
Abstract
This quasi-experimental study examined the effects of computerized cognitive training (CCT) on cognition, mental health, and quality of life (QoL) in healthy older adults. One hundred thirty community-dwelling older adults (mean age = 71.5 ± 5.3 years, range 60–86; 93% women) chose either an individual home-based CCT program or a group-based CCT program delivered at a university center. Both groups participated in weekly 60-minute sessions for 20 weeks. Validated measures were used to assess cognition (Montreal Cognitive Assessment (MoCA), Naming of Pictures and Their Recall, animal verbal fluency), mental health (Geriatric Depression Scale, Geriatric Anxiety Inventory), and QoL (Older People’s Quality of Life Questionnaire–Brief). Wilcoxon tests showed small to medium improvements in cognitive and emotional outcomes within each group, with greater cognitive gains in the group-based format (e.g. MoCA total: p = 0.027; MoCA memory domain: p = 0.029; Naming of Pictures and Their Recall: p = 0.023). No significant change was found for QoL. These findings suggest that group-based CCT, which incorporates regular social interaction, may be a promising and scalable approach to promoting cognitive and emotional well-being among older adults in community settings.
Introduction
Aging is a natural stage of life in which progressive changes occurs (Karlı and Can, 2024) in biological (e.g. cellular inflammatory pathways), psychological (e.g. cognitive and behavioral changes), and sociocultural (e.g. shifting family or community roles) processes. Among these age-related changes, cognitive decline is one of the most prevalent and impactful, and in some individuals, it may progress to clinical conditions such as mild cognitive impairment or dementia (Testo et al., 2025). Around 50 million people worldwide are living with dementia and this figure is projected to rise to 152 million in the context of an aging population by 2050 (GBD 2019 Dementia Forecasting Collaborators, 2022; Livingston et al., 2020). Although some studies report a decreasing trend in age-specific dementia incidence, the absolute number of people living with dementia continues to rise due to population aging (GBD 2019 Dementia Forecasting Collaborators, 2022). Dementia is now one of the most pressing global public health challenges due to its increasing prevalence, high economic burden, and profound impact on individuals and their families (Gates et al., 2020). In 2019, the global cost of dementia was estimated at over US$1.3 trillion, and this figure is projected to double by 2030 as populations age (GBD 2019 Dementia Forecasting Collaborators, 2022; WHO, 2002). The condition not only leads to a progressive loss of cognitive and functional independence but also significantly impairs quality of life (QoL) and increases caregiver burden. Dementia care requires long-term support, often involving formal and informal care networks, which places growing pressure on health and social care systems worldwide (Olivari et al., 2020).
In response to these challenges, the Czech Republic developed a National Strategy for Preparing for an Aging Society 2019–2025, which emphasizes the early detection of cognitive disorders, timely intervention, and the promotion of mental well-being in older adults (MPSV; Ministry of Labour and Social Affairs of the Czech Republic, 2019). This strategy adopts a holistic view of health in later life, recognizing that physical, mental, social, and spiritual well-being are interconnected components of healthy aging, in line with frameworks such as the WHO Active Aging model (World Health Organization, 2002). Among its main objectives is the development of effective dementia prevention programs focused on the aging population, particularly those at risk of cognitive decline and mental illness. Recommended measures include the promotion of cognitive, physical, and social activities to help maintain cognition (Lin et al., 2023; Lloyd-Hazlegreaves et al., 2023; Walsh et al., 2022, 2023). Although growing evidence supports the value of these interventions, findings remain mixed regarding the long-term effectiveness of specific activities in preventing dementia, especially among cognitively healthy older adults (Kane et al., 2017; Lampit et al., 2020).
Although pharmacological treatments for dementia have received significant attention, their effectiveness in preventing or reversing cognitive decline in healthy older adults remains limited. Medications targeting brain health may be associated with side effects, high costs, and modest clinical benefits, particularly in the early or preclinical stages of cognitive impairment (Gauthier et al., 2006; Livingston et al., 2020; Simons et al., 2016). These limitations have increased interest in non-pharmacological strategies to support cognition in aging populations.
Traditional formats of cognitive training often involve paper-and-pencil exercises or therapist-led group activities aimed at enhancing targeted cognitive domains. In recent years, these methods have evolved into computerized cognitive training (CCT), which offers interactive, adaptive tasks delivered through digital devices such as computers, tablets, or smartphones (Bang et al., 2024; Duda and Sweet, 2020; Lampit et al., 2014). The rise of commercially available brain-training applications such as Lumosity, BrainHQ, or CogniFit has made CCT increasingly accessible to older adults and easier to implement on a larger scale (Ge et al., 2018; Simons et al., 2016). CCT is believed to strengthen underlying neural networks through mechanisms of neuroplasticity (Dimitriadis et al., 2024; Gates and Valenzuela, 2010; Nicastri et al., 2022) and can be delivered in both individual and group formats, offering flexibility and scalability (Kelly et al., 2017; Lampit et al., 2014). Moreover, many older adults also engage in cognitively stimulating leisure activities such as puzzles, card games, or general computer use, which have been associated with a reduced risk of cognitive impairment in later life (Yates et al., 2016). These activities, while less structured than standardized CCT, illustrate the broader potential of mental stimulation to support cognitive health.
Evidence for the effectiveness of CCT varies depending on the target population. Studies among older adults with mild to moderate cognitive impairment have shown promising results, with improvements observed in domains such as memory, executive function, and processing speed (Bahar-Fuchs et al., 2013; Li et al., 2019, 2022; Tortora et al., 2024). In contrast, research on CCT in cognitively healthy older adults is more limited and has yielded mixed results (Gates et al., 2019; Kane et al., 2017; Lampit et al., 2014; Simons et al., 2016). Systematic reviews suggest that while CCT may lead to modest gains in specific trained domains (e.g. working memory or attention), there is limited evidence that these improvements generalize to everyday functioning or long-term cognitive resilience (Lampit et al., 2020). These mixed findings have encouraged researchers to explore new ways to enhance the impact of cognitive training, including the integration of social and emotional elements to increase engagement, motivation, and well-being.
To address this limitation, growing attention has been directed toward integrating social elements into cognitive training. Combining cognitive exercises with structured social interaction may not only enhance engagement and motivation, but also improve emotional and psychological outcomes (Ben Izhak et al., 2024; Kelly et al., 2017; Lampit et al., 2014; Rieker et al., 2022). Evidence indicates that socially enriched cognitive training can reduce loneliness and support psychological well-being, while also reinforcing cognitive self-efficacy, defined as the individual’s confidence in their ability to perform cognitively demanding tasks (Goghari and Lawlor-Savage, 2018). Higher self-efficacy has been linked to grater adherence and stronger perceived benefits of training. Psychosocial factors such as social engagement and perceived social support are closely linked with better cognition and higher quality of life in later life (Kelly et al., 2017). A systematic review further demonstrated positive associations between social support and multiple cognitive domains, including global cognition, executive functioning, working memory, visuospatial skills, processing speed, and episodic memory (Kelly et al., 2017). Several theoretical frameworks, including the Convoy Model, Socioemotional Selectivity Theory, the Strength and Vulnerability Integration (SAVI) model, and the Functional Specificity Theory, provide insight into these mechanisms (Kelly et al., 2017). Together, these perspectives highlight the importance of designing cognitive interventions that incorporate both individual and group-based formats in order to optimize not only cognitive but also emotional and social outcomes for older adults.
