
Abstract
While health-related awareness has been extensively studied, the concept of health uncertainty in the general population remains inadequately conceptualized and operationalized. This study aims to develop a conceptual framework and measurement tool for health uncertainty, and to examine its associations with health anxiety and health behaviors. The research comprised two studies conducted in China. Study 1 developed and validated a health uncertainty scale using data from 709 participants. The scale, which comprises dimensions of health status uncertainty, health changes unpredictability, and health threat and information ambiguity, demonstrated good reliability and validity. Study 2 employed a questionnaire-based approach with 345 participants and showed that health uncertainty negatively predicted health behaviors, with health anxiety acting as a mediator. The findings highlight the impact of health uncertainty on psychological and behavioral responses, emphasizing the need for strategies to reduce uncertainty during public health crises to promote healthier behaviors and achieve public health goals.
Keywords
Introduction
Public health emergencies, such as the COVID-19 pandemic, have revealed complex and elusive health threats. Factors like infection risk, health-related anxiety, misinformation, and conspiracy theories significantly amplify uncertainty about individual health (Akbari et al., 2021; Farias and Pilati, 2023). However, the pandemic did not create this phenomenon; it intensified a form of uncertainty people encounter every day. While everyday experiences frequently engender a degree of health uncertainty, the concept itself lacks a standardized definition. Researchers have extensively examined and developed related constructs, such as illness uncertainty (Mishel, 1990; Wright et al., 2009; Zhang, 2017), patient uncertainty (LaNoue et al., 2020) and uncertainty in healthcare (Han et al., 2019; Simonovic et al., 2023). However, this body of research has predominantly focused on patients with chronic diseases (Landis, 2009; Mullins et al., 2017; Wright et al., 2009), their family members (Gold-Spink et al., 2000), and family caregivers (Im et al., 2019), without extending to the broader population. These observations highlight a critical gap in understanding how health uncertainty affects the emotional, cognitive, and behavioral responses of the general population. In response, the present study aims to conceptualize and measure health uncertainty and examine its psychological and behavioral consequences, particularly its associations with health anxiety and general health behaviors.
This study defines health uncertainty as an individual’s limited capacity to accurately understand and predict their own health status, including difficulties in anticipating and managing changes or developments in their health. Health uncertainty shares conceptual similarities with related constructs but also exhibits important distinctions. Like other well-studied forms of health-related uncertainty, such as illness uncertainty (Mishel, 1990) and healthcare uncertainty (Han et al., 2019), they all involve perceptions of ambiguity or unpredictability. However, these constructs differ primarily in their target populations. Another related concept is health consciousness (Gould, 1990), which also involves a general attentiveness to health. However, health consciousness stems from self-consciousness as a personality trait and emphasizes awareness, attention, and reflection concerning one’s health. It captures the degree to which individuals focus on health-related issues. In contrast, uncertainty centers on the recognition of unknowns and unpredictability (Hogg, 2007). Furthermore, health uncertainty should be distinguished from the emotional responses it may elicit, such as health anxiety. Uncertainty refers to a cognitive state arising from insufficient information or an inability to foresee outcomes, which can lead to emotional reactions like anxiety or fear (Morriss et al., 2022). These emotional responses, while triggered by uncertainty, are distinct from the cognitive state itself; they reflect individuals’ subjective experiences and may influence how uncertainty is perceived and managed (Heilman et al., 2010).
Following the conceptual clarification of health uncertainty, its structural framework emerges as a critical issue. Given that the Illness Uncertainty Theory (Mishel, 1990) represents a well-established conceptual framework, we draw on this theoretical model to inform the dimensional construction of health uncertainty. The Illness Uncertainty Theory focuses on patients with various diseases and categorizes illness uncertainty into four dimensions: Ambiguity, Complexity, Inconsistency, and Unpredictability (Mishel, 1990). This framework explores challenges in understanding medical diagnoses, the complexity of treatment and care procedures, the lack of information regarding symptoms and disease severity, and the unpredictability of illness progression (e.g. an unpredictable prognosis). Among the original dimensions, this study adapted Ambiguity and Unpredictability to fit general health contexts, reframing them as the ambiguity of health information and the unpredictability of health changes. We regarded the dimensions of Complexity and Inconsistency as less applicable, given the general knowledge about one’s health and the absence of direct medical treatment. Because uncertainty involves individuals’ subjective evaluations of an unclear state in everyday life (van Den Bos, 2001), we introduced the dimension of Health Status Uncertainty to capture individuals’ awareness and judgment regarding their own health. Furthermore, health uncertainty often arises in the context of public health crises, driven by contagious viruses and various unknown health threats being major contributors to this uncertainty (Pappas et al., 2009). Thus, we also included the dimension of health threat perception. In summary, we adapted the illness uncertainty framework to include Health Status Uncertainty and Health Threat Perception, alongside the existing dimensions of Health Information Ambiguity and Health Changes Unpredictability, to fully encapsulate the facets of health uncertainty in the general population.
Following the definition of health uncertainty, it becomes essential to explore its relationship with health behaviors. Health behaviors are protective actions aimed at safeguarding individual health and are habits that promote well-being (Duffy, 1986), such as keeping a regular routine, eating a balanced diet, and exercising (Hu et al., 2022). While the role of uncertainty in health decisions is often overlooked, it is a critical factor influencing these behaviors (Berrigan et al., 2023). The relationship between health uncertainty and health behaviors appears complex and multifaceted.
