
Abstract
This narrative review synthesizes current knowledge on emotional support (ES) in the context of illness. Based on 78 empirical and theoretical studies across psychology, health, and caregiving, it examines diverse populations facing various illnesses (chronic/acute conditions, mental disorders). First, the definitions, characteristics, and theoretical underpinnings of ES are examined, highlighting its heterogeneity and conceptual fragmentation in the literature. The impacts of ES are then explored, including its beneficial effects on patients’ well-being and the emotional cost for caregivers. A novel conceptual model is subsequently proposed that accounts for the bidirectional nature of ES and integrates key components such as emotional availability, recognition, relational balance, and expectations. This model is the first to conceptualize ES specifically within illness contexts, emphasizing its reciprocal dynamics between the patient and the relative. It aims to guide future empirical studies and inform clinical practice by clarifying how ES is perceived, provided, and experienced.
Introduction
Social support is a key process for coping with stressful situations, such as illness (Moss-Morris, 2013). Despite the lack of consensus regarding its definition (Beauregard and Dumont, 1996; Dambi et al., 2018; Gottlieb and Bergen, 2010), some scholars agree that social support can be divided into different types of support, including emotional support (Bruchon-Schweitzer and Boujut, 2021; Rascle, 1994; Vaux et al., 1987). Emotional support (ES) is characterized by expressions of attention, concern, love and interest, particularly at times of stress (Cutrona and Russell, 1990). Nevertheless, several definitions and conceptualizations of ES have been proposed (e.g. Abendroth and Den Dulk, 2011; Bruchon-Schweitzer and Boujut, 2021; Capponi et al., 2013; Wolff et al., 2013), making this field of research vast and slightly opaque.
Receiving ES has been shown to have beneficial effects on both physical and mental health (Georgopoulou et al., 2018). Moreover, it appears to play a key role in the management of sick patients in terms of their satisfaction and remission (Adamson et al., 2012; Bruchon-Schweitzer and Boujut, 2021; Tempier et al., 2013). Despite its apparent importance for health, relatively few studies have examined the consequences of either providing or receiving ES.
To gain a better understanding of ES in the context of illness, a narrative review was carried out. This aimed to clarify (a) the conceptualization and evaluation of ES, (b) the individual who provide ES, and (c) the consequences of giving and receiving ES. This narrative review is based on 78 articles, including both theoretical contributions (e.g. definitions, conceptual models) and empirical studies. These contributions cover a wide range of populations (patients, caregivers, adults, children) and diverse methodologies (qualitative, quantitative, and mixed methods). This heterogeneity reflects the intention to provide an initial broad synthesis of ES in the context of illness and to integrate perspectives rarely examined together. Based on this synthesis of this scientific findings, a model of ES specific to the context of illness was proposed.
Definition, conceptualization, and assessment of emotional support
Definitions of emotional support
ES is rarely explicitly defined. This omission likely reflects the broad and subjective nature of ES, which highlights the challenges in defining it due to the extensive range of behaviors it encompasses and personal interpretations of what constitutes ES (Dambi et al., 2018). Despite this, several definitions have been proposed that vary according to the authors’ field of expertise, the contextual factors surrounding ES provision, and the level of detail involved in its characterization. For example, ES can be broadly defined as any behavior aimed at enhancing a person’s well-being (Abendroth and Den Dulk, 2011), or more specifically, as a set of behaviors that provide comfort, transmit affection, enhance feelings of inclusion, and facilitate adaptation (Barnes and Duck, 1994; Burleson, 2003; Reis, 2001).
Other definitions further clarify the concept of ES by specifying the emotional behaviors involved in its implementation. Burleson (2003) claims that ES consists of assisting a distressed person by listening, empathizing, legitimizing, and actively exploring their feelings. Moreover, some definitions emphasize the effects of ES on the recipient. For example, Capponi et al. (2013) suggest that ES can provide relaxation, consolation, and improved well-being during challenging times through emotional exchange.