Aim
The aim of this study was to evaluate the effects of CCT on cognition, mental health, and QoL in community-dwelling older adults, and to examine whether these outcomes differ based on the format of the intervention – specifically, individual home-based CCT versus group-based CCT sessions incorporating social interaction. This study addresses a gap in the literature by comparing two delivery formats using the same intervention content, thereby contributing to current understanding of how the context of cognitive training may influence its effectiveness in cognitively healthy older adults.
Methods
Design
This study employed a prospective quasi-experimental pretest–posttest design comparing two non-randomized intervention groups: (1) individual CCT performed at home, and (2) group-based CCT conducted in a structured setting with additional social interaction and trainer support. Participants were not randomly assigned but voluntarily chose their preferred intervention group. No control group without intervention was included in the study. This decision was based on ethical and practical considerations: participants were older adults actively seeking cognitive support, and withholding any form of intervention in a context of voluntary enrollment was deemed inappropriate. Additionally, the study aimed to compare two real-world delivery formats of the same intervention, rather than to evaluate efficacy against a no-treatment baseline.
This design corresponds to a patient preference trial model, which is appropriate when participants are likely to have strong preferences and when blinding is not feasible (King et al., 2005). The rationale for offering both formats was informed by theoretical models of cognitive aging. Individual CCT supports cognitive maintenance through self-directed practice and the principles of neuroplasticity (Gates and Valenzuela, 2010), whereas group-based CCT builds upon the “use it or lose it” hypothesis and incorporates elements of social facilitation theory (Zajonc, 1965), which suggests that learning and motivation can be enhanced through social interaction and peer presence. The group format also reflects aspects of the cognitive enrichment model, which emphasizes the synergistic benefits of combining mental stimulation with social engagement to promote healthy cognitive aging (Hertzog et al., 2008).
The study is reported in accordance with the TREND (Transparent Reporting of Evaluations with Nonrandomized Designs) statement (Des Jarlais et al., 2004), and a completed TREND checklist is available as Supplemental File 1.
Ethical aspects
The study was carried out according to the provisions of the Declaration of Helsinki and was approved by the Ethics Committee of the University of Ostrava (no. 14/2020). All subjects gave their informed consent to inclusion before participating in the study.
Participants
Older people living in the community were contacted to participate in the study through the Center for Prevention and Promotion of Healthy Aging of the Faculty of Medicine of the University of Ostrava. This center regularly publishes information about the activities offered on its website, as well as through general practitioners, libraries, and older people’s clubs. The criteria for inclusion in the research group were: age 60 years or older; no clinical diagnosis of cognitive impairment; sufficient vision and hearing to perceive computer-based stimuli; and access to an email account. All participants were assessed as having adequate capacity to understand study procedures and voluntarily provide informed consent. The ability to provide informed consent was assessed during the initial enrollment session by trained research staff (psychologist). Participants were asked to explain, in their own words, the purpose of the study, the nature of their participation, and their rights as research subjects. In addition, participants who chose the individual CCT group were required to have access to a personal computer, laptop, or tablet with internet connection and basic audiovisual functionality (screen and speakers or headphones), as the training was carried out independently at home. All participants were also required to have an active email account for communication and support.
We calculated the number of participants to ensure a sufficient sample size to demonstrate the impact of CCT training. With α = 0.05 and a power of 90% (the effect size 0.6), SPSS software indicated that minimally 32 subjects were needed for each group for the study.
Of the 198 older people who met the inclusion criteria, 160 agreed to be included in the research study and 130 completed the cognitive program (Figure 1). Seventeen participants in the group program and 13 in the individual program ultimately chose not to start the intervention due to a deterioration in their health status.
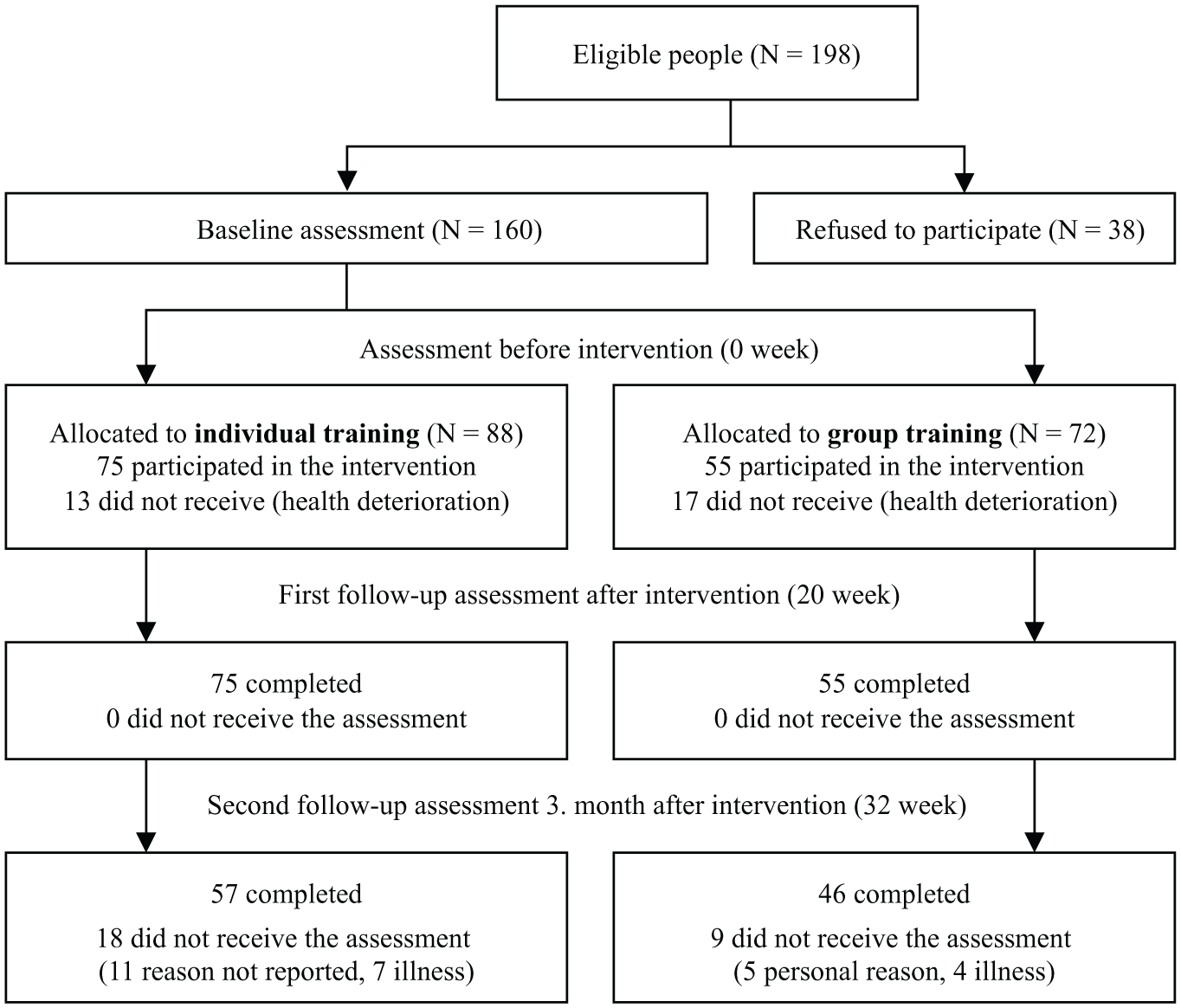
Flow diagram of study participants in the two intervention groups of individual computerized cognitive training, and group computerized cognitive training.
