinavia, and the United Kingdom found that 90% agreed “cancer is often treatable” (Robb et al., 2014).
Illness perceptions-individuals’ cognitive and emotional representations of their disease-strongly influence psychological resilience, emotional regulation, coping, treatment adherence, and health outcomes (Hagger et al., 2017; Hopman and Rijken, 2015). These perceptions not only shape adjustment but also influence prognosis (Czerw et al., 2020; Wang et al., 2024). Thus, understanding how patients perceive cancer is essential for healthcare professionals, particularly nurses, who guide patients throughout the illness trajectory (Günüşen et al., 2013; Leal et al., 2015).
Recovery-oriented models in mental health emphasise meaning-making and narrative reconstruction as key to adaptation (Soundy et al., 2015), parallelling how cancer patients may hold paradoxical illness representations. Although many studies address cognitive and emotional aspects of cancer, few examine how conflicting meanings coexist simultaneously. To capture this complexity, the present study adopts a paradox framework—defined as the persistent coexistence of contradictory experiences (e.g. viewing cancer as both ordinary and lethal). Unlike dialectical tensions that imply resolution, paradoxes underscore the enduring presence of both poles. This perspective provides a deeper insight into how individuals navigate ongoing contradictions in their illness experience (Leal et al., 2015; Vehling and Philipp, 2018).
Aims
This study aimed to explore and analyse the illness perceptions of cancer patients, focusing on the paradoxical experiences they face regarding their disease, its causes, the effects of treatment, and the overall impact on their lives.
Methods
Design
This study employed a descriptive qualitative design, which enables participants to articulate their views and experiences related to the research topic, thereby providing rich and detailed data for in-depth analysis (Creswell, 2013). Reporting followed SRQR and, for focus-group studies, we additionally completed the COREQ (32-item) checklist; relevant items are integrated into the text below. The research process was guided by the Standards for Reporting Qualitative Research (SRQR) checklist, and the development of the interview guide was informed by Leventhal’s Common-Sense Model (CSM) to capture both cognitive and emotional dimensions of illness perceptions (Cameron and Leventhal, 2012; Diefenbach and Leventhal, 1996; Hagger et al., 2017; Leventhal et al., 1980). A dedicated reflexivity statement is included to describe the researcher’s background, assumptions, and relationships with participants (Berger, 2015).
Study setting and recruitment
The study was conducted over a 2-month period in six hospitals located across two major cities in Turkey, comprising two universities, two public hospitals, and two private hospitals. These hospitals serve patients from various regions of Turkey, representing diverse socioeconomic and cultural backgrounds, thereby ensuring a diverse participant pool. These hospitals were selected based on their capacity to yield comprehensive data on the illness perceptions of Turkish cancer patients. Focus groups were held in private meeting rooms adjacent to oncology clinics to maximise comfort and confidentiality; only participants and the research team were present.
This study constitutes the third phase of a larger project titled “The Psychosocial Needs, Coping Styles, and Quality of Life of Cancer Patients.” Using purposive sampling, participants were selected from those who participated in the project’s second (quantitative) phase.
A total of six focus groups were conducted (n = 35; groups typically ranged from 5 to 7 participants), with variation in cancer type and disease stage to enable contrasting perspectives while maintaining sufficient common ground for psychological safety. Group composition, balanced for homogeneity (e.g. similar treatment trajectories) and heterogeneity (e.g. diagnosis/stage differences), fosters disclosure and elicits divergent meanings. Sessions were moderated by the principal investigator (PG; mental health nursing/psycho-oncology qualitative experience) and a co-facilitator, who took field notes and supported the group process (time-keeping, turn-taking). The adequacy of the sample size was guided by information power, considering the focused aim, participant specificity, high interview quality, and an interpretive analytic strategy. We monitored redundancy through reflexive analytic memos and observed no substantially new patterns in the final two groups. (Accordingly, “data saturation” language has been replaced with an information-power justification consistent with reflexive thematic analysis (Braun and Clarke, 2006).) Consequently, 35 patients have been included: 4 lung cancer patients, 15 breast cancer patients, 10 colorectal cancer patients, and 6 gastric cancer patients. None of the participants declined participation or withdrew from the study.
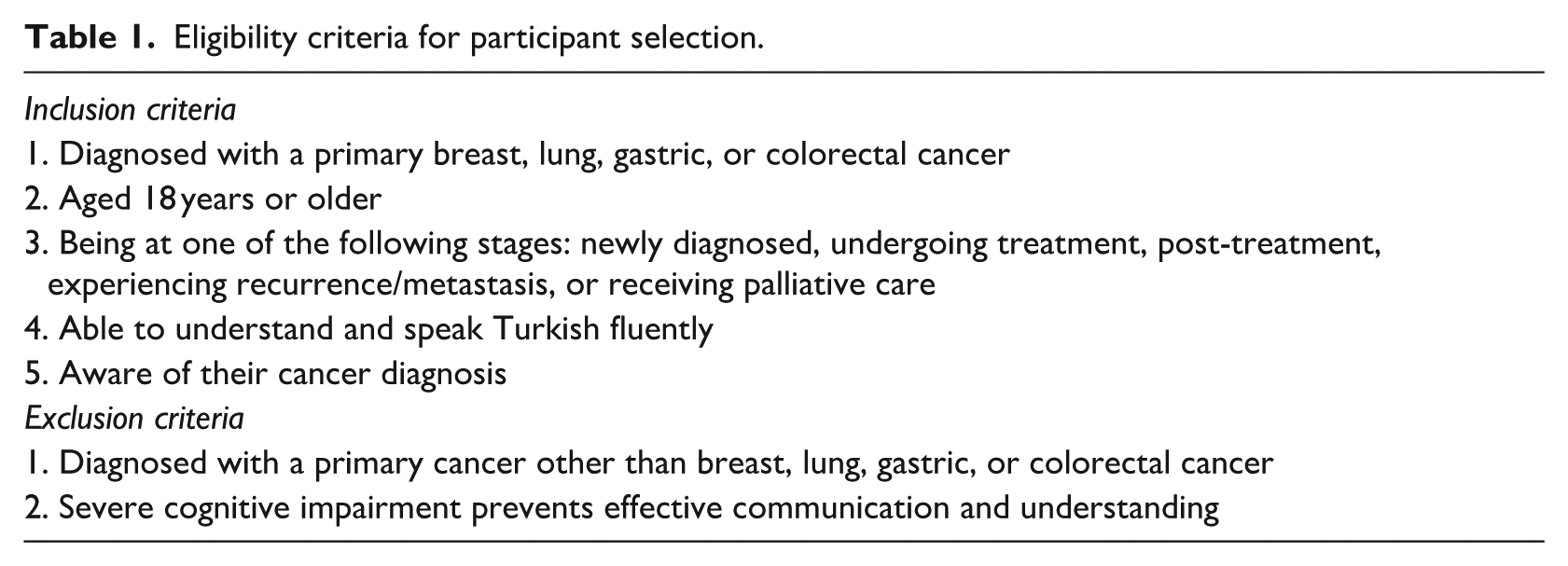
Inclusion criteria were as follows: (1) having a primary diagnosis of breast, lung, colorectal, or gastric cancer; (2) being aged 18 years or older; (3) being in any disease stage (newly diagnosed, undergoing treatment, post-treatment, recurrence/metastasis, or palliative stage); (4) having good proficiency in the Turkish language; and (5) being aware of their cancer diagnosis. Patients were excluded if they had a primary diagnosis other than one of the four specified cancers or if cognitive impairments prevented effective communication, as detailed in Table 1.