On one hand, factors triggering health uncertainty can promote health behaviors. Protection Motivation Theory (PMT; Floyd et al., 2000; Prentice-Dunn and Rogers, 1986) posits that individuals who perceive a severe threat and believe in effective coping strategies are more likely to develop strong protective motivation and adopt corresponding protective behaviors. Studies suggest that heightened awareness of health risks can prompt proactive health actions and healthier lifestyle (Mozgovaya et al., 2021). Moreover, during the COVID-19 pandemic, some individuals improved their diets and exercise routines, with one study noting a 25% increase in positive health behaviors (Delgado-Ortiz et al., 2023).
On the other hand, substantial evidence suggests that health uncertainty might negatively influence health behaviors. Ongoing concern about health uncertainty can negatively affect emotional well-being (Howell et al., 2023; van Den Bos, 2001). Stress and anxiety triggered by uncertainty may lead to avoidance and poor health choices. Research on illness uncertainty shows that heightened perceptions of vulnerability and severity of potential illnesses reduce engagement in health-promoting behaviors (e.g. exercising, maintaining a healthy diet), delays in prescription refills, and a greater tendency to cancel or postpone clinic visits (Chiu et al., 2021; Giovannetti et al., 2017; Orom et al., 2020). These perceptions are also associated with poorer psychological adjustment (Skojec et al., 2025). Uncertainty Management Theory further suggests that facing uncertainty reduces perceived control, prompting individuals to manage it through strategies such as seeking or avoiding information and regulating emotions (Hogg, 2007). Studies have found that individuals also manage uncertainty by engaging in passive or avoidant behaviors (Steptoe and Wardle, 2001; Van Den Bos et al., 2007). From an intertemporal decision-making perspective, individuals facing uncertainty may prioritize immediate gratification, such as overeating, staying up late, smoking, or substance use, over long-term health benefits (Ahlbrecht and Weber, 1997; Anderson and Stafford, 2009). Maintaining health behaviors for long-term well-being requires delaying such gratification, which can be especially challenging under conditions of health uncertainty. As a result, individuals may be more inclined to choose immediate gratification behaviors that ultimately compromise their long-term health. Therefore, this study proposes
Adding further complexity to this relationship is the role of emotional mechanisms, particularly health anxiety. A considerable body of research has suggested that uncertainty can trigger a range of negative emotions, with anxiety being one significant emotional response that drives subsequent behaviors (Hogg, 2007). Health anxiety refers to excessive or inappropriate worry about one’s health or the possibility of having a serious illness, often based on misinterpretation of bodily sensations (Alberts et al., 2011). Elevated health anxiety, particularly noted during public health crises, can severely disrupt normal health behaviors, leading to avoidance and maladaptive coping strategies (Dattilo et al., 2021; Tan, 2023; Wu et al., 2021). For instance, uncertainty may contribute to post-traumatic stress symptoms in children and adolescents, disrupting their engagement in health-promoting behaviors (Lee et al., 2009). Individuals with high health anxiety tend to focus on physical symptoms, worry excessively, and adopt avoidance coping strategies, which in turn reinforce anxiety and impair coping (Horenstein and Heimberg, 2020; Mogg and Bradley, 2016). Moreover, generalized anxiety correlates with increased alcohol and substance use and inactive lifestyles (Mason et al., 2019; Strine et al., 2005), and health anxiety similarly associates with poor lifestyle choices (Tang et al., 2024). These findings suggest that health anxiety may act as a psychological mediator between health uncertainty and health behaviors. Therefore, this study proposes
To test the above hypotheses, we designed two sub-studies. First, the study developed and evaluated a health uncertainty questionnaire for reliability and validity. Subsequently, the study examined the association between health uncertainty and health behaviors, with particular attention to the mediating role of health anxiety.
Study 1: Development of the health uncertainty scale
This study aimed to develop a health uncertainty questionnaire. We administered the initial version of the questionnaire, collected data for evaluation and revision, and ultimately produced a standardized Health Uncertainty Questionnaire.
Materials and methods
Ethical statement
The study protocol received ethical approval from the Psychology Academic Ethics Committee of the first authors’ affiliated institution on December 26, 2022. Participants voluntarily took part in the study. Before completing the questionnaire, we provided participants with detailed information about the study, which was prominently displayed on the questionnaire. For online questionnaires, we considered submission as providing informed consent; for offline questionnaires, we obtained oral consent from the participants. Throughout the process, participants could withdraw from the study at any time. All data were collected, sorted, and analyzed anonymously, without any identifiable personal information.
Participants
This study conducted a total of three rounds of testing. The questionnaire was administered in Chinese, and data were collected via WJX (https://www.wjx.cn/), a widely used online survey platform in China. Pilot testing involved 51 participants to evaluate the clarity and reasonableness of the items’ wording. Sample 1, consisting of 356 participants, served for exploratory factor analysis and item analysis. The participants’ average age was M = 23.34, SD = 1.85, comprising 153 males (43.0%) and 203 females (57.0%). Sample 2, with 302 participants, served for confirmatory factor analysis and assess internal consistency reliability testing. The participants’ average age was M = 21.16, SD = 1.77, comprising 116 males (38.4%) and 186 females (61.6%).