Procedure
All participants enrolled in the study were invited to an individual meeting with a research assistant (psychologist or research nurse), where the course of the selected program was explained to them. Participants voluntarily chose whether to join the supervised group CCT or the individual CCT program. Both groups also received a written manual that they could review at home. During this meeting, the first cognitive assessment and questionnaire completion took place (baseline, week 0). They also signed an informed consent form. They were then enrolled in the next scheduled training group.
The cognitive program was implemented for 6 months in four runs (1: September 2021–February 2022; 2: March–August 2022; 3: September 2022–February 2023; 4: March–August 2023). The maximum number of participants in one run was 40 (group training max. 20 people). The cognition testing and questionnaire completion took place before the start of the program (first measurement – T1 – baseline), after its completion (second measurement – T2 – post-intervention) and 3 months after its completion (third measurement – T3 – follow-up).
Intervention
The CCT program consists of activities that develop cognition (primarily memory, attention, imagination, spatial orientation, and decision-making speed) using the complex computer training program MENTEM (www.mentem.cz), practical training, and motivation for regular long-term strengthening of cognition. The MENTEM.cz program operates online. It was developed by the Czech Non-profit company Mentem – brain training, z.s. (registered association). The MENTEM program is available only in a Czech language version. The MENTEM program was chosen for its accessibility, user-friendliness for older adults, and availability in the Czech language. Although no peer-reviewed validation studies have been published to date, the program is based on cognitive training principles and is widely used in applied practice across the Czech Republic.
The MENTEM training program offers 24 different games to exercise cognition using randomly selected tasks. Psychological exercises and principles take the form of fun games that help improve cognition of the brain – primarily memory, attention, and solving common tasks. For each day, the computer prepares five games. Other games can be chosen by the client according to their interests or preferences. Individual games allow the exercise of cognition such as attention, memory, speed, spatial orientation, imagination, thinking, and judgment. After each game, feedback on performance was given on the screen in the form of percentage of improvement in a game. The MENTEM program records the total score for each game and calculates the percentage of improvement or decline for each game, making this information accessible to participants for self-monitoring. The MENTEM program also contains a calendar with highlighted days of already completed trainings to help participants keep an overview of the training intervals.
All participants in the study had access to the MENTEM computer program for 6 months. A condition of completing the course was to perform tasks at least three times a week. Study participants were divided into two groups (group and individual training).
A trained instructor (registered nurse or psychologist with experience in cognitive training) provided initial instruction, written materials, and ongoing support – via email for the individual group and in-person for the group-based sessions. Fidelity was supported through automatic tracking of session completion and regular instructor oversight. However, no formal fidelity assessment was conducted. The choice between individual and group formats was based on participant preference. Study participants chose to participate in one of two possible intervention groups (i.e. individual training or group-based CCT), as detailed below.
Individual CCT
As part of the individual CCT program, older adults completed the training at home using their personal computers over a 20-week period. Participants were instructed to complete tasks in the MENTEM program every day for at least 20 minutes. The instructor was in contact with the participants of individual CCT weekly via email, motivating the participants to perform daily tasks.
Group CCT
As part of the group training, older people performed the training on the PC individually in their home environment for 20 weeks, participating once a week for 60 minutes in a group training with the instructor at the Center for the Prevention of Healthy Aging. In addition to the computer-supported program (30 minutes), the group training was enriched with tasks mainly focused on vocabulary, counting, or logical thinking tasks (30 minutes). In the group training, social interaction was fostered through regular group sessions where participants could interact with each other, exchange feedback, and collaborate on some of the non-computer-based exercises.
Data collection
All of the instruments described below were administered in printed (paper) format and in the Czech language. Data were collected at three time points: at baseline (week 0, prior to the start of the intervention), immediately after completion of the 20-week training program (week 20), and at a 3-month follow-up (week 32). All assessments were conducted in person by trained healthcare professionals – licensed nurses or psychologists – who were experienced in administering standardized cognitive and psychosocial measures.
Assessment of cognition
To evaluate cognition, we used the Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005), the POBAV test (Pojmenování Obrázků A jejich Vybavení = Naming of Pictures and Their Recall; Bartoš, 2016), and a verbal fluency task focused on naming animals. These tools were selected to assess key cognitive domains including memory, executive function, language, visuospatial ability, and semantic fluency, which are important in early detection of cognitive changes associated with aging. The test battery was selected in consultation with clinical neuropsychologists to ensure appropriateness for cognitively healthy, community-dwelling older adults, and to balance diagnostic sensitivity with feasibility for repeated assessments in a non-clinical setting.
The MoCA assesses seven cognitive domains (Nasreddine et al., 2005), namely, Visuospatial/Executive (0–5 points), Naming (0–3 points), Attention (0–6 points), Language (0–3 points), Abstraction (0–2 points), Memory: Delayed Recall (0–5 points), and Orientation (0–6 points). The total score ranges from 0 to 30, with a score ⩾ 26 considered normal. Memory score are scores for Memory and Delayed Recall (0–25 points). The MoCA has been validated in the Czech population and is considered more sensitive than the Mini-Mental State Examination (MMSE) for adults over 60 years of age (Ciesielska et al., 2016). The MoCA has shown high sensitivity and specificity in detecting mild cognitive impairment (MCI), especially compared to the MMSE. In the original validation study by Nasreddine et al. (2005), the MoCA demonstrated a sensitivity of 90% and a specificity of 87% for MCI detection, with a test–retest reliability of r = 0.92. The Czech version has also been validated for the elderly population (Bartos and Fayette, 2018), confirming its diagnostic usefulness and cultural applicability.
The POBAV test is a a Czech-language cognitive screening tool that assesses visual memory, semantic recall, and written naming. Participants are shown 20 black-and-white images and asked to write down the name of each while attempting to remember them. They are then asked to recall and write down as many as they remember (Bartoš, 2016). One point is awarded for each correctly recalled and named item, resulting in a total score ranging from 0 to 20. The test is freely available for professional use and culturally adapted for Czech older adults. While formal standardization studies are limited, preliminary evidence suggests it has good face validity and is useful in detecting early cognitive changes in clinical and community settings (Bartoš, 2016).
Animal verbal fluency was assessed using a standard semantic verbal fluency task, where participants were instructed to name as many animals as possible within 60 seconds. Each correctly named, non-repeated animal counted as one point. This test is commonly used to assess executive functioning and semantic memory and is sensitive to cognitive decline in older adults. It has demonstrated good test–retest reliability (r = 0.70–0.90) and strong construct validity in aging populations (Whiteside and Luu, 2016).
The testing was conducted individually in a quiet room at the Center for the Prevention of Healthy Aging, Faculty of Medicine, University of Ostrava, by trained healthcare professionals, that is, licensed nurses or psychologists experienced in standardized cognitive assessment.
Assessment of mental health
Mental health was evaluated using the Geriatric Anxiety Inventory - GAI (Pachana et al., 2007) and the Geriatric Depression Scale – short version - GDS-15 (Sheikh and Yesavage, 1986).
The GAI consists of 20 dichotomous (yes/no) items evaluating symptoms of generalized anxiety. Scores range from 0 to 20, with a cut-off score of ⩾9 used to identify clinically relevant anxiety symptoms (Champagne et al., 2021). The Czech version of the GAI also shown excellent internal consistency (Cronbach’s alpha = 0.90) and good construct validity, supporting its use as a screening tool for anxiety in the elderly (Zvolská and Kotalová, 2021).
