
Abstract
Systemic Lupus Erythematosus (SLE) is a prevalent chronic autoimmune disease, with about 5 million cases worldwide. This study aimed to understand the meanings attributed to illness by individuals with SLE. A national mixed-methods study was conducted with an exploratory focus. Data were collected online from 663 Brazilian adults through a sociodemographic questionnaire and the Free Association of Ideas Technique. Lexical analysis was performed using IRaMuTeQ, identifying four thematic classes: (1) Challenges and Coping Efforts in Daily Life with Lupus, (2) Physical Repercussions of Illness, (3) Resilience and Resistance in Coping with the Disease, and (4) Emotional and Psychological Repercussions of Illness. Results reveal how SLE affects various life dimensions, physical, emotional, and social and highlight coping mechanisms such as faith, strength, and acceptance. The study emphasizes the relevance of psychosocial support and the need to address social determinants of health to promote well-being among individuals with SLE.
Keywords
Introduction
Systemic Lupus Erythematosus (SLE) is a chronic, inflammatory, and multifactorial autoimmune disease, characterized by a broad spectrum of clinical manifestations, diverse symptomatology, and heterogeneous disease behavior (Siegel and Sammaritano, 2024). Due to its multisystemic involvement, SLE produces not only physical repercussions but also psychological and social impacts (Char et al., 2024). Individuals living with the condition face a range of challenges, including debilitating symptoms, treatment side effects, and restrictions imposed by the illness, which directly affect their quality of life and perception of the disease (Petrocchi et al., 2022). According to the World Lupus Federation (World Lupus Federation, 2023), it is estimated that approximately 5 million people worldwide live with lupus, while the Brazilian Society of Rheumatology (2021) reports about 65,000 cases in Brazil.
In Brazil, SLE affects individuals across a wide range of age groups and presents significant challenges for the lives of those who have the disease as well as for the organization of healthcare services. The disease is closely linked to major social inequalities and inequities, highlighting the structural vulnerabilities present within Brazilian society (Brazilian Society of Rheumatology, 2021). In this context, the impact of SLE is further intensified by the unequal distribution of risk factors and limited access to specialized care, reflecting the broader social complexities in which the disease is embedded.
This reality underscores the role of the Social Determinants of Health, understood as a set of biological, economic, cultural, and social factors that directly influence the health–illness continuum. Elements such as race, gender, income, and access to healthcare services significantly shape individuals’ life trajectories and their experiences of illness. These conditions are mediated by broader economic, social, and political forces that contribute to the perpetuation of inequalities and have a profound impact on both individual and collective health (Melo et al., 2024a; Sajjadi et al., 2022).
Given this context and the distinct trajectory of chronic illnesses, it is essential to understand how individuals with SLE assign meaning to their health-illness process and to the broader context of their condition. Understanding these lived experiences and meaning-making processes enhances the recognition of protective factors and provides a solid foundation for empathetic, person-centered care and for the development of effective health policies and interventions tailored to people living with SLE.
The significance of this study lies in the scarcity of research that explores the experiences of individuals with SLE from their own perspective. Although previous research has documented the mental health burden associated with systemic lupus erythematosus (SLE), the most widely cited and highly sought systematic reviews have primarily concentrated on the biological and clinical aspects of the disease, particularly regarding diagnosis and treatment strategies (Barber et al., 2021; Fanouriakis et al., 2021; Fava and Petri, 2019; Gurevitz et al., 2013; Siegel and Sammaritano, 2024). These investigations recognize the importance of psychological factors but prioritize biomedical outcomes—which are indeed of great importance, considering that SLE is a medical condition. However, the subjective and qualitative dimension of living with SLE, including how people deal emotionally with the diagnosis and manage daily challenges, does not seem to have received the same priority in the published literature. Addressing this aspect is essential, as these factors can directly influence treatment adherence and symptom management.
In response to the growing demand for scientific production that enriches international databases and informs decision-making regarding multi-professional interventions in the healthcare of individuals with chronic diseases, this study aimed to identify the meanings attributed to illness by people with Systemic Lupus Erythematosus (SLE).
Methods
Research design
This study employs a mixed-methods design with a national scope, implemented in a complementary manner (Barbieri et al., 2023; Creswell and Creswell, 2021). The rationale for this methodological choice is its capacity to provide a more comprehensive understanding of complex phenomena, such as health, through the integration of distinct data collection instruments (Domínguez et al., 2024).
Participants
A non-probabilistic convenience sample of 663 Brazilian participants diagnosed with Systemic Lupus Erythematosus and aged over 18 years was recruited. Participants without internet access or who were illiterate were excluded. A diagnosis of lupus and being 18 years of age or older were established as inclusion criteria, encompassing individuals of both sexes and with varying educational levels. This type of recruitment was chosen because lupus is a low-prevalence condition in the general population, which makes probabilistic sampling unfeasible at a national level. Online recruitment through specific groups made it possible to reach a larger number of participants and, consequently, to maximize access to individuals willing and able to contribute to the study.
This study was conducted in accordance with international recommendations for qualitative research, particularly the Consolidated Criteria for Reporting Qualitative Research (COREQ), which guide the transparent and systematic reporting of qualitative designs (Tong et al., 2007). The COREQ checklist is provided in Supplemental File 1.
With regard to sample adequacy, the final sample size was established after the predefined data collection period. Based on the quantity and richness of the material obtained, the researchers verified that the narratives no longer added new or substantive information to the emerging categories. Therefore, thematic saturation was used as a post-hoc validation criterion (Saunders et al., 2017), supporting the adequacy of the final sample and the robustness of the analyses and interpretations presented.