Questionnaire development process
First, conceptualizing
We conducted literature analysis, focus group evaluations (See Supplemental Materials for details), and open-ended consultations with four experts. All the experts hold doctoral degrees and specialize in clinical psychology or public health. We asked them about their understanding of health uncertainty, its components, distinctions from and overlaps with related health constructs, and the theoretical inferences connecting these concepts. Based on these processes, we operationally defined health uncertainty and identified its four dimensions: health status uncertainty, health threat perception, health information ambiguity, and health changes unpredictability.
Second, draft initial questions
Based on the operational definition, we developed an initial questionnaire with 35 items. We adapted items from the Mishel Uncertainty in Illness Scale–Adult (Mishel, 1990), and added additional items to reflect the conceptualization of newly proposed dimensions. The dimensions included 9 items each for health status uncertainty, health threat perception, and health information ambiguity, while the dimension health changes unpredictability included 8 items. Responses were scored on a 5-point Likert scale.
Third, content validity assessment
Ten experts evaluated the relevance of the initial questionnaire items to the concept of health uncertainty, and the Content Validity Index (CVI) was calculated accordingly. All experts held expertise in health psychology or social psychology, were familiar with the research topic, and either held a doctoral degree in psychology or were current PhD candidates. The experts first reviewed a definition of health uncertainty and its conceptual dimensions, and then assessed the relevance of each item to the construct using a 4-point Likert scale (1 = Not Relevant, 2 = Somewhat Relevant, 3 = Moderately Relevant, 4 = Highly Relevant). In addition, they provided open-ended feedback on item wording clarity and suggestions for improvement.
Fourth, pilot testing
We used the test sample for preliminary testing to gather feedback on items wording. Each participant evaluated whether the phrasing of each item was reasonable and easy to understand, and we modified items based on their feedback. Additionally, we recorded response times as a criterion for evaluating the validity of the online questionnaire.
Fifth, revise the questionnaire
We conducted exploratory factor analysis with Sample 1 to extract the dimensions of the questionnaire and removed items with factor loadings below the standard threshold. We then analyzed item-total correlations and discarded items that did not meet the criteria.
Finally, validity and reliability testing
We tested the questionnaire for construct validity using confirmatory factor analysis with Sample 2. We also calculated the internal consistency reliability of each dimension and the overall scale.
Statistical methods
We conducted exploratory factor analysis, item analysis, and internal consistency testing using SPSS 26.0, and performed confirmatory factor analysis using Mplus 8.0.
Results and discussion
Content validity
We assessed content validity using both the Item-Content Validity Index (I-CVI) and the Scale-Content Validity Index (S-CVI). The I-CVI represents the proportion of experts who rated an item as “3-Moderately Relevant” or “4-Highly Relevant.” We calculated the S-CVI as the average of all I-CVI values across the scale. I-CVI values ⩾ 0.78 (when the number of experts ⩾5) and S-CVI values ⩾ 0.80 indicate acceptable content validity (Almanasreh et al., 2019).