The GDS-15 contains 15 yes/no items screening for depression in older adults. Interpretation is based on cut-off ranges: 0–4 = normal, 5–8 = mild depression, 9–11 = moderate depression, 12–15 = severe depression. The Czech version of the GDS-15 has demonstrated good psychometric properties. Studies report high internal consistency (Cronbach’s alpha between 0.83 and 0.89) and strong test-retest reliability (ICC > 0.85), with confirmed construct validity in older adults in both community and institutional care settings (Ožanská et al., 2014).
Assessment of QoL
QoL was evaluated through The Older People Quality of Life - Brief (OPQOL- brief) questionnaire (Bowling et al., 2013; Bužgová et al., 2022). The scale consists of 13 statements rated on a five-point Likert scale (strongly disagree to strongly agree), with total scores ranging from 13 to 65 (OPQoL-brief score), where higher scores indicate better QoL. One additional item assessed global self-rated QoL (Global QoL) on a five-point scale (1 = very poor, 5 = very good), and was analyzed separately (Bowling et al., 2013). The questionnaire has demonstrated good psychometric properties, including high internal consistency (Cronbach’s alpha = 0.87) and satisfactory construct validity, as shown by its correlations with other established quality-of-life measures (Bowling et al., 2013). The Czech version of the OPQOL-brief was validated by Bužgová et al. (2022) showing excellent internal consistency (Cronbach’s alpha = 0.92) and test-retest reliability (ICC = 0.90). The scale also demonstrated good construct and convergent validity in a large sample of community-dwelling older adults.
Assessment of sociodemographic and health-related information
Sociodemographic and health-related information (e.g. age, gender, marital status, living arrangement, employment status, and chronic diseases) was collected using a structured questionnaire administered at baseline prior to the intervention. Participants were asked to report whether they were currently receiving treatment for chronic conditions, including cardiovascular, metabolic, musculoskeletal, neurological, sensory, and mental health disorders.
Data analysis
Data were processed in the SPSS software, v. 29. Descriptive statistics were used for the basic description of the data – absolute number (N), relative frequency (%), arithmetic mean, standard deviation (SD), and median (med.). We also evaluated the normality of the data. Data did not have a normal distribution (Shapiro-Wilk test (p < 0.001)). For this reason, we chose nonparametric tests.
Comparison of the difference in monitored parameters between measurements was made using the paired Wilcoxon test. The effect size of the results for the variables was also calculated using Cohen’s d, and their values were classified as insignificant (<0.19), small (0.20–0.49), medium (0.50–0.79), large (0.80–1.29), and very large (greater than 1.30; Sullivan and Feinn, 2012). To compare the differences between groups (individual and group program) the Mann-Whitney test was used. For all statistical level analyses, the significance level was set at p < 0.05.
Results
Demographic and health characteristics of participants
A total of 130 older people participated in the program, of whom 75 participated in the individual program and 55 participated in the group program. A total of 130 older people took part in the first and second measurements, while 103 older people took part in the third measurement after the third month (see Figure 1).
The average age of the participants was 71.5 years (SD = 5.3; range: 60–80 years), and they were primarily women (n = 121; 93%), married (n = 56; 43%), living alone (n = 63; 49%), and not working (n = 114; 88%). The group program with full-time participation was more often chosen by older participants, those living alone, not working, single, widowed, or divorced, and with greater anxiety and depression. However, the differences between groups were not statistically significant (see Table 1).
Sociodemographic and health characteristic of sample.
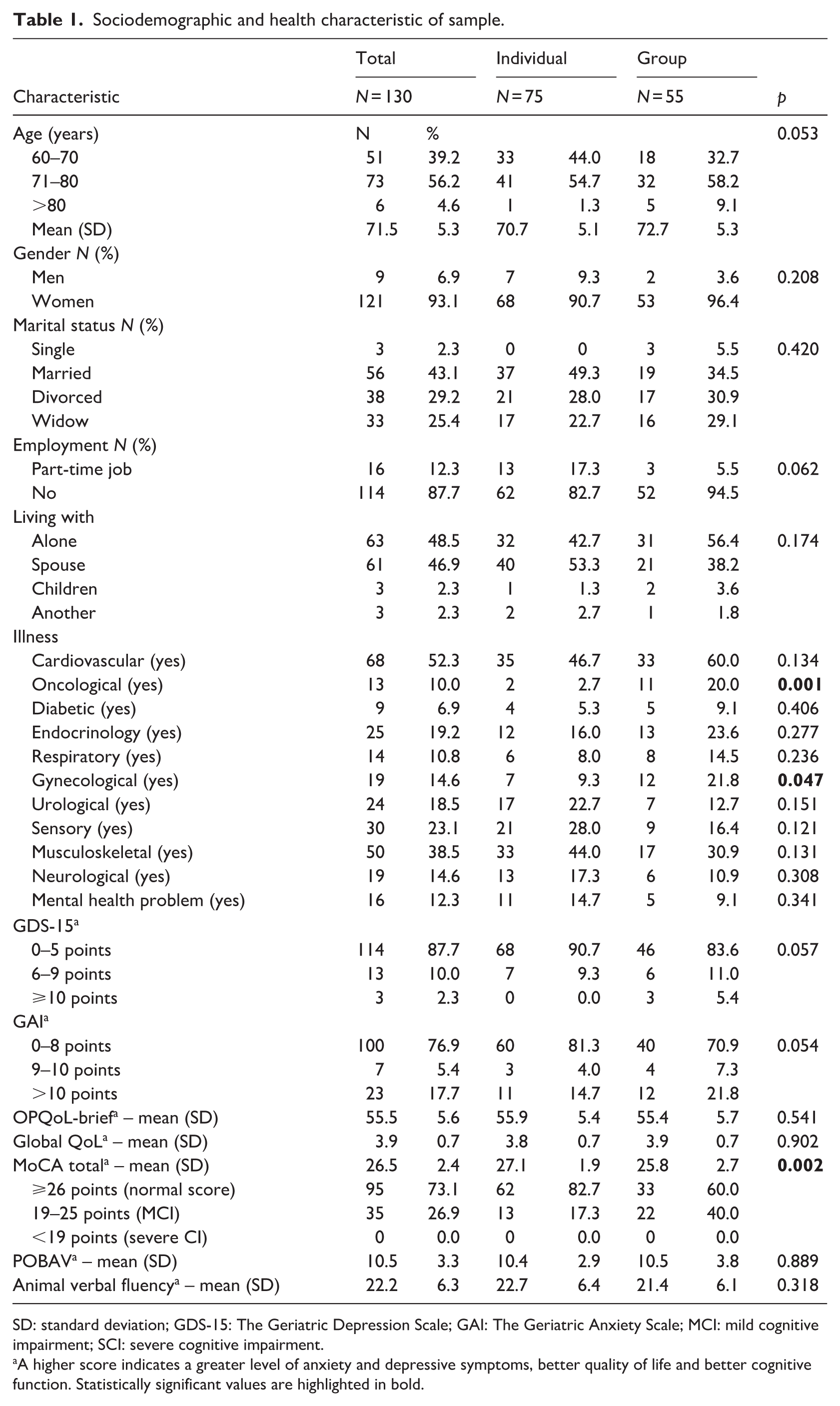
SD: standard deviation; GDS-15: The Geriatric Depression Scale; GAI: The Geriatric Anxiety Scale; MCI: mild cognitive impairment; SCI: severe cognitive impairment.
A higher score indicates a greater level of anxiety and depressive symptoms, better quality of life and better cognitive function. Statistically significant values are highlighted in bold.