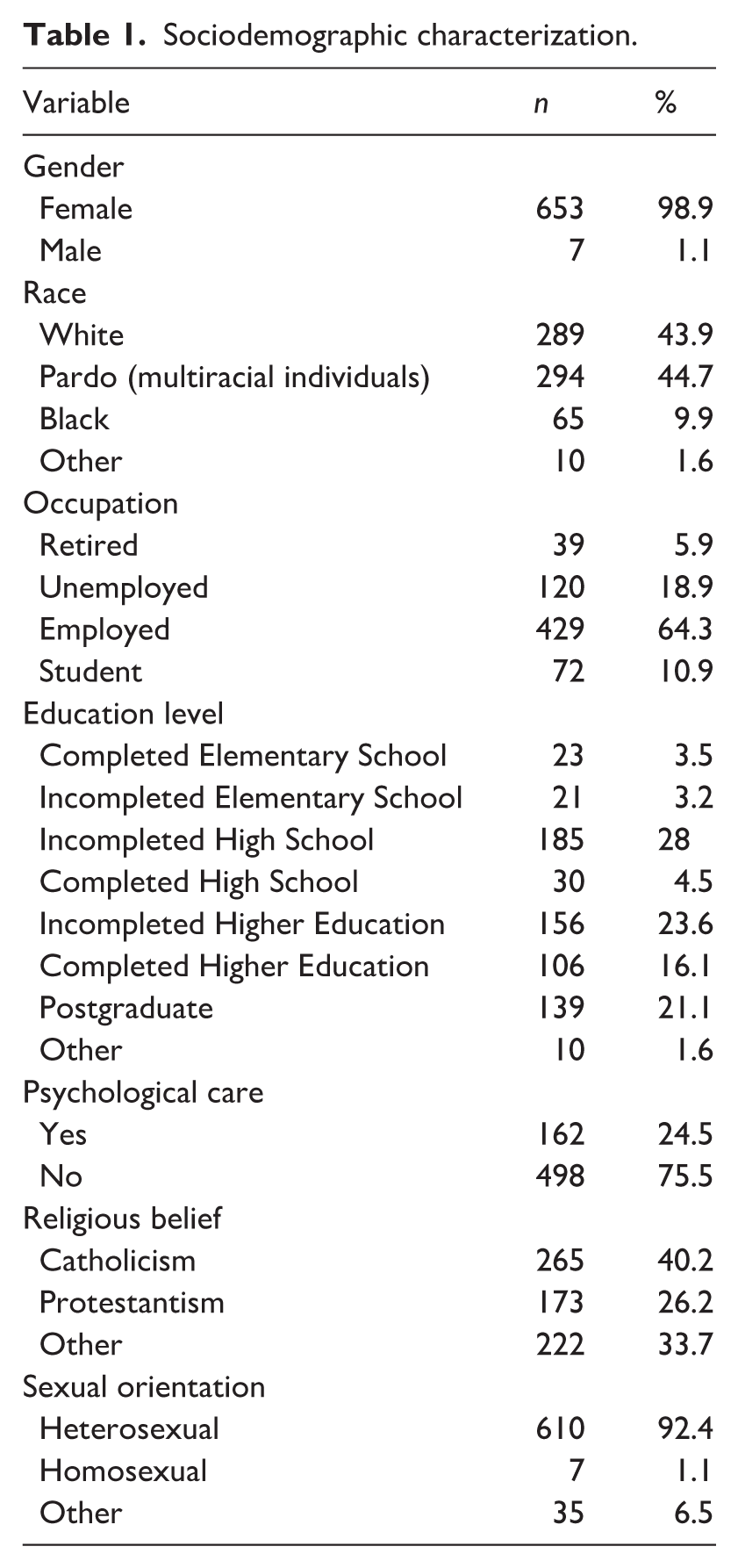
Sociodemographic data revealed that participants had a mean age of 34.2 years (SD = 10.4). The majority were female (98.9%, n = 653), heterosexual (92.4%, n = 610), identified as mixed-race individuals (referred to in Brazil as pardos, an official census category that designates people of mixed European, African, and Indigenous ancestry; 44.7%, n = 294) professed the Catholic faith (40.2%, n = 265), did not receive psychological support (75.5%, n = 498), had a monthly income of 1–3 minimum wages (35.9%, n = 237), and were formally employed (42.4%, n = 280; see Table 1).
Sociodemographic characterization.