Among all the items, only a few received a rating of “2-Somewhat Relevant” from individual experts, and no item received a rating of “1-Not Relevant.” The I-CVI values ranged from 0.80 to 1.00, and the average S-CVI (S-CVI/Ave) was 0.92. These results meet the recommended thresholds, indicating that the items of the initial questionnaire adequately reflect the construct of health uncertainty and demonstrate good content validity.
Exploratory factor analysis
We performed exploratory factor analysis on 35 items using principal component analysis. We excluded items with factor loadings below 0.4, items exhibiting cross-loadings, and items that failed to cluster into any factor (DeVellis and Thorpe, 2021), yielding a final set of 17 items. The refined health uncertainty scale revealed three distinct factors, which collectively accounted for 56.23% of the total variance. Factor 1 had an eigenvalue of 6.87 and explained 40.43% of the variance, Factor 2 had an eigenvalue of 1.51 and explained 8.89%, while Factor 3 had an eigenvalue of 1.18 and explained 6.91%. Table 1 presents the factor loadings for each item.
Factor loadings for each item in the health uncertainty scale.
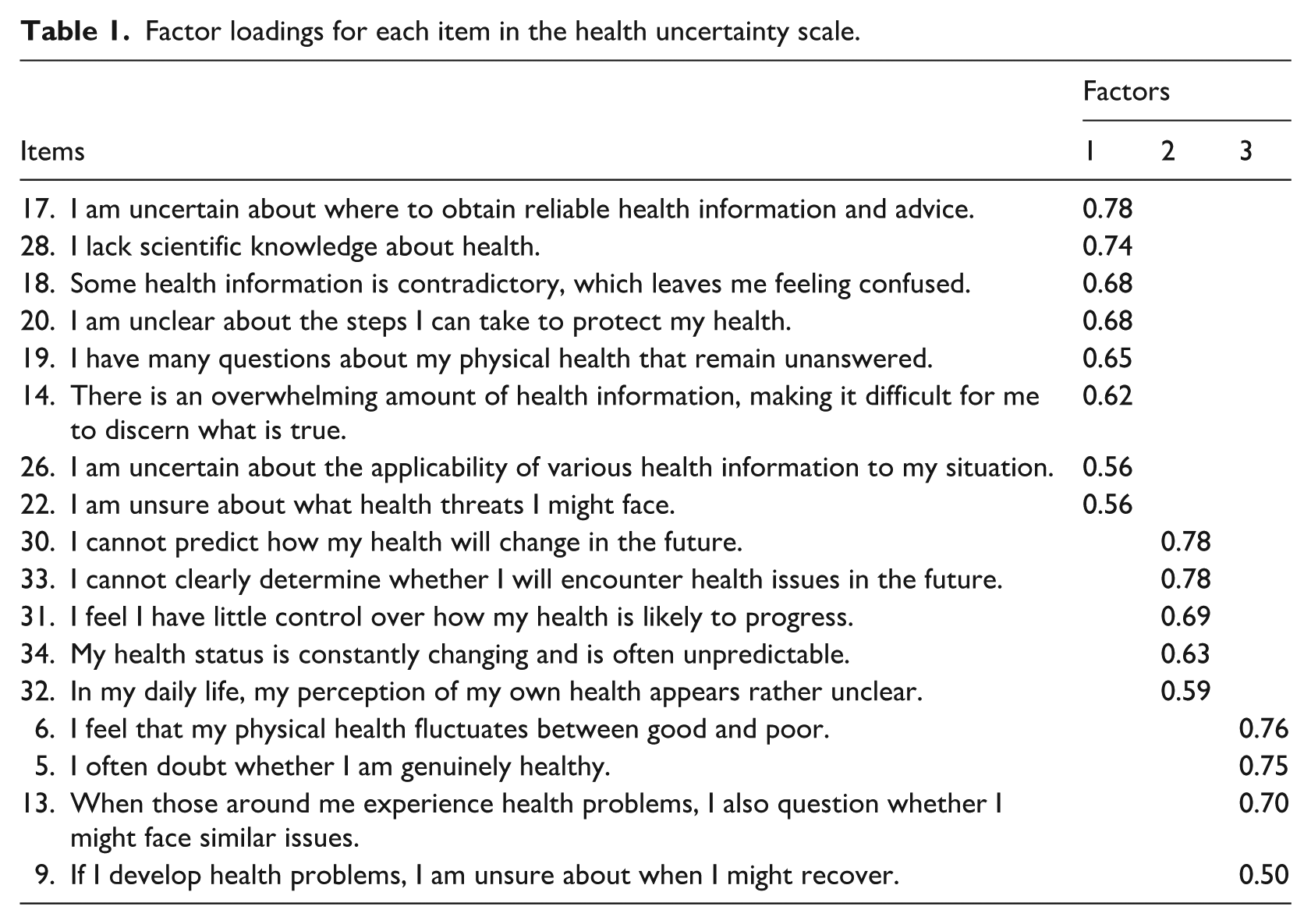
EFA revealed considerable overlap between the health threat perception and health information ambiguity dimensions, grouping them into Factor 1. This overlap, resulting from their similar manifestations, prompted the decision to merge them into a single dimension. Consequently, three dimensions remained: (1) Health status uncertainty (individuals expressing uncertainty about their health status); (2) Health threat and information ambiguity (individuals feeling uncertain about the sources and accuracy of information regarding health threats and healthcare knowledge); and (3) Health changes unpredictability (individuals expressing uncertainty about the future development of their physical health).
Item analysis
We conducted an item analysis based on total item correlation using data from Sample 1 to enhance the representativeness and reliability of the items in the final scale. Following the criterion of retaining items with correlation coefficients of ⩾0.4 with their corresponding dimensions (DeVellis and Thorpe, 2021), the analysis revealed that only Item 28 (r = 0.349) did not meet this standard. The remaining items exhibited correlation coefficients ranging from 0.45 to 0.81 with their respective dimensions. Consequently, we eliminated Item 28, resulting in a final selection of 16 items.
Confirmatory factor analysis
To test the structural validity of the health uncertainty scale, we conducted confirmatory factor analysis using Sample 2, which indicated good model fit: χ2/df = 2.84, RMSEA = 0.078, CFI = 0.945, TLI = 0.935, SRMR = 0.041, all of which meet established statistical criteria (Thompson, 2004). Figure 1 illustrates the model structure.
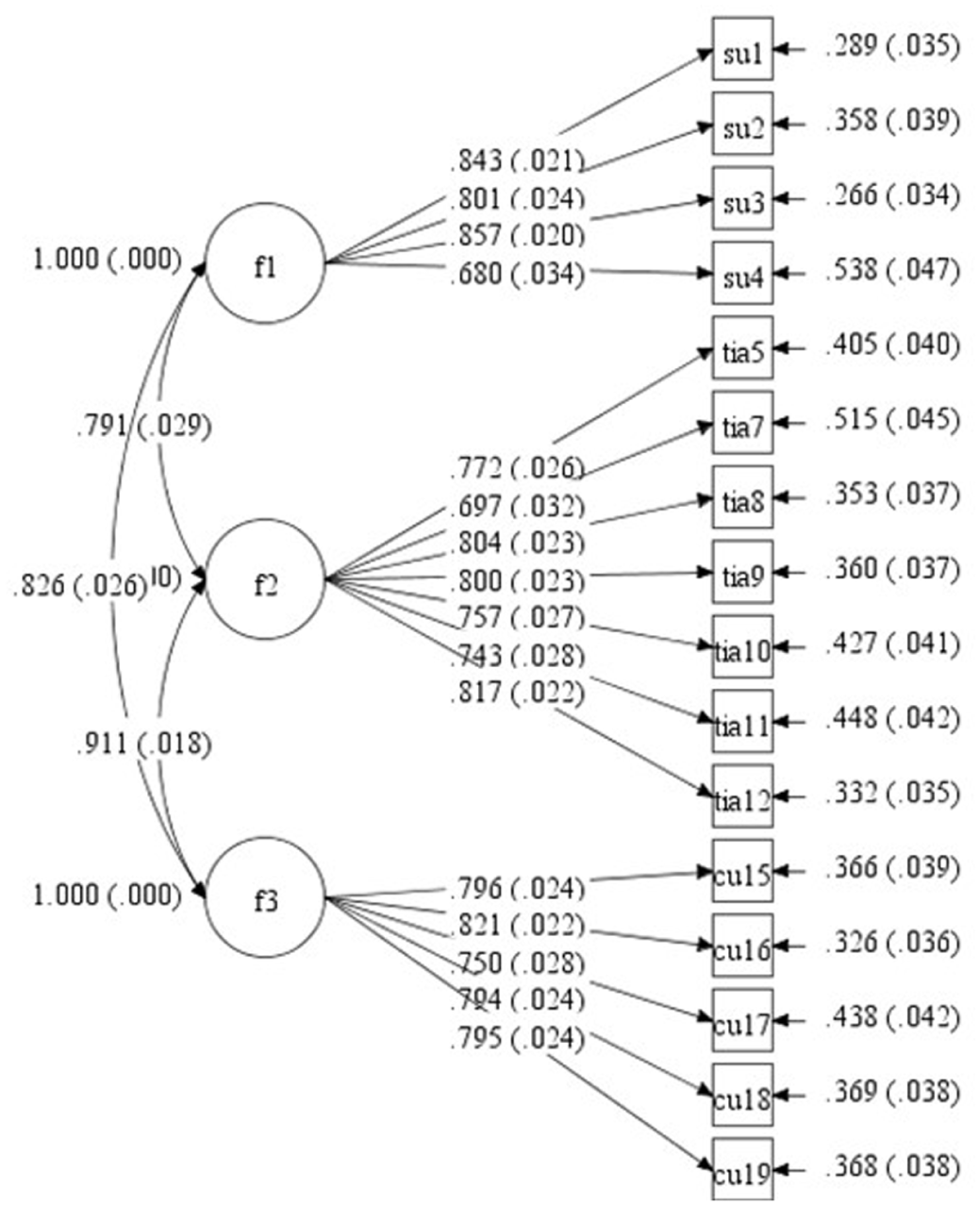
Three-factor structure diagram of the health uncertainty scale.
Internal consistency reliability
We assessed internal consistency for the Health Uncertainty Scale and its dimensions was assessed using Cronbach’s α coefficients based on data from Sample 2. The results indicated Cronbach’s α values of 0.86 for the dimension of health threat and information ambiguity, 0.79 for the health changes unpredictability, and 0.75 for the health status uncertainty. The overall scale demonstrated a Cronbach’s α of 0.90. A Cronbach’s α between 0.7 and 0.9 indicates good reliability (Guilford, 1956), confirming the high internal consistency of the questionnaire.