Older people were also asked if they were regularly treated for chronic disease. Most frequently they reported cardiovascular (52.3%), musculoskeletal (38.5%) and sensory diseases (23.1%). A statistically significant difference was found between the two groups in terms of cancer (p = 0.001) and gynecological diseases (p = 0.047). Older people who participated in the group program were more likely to be treated for these conditions.
A statistically significant difference was found in baseline cognition, as measured by the MoCA test: the individual group had a higher mean score (M = 27.08, SD = 1.97) compared to the group intervention (M = 25.76, SD = 2.65; p = 0.002), indicating slightly better baseline cognitive abilities in the individual training arm. Notably, older adults with lower cognitive performance were more likely to choose the group training format, potentially seeking more structure or social support. When applying the MoCA classification thresholds, 17% of participants in the individual training group met the criteria for mild to moderate cognitive impairment (MoCA 18–25), compared to 38% in the group training arm. No statistically significant differences were found in the POBAV test or the animal verbal fluency task.
Effect on cognition
Evaluation of the difference in monitored parameters before, after intervention (individual CCT) and follow-up (N = 75).
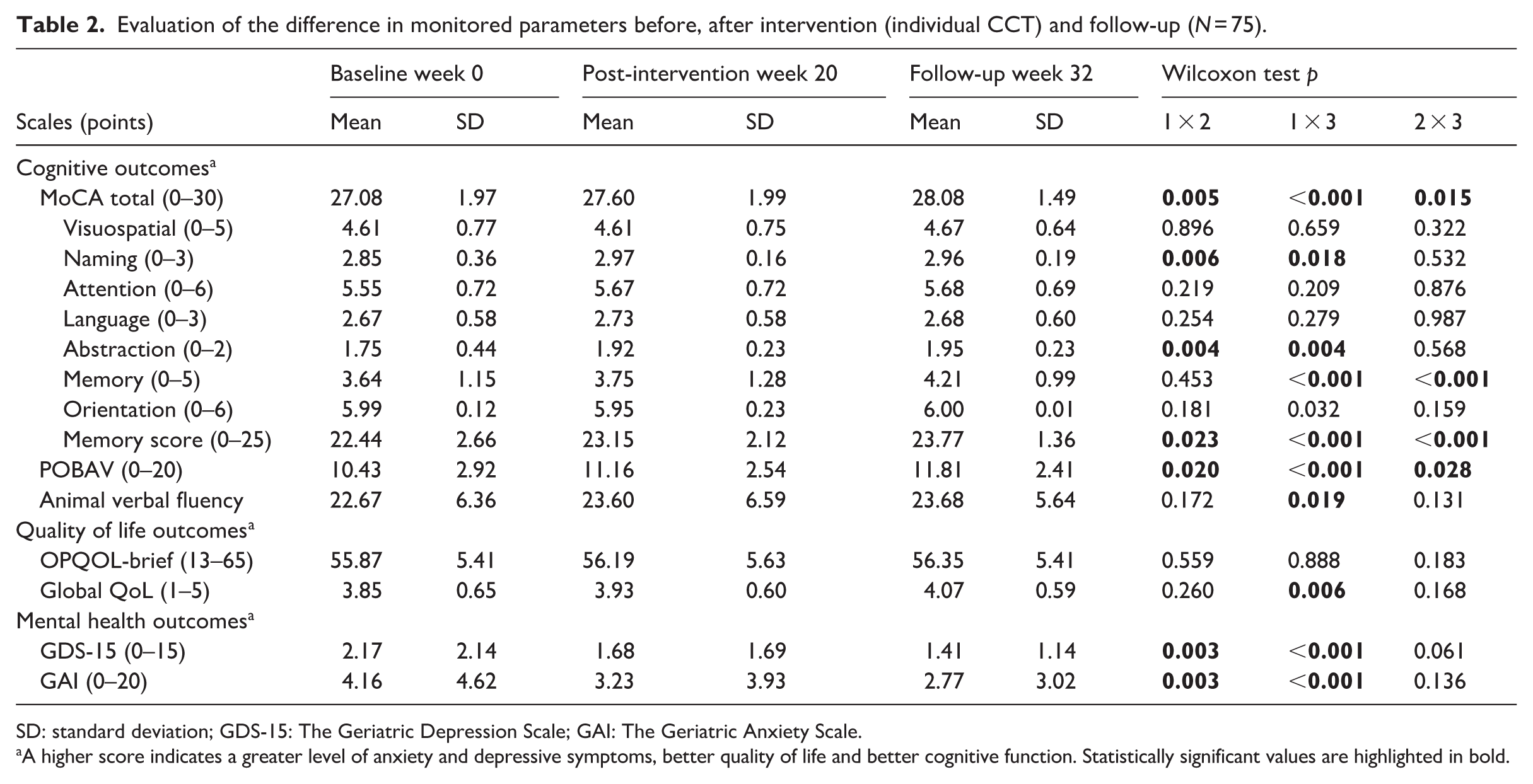
SD: standard deviation; GDS-15: The Geriatric Depression Scale; GAI: The Geriatric Anxiety Scale.
A higher score indicates a greater level of anxiety and depressive symptoms, better quality of life and better cognitive function. Statistically significant values are highlighted in bold.
A large effect was observed for the MoCA total score at the 3-month follow-up (Cohen’s d = 0.61), suggesting sustained cognitive improvement. Medium effects were found for memory (d = 0.51) and memory score (d = 0.55). Small effect sizes were observed for abstraction, naming, and POBAV, while other domains – such as attention, language, and orientation – did not show meaningful changes (Table 3).
Analysis of the effect size of the individual CCT (pre vs post vs follow-up).