This diversity of definitions reflects the interdisciplinary nature of the concept. While not problematic itself, such plurality creates challenges for comparing findings or building shared framework. Any attempt at greater definitional clarity must remain sensitive to epistemological diversity and to the subjective meaning that individuals assign to ES.
Despite these variations, most definitions converge on a common understanding of ES as a form of aid provided in situations where the recipient faces difficulties or challenges that require the provider to deploy emotional behaviors and expressions to support them. Thus, in the context of illness, ES is crucial.
Conceptualizations of emotional support
Going beyond the variability in its definition, the challenge of conceptualizing ES remains significant. To our knowledge, no theoretical model focuses specifically on ES, particularly in the context of illness. However, several models provide relevant insights into the role of ES in stress adjustment, social relationships, and interpersonal interaction. The models presented below, which are not exhaustive, follow an order that progresses from the general to the more specific regarding the concept of ES.
The concept of social support
ES is fully integrated into the concept of social support as a crucial component. Social support is generally defined as the perception or experience of being cared for, esteemed, and part of a mutually supportive social network (Taylor, 2011). This concept, which was formalized in the 1970s, was developed to explore how interpersonal and community relationships impact mental and physical health. Social support is conceptualized as a multidimensional construct that encompasses several types of support, although classification differs across authors (Barrera and Ainlay, 1983; Cutrona and Russell, 1990).
Pioneers such as Cassel (1976) and Cobb (1976) investigated how support from social networks could both enhance health and moderate the effects of stress. Subsequently, extensive research has produced diverse and sometimes contradictory findings, which has contributed to the complexity and heterogeneity in how ES is defined and operationalized (Barrera and Ainlay, 1983). For instance, some studies have shown that social support significantly buffers stress and improves health outcomes (Capponi et al., 2013; Cassel, 1976), while others have found no such effects or have even reported negative consequences (Cherba et al., 2019; Heller et al., 1986). This variability reflects the complexity of social interactions and the multiple ways in which ES can manifest, which have impacted its study and application across different contexts.
Transactional model of stress and coping
The transactional model of stress and coping (Lazarus and Folkman, 1984) provides a framework for understanding how individuals respond to stressful situations. Within this model, ES is conceptualized as a perceived resource, but also as a coping strategy, given that people may actively seek ES. Perceived social support, particularly ES, is an essential resource that helps individuals feel more equipped to manage stress. It specifically refers to the individual’s perception of the ES that is available for them, such as the belief they can rely on their family to provide reassurance and comfort in times of need. During a primary appraisal of the stressful situation, an individual assesses the perceived stress and its potential impact. In the secondary appraisal, they evaluate the available resources, including social support. This evaluation will allow the individual to develop coping strategies to face the situation. Thus, they may seek ES by sharing their emotions with family members or close others to receive comfort. According to Muller and Spitz (2003), ES involves handling a stressful situation by seeking moral support, sympathy, and understanding.
Conceptualization of social support by Bruchon-Schweitzer and Boujut (2021)
More recently, Bruchon-Schweitzer and Boujut (2021) clarified social support theory by synthesizing various studies and frameworks. Their framework defines social support as comprising three components: the social network, received social support, and perceived social support (Barrera and Ainlay, 1983; Procidano and Heller, 1983; Thoits, 1995).
The social network refers to the structure of an individual’s social relationships, characterized by the number, frequency, and intensity of these relationships. Ultimately, a social network refers to the people a person knows and can communicate with.
Received social support refers to the tangible assistance provided by one’s social network (Winnubst et al., 1988). House (1981) categorized the functions of received social support, specifically emphasizing the role and uniqueness of ES. According to this classification, there are four forms of received social support that manifest in four main ways. First, informational support includes offering advice and knowledge to help solve problems. Second, material support encompasses tangible assistance, such as financial aid and physical resources, provided during challenging times; this form of support can be considered a type of instrumental support (it provides practical and concrete help). Third, esteem support involves affirmations of the receivers’ skills and value, which ultimately enhance their self-confidence. Fourth, emotional support (ES) involves receiving expressions of positive feelings from others (such as trust, friendship, and love), along with behaviors that provide reassurance, protection, and comfort. These last two forms of received social support are closely related because they both involve enhancing an individual’s sense of value and security. Nevertheless, Capponi et al. (2013) emphasize the importance of distinguishing between these four forms of support. Not all are equally appropriate in every context, despite their complementary nature, and their use depends on several factors, such as the context of the situation and the expectations of the recipient.