Eligibility criteria for participant selection.
Data collection
Data were collected through six semi-structured focus group discussions conducted in private, independent hospital settings to ensure participant comfort and confidentiality. The discussions were facilitated by a principal investigator (PG) experienced in qualitative research, supported by another researcher who took field notes. The moderator fostered inclusive participation, explicitly inviting quieter voices and negotiating turn-taking to protect disclosure in a sensitive context.
The semi-structured interview guide was developed by the principal investigator through a literature review and consultations with experts in psycho-oncology and qualitative research. It was pilot-tested with two patients and revised for clarity and cultural sensitivity. Grounded in Leventhal’s Common-Sense Model (CSM) of Illness Representation, each question corresponded to one or more CSM dimensions (e.g. identity, cause, timeline, controllability, emotional representation). Probe questions were used to facilitate deeper exploration of participants’ experiences (see Table 2).
Interview guide with corresponding dimensions of the common-sense model and probe questions.
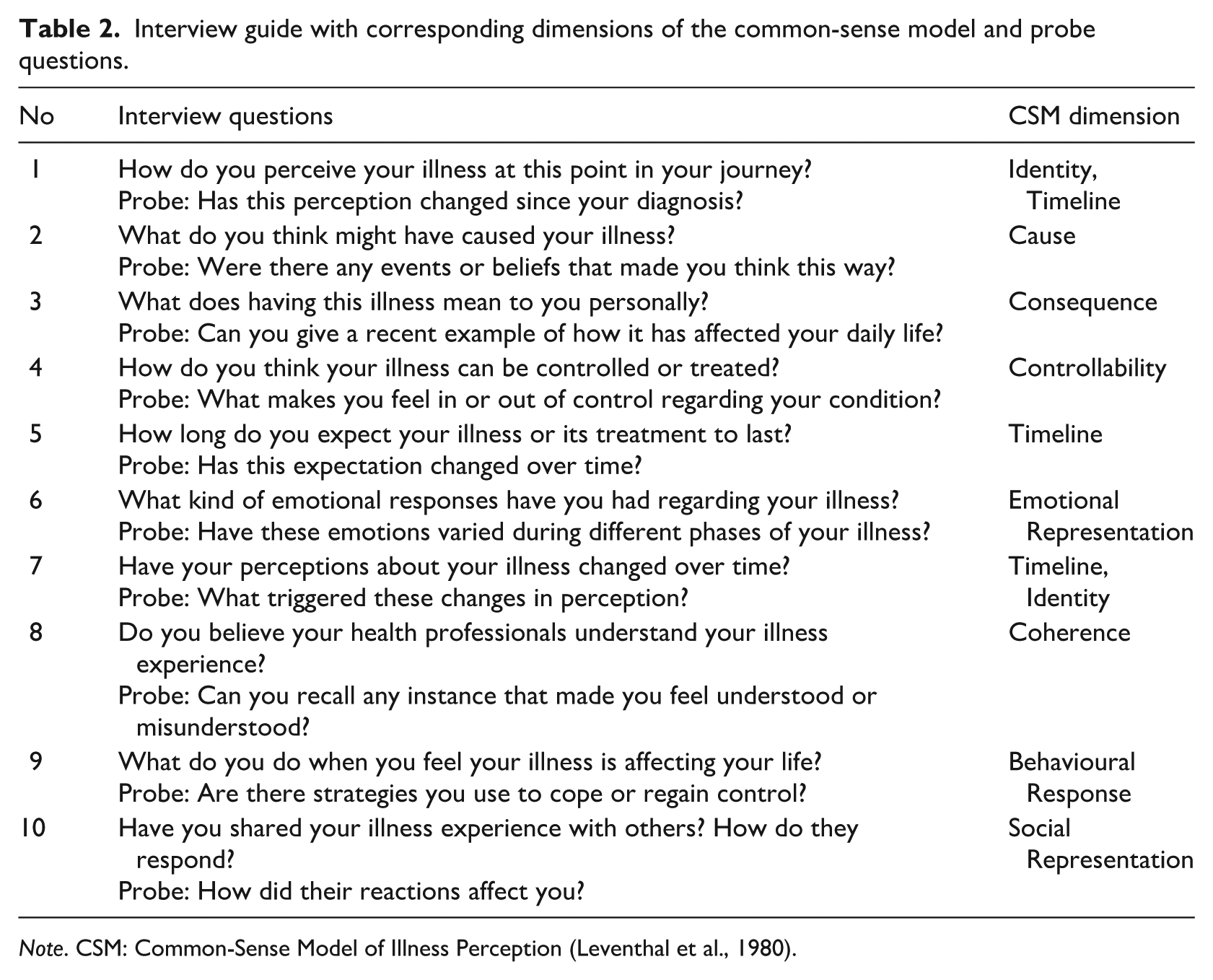
Note. CSM: Common-Sense Model of Illness Perception (Leventhal et al., 1980).
Focus group discussions, lasting 70–130 minutes, were conducted using this guide and audio-recorded with consent. Flexibility in question order allowed natural conversation flow while maintaining consistency across sessions. The focus group method was selected to harness group interaction and generate rich, reflective insights into patients’ perceptions of their illness. Researcher characteristics, relationship with participants (none clinically), and recruitment flow are summarised in Supplemental File S1 (COREQ).
