
Abstract
Colorectal and lung cancers are among the most common and deadly worldwide, often carrying significant stigma—especially when linked to preventable behaviors like drinking and smoking. Alcohol increases colorectal cancer risk, while smoking is the primary cause of lung cancer, leading to perceptions of self-infliction that can worsen distress, delay diagnosis, and hinder treatment. This study is the first to compare the acceptability of smoking versus drinking in cancer contexts. Using a factorial design, 132 community members and 126 healthcare professionals evaluated 72 scenarios varying by cancer type, behavior levels, diagnosis stage, post-diagnosis behavior, and activity level. Overall, drinking was viewed as more acceptable than smoking, especially among those physically active or who quit post-diagnosis. Healthcare professionals were slightly more accepting than the general public. Notably, stigma around smoking lessened at advanced cancer stages. Findings suggest the need for stigma-reducing interventions and more compassionate, nonjudgmental care in oncology settings.
Introduction
Worldwide, colorectal cancer and lung cancer are among the most prevalent and deadly cancers, with colorectal cancer annually accounting for almost 2 million new cases and lung cancer affecting nearly 2.5 million people each year (Ferlay et al., 2024; Hirsch et al., 2017; Rawla et al., 2019). Both cancers are associated with significant physical and psychological burdens, including anxiety, depression, and stigma, which can severely impact patients’ quality of life (Esser et al., 2018; Hamann et al., 2018; Li et al., 2025; Lim et al., 2024; Mi et al., 2025; Siwik et al., 2022). Stigma, defined as a discrediting attribute that marks someone as different, often leads to a spoiled identity, characterized by feelings of inferiority and social undesirability (Goffman, 2018; Webb et al., 2019). This stigma is particularly pronounced in cancers perceived to be linked to preventable behaviors, such as alcohol consumption and tobacco smoking (Grauman et al., 2024; Lebel et al., 2013; Scharnetzki and Schiller, 2021).
Alcohol consumption is a well-established risk factor for colorectal cancer, with approximately 17% of cases attributable to alcohol use (Connor, 2017; Islami et al., 2018). Similarly, tobacco smoking is the leading cause of lung cancer, contributing to the public perception that these cancers are self-inflicted (Hirsch et al., 2017; Rigney et al., 2021; Williamson et al., 2020a). This perception fosters stigmatizing attitudes, which can exacerbate psychological distress and delay diagnosis and treatment (Carter-Harris et al., 2014; Cataldo et al., 2012; McLaughlin-Barrett and Brunelli, 2021; Williamson et al., 2020a). For instance, patients with colorectal cancer may face stigma due to beliefs that their cancer was caused by alcohol consumption or an unhealthy diet, while lung cancer patients often encounter blame for their smoking history (Chapple et al., 2004; Wang et al., 2015).
Stigma surrounding alcohol use and tobacco smoking not only affects patients but also influences public and healthcare professionals’ attitudes. Studies have shown that individuals with high alcohol use or smoking habits are often stigmatized, leading to barriers in seeking help and treatment (Gutierrez et al., 2020; Schomerus et al., 2011; van Boekel et al., 2013). Both health professionals and the general public tend to view these behaviors negatively, with more severe stigma directed toward those with higher levels of consumption or dependence (Diaz et al., 2022; Dschaak and Juntunen, 2018; Studts et al., 2024). This stigma can manifest as social exclusion, blame, and devaluation, further isolating patients and worsening their psychological well-being (Link and Phelan, 2006; Weiss et al., 2006; Xu et al., 2025).
Given the detrimental effects of stigma on cancer patients, understanding the factors that influence public and professional judgments about alcohol and tobacco use is crucial. This study aims to compare acceptability judgments regarding alcohol consumption and tobacco smoking in the context of cancer, using an experimental method based on the Functional Theory of Cognition (Anderson, 2014; Kpanake et al., 2018). The Functional Theory of Cognition is directly relevant to this study because it provides a framework for understanding how individuals integrate multiple pieces of information when making judgments (Anderson, 2014). It supports the factorial design and the scenario method, allowing to explore how different cancer-related and behavioral factors combine to shape acceptability judgments. By examining how factors such as consumption levels, post-diagnosis behavior, and cancer stage influence these judgments, this research seeks to identify profiles of patients most at risk of stigmatization. The findings may help to deepen the understanding of stigma related to alcohol and tobacco consumption in cancer (Kirby, 2020; Ostroff et al., 2022).