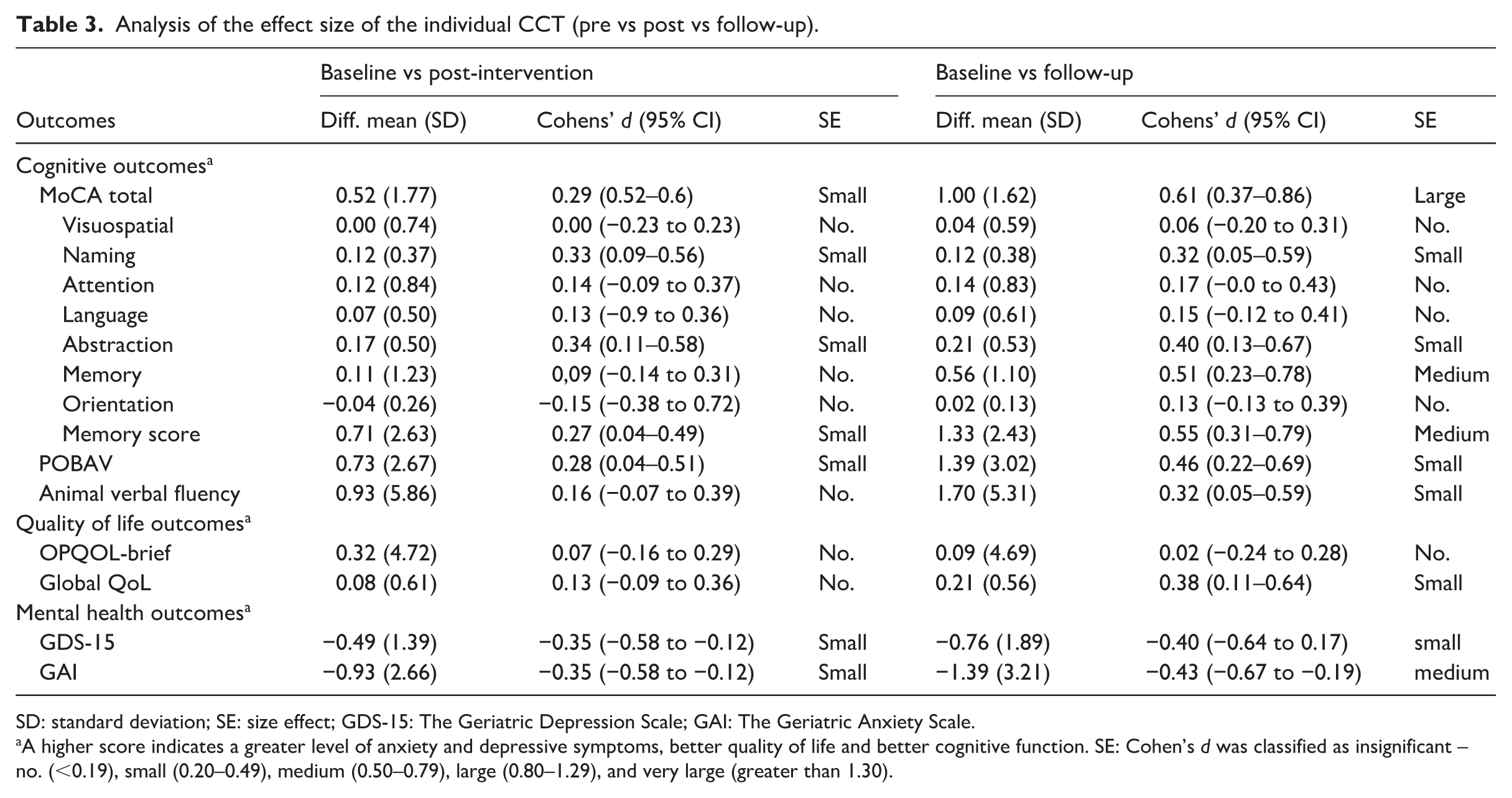
SD: standard deviation; SE: size effect; GDS-15: The Geriatric Depression Scale; GAI: The Geriatric Anxiety Scale.
A higher score indicates a greater level of anxiety and depressive symptoms, better quality of life and better cognitive function. SE: Cohen’s d was classified as insignificant – no. (<0.19), small (0.20–0.49), medium (0.50–0.79), large (0.80–1.29), and very large (greater than 1.30).
Evaluation of the difference in monitored parameters before, after intervention (group CCT) and follow-up (N = 55).
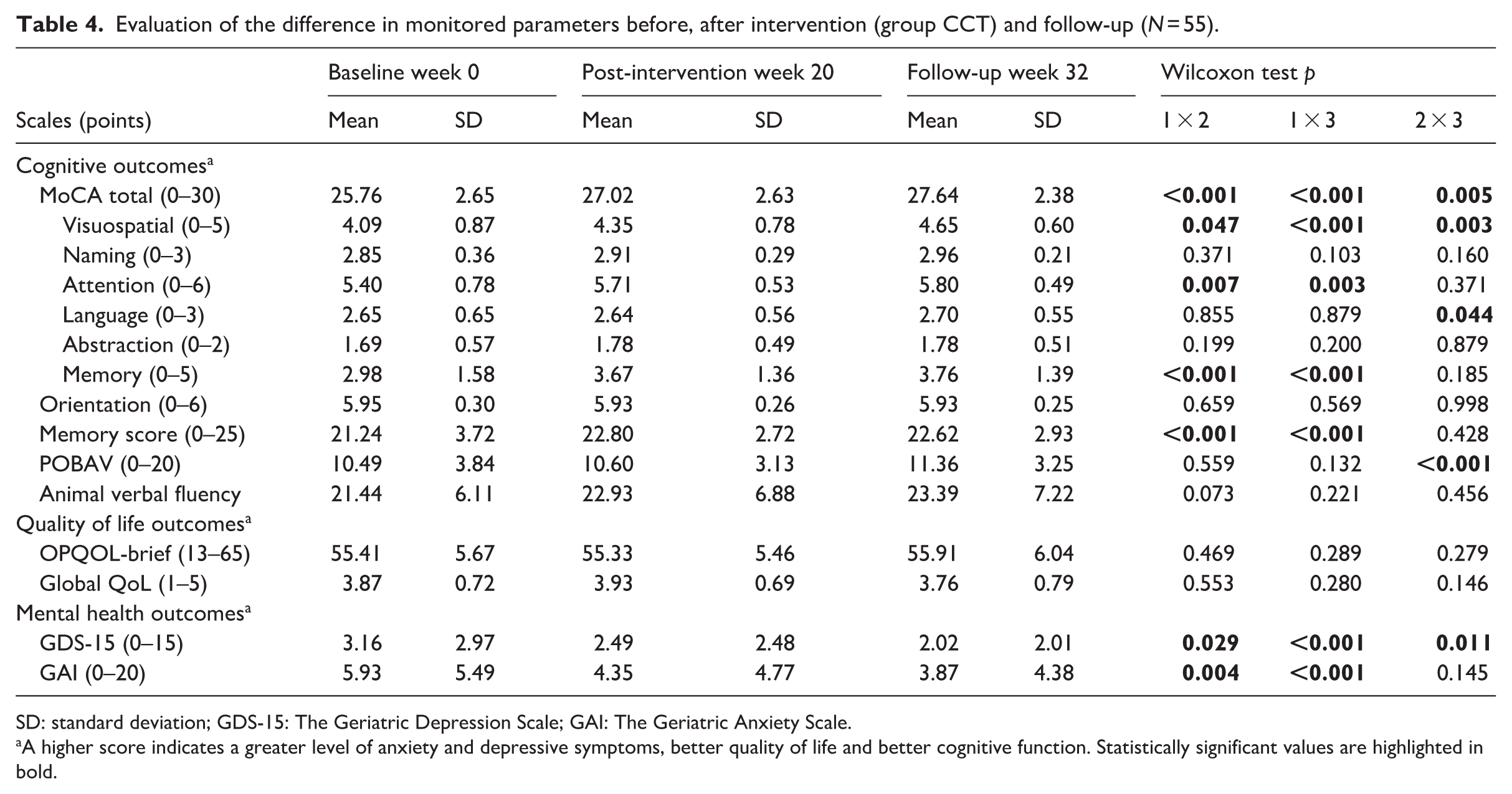
SD: standard deviation; GDS-15: The Geriatric Depression Scale; GAI: The Geriatric Anxiety Scale.
A higher score indicates a greater level of anxiety and depressive symptoms, better quality of life and better cognitive function. Statistically significant values are highlighted in bold.
Analysis of the effect size of the group CCT (pre vs post vs follow-up).