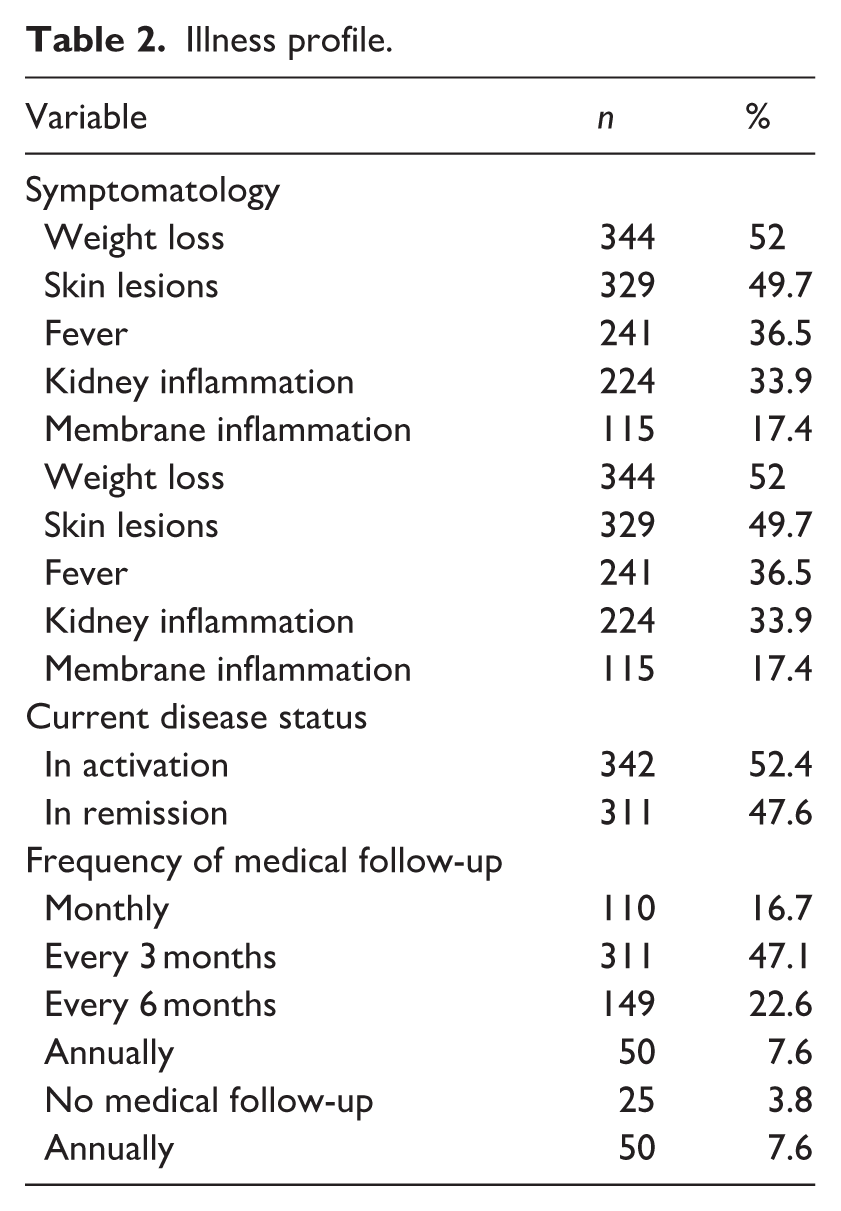
Regarding the characterization of the sample concerning SLE aspects, it was observed that the majority of participants reported being in the active phase of the disease (52.4%; n = 342). Concerning symptoms, the most prevalent were joint pain (85.3%, n = 565), weight loss (52%, n = 344), and cutaneous lesions (49.7%, n = 329; see Table 2).
Illness profile.
Data collection and instruments
Data collection was conducted in two distinct stages. In the first stage, participants completed a sociodemographic questionnaire designed to gather information on biological and identity variables, such as age group, age at lupus diagnosis, sex, and sexual orientation. Social aspects, including education level, occupation, family income, ethnicity, and religious belief, were also addressed, alongside clinical variables such as frequency of medical follow-up, psychological care, and symptomatic manifestations of SLE.
In the second stage, the Free Association of Ideas Technique (FAIT) was employed as a methodological instrument to investigate subjective representations of living with lupus. FAIT is an adaptation of the Word Association Technique (WAT), allowing for greater freedom of verbal expression and expanding possibilities for discursive elaboration. This is particularly useful in contexts where participants may have language limitations, low educational attainment, or emotional burden (Almeida, 2018). In this study, the inductive stimulus used was “Lupus,” and participants were asked to express the ideas, sensations, or images that emerged from these words. This approach facilitates the apprehension of symbolic and affective meanings related to the experience of illness.
Procedure
A questionnaire, comprising the aforementioned instruments and the necessary Free and Informed Consent Form (FICF), was developed. This questionnaire was hosted on an online survey platform and subsequently disseminated through closed groups or communities on social media platforms dedicated to individuals with SLE. The form had an average completion time of 10 minutes and was accessible for 1 month, between June and July 2024. Respondents were able to participate in the research autonomously and complete the instruments individually, self-administered, and anonymously.
Data analysis
The analyses were carried out in five stages: the first using Jamovi software (v.2.3), and the others with the support of the Interface de R pour les Analyses Multidimensionnelles de Textes et de Questionnaires (IRaMuTeQ). The main purpose of this program is to analyze the structure and organization of discourse, enabling the identification and visualization of relationships among the lexical fields most frequently mobilized in the analyzed documents (Camargo and Justo, 2013). Each of the analyses performed is described below:
Step 1 – Descriptive sociodemographic statistics
Sociodemographic data were analyzed using descriptive statistics (frequencies, percentages, measures of central tendency, and dispersion) in Jamovi (v.2.3), in order to characterize the sample and contextualize the textual findings.
Step 2 – Frequent terms
The narratives obtained through the Free Association of Ideas Technique (FAIT) comprised the textual corpus processed in IRaMuTeQ. We first extracted the absolute frequencies of the most recurrent terms in the statements and presented them in a table (e.g. “fear,” “pain,” “sadness,” “faith,” “strength,” etc.), to provide a direct view of the predominant lexicon in participants’ representations.
Step 3 – Classical lexicographic analysis
Next, we performed a classical lexicographic analysis, which provides global corpus statistics such as the number of forms/lemmas, hapax (words occurring only once), segmentation into Elementary Context Units (ECUs), and the classification/use rate of ECUs for subsequent analyses. These indicators are essential for assessing the quality of the material and the consistency of data processing. In the literature, a classification rate of ⩾75% of ECUs is considered satisfactory (Camargo and Justo, 2013).
Step 4 – Descending Hierarchical Classification (DHC)
The corpus was segmented into ECUs and subjected to Descending Hierarchical Classification (DHC), based on Reinert’s method. This procedure groups ECUs according to shared vocabulary, using the chi-square test (χ2) to assess the strength of association of each word with the emerging content classes. Only words with χ2 ⩾ 3.84 (p < 0.05) were retained, ensuring statistical significance and discarding weak associations. Thus, DHC goes beyond identifying word frequencies, functioning as a hypothesis-testing procedure that produces statistically consistent lexical classes.