Researcher reflexivity and positionality
The research team consisted of three oncology nursing scholars and one psycho-oncology specialist, all of whom were experienced in qualitative research and cancer care; however, none had established therapeutic relationships with the participants. This positioning provided both insider insight and outsider critical distance. Reflexivity was maintained through analytic memos, field notes, and iterative team discussions addressing assumptions, emotions, and interpretations. The lead author moderated all focus groups and documented reflections after each session. Peer debriefing was used to challenge emerging interpretations and minimise over-identification with participants’ narratives. These strategies enhanced transparency and credibility, ensuring that themes reflected participants’ lived experiences rather than researchers’ biases, consistent with principles of reflexive thematic analysis and qualitative rigour (Berger, 2015; Braun and Clarke, 2021).
Rigour
Trustworthiness was ensured through multiple strategies. A table illustrating the progression from initial codes to final themes enhanced analytic transparency (Braun and Clarke, 2006; see Table 3). Credibility was supported by triangulation, member checking with selected participants, and peer debriefing with qualitative experts (Creswell, 2013). Dependability and confirmability were achieved via an audit trail of analytic memos and decision logs, complemented by reflexive team discussions rather than intercoder reliability checks. Negative and deviant cases were analysed to test the robustness of each paradox.
Themes, sub-themes, descriptions, and illustrative quotes (supplementary analytical table showing the code-subtheme-theme linkage).
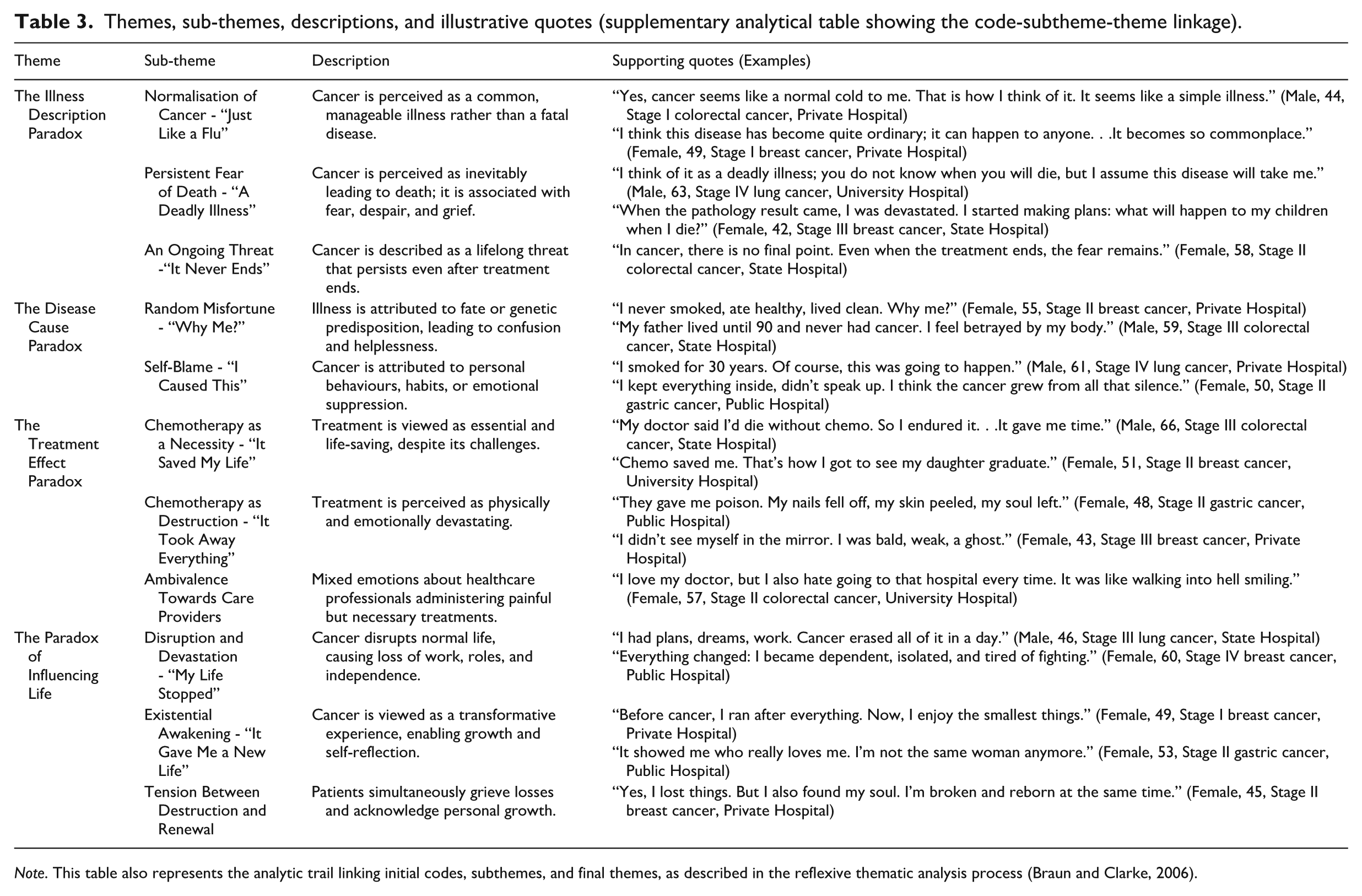
Note. This table also represents the analytic trail linking initial codes, subthemes, and final themes, as described in the reflexive thematic analysis process (Braun and Clarke, 2006).
Rich contextual descriptions, detailed participant demographics, and transparent documentation enhanced transferability. A bilingual qualitative expert reviewed the quotations to ensure accurate translation from Turkish to English (Berger, 2015). Researcher reflexivity and positionality, encompassing professional backgrounds, assumptions, and lack of care relationships, are detailed in the Methods, clarifying how these factors shaped data interpretation (Berger, 2015; Bury, 1982).
Ethical considerations
Ethical approval for this study was obtained from the Koç University Ethics Committee (Approval No: 2016.155.IRB3.086). Institutional permissions were secured from all participating hospitals. Participants were informed verbally and in writing about the study’s purpose, voluntary participation, withdrawal rights, and confidentiality. Written and verbal informed consent was obtained before data collection. All data were anonymised and securely stored.