Finally, the third and last component of social support is perceived social support, which reflects the subjective evaluation of the aid provided by an individual’s social network and the extent to which this individual believes their needs and expectations are met (Procidano and Heller, 1983). This form of support is considered to be the most indicative, as social support is only satisfying if the recipient perceives that the support they receive (or believe they can receive) is adequate relative to their expectations and needs (Sarason et al., 1983). This aspect implies the existence of perceived ES, which is characterized by the individual’s belief in the amount and quality of help they could receive and their overall satisfaction with the support provided (Sarason et al., 1990). Although perceived ES is not explicitly included in Bruchon-Schweitzer and Boujut’s (2021) conceptualization of social support, such inclusion is widely recognized in the literature (Dambi et al., 2018; Gottlieb and Bergen, 2010; Haber et al., 2007). Numerous studies have shown that perceived ES plays a more important role than received ES in health (e.g. Thong et al., 2007). Given the significant role of perceived ES, we argue that it should be incorporated as a subcomponent of perceived social support.
Balance reciprocity model of social support
Although research indicates that perceived ES has a more optimal effect on health than received ES (e.g. Thong et al., 2007), the results are nuanced. Indeed, studies have shown that reciprocal ES, which represents a balance between giving and receiving, is associated with beneficial health outcomes, whereas an imbalance between giving and receiving is linked to less favorable effects (Ingersoll-Dayton and Antonucci, 1988; Keyes, 2002). Furthermore, for ES to be beneficial, it must be both perceived by the recipient and also desired, otherwise its effects can be detrimental (Reynolds and Perrin, 2004; Smith and Goodnow, 1999; Wolff et al., 2013).
Based on the findings of earlier studies, Wolff et al. (2013) tested a new balance reciprocity model of ES among two samples: young adults (23–34 years of age) and the elderly (68–83 years). In their sample of young adults, they identified a quadratic relationship between health complaints and well-being: compared to receiving adequate support, receiving too much or too little support was associated with higher levels of health complaints and negative effects. Wolff et al. (2013) hypothesized that excessive support from family and friends could raise health concerns; in addition, it can also strengthen the receiver’s complaints and thus reduce their well-being due to the negative thoughts generated by the excessive support.
However, among older adults, such patterns were not observed; instead, a negative linear relationship was found between the amount of support received and both health complaints and negative affect. Wolff et al. (2013) hypothesized that because older adults tend to be more stable—emotionally, socially, and physically—they are less affected by unbalanced ES than younger adults. Similarly, they are more likely to expect their relatives to be able to provide ES when they can. These findings are particularly important because they show that the consequences of ES vary with age.
Limitations of emotional support and the impact on evaluation
The various models of social support indicate the understanding of ES is heterogeneous, which has implications for its evaluation. Indeed, few standardized tools measure ES directly and its assessment only appears as a subscale of broader social support, and is often measured with only a few items; for example, see the Multidimensional Perceived Social Support Scale (MSPSS (Dambi et al., 2018)), the Berlin Social Support Scales (BSSS (Schulz and Schwarzer, 2003)), and the Social Support Behaviors Scale (SS-B (Vaux et al., 1987)). Moreover, the distinction between received and perceived ES is rarely addressed in these tools. Hence, these tools are rarely used in studies that specifically focus on ES. Indeed, researchers have constructed specific measures of ES that are tailored to the objectives of their studies. Previous assessments of ES have therefore been proposed according to the specific context (e.g. daily life, illness), the receivers (e.g. adolescents, adults, the elderly), and sometimes to the providers (e.g. Doran et al., 2019; Joo et al., 2020; Pilato et al., 2024). Given this, it is difficult to generalize the findings on ES to a wider range of contexts.