The results of DHC are presented in the form of content classes, which reflect the predominant semantic contexts in participants’ responses. Each class brings together ECUs that share a specific vocabulary distinct from the other classes, forming clusters of meaning that approximate the central themes of the research: understanding the subjective experience of living with the disease. Consequently, the number and structure of content classes emerge from the textual data itself rather than from the evaluator’s subjectivity, thereby reducing potential bias in the process.
After class extraction, the results were subjected to complementary qualitative analysis based on Bardin’s (2016) Content Analysis. In this step, researchers examined the lexical groupings in detail, naming them according to their predominant semantic content and interpreting their meanings. This process involved the three phases described by Bardin: (1) pre-analysis, with reading and organization of the material; (2) exploration, with identification of meaning axes; and (3) treatment and interpretation, with synthesis and discussion of results. In this way, the statistical objectivity of the DHC was combined with the interpretive depth of qualitative analysis, allowing for an integrated understanding of the meanings attributed by participants in their representations of illness.
Step 5 – Specificity analysis
Finally, we conducted a Specificity Analysis in IRaMuTeQ, which identifies words statistically most associated with sociodemographic subgroups (e.g. sex, age, time since diagnosis). This procedure enabled comparisons between groups and revealed distinctive linguistic features in the analyzed representations, thereby contributing to a deeper understanding of the different meanings attributed to illness.
Ethics approval
This study received ethical approval from the Research Ethics Committee of University of Fortaleza, under opinion number 75771423.6.0000.5052.
Results
Frequent terms
This section presents the most frequent terms found in the participants’ narratives. The main ones were: Fear (f = 251), Pain (f = 181), Sadness (f = 127), Faith (f = 72), Strength (f = 63), Anxiety (f = 58), Death (f = 42), Tiredness (f = 42), Life (f = 42), Anguish (f = 42).
To enhance comprehension, Table 3 presents these words and their respective frequencies.
Frequent terms.
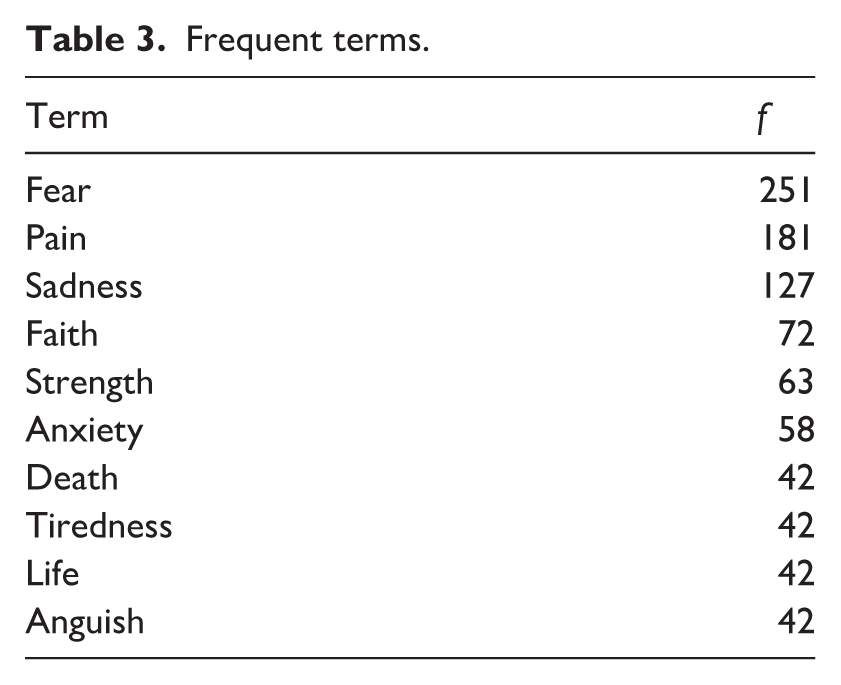
These words suggest that the experience of living with SLE is primarily characterized by feelings of fear, sadness, and anxiety. However, beyond physical and emotional suffering, expressions of coping also emerged, such as strength, faith, and life. Daily life aspects like pain and tiredness were also present, alongside the importance of family relationships and care. In this sense, the overall set of words may indicate that SLE profoundly affects the lives of individuals who have the disease, requiring adaptation and the mobilization of both internal and external resources.
Classical lexicographical analysis and descending hierarchical classification
The overall corpus was segmented into 627 text segments (TS), with 497 TS (79.27%) being utilized. A total of 3,854 occurrences (words, forms, or vocabulary items) emerged, comprising 762 distinct words and 692 with a single occurrence. The analyzed content was categorized into four classes: Class 1, “Challenges and Coping Efforts in Daily Life with Lupus”, with 80 TS (16.7%); Class 2, “Physical Repercussions of Illness” with 127 TS (26.6%); Class 3 “Resilience and Resistance in Coping with the Disease” with 141 TS (29.5%); and Class 4 “Emotional and Psychological Repercussions of Illness” with 129 TS (27.04%).
To better visualize these classes, a dendrogram was generated, displaying the word list for each class based on chi-squared (χ2) testing. This representation demonstrated evocations that exhibited similar vocabulary within their respective classes and distinct vocabulary from other classes (see Figure 1).