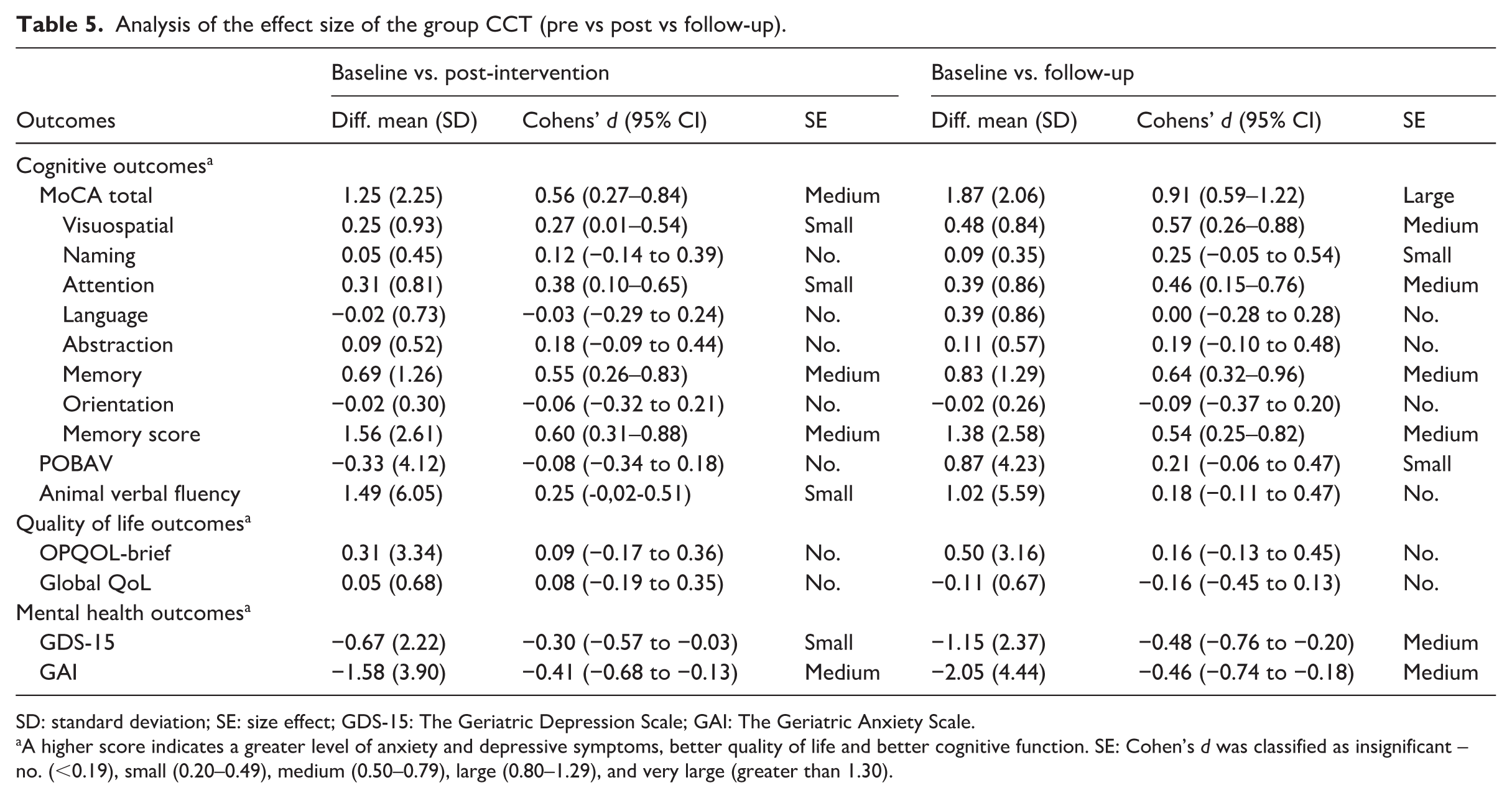
SD: standard deviation; SE: size effect; GDS-15: The Geriatric Depression Scale; GAI: The Geriatric Anxiety Scale.
A higher score indicates a greater level of anxiety and depressive symptoms, better quality of life and better cognitive function. SE: Cohen’s d was classified as insignificant – no. (<0.19), small (0.20–0.49), medium (0.50–0.79), large (0.80–1.29), and very large (greater than 1.30).
When comparing the individual and group CCT programs, statistically significant differences were found immediately after the intervention in the overall MoCA score (p = 0.027) and in the memory domain (p = 0.023), with greater improvements observed in the group CCT program. Furthermore, at the 3-month follow-up, a significant improvement in the overall MoCA score remained evident in the group CCT program (p = 0.045; Table 6).
Differences in evaluation of monitored parameters by form of cognitive program (group vs individual).
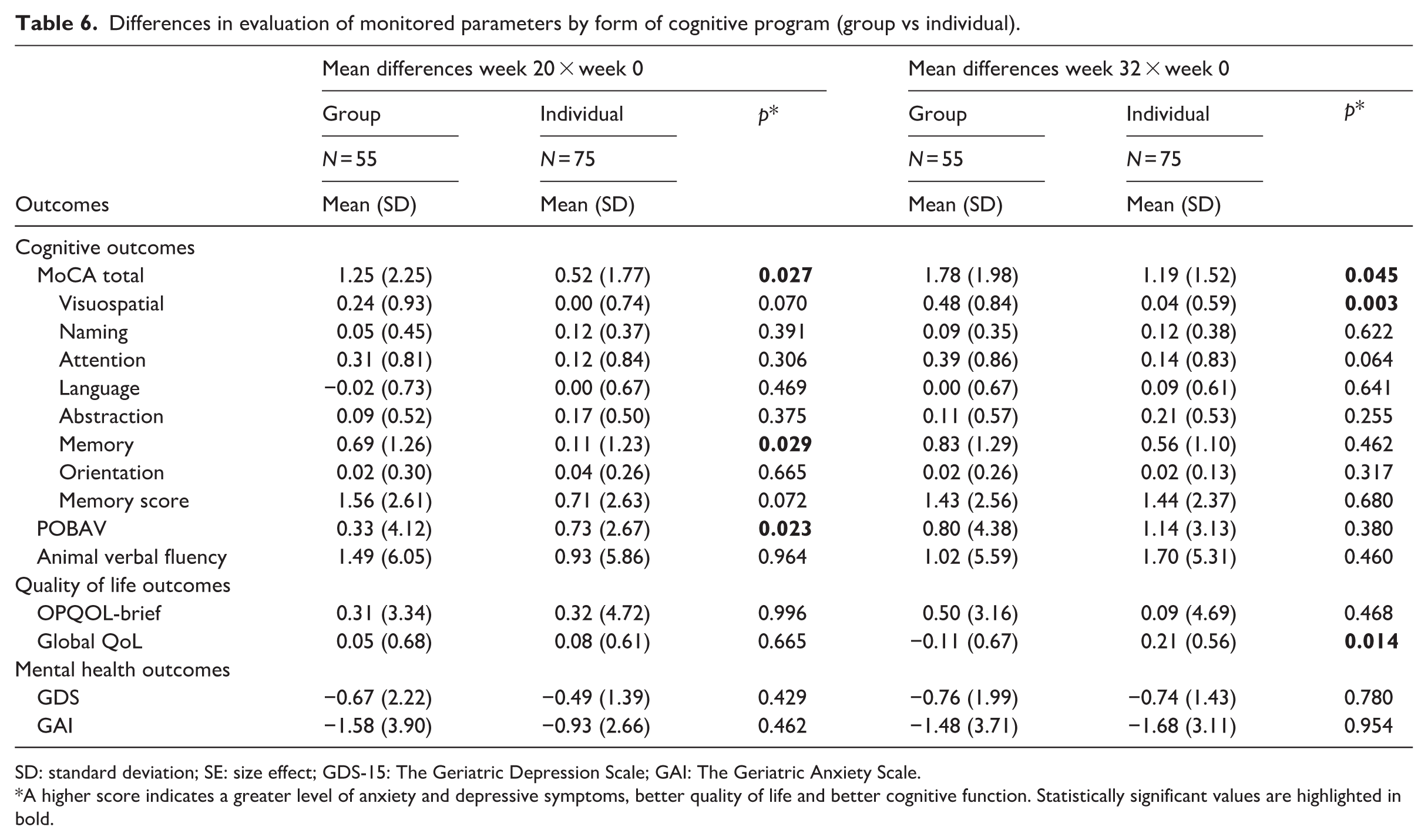
SD: standard deviation; SE: size effect; GDS-15: The Geriatric Depression Scale; GAI: The Geriatric Anxiety Scale.