Going beyond the issue of assessing ES, some limitations exist in current models. First, all the theoretical models have focused on adults and the elderly. To date, no model has been designed that represents the ES given and received by children and adolescents. Although ES is beginning to be evaluated in these populations, there is still a need to propose a theoretical model specific to—or including—children and adolescents. Indeed, understanding the dynamics of ES in younger populations could provide valuable insight into its expression and consequences. Second, previous models have focused on ES from the recipient’s point of view, but none consider the provider. This is especially important in the context of illness as providing ES may have positive or negative impacts for the provider. Thus, in the remainder of this article, both the recipient and the provider of ES are considered.
Who provides emotional support and why?
Primary provides of emotional support in illness contexts
ES is primarily provided within the family sphere (e.g. Doran et al., 2019; Georgopoulou et al., 2018; Taylor et al., 2023; Tempier et al., 2013; Wu et al., 2025; Yuan et al., 2021), especially in the context of illness. Indeed, when faced with illness, family members are generally the first and most important source of support for the patient (Untas et al., 2012). Patients often express their feelings and thoughts related to the illness to their relatives (Herbette and Rimé, 2004). However, healthcare professionals and friends also play a significant role in providing ES to patients during illness (e.g. (Adamson et al., 2012; Doran et al., 2019; Georgopoulou et al., 2018; Son et al., 2023; Taylor et al., 2023).
Studies have also shown that individuals living in the same household as the ill person are more likely to offer ES (e.g. Hobson et al., 2006; Richardson et al., 2007). When the ill person is a child or an adolescent, the received support comes from their parents (e.g. Miller and DiMatteo, 2013; Ritchie, 2001), siblings (e.g. Chalhoub et al., 2023; Ritchie, 2001), and peers (e.g. de Beer et al., 2024; La Greca et al., 1995; Son et al., 2023). When the ill person is an adult or elderly person, it has been widely shown that the partner or spouse is one of the main sources of ES (e.g. Richardson et al., 2007; Yuan et al., 2021). ES is also provided by the ill person’s friends (e.g. Doran et al., 2019) and children, regardless of whether they are minors or adults (e.g. Doran et al., 2019; Richardson et al., 2009; Thomas, 2010). These people are known as family caregivers (Schulz and Eden, 2016), who, when under 18 years old, are referred to as “young carers” (Becker, 2000). It is important to note that those who provide ES to an ill person also regularly provide other types of help.
Barriers to the provision of emotional support
However, not everyone will provide ES to someone they know with a health problem. A qualitative study by Ray et al. (2019) explored the factors that determine the provision of ES to an acquaintance/friend/family member with cancer. The researchers questioned why friends, colleagues, and nuclear and extended family members had not provided ES. Some participants reported being unsure of how to react to the disease (e.g. not knowing what to say, or feeling uncomfortable), while others felt unable to provide ES. Similarly, physical distance seemed to be a barrier to providing ES. Other participants considered that the ill person already received enough support, or did not want any support.
While Ray et al.’s (2019) study provides important information on the reasons for providing or withholding ES, it did not explore the relationship between the participants and the ill person. However, numerous studies have shown that physical and emotional closeness to the person in question is a determining factor in the provision of ES, as it influences the ability to offer support within close relationships (Burleson, 2003; Ray et al., 2019). In this sense, ES from loved relatives seems to be the most desired by the person suffering from illness; but what are the consequences for the person receiving the support, and the person providing it?
What are the consequences associated with receiving and providing emotional support?
Positive effects of receiving emotional support
ES has been extensively studied for its beneficial effects on the mental and physical health of the recipient. In the context of illness, some researchers have identified that ES improves mental health and psychological well-being by reducing the impact of perceived stress (Joo et al., 2020; Shaw et al., 2021; Umberson and Montez, 2010); hence, it increases perceived control, which facilitates better adjustment to the event (Bruchon-Schweitzer and Boujut, 2021). Some authors emphasize the significant role of how this support, or the feeling of being supported, is perceived in modulating the stress response (Umberson and Montez, 2010). In this regard, Georgopoulou et al. (2018) showed that a high level of perceived ES from a close individual was associated with better mental health outcomes for the recipient. As previously discussed, these findings underscore the importance of recognizing the perceived ES component within conceptualizations of social support, such as that by Bruchon-Schweitzer and Boujut (2021), to allow for a finer understanding of ES and its challenges.