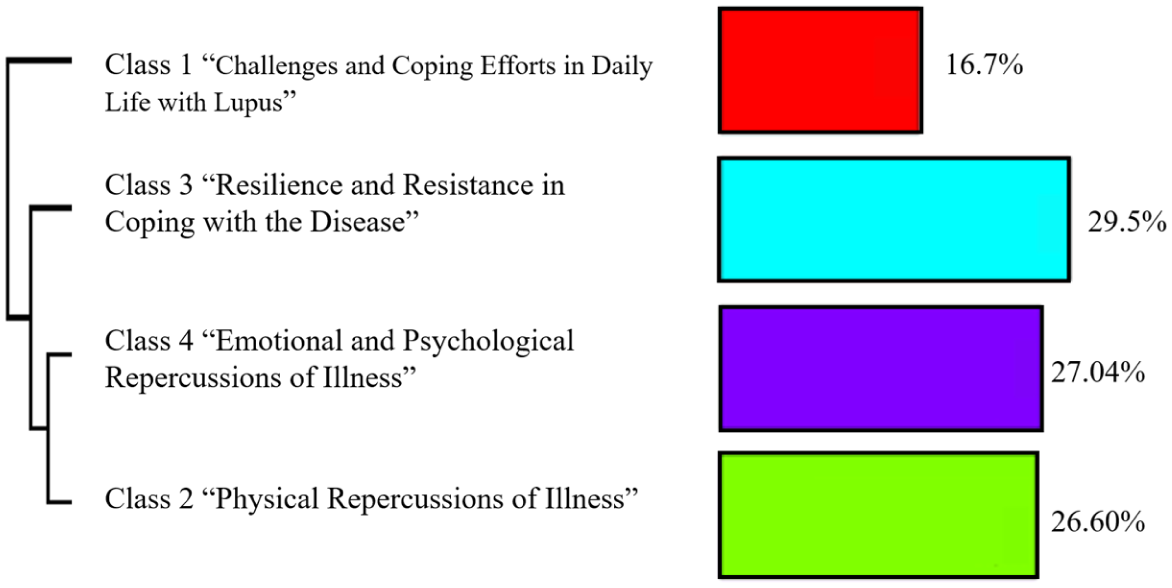
Dendrogram of classes emerged from the DHC.
Hereafter, each of the classes identified through the Descending Hierarchical Classification will be described, exemplified, and operationalized.
Class 1 – “Challenges and Coping Efforts in Daily Life with Lupus”
This class comprises 16.7% (f = 80 TS) of the total corpus analyzed. It is constituted by words and stems within the χ2 interval of 44.36 (Difficult) to 5.09 (Live). This class includes words such as “Difficult” (χ2 = 44.33); “Strength” (χ2 = 35.49); “Faith” (χ2 = 32.04); “Care” (χ2 = 30.15); “Diagnosis” (χ2 = 25.07); “Achieve” (χ2 = 25.07); “Want” (χ2 = 24.19), “No” (χ2 = 20.01); “Help” (χ2 = 20.01); and “Still” (χ2 = 20.01).
The words highlighted above primarily focus on emotional and psychological aspects related to the challenges, difficulties, and life changes experienced by participants. Terms like “Difficult” and “Still” suggest resistance and obstacles when confronting the illness and its repercussions, as demonstrated by participants through expressions such as “It’s difficult to digest and move forward,” “They are constant challenges, it’s difficult to live content with pain,” and “I still have to adapt to things I loved doing before the diagnosis but can’t do as before anymore.”
The word “No” may convey participants’ expressions regarding the negatives and limitations imposed by the disease, in addition to suggesting an inability to cope with the diagnosis, as articulated in expressions like “I’m lost, I don’t know how to live with this diagnosis,” “I feel like I can’t do what I need to,” and “I’m afraid of not being able to achieve my dreams, not being able to be a mother or have a normal life.”
Furthermore, words such as “Faith,” “Strength,” “Care,” “Help,” and “Achieve” reveal coping efforts that coexist with the difficulties imposed by the disease. Rather than simply expressing optimism, these terms highlight participants’ attempts to adapt and maintain continuity in the midst of suffering. For example, references to “Faith” and “Strength” often appear in contexts where individuals acknowledge their limitations but also emphasize the inner resources that allow them to persevere. Similarly, “Care” and “Help” point to the importance of support systems and healthcare practices as means of dealing with the diagnosis, while “Achieve” and “Want” suggest a desire to pursue goals and maintain agency despite constraints. Taken together, these words illustrate that coping with lupus is not limited to enduring its challenges but also involves active strategies to seek support, mobilize internal resources, and sustain everyday life.
Class 2 – “Physical Repercussions of Illness”
This class comprises 26.6% (f = 127 TS) of the total corpus analyzed. It is constituted by words and stems within the χ2 interval of 79.72 (Death) and 2.47 (Joint). This class includes words such as “Death” (χ2 = 79.72); “Medicine” (χ2 = 42.13); “Pain” (χ2 = 38.71); “Sun” (χ2 = 38.31), “Lack” (χ2 = 32.38), “Fatigue” (χ2 = 23.14), “Hair” (χ2 = 17.55), “Cure” (χ2 = 17.30), “Medication” (χ2 = 16.74), and “Swelling” (χ2 = 16.74).
The occurrences in this class represent the experience of illness and are strongly associated with how individuals with SLE understand their own health, focusing on the physical aspects and the medical context of treatment routines, as reflected in occurrences directly related to the experience of the illness (e.g. “medicine,” “medication”). The presence of occurrences referring to the symptomatology of the illness, such as “pain,” “fatigue,” and “swelling” also verifies that the symptoms and characteristics of the disease are frequent and strongly associated with the experience of living with the diagnosis.
Finally, important terms like “Sun,” “Hair,” and “Lack” also express the practical and emotional implications arising from the physical changes brought on by the illness, as portrayed in expressions like “I don’t leave the house because of the Sun,” “I have a lack of self-esteem due to bodily changes, like hair loss,” and “I can’t be in the sun.”
Class 3 – “Resilience and Resistance in Coping with the Disease”
This class comprises 29.5% (f = 141 TS) of the total corpus analyzed. It is constituted by words and stems within the χ2 interval of 57.9 (Resilience) and 2.24 (Understanding). This class includes words such as “Resilience” (χ2 = 57.90), “Love” (χ2 = 44.24), “Courage” (χ2 = 41.96), “Overcoming” (χ2 = 36.47), “Perseverance” (χ2 = 26.83), “Family” (χ2 = 25.27), “Patience” (χ2 = 22.80), “Learning” (χ2 = 21.85), “Hope” (χ2 = 21.42), and “Acceptance” (χ2 = 20.35).