Data analysis
All focus group recordings were transcribed verbatim. Data were analysed using reflexive thematic analysis, as described by Braun and Clarke (2006). This method emphasises the active role of the researcher in theme development and recognises that themes are not passively discovered but constructed through deep engagement with the data. The analysis proceeded in six recursive phases (Braun and Clarke, 2006):
Familiarisation with the data: All focus group recordings were transcribed verbatim. The researchers repeatedly read the transcripts to immerse themselves in the participants’ narratives.
Generating interpretive leads (initial coding): Multiple analysts coded meaning units inductively and met to compare interpretations (rather than to calculate agreement), using reflexive memoing to track assumptions and analytic decisions.
Constructing candidate themes: Codes were discussed in team meetings to elaborate patterns and explore alternative readings; conceptual links to CSM dimensions were developed iteratively.
Reviewing themes: Emerging themes were checked against the full dataset to ensure coherence and distinctiveness. Overlapping themes were merged, and ambiguous codes were clarified.
Defining and naming themes: The final themes were refined and named to capture the essence of the participants’ paradoxical experiences. A narrative structure was developed to reflect each theme and its corresponding sub-themes.
Producing the report: The final analysis included a synthesis of each theme, accompanied by illustrative quotations. Themes were contextualised within existing literature and the theoretical framing of illness perceptions. In addition to transcripts, field notes and reflexive memos were used to enrich interpretation. Researcher triangulation and peer debriefing strengthened analytical rigour. The Common-Sense Model (CSM) informed the interpretation of themes, particularly in identifying representations of cognitive and emotional illnesses consistent with theoretical constructs (Hagger et al., 2017; Leventhal et al., 1980). An audit trail documenting code → subtheme → theme development (with exemplar quotes) is provided as Table 3.
Findings
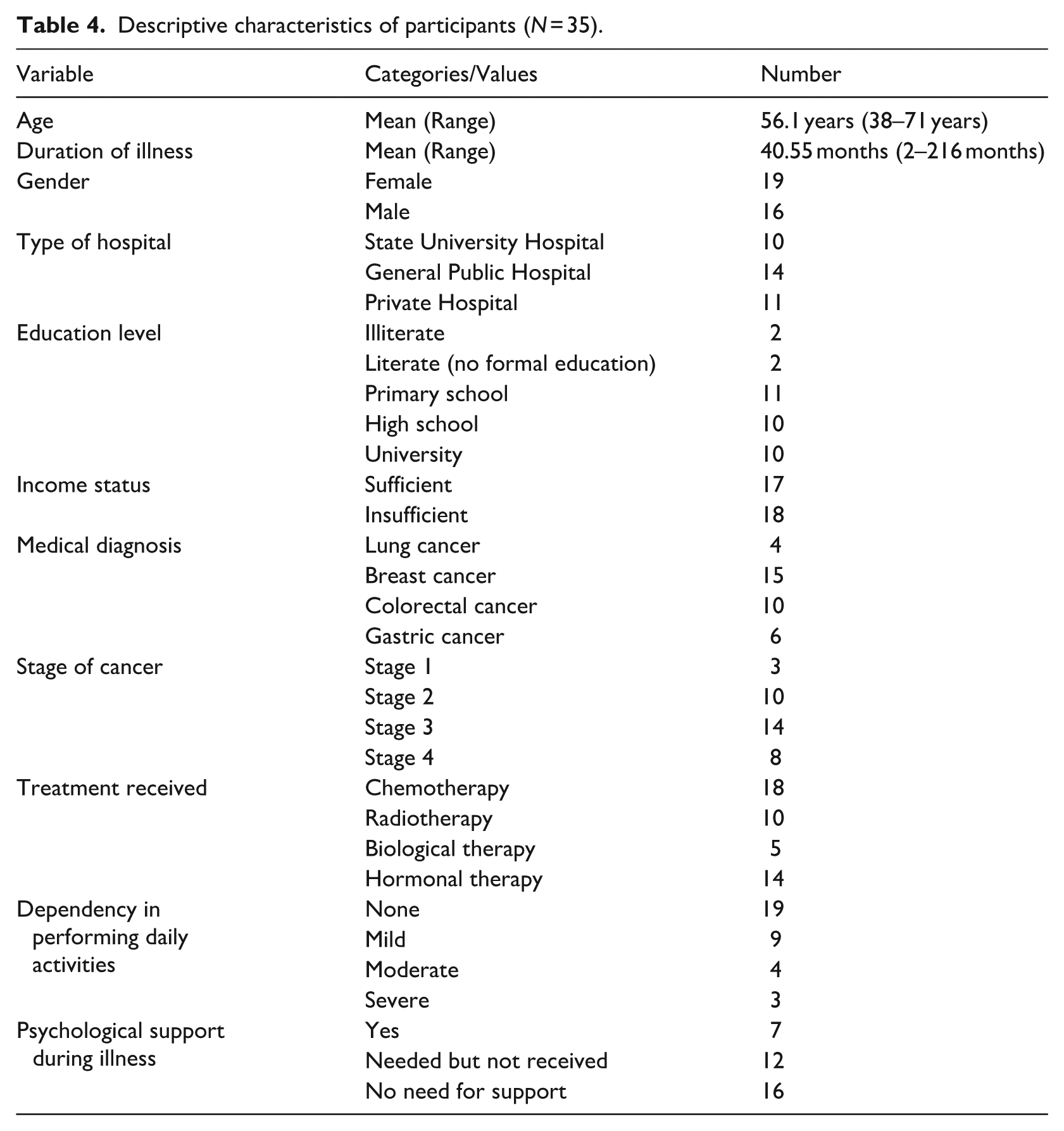
A total of 35 participants (19 women and 16 men), with a mean age of 56.1 years (ranging from 38 to 71), took part in the study. The average duration of illness was 40.55 months, ranging from 2 to 216 months. Participants represented a range of educational backgrounds, from illiterate to university graduates, and nearly half reported insufficient income. The majority had advanced-stage cancer (22 participants in Stage 3 or 4), and many were undergoing or had completed chemotherapy, radiotherapy, hormonal, or biological therapy. While 19 participants reported no dependency in daily activities, others experienced varying levels of impairment. Notably, only 7 participants had received psychological support, and 12 stated they needed it but did not receive any. These descriptive characteristics are summarised in Table 4. For interpretive clarity, the findings are reported using the same four paradox labels that are retained verbatim in the conclusion (ordinary yet deadly; random yet deserved; life-saving yet damaging; destroying yet transformative). Reflexive thematic analysis identified four overarching paradoxes that captured the ambivalence in cancer patients’ illness perceptions ( see Figure 1)
Descriptive characteristics of participants (N = 35).