Study 2: Examination of the mediating model among health uncertainty, health anxiety, and health behaviors
This study utilizes a questionnaire approach to investigate the relationship between individuals’ health uncertainty and health behaviors, and to analyze the mediating role of health anxiety.
Materials and methods
Ethical statement
Study 2 followed the same ethical approval and informed consent procedures as Study 1.
Participants
We recruited participants using a random sampling method within China through both online (via https://www.wjx.cn , the most used online testing platform in China) and offline channels, with the offline participants drawn from a psychology-related undergraduate course. A total of 381 questionnaires were distributed, with 345 returned, resulting in an effective response rate of 90.55%. The average age of the participants was M = 23.33, SD = 1.85, comprising 147 males (42.6%) and 198 females (57.4%).
Materials
Health uncertainty We used the Health Uncertainty Scale developed in Study 1. The scale consists of three dimensions and a total of 16 items, responses were scored on a 5-point Likert scale, ranging from 1 (“Strongly Disagree”) to 5 (“Strongly Agree”), with higher scores indicating a higher level of health uncertainty.
Health behaviors We used the Healthy Lifestyle Questionnaire (HLQ) developed by Wang (2009). This scale comprises eight dimensions: exercise behavior, regular behavior, dietary and nutritional behavior, health risk behavior, health responsibility behavior, interpersonal support behavior, stress management behavior, and appreciation of life. The first five dimensions represent explicit health behaviors, while the last three reflect implicit health behaviors. Given that this study primarily focuses on explicit behavioral patterns, we administered only the first five dimensions, which include 22 items. A sample item is “Do you eat your three meals at regular times every day?” Responses were scored on a 5-point Likert scale, ranging from 1 (“Never”) to 5 (“Always”). The health risk behavior dimension was reverse-scored before being incorporated into the total score, with higher total scores indicating a higher level of health behaviors. The Cronbach’s α coefficient for the health behaviors scale in this study was 0.769.
Health anxiety We used the China Short Health Anxiety Inventory (CSHAI) developed by Zhang et al. (2015). This scale consists of 18 items. A sample item is “I feel worried about my health.” Responses were scored on a 4-point Likert scale, ranging from 1 (“Never”) to 4 (“Always”), with higher scores indicating a higher level of health anxiety. The Cronbach’s α coefficient for this scale in this study was 0.82.
Results
Common method bias test
Since participants self-reported the data in this study, there is a potential risk of common method bias. To address this issue, we conducted a Harman’s single-factor test. An exploratory factor analysis on all items identified 15 factors with eigenvalues greater than 1. The variance explained by the first factor was 17.07%, which falls below the 40% threshold. Therefore, this study does not appear to suffer from significant common method bias.