The positive effects of ES also extend to physical health; ES can indirectly contribute to its improvement. Capponi et al. (2013) demonstrated that tailored ES can significantly reduce perinatal anxiety, positively impacting the overall well-being of both the mother and the child. Furthermore, Seeman et al. (2001) found that individuals who receive a high level of ES had less pronounced physiological stress responses, contributing to better cardiovascular health and a reduction in symptoms of some chronic diseases. Additionally, receiving ES appears to enhance patients’ adherence to therapy. For example, Adamson et al. (2012) showed that patients who perceived they were getting a high quality of ES from caregiving staff expressed greater satisfaction with the care they received; in turn, this can promote better adherence to prescribed treatments and improve clinical outcomes.
Negative effects and conditions undermining emotional support
ES may also have negative impacts, depending on how the support is perceived by the recipient. Wittenberg-Lyles et al. (2014) highlight that when ES is perceived as being invasive or inappropriate, it may increase stress for the receiver rather than alleviate it. This perception can be problematic when the support provider and the recipient do not share a mutual understanding of what constitutes appropriate support. Additionally, when the recipient feels unable to reciprocate the ES they receive, it can lead to feelings of indebtedness, which may negatively affect the relational dynamics and contribute to relational stress (Antonucci and Jackson, 1990).
Some other negative consequences of ES are associated with the relational status between the recipient and the provider. For instance, Silverstein and Bengtson (1994) showed that receiving ES from a child was negatively associated with the parent’s well-being. This may be explained by the fact that receiving ES from a child violates norms associated with the parental role and diminishes the parent’s sense of independence.
Moreover, the quality of ES is crucial to ensuring its positive effects (Schwarzer and Knoll, 2007; Warner et al., 2010). High-quality ES should meet the recipient’s needs. A poor alignment between the support provided and the recipient’s needs can lead to feelings of frustration and misunderstanding, ultimately hindering the potential benefits of ES. Therefore, a complex balance is required between the provider and the receiver. Indeed, this is one of the postulates of social exchange and equity theory (Joo et al., 2020), whereby individuals tend to maintain an interpersonal relationship based on a balance between the cost of giving and the benefits received from the relationship.
Taken together, these findings highlight that it is equally important to consider the impacts of ES on those who offer it, as their experiences can influence the dynamics and outcomes of ES interactions for the receiver (Joo et al., 2020).
Benefits of providing emotional support
Fewer studies have been undertaken on giving ES compared to receiving it, and the results show both positive and negative effects. The literature has primarily focused on the consequences of providing social support in general social interactions. Studies specifically addressing the impact of providing ES within the context of illness are less common. Roach et al. (2021) investigated how adolescents who support a friend with mental health issues perceive their role. The results indicated that providing ES could elicit feelings of validation and usefulness. These observations align with Fuligni (2019), who highlights that the motivation to contribute to others’ well-being emerges during adolescence. Similar findings among older caregivers suggest that providing ES can enhance their well-being by fostering their sense of usefulness, supporting personal goal achievement, and strengthening their social identity, in line with self-determination theory (Deci and Ryan, 2012; Fuligni, 2019; Warner et al., 2010).
Just as the outcomes of receiving ES vary, the experience of providing it can also lead to both beneficial and negative effects. According to social exchange theory, providing ES naturally creates an expectation of reciprocity (Antonucci and Jackson, 1990). In the context of illness, where support is primarily directed toward the ill individual, providers may lack this normally reciprocated support, which potentially leads to an emotional imbalance in the relationship, relational difficulties, and broader negative consequences.