From the words grouped in this class, it was possible to verify a tendency to represent human qualities that drive the resolution or confrontation of obstacles. In this sense, these occurrences evoke positive emotions and denote a tone of hope and optimism when facing the need to deal with the challenges and limitations imposed by the illness.
Class 4 - “Emotional and Psychological Repercussions of Illness”
This class comprises 27.04% (f=129 TS) of the total corpus analyzed. It is constituted by words and stems within the χ2 interval of 121.74 (Sadness) and 2.4 (Expense). This class includes words such as “Sadness” (χ2 = 121.74); “Fear” (χ2 = 110.00); “Anxiety” (χ2 = 88.58); “Anguish” (χ2 = 57.68); “Loneliness” (χ2 = 37.29); “Discouragement” (χ2 = 32.35); “Uncertainty” (χ2 = 24.65); “Frustration” (χ2 = 21.95); “Worry” (χ2 = 16.85); and “Anger” (χ2 = 14.40).
The words mentioned above represent an uncomfortable mental or emotional state. Generally, they describe distinct nuances of physical or emotional discomfort, conveying a sense of dismay, sorrow, and affliction, exemplified by the words “sadness,” “anguish,” and “fear.”
Specificity analysis
Through specificity analysis, it was possible to conduct comparisons and descriptions of the evocations (considering the frequency of word incidence and their hypergeometric indices/χ2) across various collected variables such as sex, age, monthly income, occupation, race/ethnicity, religious belief, and engagement in psychological care.
Regarding participants’ age, the most frequent responses in the younger groups (up to 28 years old) referred to negative emotional aspects stemming from illness (e.g. “worry,” “anxiety,” “depression”). The same pattern was observed in the group of participants aged 29–59 years (“death,” “fatigue,” “crying”). Conversely, the most prevalent responses in the older participant group (above 60 years old) depicted aspects related to acceptance (e.g. “power,” “perseverance,” “acceptance,” and “love”).
Concerning psychological care, participants who engage in it frequently reported words related to adaptation (e.g. “resilience,” “struggle,” and “learning”). Conversely, responses from the group not undergoing psychological care concentrated on expressions of vulnerability and suffering (e.g. “lack,” “illness,” and “discouragement”).
Regarding the variable of race/ethnicity, the response pattern expressed by the group of White participants more frequently referred to a more hopeful conception of diagnosis and treatment (e.g. “overcoming,” “treatment,” “care,” “life,” “acceptance”). In contrast, responses from Black participants expressed uncertainty and vulnerability (e.g. “death,” “insecurity,” “dying,” “suffering,” and “limitation”).
Concerning the variable of monthly income, it was observed that participants with lower incomes (up to 1 minimum wage) expressed responses referring to sensations of loss and fragility (e.g. “crying,” “dying,” “suffering,” “discouragement”). For participants whose income was concentrated around 5 to 10 minimum wages, the response pattern centered around words related to hope and the existence of possibilities (“care,” “limitation,” “family,” “change,” “medicine”). Conversely, participants with higher incomes (more than 15 minimum wages) expressed responses referring to strength, relief, restoration, and perceived control (e.g. “power,” “cure,” “care,” “resilience,” and “struggle”).
Discussion
Overall, the results indicate that a lupus diagnosis significantly impacts various dimensions of individuals’ lives, encompassing psychological, physical, and social aspects, as analyzed in this research through a qualitative approach. The findings reflect diverse perspectives related to coping with the disease, revealing both the challenges and the strategies developed by individuals to manage the condition. It can be observed that some of the words mentioned in the questionnaire, such as “fear,” “pain,” and “sadness,” highlight the prevalence of feelings of vulnerability, suffering, and uncertainty when facing the complexity of the disease. In this sense, these expressed feelings illustrate the emotional and psychological challenge that accompanies the diagnosis and daily lives of individuals with chronic diseases (Martínez et al., 2023; Melo et al., 2024b).
In the Descending Hierarchical Classification analysis, four classes emerged. The first of these – “Challenges and Coping Efforts in Daily Life with Lupus” – it was possible to identify words that characterize impediments and restrictions stemming from the condition, portrayed through expressions such as “never,” “no,” “achieve,” and “difficult.” These words may highlight daily limitations experienced by individuals, who frequently face significant routine changes due to the condition’s side effects. Regularly, individuals confronting chronic illnesses encounter the need to abandon pleasurable activities and even work tasks, owing to the limitations imposed by the disease. This reality demands not only cognitive restructuring and greater psychological flexibility regarding daily habits (Zukerman et al., 2023) but also continuous, multi-professional support that assists and addresses the individual’s psychological, social, and physical dimensions, while also considering the chronic pain experienced by these individuals (Bosma et al., 2024; Melo et al., 2024b).
The second class, termed “Physical Aspects, Symptomatology, and Side Effects,” addresses the physical dimension of illness. This dimension is detailed through categories such as “swelling,” “pain,” “weakness,” “fever,” and “fatigue,” in addition to representing individuals’ perception of undergoing treatments imposed by the diagnosis, as seen in words like “exam,” “medication,” “medicine,” “hospital,” and “hospitalization.” Given this, it is fundamental to understand the broad symptomatic manifestation of SLE, which can include cutaneous lesions, joint pain, weight loss, inflammation in membranes and mucous membranes, among others (Petrocchi et al., 2022). In this sense, the constant presence of symptoms can imply a significant impairment in individuals’ quality of life, as it affects well-being and self-esteem through perceived beauty and the reduction of the body’s functional capacities (Char et al., 2024).