This study builds on previous research that has explored stigma in both colorectal and lung cancer patients, using scenarios to assess acceptability judgments among community members and health professionals (Auriol et al., 2023a, 2023b). While these prior studies focused on identifying factors shaping participants’ judgments, the current study examines whether participants hold similar or differing acceptability judgments regarding smoking and alcohol consumption for patients with cancer—a question that has not been previously explored. By comparing the acceptability of alcohol and tobacco use in these contexts, this study aims to provide a comprehensive understanding of the factors driving stigmatization and to highlight potential paths for reducing its impact on cancer patients.
Materials and methods
Transparency and openness promotion
The data used in this study were drawn from two datasets available from the Zenodo database (accession numbers https://doi.org/10.5281/zenodo.7525614 and https://doi.org/10.5281/zenodo.7900049). These datasets have been previously analyzed in studies examining factors influencing the acceptability of smoking for patients with lung cancer and the acceptability of alcohol consumption for patients with colorectal cancer (Auriol et al., 2023a, 2023b), respectively.
Participants
Participants were recruited through targeted advertisements on social media, as well as via the authors’ professional networks, personal contacts, and snowball sampling. Regarding social media, advertisements were shared via Instagram® and Facebook® lifestyle groups, while health professionals were recruited through LinkedIn® and Facebook® healthcare worker groups. Those who responded to the advertisements were contacted via private messaging on these platforms. Individuals who consented to participate were enrolled in the study by one of the authors (CA or AP), both of whom were Ph.D. students and certified psychologists. All individuals who volunteered to participate were included, and every participant completed the study in full. All protocols were conducted in the presence of one of the authors, which ensured complete participation and no attrition. The study included adult participants of all ages and genders residing in France. Health professionals represented various occupations, including nurses, paramedical professionals, medical doctors, nurse assistants, and health executives. Participation was voluntary and uncompensated, and all responses were anonymized. The study protocol was in accordance with the Helsinki Declaration and approved by the local ethics committee (Comité d’Ethique de la Recherche de l’Université de Toulouse, File Number 2021-363) and the Data Protection Officer of Université de Toulouse-Jean Jaurès. All participants provided written informed consent. Data collection took place between October 2021 and May 2022.
Material
Experimental design
Participants were presented with the experimental material consisting of scenarios describing the health-related habits of fictitious 60-year-old women. These women were either recently diagnosed with colorectal cancer (alcohol context) or lung cancer (smoking context). The scenarios were constructed based on a factorial design following standard procedures (Anderson, 2014), ensuring an orthogonal combination of the following 4 factors with their respective levels: 1- “Behavioral habits” had 2 levels: (1) lower consumption or (2) higher consumption; 2- “Type of diagnosis/prognosis” had 3 levels: (1) pretumoral lesions that may not turn into cancer but require follow-up, (2) early-stage cancer with life expectancy greater than several years, or (3) advanced cancer with life expectancy no greater than several months; 3- “Post-diagnosis behavior” had 3 levels: (1) quits smoking/drinking, (2) thinks about quitting, or (3) continues smoking/drinking; 4- “Physical activity” had 2 levels: (1) physical exercise or (2) sedentary lifestyle. The exhaustive combination of these factors (orthogonal crossing) resulted in the following factorial design: 2 × 3 × 3 × 2 = 36 scenarios for each context, covering all possible combinations of factors and levels. The alcohol and smoking contexts were comparable, as both incorporated similar factorial designs with parallel factors and levels. For instance, for the “Behavioral habits” factor, lower alcohol consumption (1 drink/day) corresponded to lighter smoking (1–2 cigarettes/day), while higher consumption (5–6 drinks/day) aligned with heavier smoking (20 cigarettes/day). This factorial structure followed the Functional Theory of Cognition (Anderson, 2014), which provides a framework for systematically varying factors to model how individuals integrate multiple sources of information when making acceptability judgments.