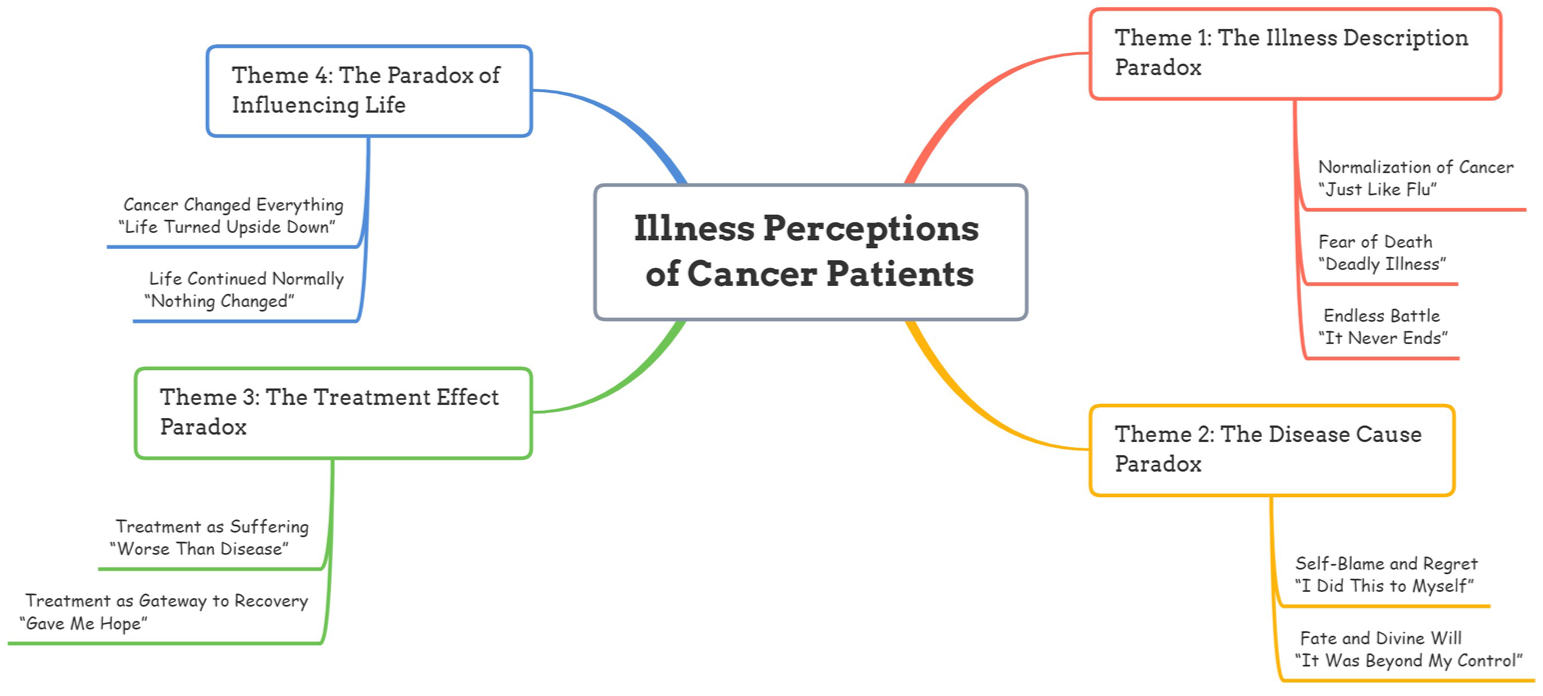
Thematic map illustrating the four major paradoxes of illness perception among cancer patients.
Each paradox consists of conflicting sub-themes that illustrate the internal struggle patients face as they try to make sense of their illness. These paradoxes align with key dimensions of Leventhal’s Common-Sense Model (CSM)-including illness identity, timeline, cause, consequences, control, and emotional representation (Leventhal et al., 1980). Below, we explicitly map each paradox to its primary CSM dimensions and note clinically relevant subgroup patterns observed in our data.
The Illness Description Paradox: Ordinary yet deadly
This paradox reflects patients’ oscillation between normalising cancer and perceiving it as a life-threatening illness. While some viewed cancer as a common, manageable condition, others described it as synonymous with death. This contradiction often coexisted within the same narrative, depending on emotional state and treatment trajectory.
Normalisation of cancer –“Just like a flu”
Some participants minimised the seriousness of cancer, describing it in everyday terms. This normalisation appeared to serve as a coping strategy that downregulated fear, stigma, and helplessness.
“Yes, cancer seems like a normal cold to me. That is how I think of it. It seems like a simple illness.” (Male, 44, Stage I colorectal cancer, Private Hospital) “I think this disease has become quite ordinary; it can happen to anyone. . . It becomes so commonplace” (Female, 49, Stage I breast cancer, Private Hospital)
These expressions align with the “identity” and “consequence” dimensions of CSM, suggesting lowered perceived severity, possibly to preserve psychological equilibrium.
Persistent fear of death –“A deadly illness”
Conversely, many participants described cancer as a death sentence. This view was often accompanied by intense emotional responses such as anxiety, despair, and grief.
“I think of it as a deadly illness; you do not know when you will die, but I assume this disease will take me” (Male, 63, Stage IV lung cancer, University Hospital) “When the pathology result came, I was devastated. I started making plans: what will happen to my children when I die?” (Female, 42, Stage III breast cancer, State Hospital)
This narrative reflects strong activation of the “emotional representation” and “timeline” domains of the CSM, linking diagnosis with anticipated loss and existential threat.
An ongoing threat—“It never ends”
Participants often expressed that even after treatment completion, cancer remained a psychological burden, representing an indefinite threat rather than a closed chapter.
“In cancer, there is no final point. Even when the treatment ends, the fear remains.” (Female, 58, Stage II colorectal cancer, State Hospital)
This experience reflects a cyclical illness timeline representation, disrupting conventional notions of cure and creating sustained anxiety and hypervigilance. Identity, Consequences, Emotional Representation, and Cyclical Timeline are co-activated in this paradox. Participants with early-stage disease more often emphasised “ordinary/manageable,” whereas those with advanced/recurrent disease foregrounded lethality and enduring threat.
The Disease Cause Paradox: Random yet deserved
This paradox demonstrates patients’ struggle to identify the causes of their illness. While some participants perceived cancer as a random or hereditary misfortune, others blamed themselves due to lifestyle habits or emotional suppression.