Descriptive statistics and correlation analysis
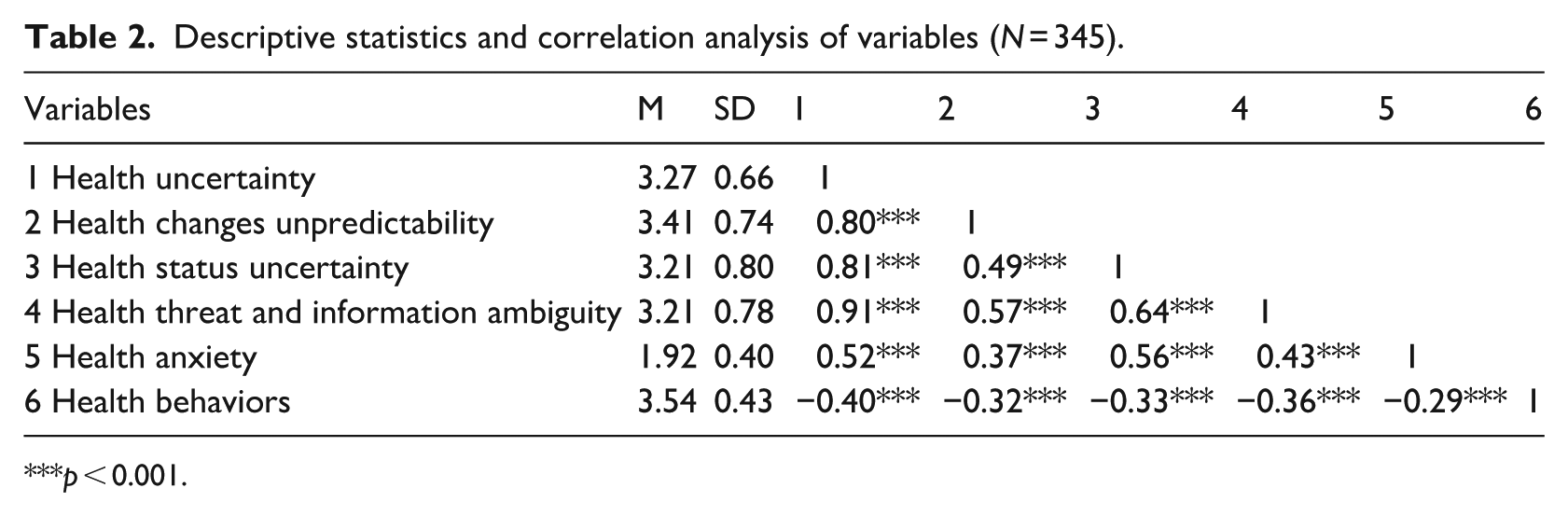
We performed descriptive and correlational analyses for health uncertainty (including its three dimensions), health anxiety, and health behaviors, as shown in Table 2. The results indicated that health anxiety was significantly positively correlated with health uncertainty and all three of its dimensions. In contrast, health behaviors showed significant negative correlations with health uncertainty and its three dimensions. Additionally, results revealed a significant negative correlation between health anxiety and health behaviors.
Descriptive statistics and correlation analysis of variables (N = 345).
p < 0.001.
Mediating model test of health uncertainty, health anxiety, and health behaviors
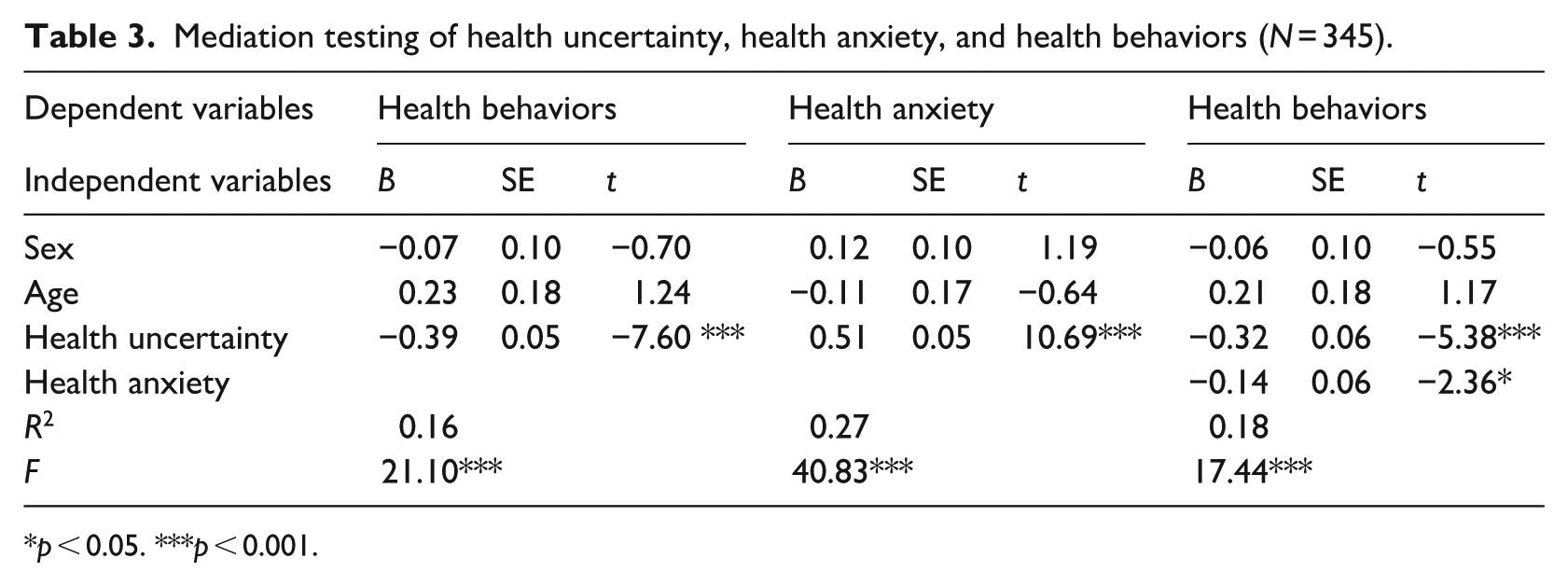
We employed Model 4 of PROCESS macro to examine the mediating effect, with health uncertainty as the independent variable, health anxiety as the mediating variable, health behaviors as the dependent variable, and demographic variables as control variables. The results of a Bootstrap non-parametric test revealed that health uncertainty significantly predicted health behaviors (b = −0.39, SE = 0.05, 95% CI [−0.49, −0.29]). Furthermore, the analysis identified a significant mediating effect of health anxiety (direct effect: b = −0.32, SE = 0.06, 95% CI [−0.44, −0.20]; indirect effect: b = −0.07, SE = 0.04; 95% CI [−0.15, −0.01]). The indirect effect accounted for 17.95% of the total effect, indicating that health anxiety played a partially mediating role, thus supporting
Mediation testing of health uncertainty, health anxiety, and health behaviors (N = 345).