The rationale for studying these four factors and their specific levels has been detailed in previous publications (Auriol et al., 2023a, 2023b). Briefly, these factors were chosen for their potential influence on how individuals diagnosed with cancer are perceived. Two of them relate directly to consumption behaviors: smoking and drinking habits, as well as changes in behavior following a diagnosis. Smoking was categorized as light (1–2 cigarettes/day) or heavy (20 cigarettes/day), reflecting differences in stigma and health risks, with heavier smoking doubling the likelihood of health complications (Hackshaw et al., 2018). Similarly, drinking was classified as occasional (one drink per day) or heavy (several drinks per day), based on research indicating greater stigmatization of heavy drinkers compared to moderate ones (Dschaak and Juntunen, 2018). The second factor, behavior change after diagnosis, included three categories: continuing the behavior, considering quitting, or quitting altogether. These align with the stages of change of the Transtheoretical Model of Behavior Change—precontemplation (no intention to change), contemplation (awareness of the issue), and maintenance (sustained behavioral change; Prochaska and DiClemente, 1983). Previous studies suggested that individuals who continue smoking or drinking post-diagnosis are judged more harshly than those who quit (Cataldo et al., 2010). The third factor was cancer type and prognosis, as different stages of cancer are associated with varying levels of psychological distress (Eichler et al., 2018). The fourth factor was physical activity versus a sedentary lifestyle, given that exercise benefits cancer patients and is considered protective against colorectal cancer, while sedentariness is viewed as an avoidable risk (Avancini et al., 2020; Clinton et al., 2020).
Example scenarios
Alcohol scenario: “Elisabeth is a 60-year-old woman, working as an office employee. Elisabeth enjoys physical exercise and, during her free time, she attends a walking club twice a week. For the last 30 years, Elisabeth has been having a daily consumption of 5-6 drinks of alcoholic beverages. She tried several times to quit drinking, without success. For the past three weeks, she has been experiencing abdominal pain with diarrhea and bleeding. She thus undertook a medical evaluation. The medical results showed the presence of polyps. These lesions will require a follow-up, so that they do not turn into colorectal cancer. She thus makes an appointment for a follow-up consultation. A few weeks later, Elisabeth continues to drink. Likewise, she continues to spend her leisure time as she did before.”
Smoking scenario: “Anne is a 60-year old woman, working as an office employee. Anne enjoys physical exercising and, during her free time, she goes in a walking club twice a week. For the last 30 years, Anne has smoked 20 cigarettes daily. She tried several times to quit smoking, without success. For the past three weeks, she experienced shortness of breath and coughing spell. She thus undertook medical evaluation. The medical results showed pre-tumoral lung lesions. These lesions will require a follow-up, so that they do not turn into lung cancer. She thus makes an appointment for a follow-up consultation. A few weeks later, Anne continues to smoke. Likewise, she continues to spend her leisure time as she did before.”
Procedure
Each scenario was printed on a separate sheet of paper. Below each story, participants were asked the following question: “Taking into account all these elements, according to you, does this individual behave in an acceptable manner?.” Responses were collected on an 11-point (non-numerical) scale ranging from “Not at all acceptable” to “Totally acceptable.” The procedure followed two phases (Anderson, 2014), detailed in previous reports (Auriol et al., 2023a, 2023b). In Phase 1 (familiarization), participants reviewed nine randomly selected scenarios, rated their acceptability, and adjusted responses as needed. In Phase 2 (experimental), they rated 36 alcohol-related scenarios followed by 36 smoking-related ones, without comparison or clarification. Finally, participants answered questions about sociodemographic data (age, gender, marital status, education, and occupation). After data collection, participants were categorized into either the health professional sample or the community sample based on whether or not they worked as health professionals.