Random misfortune—“Why Me?”
Participants who could not identify any risk factors perceived cancer as a betrayal by their body or fate. This external attribution helped reduce guilt but increased helplessness.
“I never smoked, ate healthy, lived clean. Why me?” (Female, 55, Stage II breast cancer, Private Hospital) “My father lived until 90 and never had cancer. I feel betrayed by my body.” (Male, 59, Stage III colorectal cancer, State Hospital)
These narratives reflect an external locus of control and activate the “cause” domain of CSM, while simultaneously weakening perceived “control” over illness onset.
Self-blame—“I caused this”
In contrast, some participants assumed full responsibility for their cancer, linking it to unhealthy behaviours or psychological states such as repressed anger or chronic stress.
“I smoked for 30 years. Of course, this was going to happen.” (Male, 61, Stage IV lung cancer, Private Hospital) “I kept everything inside, didn’t speak up. I think the cancer grew from all that silence.” (Female, 50, Stage II gastric cancer, Public Hospital)
This internalised guilt illustrates how causal representations can contribute to emotional distress and self-punishment. Culturally shaped beliefs, such as somatisation of suppressed emotion, may further exacerbate this perception. Cause attributions intersect with perceived Control and Emotional Representation. Men in our sample more frequently framed causation as external/random, while women, especially breast cancer patients, more often articulated internalised self-blame shaped by gendered expectations.
The Treatment Effect Paradox: Life-saving yet damaging
This paradox captures patients’ ambivalence towards cancer treatment, particularly chemotherapy. Treatments were perceived both as essential to survival and as sources of intense physical and emotional suffering.
Chemotherapy as a necessity—“It saved my life”
Many participants acknowledged that without treatment, their survival chances would have been minimal. They recognised the life-preserving value of medical interventions, even when they were accompanied by discomfort.
“My doctor said I’d die without chemo. So I endured it. . . It gave me time.” (Male, 66, Stage III colorectal cancer, State Hospital) “Chemo saved me. That’s how I got to see my daughter graduate” (Female, 51, Stage II breast cancer, University Hospital)
These accounts reflect high perceived benefit and “treatment control,” a key element of Leventhal’s model. Patients accepted harsh side effects as the cost of survival.
Chemotherapy as destruction –“It took away everything”
Simultaneously, participants described treatment as physically debilitating and identity-shattering. Chemotherapy was associated with loss of hair, strength, femininity, sexuality, or personhood.
“They gave me poison. My nails fell off, my skin peeled, my soul left.” (Female, 48, Stage II gastric cancer, Public Hospital) “I didn’t see myself in the mirror. I was bald, weak, a ghost.” (Female, 43, Stage III breast cancer, Private Hospital)
These vivid metaphors underscore how treatments, while medically effective, often violate patients’ sense of control and self. The emotional representation domain of the CSM is especially activated here, revealing the depth of psychological trauma.
Ambivalence towards care providers
Some patients even described feelings of resentment towards oncologists or nurses who administered treatments that caused them pain-even while trusting them medically.
“I love my doctor, but I also hate going to that hospital every time. It was like walking into hell smiling.” (Female, 57, Stage II colorectal cancer, University Hospital)
This paradox underscores the importance of healthcare providers being attuned to patients’ complex and often conflicting emotional states regarding treatment. Shared decision-making and anticipatory guidance can help restore a sense of agency. Treatment, Control, and Consequences are appraised alongside intense Emotional Representation; the perceived Timeline (acute vs enduring effects) shapes meaning. Those in active treatment stressed exhaustion and loss of control; survivors retrospectively emphasised life-extension and meaning-making.
The Paradox Of Influencing Life: Destroying yet transformative
The final paradox involves the overall impact of cancer on life trajectories and identities. While cancer disrupted careers, relationships, and futures, some participants also reported personal growth, emotional awakening, and existential clarity.
Disruption and devastation—“My life stopped”
Participants spoke of cancer as an intruder that derailed their lives. This disruption included financial loss, interrupted parenting roles, and existential shock.
“I had plans, dreams, work. Cancer erased all of it in a day.” (Male, 46, Stage III lung cancer, State Hospital) “Everything changed: I became dependent, isolated, and tired of fighting” (Female, 60, Stage IV breast cancer, Public Hospital)
These descriptions activate the “consequence” and “timeline” elements of the CSM, painting cancer as a long-term, all-encompassing event rather than a discrete illness.
Existential awakening—“It gave me a new life”
In contrast, others described cancer as a catalyst for profound personal transformation. Many adopted a new appreciation for life, simplified their priorities, or deepened their spirituality.
“Before cancer, I ran after everything. Now, I enjoy the smallest things.” (Female, 49, Stage I breast cancer, Private Hospital) “It showed me who really loves me. I’m not the same woman anymore.” (Female, 53, Stage II gastric cancer, Public Hospital)
This growth-through-adversity narrative aligns with the concept of “post-traumatic growth” and suggests that illness representations are not always maladaptive. Some patients construct meaning that fosters psychological resilience.
Tension between destruction and renewal
Many participants held both perspectives simultaneously-grieving what cancer had taken while appreciating what it revealed.
“Yes, I lost things. But I also found my soul. I’m broken and reborn at the same time.” (Female, 45, Stage II breast cancer, Private Hospital)
This final paradox highlights that illness representations are not merely cognitive schemas, but rather dynamic, emotionally rich, and narrative-based identity projects. Identity, Consequences, and Coherence (sense-making) are engaged as patients reconstruct life narratives over an extended Timeline. Women (particularly breast cancer) more frequently voiced identity and body-image reconstruction; men more often emphasised ro le disruption experiences
Summary of findings
These four paradoxes-ordinary yet deadly, random yet deserved, life-saving yet damaging, and destroying yet transformative-reveal the complexity and multidimensionality of cancer illness perceptions. By embedding patients’ voices within a structured framework (CSM), we show that meaning-making is nonlinear, contradictory, and often ambivalent. Recognising and addressing these paradoxes may support interventions aimed at improving patient adjustment, adherence, and quality of life. These four labels are retained in the Conclusion to ensure section-to-section consistency and to foreground paradox as the overarching interpretive lens.