Negative consequences of providing emotional support in caregiving contexts
The negative effects associated with providing ES can also depend on the relational status between the provider and the receiver. For instance, it can be challenging for children to provide ES to their parents (e.g. Warner et al., 2010), especially when the parent is ill (Richardson et al., 2007). This issue is particularly relevant in the context of young carers. For example, Warren (2007) showed that young carers are more likely to provide ES to family members with health problems than non-caregiving peers. Furthermore, interviews with young adult caregivers have shown that providing ES to an ill relative can lead to feelings of burden and emotional exhaustion (Lacombe et al., 2024). Thus, providing ES might require a greater psychological and emotional investment than providing instrumental support (Chevrier et al., 2022; Rahal and Singh, 2024). Indeed, ES often necessitates suppressing one’s own emotions to cater to the needs of others (Lacombe et al., 2024). Adult family caregivers report both positive outcomes (e.g. sense of usefulness, strengthened bonds with the person receiving care) and negative outcomes (e.g. emotional overload, psychological exhaustion) related to their caregiving role, which includes providing ES (Rezaei et al., 2024). Moreover, caregivers’ perceptions of the support they receive themselves play a crucial role in shaping their caregiving experience. Caregivers who perceive they have adequate social support and ES themselves feel better equipped to handle the challenges of caregiving, whereas isolated or unsupported caregivers report higher levels of distress and emotional fatigue (Schulz and Sherwood, 2008).
Challenges and future directions for research
Toward a definition of emotional support
One of the main challenges when studying the concept of ES, particularly in the context of illness, is the lack of consensus and homogeneity in its definition and assessment. Consequently, comparing and generalizing the findings across studies becomes difficult. It therefore appears important to work toward greater definitional clarity. In our opinion, this definition should incorporate the bidirectional nature of ES and consider elements that are linked to both the provider and the recipient of ES (Liu et al., 2020). Such a conceptualization would make it possible to consider both the act of receiving and the act of providing support. Furthermore, such a definition would allow for a clearer distinction between received ES and perceived ES. This would allow for a better understanding of the complex dynamics at play in ES and provide greater conceptual clarity. To address this gap, we propose a synthesis of what ES entails in the context of illness.
In the context of illness, ES refers to a range of actions and behaviors—including listening, empathy, comfort, and attention—that are directed toward an individual with a health problem. ES encompasses both received ES (concrete actions and behaviors provided by the provider) and perceived ES (the availability and quality of support as experienced by the recipient). In most cases, this support is provided by someone close to the individual, typically a family member. By its very nature, ES involves a relationship between two individuals and has bidirectional effects, which impact both the receiver and the provider, either positively or negatively. The effectiveness of ES depends on various factors, including a balance between the expectations of the ill person (the receiver) and the availability of the relative (the provider), as well as a relational balance that allows the receiver to feel supported while enabling the provider to find meaning, satisfaction, and a sense of reciprocity in offering support.
Toward a model of emotional support in the context of illness
The findings of this narrative review underscore the need to conceptualize ES from a relational and dyadic perspective. While some models adopt this approach (e.g. Berg and Upchurch, 2007), none focus specifically on ES in the context of illness. To address this gap, we propose a theoretical model centered on ES as it unfolds between a patient and a relative. This integrative and dynamic framework is grounded in the comprehensive synthesis of the literature reviewed throughout the article as well as our own analytical interpretation of these findings and the gaps they reveal. The model considers the individual, relational, and contextual factors that influence the provision and reception of ES, along their consequences. This model is not offered in a finalized form, but instead aims to clarify the main components and processes identified in the literature, thus providing foundation for future research and practical guidance for clinical settings.
The main actors: The patient and the relative
At the heart of the model presented in Figure 1 are two essential actors: the patient, who is directly affected by the illness and requires ES to cope with its challenges, and the relative who provides this support, who is often a family member. These two actors form a dyadic relationship in which their interactions and exchanges play an important role in shaping the dynamics of ES, influencing both its quality and effects.