Data preparation and statistical analysis
Data were screened for missing values and outliers to account for potential invalid responses. Comparisons between means were performed using paired t-tests. Statistical significance was set at p < 0.05. Given the number t-tests conducted (10), a Bonferroni correction was applied to control for multiple comparisons, setting the adjusted significance threshold at p < 0.005 (0.05/10). Both the tables and the Results section indicate which findings remained significant after correction. Analyses were conducted using IBM SPSS Statistics 26.
Results
Participants characteristics and descriptive statistics
The sociodemographic characteristics of the health professional sample or the community sample have been previously reported (Auriol et al., 2023b). Briefly, the community sample consisted of 132 individuals (62% women, mean age = 35.45, SD = 15.60, range 18–85), while the health professional sample included 126 participants (70% women, mean age = 38.37, SD = 12.29, range 22–72).
The mean acceptability judgments were 6.30 (SD = 1.89) in the community sample and 6.91 (SD = 1.54) among health professionals. A t test (t = −2.83, p = 0.005) revealed a statistically significant difference between these two means. Within the community sample, the mean acceptability judgments were 6.41 (SD = 1.87) for women and 6.12 (SD = 1.92) for men, with no statistical difference between them (t = 0.85, p = 0.40). Among health professionals, the mean acceptability judgments were 6.90 (SD = 1.55) in women and 6.97 (SD = 1.52) in men, also showing no significant difference (t = −0.21, p = 0.83). The effect of participants’ educational level on acceptability judgments was examined. ANOVA analyses revealed no significant differences in acceptability judgments across education levels in either the community sample (p = 0.99) or the health professional sample (p = 0.18), despite slight variations in mean ratings.
Comparing acceptability of tobacco and alcohol across various scenarios
A series of t-tests were conducted to compare acceptability judgments of tobacco and alcohol consumption across different scenarios in the community sample (Table 1). After applying a Bonferroni correction (adjusted significance threshold = 0.005), significant differences emerged in several contexts, with alcohol generally being rated as more acceptable than tobacco. This trend was observed in scenarios involving physical exercising (t = −3.84, p < 0.001), lower consumption (t = −4.40, p < 0.001), pretumoral lesions (t = −3.49, p < 0.001), and continued consumption (t = −4.52, p < 0.001). The effect sizes were small (Cohen’s d = 0.13–0.19). Two scenarios showed effects at the uncorrected threshold but did not survive the Bonferroni adjustment: early cancer (t = −2.78, p = 0.006) and thinking about quitting (t = −2.57, p = 0.010), suggesting trends but not strong evidence of differences after correction. In contrast, participants rated quitting smoking more favorably than quitting drinking, and this difference remained significant after correction (t = 2.96, p = 0.004), indicating a small but reliable preference for quitting tobacco. No significant differences were observed in sedentary lifestyle, high consumption, or advanced cancer scenarios (p > 0.05), suggesting similar acceptability perceptions for tobacco and alcohol in these contexts.
Descriptive statistics and mean comparison using t test of acceptability judgments for tobacco or alcohol consumption in the community sample (n = 132).