Discussion
This qualitative study explored cancer patients’ illness perceptions and identified four overarching paradoxes: (1) The Illness Description Paradox, (2) The Disease Cause Paradox, (3) The Treatment Effect Paradox, and (4) The Paradox of Influencing Life. These paradoxes represent conflicting cognitive and emotional representations that patients hold simultaneously. Drawing on Leventhal’s Common-Sense Model (CSM), the findings demonstrate that patients’ perceptions are shaped across key dimensions-identity, cause, timeline, controllability, consequence, and emotional representation. We explicitly articulate how each paradox reflects simultaneous activation of multiple CSM dimensions rather than a linear progression within any single domain (Cameron and Leventhal, 2012; Diefenbach and Leventhal, 1996; Hagger et al., 2017; Leventhal et al., 1980). This dynamic interplay supports prior evidence that illness perceptions are self-regulatory and emotionally driven constructs influencing both distress and adaptation (Petrie et al., 2008).
These paradoxes capture the tensions individuals face when making sense of a chronic, life-threatening illness amid social, emotional, and medical realities. They emphasise how culturally embedded beliefs and personal experiences shape illness representations (Hagger et al., 2017; Hopman and Rijken, 2015). Consistent with Alaloul et al. (2025), perceived stigma and societal fatalism can intensify distress and hinder adaptive coping, underscoring the cultural context’s role in meaning-making
The Illness Description Paradox showed that patients viewed cancer both as an ordinary, manageable condition and as a deadly, uncontrollable disease. Those normalising cancer, especially with early-stage diagnoses or private care access, described it as “a normal cold” or “quite ordinary.” This mirrors Robb et al. (2014), who found that exposure to survivorship narratives and medical advances fostered normalisation of cancer as chronic. Such reappraisal parallels identity reconstruction seen in mental illness recovery (Soundy et al., 2015) and in Turkish women minimising illness to lessen psychological burden (Günüşen et al., 2013). Conceptually, this paradox illustrates that “identity” and “consequences” are flexibly negotiated, while “timeline” oscillates between acute threat and chronic vigilance (Johansson et al., 2018; Leventhal et al., 1980).
Participants with advanced-stage disease or treatment failure described cancer as a “deadly illness” or “a threat that never ends.” Fear of recurrence persisted even in remission, consistent with Simard et al. (2013), who found sustained recurrence fear among survivors with poor prognoses. Within the CSM, this reflects an emotional representation and a cyclical timeline, rather than a linear recovery (Hagger et al., 2017).
The Disease Cause Paradox captured attributions of cancer to either random misfortune or personal behaviours such as smoking or emotional suppression. Bashiri-Nejadian et al. (2021) similarly linked emotional ambivalence and fatigue to self-blame and poor adherence, mirroring the internalised causal attributions of our participants. Some expressed existential questioning (“Why me?”), while others accepted responsibility (“I caused this”), aligning with the “cause” and “control” dimensions of the CSM (Diefenbach and Leventhal, 1996; Hagger et al., 2017). Hajian et al. (2015) also found that Iranian women attributed illness to God’s will or emotional restraint, leading to spiritual resignation. Our findings revealed gendered patterns of causality externalisation among men and internalised blame among women, highlighting how cultural scripts intersect with CSM appraisals (Hopman and Rijken, 2015; Wang et al., 2024).
The Treatment Effect Paradox reflected ambivalence towards chemotherapy and radiation. Treatments were described as lifesaving (“Chemo saved me”) yet dehumanising (“I was a ghost”). This duality echoes identity disruption in other chronic illnesses (Higbed and Fox, 2010) and engages the “treatment control” and “emotional representation” domains of the CSM (Broadbent et al., 2015; Hagger et al., 2017). Petrie et al. (2008) similarly argued that subjective illness representations—more than disease type—shape emotional adjustment. Our findings extend this by showing how paradoxical perceptions (e.g. “life-saving yet exhausting”) help preserve coherence in the face of uncertainty. Holding contradictory beliefs, such as hope and despair, may function as a resilience mechanism (Soundy et al., 2015).
Browall et al. (2018) reported that chemotherapy side effects disrupted identity and femininity, parallelling participants’ experiences of treatment as both necessary and identity-threatening. Conversely, Seiler and Jenewein (2019) found that resilience and meaning-focused interventions foster adaptive adjustment, suggesting that anticipatory guidance and shared decision-making may buffer emotional distress while supporting treatment control (Mehnert-Theuerkauf et al., 2023; Vehling and Philipp, 2018). Participants also voiced ambivalence towards healthcare providers, simultaneously trusting doctors yet resenting treatment-induced suffering. Czerw et al. (2020) also demonstrated that perceptions of treatment outcomes influence trust and adherence, highlighting the importance of empathetic, validating communication (Gottlieb and Bergen, 2010).
The Paradox of Influencing Life revealed that cancer was both life-disrupting and transformative. Participants described loss of function and independence (“My life stopped”) alongside emotional growth and new meaning (“It gave me a new life”). Prior studies confirm that posttraumatic growth and meaning-making are central to reconstructing life narratives after cancer (Park et al., 2008; Seiler and Jenewein, 2019; Tedeschi and Calhoun, 2004). In our data, those embracing a growth narrative integrated illness more adaptively. This paradox illustrates how the “consequence” and “identity” domains of the CSM evolve dynamically—shattering some life stories while offering others the chance to reauthor them (Bury, 1982; Vehling and Philipp, 2018).
Subgroup variations enriched the understanding of each paradox. Patients with early-stage or curative cancers more often described cancer as “ordinary” or “manageable,” whereas those with advanced disease framed it as “ordinary yet deadly,” reflecting heightened existential fear (Lester et al., 2006; The Lancet Oncology, 2016). Gendered differences also emerged: women tended to internalise blame, linking illness to emotional suppression, while men emphasised external causes such as fate or heredity. Participants in active treatment expressed greater ambivalence towards chemotherapy-both life-saving and identity-threatening—whereas post-treatment survivors emphasised transformation and renewal. These nuances suggest that paradoxical illness representations emerge from the intersection of clinical, cultural, and psychosocial factors, rather than a uniform experience (Hopman and Rijken, 2015; Johansson et al., 2018; Wang et al., 2024).
Conceptually, framing illness perceptions as paradox shows that CSM dimensions are dynamic, coexisting meanings rather than linear endpoints. Ambivalence represents an adaptive cognitive–emotional process through which patients sustain contradictory beliefs-hope and despair, control and helplessness-to manage uncertainty. This reframing extends the CSM by emphasising dialectical rather than unidimensional representation patterns (Cameron and Leventhal, 2012; Hagger et al., 2017). Early-stage participants emphasised normalisation, advanced-stage participants highlighted lethality and loss of control, and post-treatment survivors described transformation and meaning-making (Park et al., 2008; Tedeschi and Calhoun, 2004; Vehling and Philipp, 2018).