The third class, “Resilience and Resistance in Coping with the Disease” – pertains to positive and optimistic aspects regarding individuals’ adaptive capacity when facing illness. In this class, terms with an empowering nature emerged concerning the challenges imposed by an SLE diagnosis (e.g. strength, faith, resilience, courage). Given that the diagnosis of a disease challenges and threatens the psychological balance of individuals with SLE, it is understood that hope, an optimistic expectation about the future, constitutes a coping resource characterized as emotion-focused coping, referring to the attempt to regulate the emotional impacts of illness on the individual (Cornet et al., 2022). Furthermore, resilience is understood to strengthen individuals’ self-management, in addition to involving interrelationships and influencing illness management. In this sense, an individual with prominent resilience is more capable of actively participating in their health-disease process, dealing positively and proactively with the adversities and challenges that arise throughout treatment (Han et al., 2021; Kim et al., 2019).
Regarding the last class – “Emotional and Psychological Repercussions of Illness” – this is related to the subjective aspects present in the health-disease process, exemplified by terms such as “sadness,” “anguish,” and “loneliness.” This can be explained by the fact that any illness generates emotional and psychological repercussions to some degree for the afflicted individual. Such manifestations involve conflicts, ambiguous feelings, states of hypersensitivity, and behavioral changes, stemming from the relationships the individual develops with their illness, treatment, and hospitalization (Straub, 2023). Thus, feelings like guilt, fear, sadness, or insecurity are part of the painful emotional aspects that accompany the diagnosis and/or worsening of a chronic illness (Azfaruddin and Rini, 2023).
Upon analyzing participants’ responses, it is noteworthy that perceptions regarding coping with the condition vary substantially according to sociodemographic variables. Markers such as age and the respondents’ social context allow for greater insight into the contrasts observed in participants’ response patterns concerning living with the illness. Thus, while some reports focus on negative and limiting aspects, others point to elements reflecting a tenor of overcoming and hope, denoting greater resilience in dealing with the stress arising from the condition (DeQuattro et al., 2024). In this sense, words like “faith” and “strength” emerge as symbolic representations of optimism and the development of positive strategies for managing the challenges of the diagnosis.
Through the Specificity Analysis, it was found that regarding participants’ age, the response pattern of younger groups displayed a more emotionally challenging character, exemplified by expressions such as “anxiety” and “depression.” This contrast can be elucidated by understanding that adolescence is a period of intense physical and emotional transformations, capable of amplifying the impact of diagnosing a chronic disease like lupus. Thus, experiencing illness during a phase marked by the search for adaptation and emotional instability can add additional challenges for adolescents in managing the condition (Boris et al., 2024). The oscillating nature of SLE, characterized by periods of remission and activation, demands not only constant adaptations but also adequate support from professionals who can assist with treatment adherence and contribute to the quality of life and psychosocial maturation of younger individuals (Melo et al., 2024b).
In contrast, the perception of the older group tends toward a perspective of acceptance regarding the illness, illustrated by the words “acceptance” and “perseverance.” This can be elucidated through the concept of resilience, which refers to the acquired ability to confront and sustain adversity. In this sense, resilience is a competence developed throughout life and is presented as the result of numerous experiences lived and accumulated over time. These experiences include adverse situations, struggles, health problems, and considerable losses. Thus, in old age, the likelihood that an individual has already faced challenging events is significantly higher than in youth, which can contribute to building a more balanced and mature perspective when confronting difficulties during moments of fragility and tribulation, such as the diagnosis and living with SLE (Asnis, 2021).
Furthermore, regarding the variable of psychological care, it is inferred that the group undergoing it exhibits discourse oriented toward appropriating the experience of the diagnosis, evoking terms such as “struggle” and “learning.” Conversely, the group not receiving psychological care expresses vocabulary that alludes to a certain psychological and emotional fragility, such as “discouragement” and “lack.” Psychological support can play a fundamental role in restructuring how individuals perceive, feel, and think about their experience with illness (Ezawa and Hollon, 2023). Situated within the biopsychosocial context, psychology offers theoretical and practical tools to promote not only emotional coping but also cognitive adaptation to the disease, contributing to the construction of a more functional relationship with treatment and the daily challenges imposed by the condition. In this sense, psychological intervention aims to reframe adverse experiences, reduce distress associated with disease unpredictability, and strengthen individual autonomy (Martinez-Calderon et al., 2024).
Regarding race/ethnicity, White participants evoked words demonstrating greater access to resources – “treatment” and “care” – in contrast to Black participants, whose vocabulary depicted insecurity, expressed, for example, in “death” and “dying.” This can be understood in light of the long history of slavery in Brazil, which contributed to the formation of what is termed structural racism, intricately involved in maintaining exploitative relations and precarious working conditions (Santos et al., 2024). In Brazil, it is emphasized that Black individuals still predominantly occupy positions of lower prestige and remuneration. In this sense, it is understood that healthcare practices often reproduce systems and concepts previously conceived by the social body, with living and working conditions being determinant in access to resources in the face of needs imposed by illness (Silva et al., 2023). In this context, through the lens of the social determination of mental health, the multifaceted dynamism of the social production of health is recognized, and it is understood that mental health, in adverse and illness-related contexts, does not result exclusively from individuals’ capacities. By moving beyond this simplistic understanding, the social and structural differences that shape each experience become evident (Melo et al., 2024a).
Concerning income, it is observed that participants in greater financial vulnerability demonstrate significant distress when mentioning terms like “crying,” “discouragement,” and “suffering.” However, the group with considerably higher purchasing power provides responses characterized by a sense of control and restoration, such as “cure,” “care,” and “power.” When discussing health, it is understood that individuals’ socioeconomic context is a decisive factor in their degree of vulnerability to illness, with socially vulnerable populations being the most affected by its repercussions. This is due both to insufficient resources or access to health services and the absence of everyday prevention and treatment strategies, further hindered, for example, by precarious employment ties (Khanna et al., 2022).