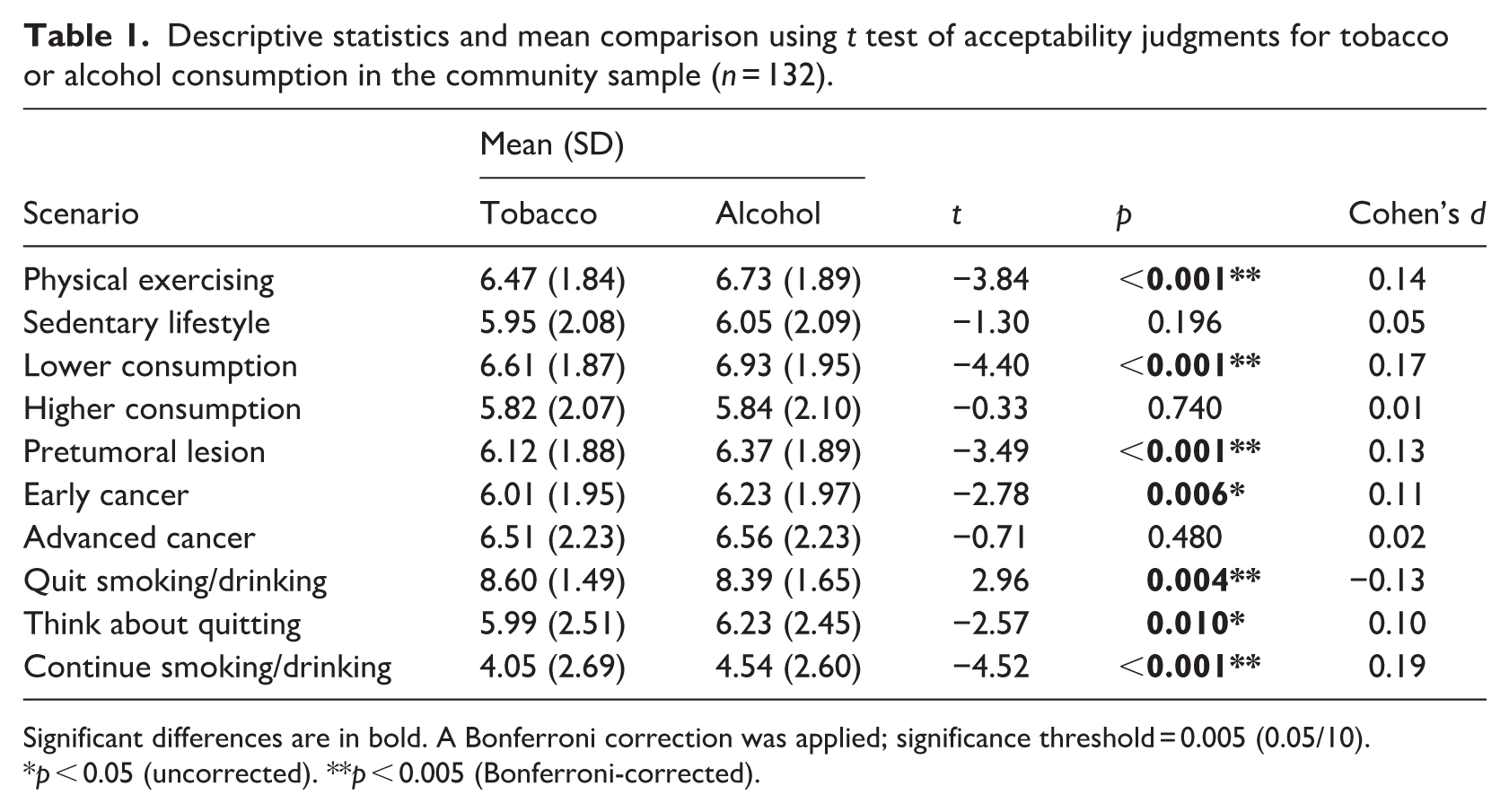
Significant differences are in bold. A Bonferroni correction was applied; significance threshold = 0.005 (0.05/10).
p < 0.05 (uncorrected). **p < 0.005 (Bonferroni-corrected).
The results from the health professional sample indicated significant differences in acceptability judgments between tobacco and alcohol consumption across various scenarios (Table 2). Overall, alcohol was consistently rated as more acceptable than tobacco. This pattern was particularly strong in scenarios involving physical exercising (t = −5.67, p < 0.001, d = 0.26), lower consumption (t = −6.87, p < 0.001, d = 0.37), pretumoral lesions (t = −5.57, p < 0.001, d = 0.30), and early cancer (t = −6.21, p < 0.001, d = 0.28), all of which remained significant after Bonferroni correction, with small to moderate effect sizes. Alcohol was also deemed more acceptable in the sedentary lifestyle scenario (t = −4.71, p < 0.001, d = 0.20), contemplating quitting (t = −4.07, p < 0.001, d = 0.18), and especially in the continued consumption scenario (t = −7.17, p < 0.001, d = 0.35), which showed one of the largest effect sizes. In contrast, the higher consumption scenario (t = −2.86, p = 0.005, d = 0.11) and quitting smoking/drinking scenario (t = 2.49, p = 0.014, d = −0.14) reached significance at the uncorrected level but did not survive Bonferroni adjustment, indicating weaker evidence for these differences. No significant difference was found in the advanced cancer scenario (p = 0.07, d = 0.08), indicating similar levels of acceptability for both substances in this context. The effect sizes across the significant comparisons suggest that while the differences are meaningful, they generally fall within the small to moderate range.