Limitations
This study has several limitations that should be acknowledged. First, the findings are based on participants recruited from six hospitals in two major cities in Turkey; therefore, the results may not fully capture the experiences of patients from more rural or socioeconomically disadvantaged regions. Second, although purposive sampling ensured variation across cancer types and illness stages, the relatively small sample size (n = 35) limits the generalisability of the findings. However, generalisation is not the primary aim of qualitative research. Third, focus group dynamics might have influenced participants’ willingness to disclose sensitive experiences, particularly for those with more introverted personalities or those in vulnerable disease stages. Future studies might purposively sample across clinical subgroups (e.g. stage, treatment phase, gender) to compare paradox configurations more systematically.
Despite the researchers’ efforts to create a comfortable and respectful environment, some participants may have engaged in impression management or withheld contradictory views. Due to the cultural context and language-specific nuances, the translation of quotations into English may have resulted in a partial loss of meaning. To mitigate this, a bilingual qualitative expert reviewed the translations for fidelity and contextual integrity. Finally, as with all reflexive thematic analysis, the researcher’s interpretation plays a role in shaping the findings. We addressed this issue through researcher triangulation, peer debriefing, and memo writing; however, subjectivity cannot be entirely eliminated.
Implications for practice and policy
The findings of this study provide several implications for clinical practice, psychosocial care, and policy-making in oncology.
First, clinicians and nurses must be aware of the paradoxical ways patients perceive their illness, as these interpretations influence treatment decisions, emotional well-being, and coping strategies. For example, if cancer is perceived as “ordinary,” patients may delay emotional engagement with their disease; conversely, viewing it as a “death sentence” may exacerbate anxiety and hinder adaptation. This underscores the need for individualised communication that explores patients’ meaning-making processes beyond diagnosis and prognosis.
Second, healthcare professionals should integrate illness perception assessments into routine psychosocial evaluations. The development or adaptation of culturally appropriate screening tools to capture illness beliefs in Turkish cancer populations could help tailor supportive interventions. These tools could help identify patients who might benefit from targeted psychological support or narrative-based interventions that address maladaptive perceptions.
Third, the paradoxes identified in this study highlight the need for effective communication training among healthcare professionals. Training programmes should incorporate modules on how to identify and respond to contradictory patient narratives with empathy, while avoiding invalidation of their experiences. This could improve trust, adherence, and patient satisfaction.
Fourth, from a policy perspective, our results suggest the importance of national psychosocial oncology guidelines that acknowledge the cultural and cognitive complexity of illness perceptions. In particular, educational campaigns that address the stigma and blame often associated with cancer, especially regarding causality, can reduce internalised guilt and facilitate help-seeking behaviours.
Finally, nursing education programmes should incorporate content on illness representations, especially through the lens of the Common-Sense Model. By understanding how patients interpret and emotionally respond to cancer, nurses can provide more effective support for adaptive coping and enhance quality of life outcomes. Embedding “paradox recognition” (e.g. screening prompts for simultaneous opposing beliefs) into routine care pathways may help clinicians validate ambivalence, preserve agency, and tailor supportive care across clinical subgroups.
Conclusion
This study explored cancer patients’ illness perceptions through a descriptive qualitative approach and identified four central paradoxes that shape how they make sense of their disease. These paradoxes-ordinary versus deadly, random versus self-blaming, life-saving versus damaging, and destroying versus transformative-reflect the complex and sometimes contradictory meanings patients attach to cancer. Such perceptions are not static; they evolve through personal, relational, cultural, and clinical interactions.
By employing Leventhal’s Common-Sense Model as a theoretical lens, this study highlights the dynamic tension between patients’ cognitive and emotional representations of illness. This conceptual framing provides insight into the way illness perceptions shape patients’ behaviours, affective responses, and help-seeking decisions.
The findings suggest that interventions should address, rather than resolve, these paradoxical tensions. Practical applications may include the development of a brief CSM-based screening tool to assess patients’ illness perceptions, as well as the integration of short narrative-based interventions within oncology nursing care to promote meaning-making and emotional regulation. The paradoxes uncovered point to a need for clinicians and policymakers to recognise that cancer is experienced not as a linear or singular narrative, but as a multifaceted and evolving process of meaning-making. Acknowledging these layered and ambivalent perceptions may foster more compassionate, culturally sensitive, and patient-centred care.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251404345 – Supplemental material for “It’s just a flu or a death sentence”: A descriptive qualitative study on illness perceptions of cancer patients across four paradoxes
Supplemental material, sj-docx-1-hpq-10.1177_13591053251404345 for “It’s just a flu or a death sentence”: A descriptive qualitative study on illness perceptions of cancer patients across four paradoxes by Perihan Guner, Figen Inci, Nazmiye Yildirim, Aycan Kucukkaya and Polat Goktas in Journal of Health Psychology
Footnotes
Acknowledgements
We would like to thank the healthcare professionals who participated in this study. No part of the data analysis, coding, or interpretation was conducted using AI tools.
Ethical considerations
The protocol for this study was approved by the Koç University Ethics Committee, ensuring adherence to ethical standards for research involving human subjects. Approval was granted via a letter under the reference code 2016.155.IRB3.086.
Consent to participate
All participants provided voluntary consent to participate in the research.
Consent for publication
Participants gave their consent for the anonymised data to be published as part of this study.
Author contributions
Perihan Guner: Conceptualisation, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing—Original Draft, Writing—review and editing. Figen Inci: Conceptualisation, Data curation, Formal analysis, Investigation, Methodology, Resources, Writing—Original Draft. Nazmiye Yildirim: Conceptualisation, Data curation, Formal analysis, Investigation, Methodology, Resources, Writing—Original Draft. Aycan Kucukkaya: Data Curation, Formal analysis, Investigation, Methodology, Resources, Software, Validation, Visualisation, Writing—Original Draft, Writing—Review & Editing; Polat Goktas: Data Curation, Formal analysis, Investigation, Methodology, Software, Visualisation, Writing—Original Draft, Writing—review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Vehbi Koç Foundation Nursing Fund in Istanbul, Turkey (Grant number [2017.2.22]). This sponsor had no role in the study design, collection, analysis, and interpretation of data, writing of the report, and the decision to submit the article for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting this study’s findings are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.