p < 0.05. ***p < 0.001.
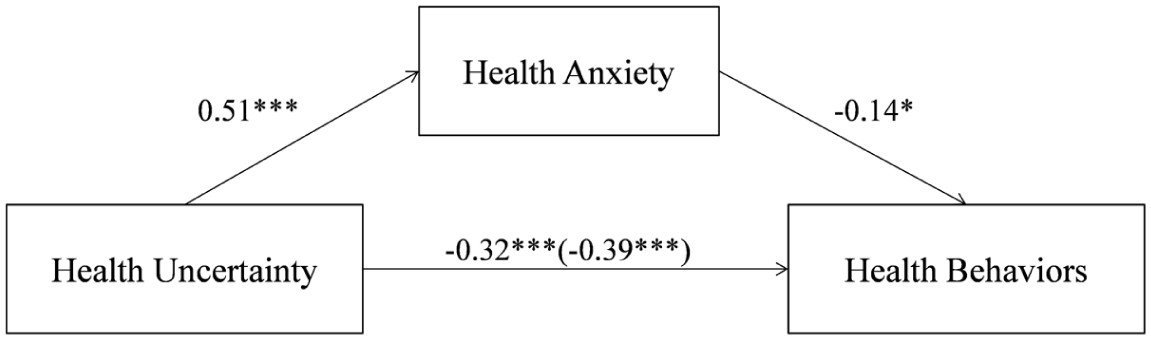
Mediation path diagram of health uncertainty, health anxiety, and health behaviors.
Discussion
This study advances the conceptualization of health uncertainty, grounded in Uncertainty Management Theory (van Den Bos, 2001) and the Theory of Illness Uncertainty (Mishel, 1990; Wright et al., 2009), and introduces a bespoke scale to measure this phenomenon within the general population, diverging from the traditional focus on specific patient groups. The newly developed Health Uncertainty Scale, comprising 16 items across three dimensions (health status uncertainty, health changes unpredictability, and health threat and information ambiguity), facilitates a broader understanding of health uncertainty’s impact on health behaviors through the mediating role of health anxiety.
Initially, we identified four hypothesized dimensions of health uncertainty. However, during the revision process, we observed that the dimension concerning health threat perception significantly overlapped with the dimension of health information ambiguity. As a result, the final factor structure retained three key dimensions that contribute to health uncertainty. First, health status uncertainty refers to an individual’s perceptions and doubts about their current health status and its variability. This dimension covers a range of health-related concerns, from mild apprehensions to conditions that meet the diagnostic criteria for Illness Anxiety Disorder (IAD; Newby et al., 2017). Unlike IAD, which is characterized by persistent, clinically significant distress or impairment, most individuals experience only transient concerns that do not reach such intensity. Second, health changes unpredictability captures the challenges individuals face in predicting changes in their health, such as sudden illnesses or injuries. This dimension mirrors the unpredictability aspect of illness uncertainty, which focuses on the inability to foresee disease progression (Mishel, 1990). The resulting unpredictability can undermine an individual’s sense of control over their future health, a phenomenon linked to increased uncertainty (van Den Bos, 2001). Third, health threat and information ambiguity reflects the often unclear, incomplete, or contradictory information regarding health risks and methods of health maintenance. It integrates the originally proposed categories of health threat perception and health information ambiguity, as perceived health threats often arise from ambiguous or conflicting information, making the two difficult to distinguish. For instance, during public health crises, individuals frequently encounter ambiguous or contradictory messages about health risks and preventive measures (Lee et al., 2018; Nagler and Shi, 2022). Such ambiguity significantly heightens threat perceptions, especially regarding emerging infectious diseases or vague health hazards (Pappas et al., 2009). Moreover, the growing reliance on online sources has further complicated health communication, amplifying anxiety when credible information is difficult to discern (Brown et al., 2020). The quality and clarity of health messaging thus play a crucial role in shaping how people perceive and respond to health threats (Zhang et al., 2020).