Descriptive statistics and mean comparison using t test of acceptability judgments for tobacco or alcohol consumption in the health professional sample (n = 126).
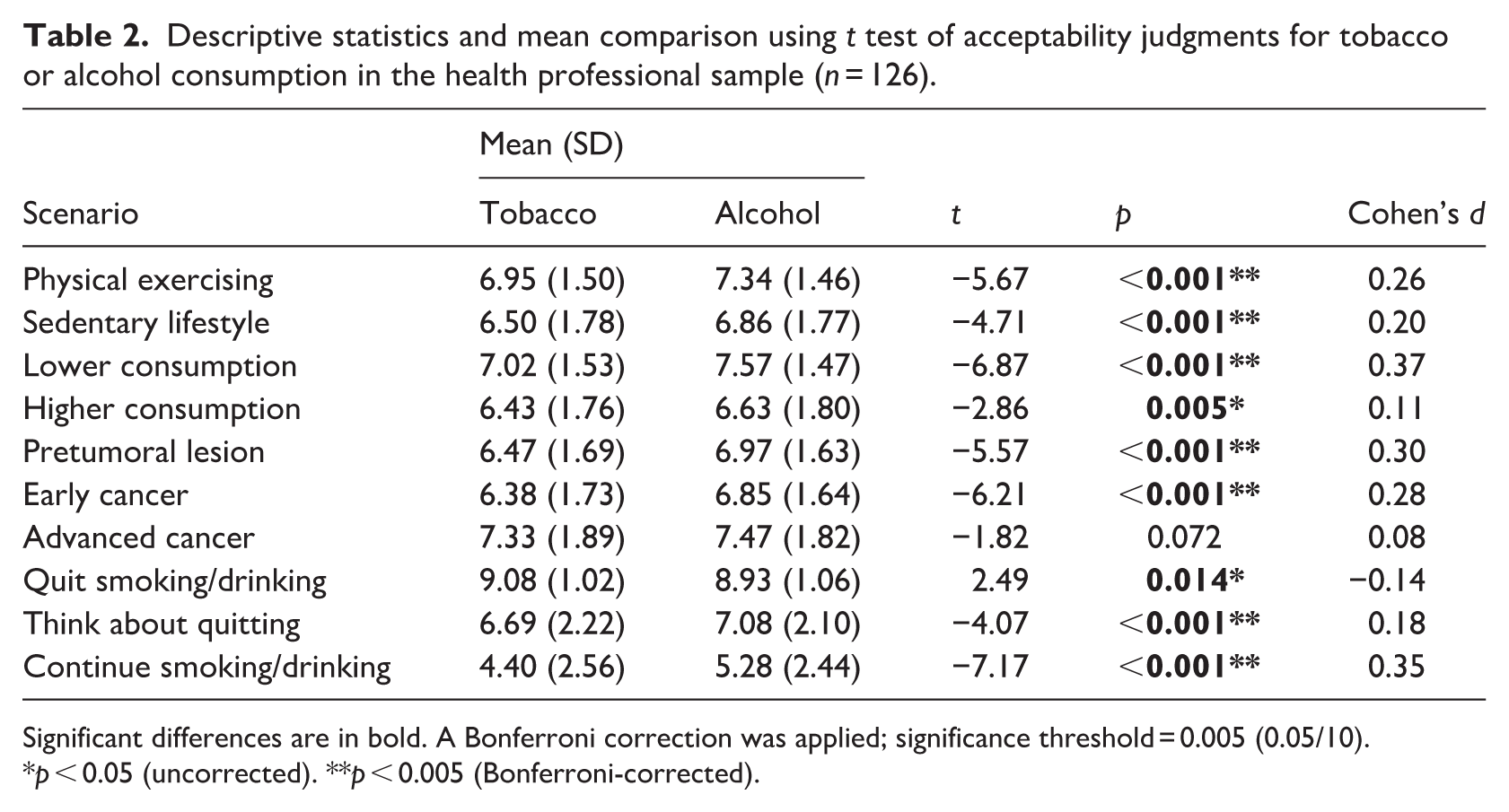
Significant differences are in bold. A Bonferroni correction was applied; significance threshold = 0.005 (0.05/10).