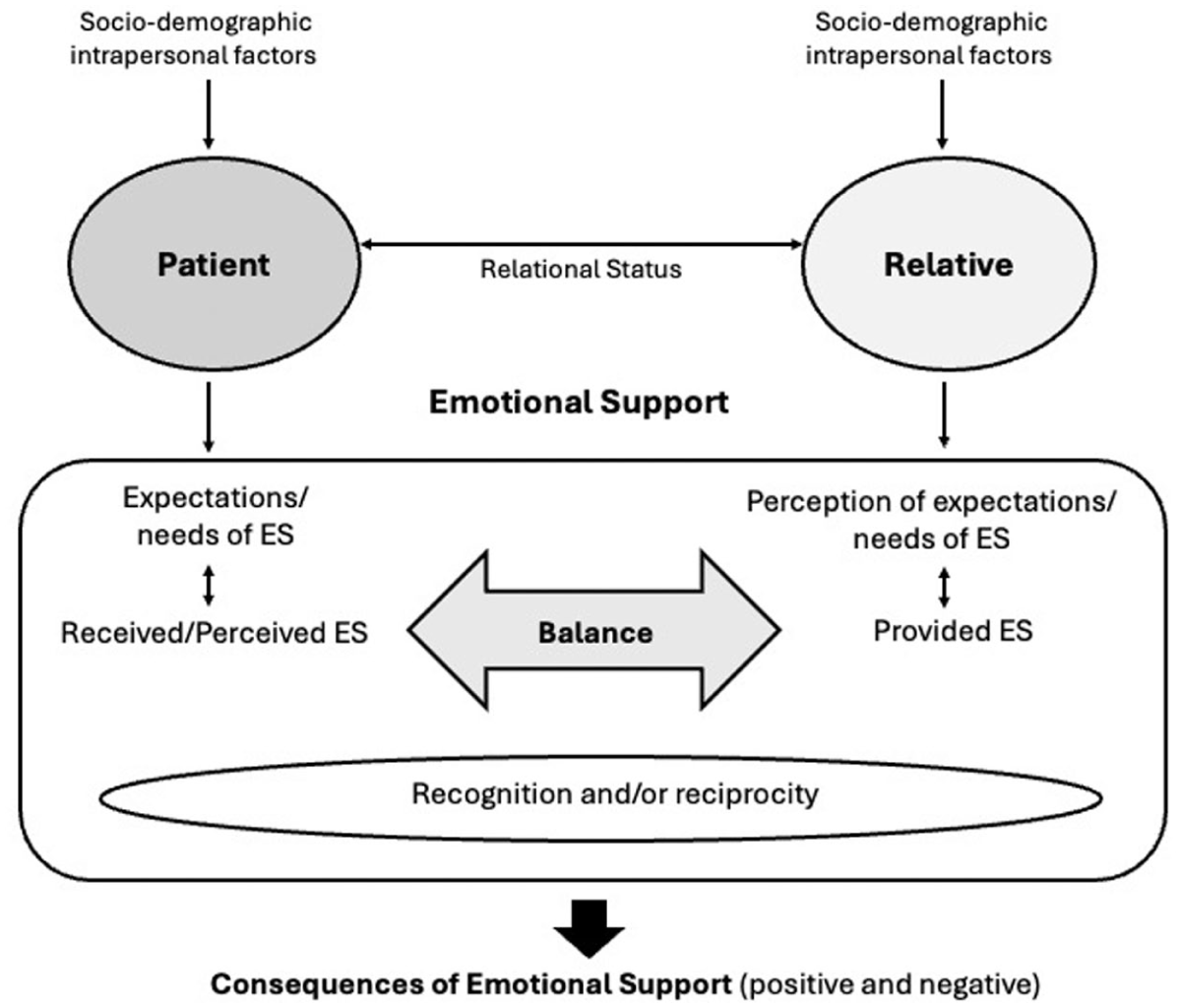
Model of emotional support in the context of illness.