In this conjuncture, it becomes pertinent to deeply consider the social, economic, and environmental conditions and their influential reverberations on collective and individual health. Such conditions, marked by social determinants of health, include factors such as income, education, housing, basic sanitation, and access to quality services. The relationship between these determinants and health is direct; that is, individuals in precarious living conditions typically experience worse health outcomes. Conversely, individuals with better socioeconomic conditions are associated with improved results concerning the treatment and management of chronic illnesses (Sajjadi et al., 2022).
In this context, it is fundamental to reaffirm that individuals with greater purchasing power have enhanced access to quality healthcare services, enabling them to invest in appropriate care, in addition to greater access to health promotion information and resources. Conversely, individuals in situations of socioeconomic vulnerability frequently encounter significant barriers, such as difficulty accessing medical care and exposure to inadequate environments. All of these factors lead to a greater propensity for an increased risk of illness (Khanna et al., 2022).
In addition to the aspects already discussed, the high prevalence of joint pain (85.3%) reported by participants deserves attention. This symptom, often chronic and disabling, directly impacts quality of life, functional limitations, and treatment adherence, being considered one of the main clinical challenges in the management of lupus (Petrocchi et al., 2022). The persistence of pain highlights shortcomings in the provision of care, particularly within public health systems (Char et al., 2024), and reinforces the need for multidisciplinary approaches that encompass not only pharmacological interventions but also self-care strategies, physical therapy, and psychosocial support.
Aggravating this problem, the absence of psychological follow-up was observed in 75.5% of participants. Given that the results revealed feelings of sadness, fear, anxiety, and loneliness as central meanings of the experience with lupus, the lack of psychological support constitutes a significant gap in comprehensive health care, which remains restricted to biomedical assistance (Silva and Bicudo, 2022; Straub, 2023) and is strongly marked by the social determination of mental health (Melo et al., 2024a). Conversely, the presence of psychological care can favor the re-signification of the disease, expand coping resources, and reduce negative emotional impacts (Ezawa and Hollon, 2023; Martinez-Calderon et al., 2024). The coping strategies developed through such care play an essential mediating role between subject, health, and illness, directly influencing treatment adherence and quality of life (Melo et al., 2024a). This scenario points to the need for expanding public policies that integrate psychological support as part of the routine care of people with chronic diseases, in line with the biopsychosocial model of health care.
This study presents some limitations that must be acknowledged. First, data collection was conducted exclusively online, which means that individuals without access to the internet or to the questionnaire were unable to participate. It is important to note that limited internet access is often linked to social and financial vulnerability, which restricts our ability to capture the perspectives of this population in particular. In addition, the methodological choice of the Free Word Association Technique imposes inherent restrictions. While this strategy is effective for mapping collective symbolic representations, it does not allow for an in-depth exploration of personal experiences and meanings related to living with lupus, since the participants provide only fragments of their perceptions through their evocations.
Furthermore, the results cannot be generalized beyond the specific context of this study. The research was conducted in Brazil, a country marked by significant social inequalities, structural barriers in healthcare access despite a universal public health system, and vast regional differences that strongly shape individuals’ experiences. Therefore, the representations captured here may not reflect the reality of individuals in other sociocultural contexts. Finally, most participants were women, which, while consistent with the higher prevalence of lupus in females, limited our ability to adequately explore the perspectives and experiences of men living with the disease.
Conclusion
This research allowed for the identification of meanings attributed by individuals with Systemic Lupus Erythematosus (SLE) to their illness experience, revealing a complex interplay of feelings, challenges, and coping strategies related to the diagnosis. In this sense, it was observed that SLE profoundly impacts individuals’ lives, generating emotional, physical, and social implications. Despite the difficulties imposed by the disease, elements of resilience and resistance were also evident, highlighting participants’ capacity for adaptation and overcoming in the face of this chronic condition.
Therefore, the importance of conducting new studies that explore the meanings of illness in more diverse groups is reinforced, including longitudinal designs to monitor possible changes in perceptions over time. Future studies could also delve deeper into the role of variables such as social support, access to healthcare, and psychological follow-up in coping with the disease.
This study contributes to the scientific literature by providing an opportunity for individuals with SLE to report their experiences, feelings, and coping strategies. The findings presented here can inform more humanized and individualized interventions, as well as guide healthcare professionals in formulating public policies that consider the biopsychosocial aspects of illness, thereby promoting more effective and sensitive care tailored to the real needs of individuals with SLE.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261417514 – Supplemental material for Fear, faith, pain, and strength: Meanings attributed to systemic lupus erythematosus by Brazilian patients – A mixed-methods study
Supplemental material, sj-docx-1-hpq-10.1177_13591053261417514 for Fear, faith, pain, and strength: Meanings attributed to systemic lupus erythematosus by Brazilian patients – A mixed-methods study by Ícaro Moreira Costa, Juliana Morais Gurjão, Nicole Campos Pontes, Luis Eduardo Pontes Luna, Maria Clara da Rocha Brito and Cynthia de Freitas Melo in Journal of Health Psychology
Footnotes
Acknowledgements
The authors would like to thank the participants in this study. It was an honor to listen to your experiences.
ORCID iDs
Ethical considerations
This study was approved by the Research Ethics Committee of University of Fortaleza (Brazil) (approval no. 75771423.6.0000.5052).
Consent to participate
All participants provided informed consent prior to participation by digitally agreeing to the Free and Informed Consent Form (FICF). Participation was voluntary, anonymous, and self-administered. Written consent was obtained electronically through the online platform.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Supplemental material
Supplemental material for this article is available online.