p < 0.05 (uncorrected). **p < 0.005 (Bonferroni-corrected).
Discussion
The findings of this study, which, to our knowledge, is the first to directly compare the acceptability of smoking and drinking in the context of cancer, highlight key differences in how alcohol consumption and tobacco smoking are perceived. Overall, both community members and health professionals rated alcohol consumption as more acceptable than smoking, but this pattern was not uniform across all contexts. This suggests a general disparity in how these behaviors are socially and morally judged, consistent with previous research indicating that tobacco use is heavily stigmatized due to its strong causal link with lung cancer and the widespread public health campaigns against smoking (Kirby, 2020; Riley et al., 2017).
A significant aspect of the findings is that acceptability judgments varied depending on factors such as consumption levels, physical activity, and post-diagnosis behavior. Participants were more lenient toward individuals engaging in lower consumption and physical exercise, and this was consistently significant in both samples, whereas continued substance use after diagnosis resulted in lower acceptability ratings. However, scenarios involving higher consumption showed no significant differences in the community sample and only a weak, non-significant trend among professionals after correction. This suggests that individuals who attempt to modify their behaviors post-diagnosis are perceived more favorably, highlighting the role of personal responsibility in shaping stigma. The FTC provides a useful lens for interpreting these findings, as it posits that judgments depend on the functional relevance of information in specific contexts (Anderson, 2014). In this study design, factors such as consumption habits, lifestyle, and post-diagnosis behavior were selected because they represent dimensions that individuals draw upon when evaluating the acceptability of health-related behaviors. The observed tendency to rate individuals more favorably when they reduced consumption or engaged in physical activity is consistent with the FTC assumption that judgments reflect the perceived adaptive value of behaviors, particularly in relation to notions of responsibility and prognosis.
One of the key methodological strengths of this study lies in its well-controlled experimental design, which ensures that the scenarios for alcohol consumption and tobacco smoking are directly comparable. Both contexts were structured using the same factorial design, incorporating parallel factors and levels, such as consumption habits, post-diagnosis behavior, cancer stage, and lifestyle factors. This methodological symmetry allowed for a rigorous comparison between the two substances, ensuring that any observed differences in participant judgments were attributable to the nature of the substance itself rather than variations in scenario structure. By maintaining this consistency, the study minimized confounding variables and enhanced the validity of the findings, while providing a strong foundation for drawing meaningful conclusions about the differences in societal acceptability of alcohol and tobacco use in the context of cancer.
Interestingly, both community members and health professionals exhibited overall similar patterns in their judgments, though professionals tended to rate behaviors as slightly more acceptable. However, professionals also showed stronger and more consistent differences in several scenarios (e.g. sedentary lifestyle, contemplating quitting), whereas some effects in the community sample (e.g. early cancer, thinking about quitting) did not remain significant after Bonferroni correction. This may reflect professional’s greater exposure to cancer patients, leading to more nuanced or empathetic perspectives. However, healthcare professionals may still hold implicit biases—unconscious attitudes or stereotypes—that could subtly influence their interactions with patients and the treatment recommendations they provide. For instance, if smoking is perceived as more blameworthy than alcohol consumption, a lung cancer patient who smokes might receive less empathy or different guidance compared to a colorectal cancer patient who drinks.