Upon establishing the dimensions of health uncertainty, we examined its associations with health anxiety and health behaviors. The results indicated that health uncertainty negatively predicts health behaviors, supporting
Moreover, our findings indicate that health anxiety mediates the relationship between health uncertainty and health behaviors, supporting
Insights and implications
First, this study introduces the concept of health uncertainty within the framework of Uncertainty Management Theory and develops the Health Uncertainty Scale. Unlike previous studies that either used vague measures of uncertainty (Brashers, 2001; Kuang and Wilson, 2017) or focused on illness uncertainty in clinical populations (Landis, 2009; Mullins et al., 2017; Wright et al., 2009), health uncertainty targets the general public’s perception of uncertainty about their own health, particularly in the context of public health emergencies. Its broader applicability expands the scope of uncertainty research within the health domain.
Second, this study examines how uncertainty during public health crises influences health behaviors. Previous research on health behaviors during public health events has primarily focused on measuring risk perception and health behaviors separately or conducting correlational analyses (Lee et al., 2009; Mozgovaya et al., 2021), with limited investigation into how risk-induced health uncertainty influences health behaviors. By identifying the sources of health uncertainty and linking them to behavioral outcomes, this study offers actionable insights for promoting health behaviors through uncertainty-reducing public health interventions.
Third, the findings offer practical implications for managing health uncertainty in times of crisis. Health threats and information ambiguity are crucial components of health uncertainty that significantly predict health anxiety and health behaviors. This underscores the importance of clear, timely, and accurate public health communication. Effective risk communication—especially via digital media—can reduce anxiety and foster positive behavioral responses (Al-Dmour et al., 2020). Moreover, improving health literacy through public education (Nutbeam, 2000; Wittink and Oosterhaven, 2018) can help individuals better process health information and manage uncertainty, ultimately supporting both individual and collective health outcomes.
Limitations and suggestions for future research
First, the development and validation of scales is an ongoing process (DeVellis and Thorpe, 2021). The conceptualization and measurement of health uncertainty remain at an early stage. As research expands, the health uncertainty scale is expected to undergo revisions and cross-cultural studies in the future, enhancing its robustness. Moreover, uncertainty can manifest as both a trait and a situational factor (Hogg, 2007). Future studies should examine its dispositional characteristics as well as the situational factors that influence it.
Second, we conducted this study exclusively in China with a primarily young adult sample, which may limit the generalizability of the findings. While this homogeneous group helps control for extraneous variables and highlights the relationships among key variables (Maydeu-Olivares and Millsap, 2009), responses to health uncertainty may vary across age groups, cultures, or countries. Future research should examine these relationships across broader demographic and cultural contexts to assess the robustness and generalizability of the current findings.
Third, the mechanisms and boundary conditions of the relationship between health uncertainty and health behaviors require further investigation. According to uncertainty management theory, increased feelings of uncertainty lead individuals to more strongly endorse their cultural norms and values orientations (Van Den Bos et al., 2007). This suggests that the predictive capacity of health uncertainty on health behaviors may vary depending on individual value orientations. For example, within the domain of value orientations, temporal orientation can predict dietary choices, while future temporal orientation is a more accurate predictor of exercise behavior (van Beek et al., 2013). Other potential moderators include attitudes, norms, and perceived behavioral control related to preventive behaviors (Seong and Bae, 2022), as well as internal versus external health control beliefs (Dogonchi et al., 2022).
Finally, this study employed a cross-sectional design to examine the mediating relationships among health uncertainty, health anxiety, and health behaviors. While this framework is theoretically sound, the relationships among these three variables may be more complex. Health behaviors, such as physical exercise, could potentially influence levels of uncertainty or anxiety (Herbert et al., 2020; Rogowska et al., 2020). Future research is encouraged to adopt longitudinal or experimental designs to investigate the dynamic relationships or causal links among these variables.
Conclusions
This study has elucidated the complex dynamics of health uncertainty, its underlying dimensions, and its significant impact on health behaviors mediated by health anxiety. By clarifying and operationalizing the concept of health uncertainty, and by identifying and validating its three dimensions, this study provides a comprehensive framework and solid foundational for understanding how individuals perceive potential health risks and uncertainties, particularly in non-clinical populations. Additionally, the study highlights health anxiety as a key mediator linking health uncertainty to health behaviors, underscoring the need to address both cognitive and emotional factors in health communication and interventions. Together, these insights contribute to a more effective approach in public health practices, aiming to reduce uncertainty and anxiety to improve health behaviors and outcomes during public health emergencies.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251405156 – Supplemental material for Health uncertainty: Scale development and its effect on health behaviors
Supplemental material, sj-docx-1-hpq-10.1177_13591053251405156 for Health uncertainty: Scale development and its effect on health behaviors by Rui Ren, Su Tao, Yuhua Ouyang and Wenchong Du in Journal of Health Psychology
Footnotes
Ethical considerations
This study was approved by the Psychology Academic Committee of the School of Marxism at China University of Geosciences (Beijing) on December 26, 2022.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Participants provided consent for the publication of anonymized data and findings.
Author contributions
Conceptualization, data curation, formal analysis, investigation, writing original draft by Rui Ren. Conceptualization, funding acquisition, methodology, project, supervision, writing, review & editing by Su Tao. Investigation, writing original draft by Yuhua Ouyang. Supervision, writing, review & editing by Wenchong Du.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by Humanities and Social Science Fund of Ministry of Education of China (grant number 19YJC710066).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.