A higher score indicates a greater level of anxiety and depressive symptoms, better quality of life and better cognitive function. Statistically significant values are highlighted in bold.
Effect on mental health
A significant reduction in symptoms of depression (GDS-15) and anxiety (GAI) was observed between baseline (week 0) and follow-up (week 32) in both the individual and group CCT program groups (p < 0.001; see Tables 2 and 4). No statistically significant differences were found when comparing the individual and group training programs (Table 6).
Effect on QoL
No statistically significant improvement in QoL was observed in either the individual or group CCT programs overall. However, in the individual CCT group, a significant improvement in Global QoL was found at the 3-month follow-up (p = 0.006; see Tables 2 and 4). No meaningful effect size was observed (Tables 3 and 5). When comparing the individual and group CCT programs, a greater improvement in Global QoL was found in the individual training group (p = 0.014; Table 6).
Discussion
This study aimed to contribute to the growing body of evidence on the effectiveness of CCT in healthy older adults. Both the individual and group-based formats of CCT produced measurable improvements in cognition and mental health, with stronger cognitive gains observed in the group program. However, no significant changes were found in overall quality of life, although emotional benefits were consistent across both formats. These findings suggest that while CCT can play an important role in supporting healthy aging, socially enriched, group-based delivery may offer additional advantages for enhancing cognitive outcomes in community-dwelling older adults (Ben Izhak et al., 2024; Kelly et al., 2017).
Our results are consistent with previous meta-analyses demonstrating that CCT can yield modest but significant improvements in executive function, memory, and global cognition (Gates and Valenzuela, 2010; Lampit et al., 2014, 2020). The stronger effects observed in the group-based program in our study may be explained by several mechanisms beyond the cognitive exercises themselves. Social interaction within group sessions likely fostered greater motivation and adherence through accountability and encouragement from peers. In addition, group participation may enhance cognitive self-efficacy, as observing others succeed in challenging tasks can strengthen confidence in one’s own cognitive abilities (Goghari and Lawlor-Savage, 2018). Emotional benefits should also be considered: regular social contact may reduce loneliness and improve well-being, which are closely linked with cognitive resilience (Kelly et al., 2017). Furthermore, the structured guidance of an instructor and peer collaboration may provide additional support, especially for participants with lower baseline cognitive performance, who in our study were more likely to choose the group format. Taken together, these social and emotional dimensions may amplify the cognitive impact of group-based CCT beyond what is typically achieved in self-directed, individual training.
Our results support these findings, with both the individual and group-based CCT formats producing measurable cognitive gains. Notably, the group-based CCT format resulted in significantly greater improvements, especially in visuospatial function and overall MoCA scores. These results are consistent with prior studies suggesting that structured group formats may enhance the effectiveness of cognitive interventions (Kelly et al., 2017; Peeters et al., 2023). In a meta-analysis by Kelly et al. (2017), interventions that incorporated social engagement demonstrated stronger effects on cognitive outcomes compared to purely individual training.
We also found that participants with lower baseline MoCA scores – potentially reflecting mild cognitive impairment (MCI) – were more likely to choose the group format. This aligns with previous observations that individuals experiencing cognitive concerns often seek structured, supportive environments (Gauthier et al., 2006; Smart et al., 2017). Offering socially enriched formats may therefore be particularly relevant for older adults at risk of decline.
In terms of emotional outcomes, both formats resulted in statistically significant reductions in anxiety and depressive symptoms, which were maintained at 3-month follow-up. These findings are in line with prior studies demonstrating that engaging in cognitive training may improve mood and reduce psychological distress (Baik et al., 2024; Viviani et al., 2023). While the mechanisms remain unclear, possible explanations include increased self-efficacy, sense of accomplishment, and daily structure.
By contrast, we did not observe significant improvements in QoL, either overall or in specific domains. This diverges from some studies reporting modest QoL gains following CCT (Klimova et al., 2017), but is consistent with others that found no significant change (Choi et al., 2021). One explanation could be a ceiling effect, as baseline QoL scores in our sample were already relatively high. In addition, the OPQOL-Brief may have limited sensitivity to short-term change or to improvements specifically tied to cognitive functioning.
Taken together, our results suggest that group-based CCT formats, especially those combining structured instruction and peer interaction, may lead to more pronounced cognitive benefits than self-directed approaches. These effects may be partly explained by social facilitation, motivation through group accountability, and shared learning experiences (Hertzog et al., 2008; Zajonc, 1965). However, the individual format may still offer emotional and psychological benefits, along with the practical advantage of flexibility – making it a viable option for those with barriers to group participation.
Limitations and strengths
This study has several limitations. First, participants self-selected into either the individual or group intervention, which may have introduced selection bias and limited the comparability of groups. Second, the absence of a non-intervention control group prevents firm conclusions about the effectiveness of the training. Third, adherence to the home-based training was not directly supervised, which may have introduced variability in actual training dose. Finally, the follow-up period was limited to 3 months, which restricts conclusions about long-term effects.
Nevertheless, as few studies have directly compared different delivery formats of CCT, our study extends the literature by highlighting the added value of the group-based CCT program compared to the individual home-based format. Another strength lies in the real-world setting of the intervention, which reflects the conditions under which CCT programs may be implemented in community practice. In addition, the use of validated measures for cognition, mental health, and quality of life enhances the reliability and comparability of our findings.
Conclusion
Computerized cognitive training appears to be a promising strategy for supporting cognitive and emotional health in healthy older adults. In our preference-based study, both individual and group formats led to improvements in cognition and mental health, with stronger cognitive gains observed in the group-based intervention. While no significant changes were found in QoL, emotional benefits were consistent across formats. The group training, enriched by structured social interaction, may offer additional advantages in cognitive domains such as memory and visuospatial function. However, the modest effect sizes, self-selected allocation, and absence of a control group limit the generalizability of the findings. Future research should explore long-term outcomes and consider integrating cognitive training with other supportive strategies to promote healthy aging.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053251409606 – Supplemental material for Individual and group computerized cognitive training for community-dwelling older adults: A quasi-experimental study investigating effects on cognition, mental health, and quality of life
Supplemental material, sj-docx-1-hpq-10.1177_13591053251409606 for Individual and group computerized cognitive training for community-dwelling older adults: A quasi-experimental study investigating effects on cognition, mental health, and quality of life by Radka Bužgová, Renáta Zeleníková, Radka Kozáková and Katka Bobčíková in Journal of Health Psychology
Footnotes
Author note
In accordance with the International Committee of Medical Journal Editors guidelines, all authors meet the authorship criteria, and all authors are in agreement with the manuscript.
Ethical considerations
The study was carried out according to the provisions of the Declaration of Helsinki and was approved by the Ethics Committee of University of Ostrava of University of Ostrava (no. 14/2020).
Consent to participate
All subjects gave their informed consent to inclusion before participating in the study. Each participant was assigned a number, ensuring anonymity throughout the study. Informed consent forms and questionnaires only referenced these assigned numbers rather than participant names or identifying data.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Ministry of Health, Czech Republic (grant AZV MZ ČR no. NU21-09–00067).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.