The observed preference for smoking cessation over alcohol cessation suggests a differential stigma, where tobacco use is viewed as more blameworthy and requiring urgent cessation. This aligns with previous research indicating that smokers often face strong moral condemnation, even from nurses and healthcare professionals (McLaughlin-Barrett and Brunelli, 2021; Studts et al., 2024; Wang et al., 2015; Williamson et al., 2020b). Given that smoking is perceived as a voluntary behavior, smokers are frequently seen as responsible for their illness, resulting in heightened blame and stigma (Bresnahan et al., 2013; Marlow et al., 2015; McLaughlin-Barrett and Brunelli, 2021; Williamson et al., 2020b). This moral judgment reflects the belief that smoking-related diseases are largely preventable, distinguishing smoking from other health behaviors. However, prior to this study, no research had directly compared perceptions of smokers with those of individuals who consume alcohol.
The finding that acceptability ratings of drinking or smoking did not significantly differ from each other in advanced cancer cases suggests that social stigma associated with these behaviors might diminish as the disease progresses to a severe stage. This observation aligns with the notion that the social judgment individuals face regarding behaviors like smoking or drinking may become less prominent when the focus shifts away from moral or personal responsibility and toward survival. The primary concern in advanced cancer stages is no longer about the person’s past choices but rather their immediate health and well-being, although this remains a subject of ongoing research and is not yet definitively supported by findings in the literature.
Limitations
Despite these insights, this study has several limitations. First, the use of hypothetical scenarios may not fully capture real-world attitudes and behaviors. Second, the study was conducted in France, and cultural differences in alcohol and tobacco perceptions may limit generalizability to other populations. In the French context, cultural norms, public health messaging, and prevailing attitudes toward alcohol and tobacco differ from those in many other countries. For example, alcohol consumption is often socially normalized in France, which could influence perceptions of alcohol-related stigma compared to countries with stricter drinking norms (Bocquier et al., 2017). Therefore, replication in other cultural settings is needed to assess the generalizability of these results. Finally, this study focused on acceptability judgments from community members and health professionals rather than on patients’ lived experiences or clinical outcomes. Future research should investigate how such judgments translate into patient experiences—such as distress, treatment avoidance, or help-seeking—in order to clarify the clinical relevance of stigma.
Conclusion
Overall, the findings contribute to a deeper understanding of cancer-related stigma and highlight the need for targeted efforts to address the differential judgments placed on alcohol and tobacco use. Notably, both community members and health professionals rated alcohol consumption as more acceptable than smoking, suggesting that alcohol-related stigma may be less pronounced than that associated with tobacco use in cancer care. While these differences are relatively small, they point to potential paths for further investigation. Further research is needed to explore how these varying perceptions may influence patient well-being and healthcare experiences, which could ultimately inform the development of interventions aimed at reducing stigma and fostering more supportive, nonjudgmental approaches to alcohol and tobacco use in cancer care.
Footnotes
Acknowledgements
The authors are grateful to participants for their time and efforts. CA was supported by a fellowship program from Institut National du Cancer and Institut pour la Recherche en Santé Publique (INCa_15747 SPADOC20-02).
Ethical considerations
The study protocol was in accordance with the Helsinki Declaration and approved by the local ethics committee (Comité d’Ethique de la Recherche of Toulouse University, File Number 2021-363) and the Data Protection Officer of the University of Toulouse.
Consent to participate
All participants provided written informed consent.
Consent for publication
Participants were informed that the anonymous data collected in this research may be made available to the scientific community, particularly as part of article submissions to scientific journals.
Author contributions
CA: Conceptualization, methodology, funding acquisition, investigation, data curation, formal analysis, writing – review & editing. PR: Conceptualization, supervision, data curation, formal analysis, writing – original draft & editing. AP: Investigation, writing – review & editing. NC: Conceptualization, methodology, supervision, formal analysis, writing – review & editing. All authors approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CA was supported by a fellowship program from Institut National du Cancer and Institut pour la Recherche en Santé Publique (INCa_15747 SPADOC20-02).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All the data from this study are available and can be accessed at https://doi.org/10.5281/zenodo.7525614 and ![]()
Grant number
INCa_15747 SPADOC20-02