Contextual factors influencing support
Two contextual factors shape the dynamics of ES in this model. The first is relational status, which encompasses the type and quality of the relationship (e.g. parent–child, patient–spouse) and affects how support is provided, received, and perceived. The second includes intrapersonal factors (e.g. personality traits, coping strategies) and sociodemographic factors (e.g. age, gender, socioeconomic status), which influence the expectations, perceptions, and behaviors of both actors.
Emotional support at the core of the model and its relational dynamics
ES lies at the core of the model presented in Figure 1 and is structured around key components that regulate the interaction between the patient and the relative. The patient has specific expectations and needs related to their illness, which the relative acknowledges to varying degrees and integrates into how they provide ES. The patient’s expectations influence how the support is delivered and how they ultimately perceive it (Bruchon-Schweitzer and Boujut, 2021; Georgopoulou et al., 2018).
The patient’s perception of this support then directly affects the sense of relational balance. When the support provided aligns with the patient’s expectations, it is perceived as beneficial, leading to a sense of balance in the relationship. Conversely, when expectations are unmet—when the support is perceived as intrusive, insufficient, or inadequate—it can result in frustration, dissatisfaction, or a sense of indebtedness toward the relative.
Recognition plays an important role in regulating this dynamic. The relative’s investment in providing ES requires at least some reciprocal acknowledgment from the patient. Recognition (e.g. expressions of gratitude) reinforces the provider’s motivation and emotional well-being, contributing to relational balance. In contrast, a lack of recognition can lead to dissatisfaction and strain the relational bond, increasing the risk of imbalance in the caregiving dynamic (Joo et al., 2020).
Thus, expectations influence the patient’s perception of ES, which in turn affects the relational balance. Recognition moderates this process by reinforcing the provider’s engagement and stabilizing the interaction. Hence, maintaining balance relies on a continuous alignment between the patient’s expectations and the adequacy of the support, as well as the mutual acknowledgment within the dyad. When this alignment is achieved, patient-relative interactions are harmonious and beneficial; otherwise, relational tensions—such as frustration for the patient and emotional exhaustion for the relative—may arise (Schulz and Sherwood, 2008).
Reciprocity enhances balance by introducing mutuality into the relationship (Antonucci and Jackson, 1990). While the patient is often the primary recipient of ES, they can also provide support in return. This reciprocal dynamic fosters mutual appreciation, thus strengthening the relational bond and reducing the risk of imbalance. For the patient, offering support in return can help alleviate any feeling of indebtedness while enhancing their sense of usefulness. Through this dynamic exchange, both actors can find meaning and satisfaction in the helping relationship.
Consequences of emotional support
This proposed model highlights the consequences of ES for both the patient and the relative and reflects and synthesizes the findings presented in Section 4. On the positive side, the relative may feel useful and accomplished in providing support, while the patient may experience improved well-being. Furthermore, the dyadic relationship itself can benefit from strengthened bonds as both parties feel understood and valued. On the negative side, the relative may experience frustration or emotional overload, especially if the support they provide is not reciprocated or if it becomes too demanding. The patient, on the other hand, may perceive the support as intrusive or inadequate, which can result in feelings of dissatisfaction or even resentment. In some cases, the relationship may suffer from misunderstandings or an imbalance in how support is exchanged. The alignment—or lack thereof—between expectations and needs directly shapes the quality of ES and its impact. When the patient’s expectations are met, balance fosters positive interactions, leading to mutual satisfaction and strengthened bonds. However, when there is an imbalance, it exacerbates tensions, leading to negative outcomes, such as emotional exhaustion for the relative or frustration for the patient.
A model that needs to be investigated
This model should be considered as an initial proposal that addresses several gaps identified through the literature review. To fully realize its potential, the model should be operationalized and tested in future empirical studies using both qualitative and quantitative methods. For example, interviews on the dynamics of emotional support among patients and their loved ones would enable the subsequent development of a self-administered scale to operationalize the model more broadly. However, there is a need for a specific tool dedicated to measuring ES in the context of illness. Developing such a tool would allow researchers to test this model and offer practical applications for clinicians. Such a tool could also help evaluate the dynamics of ES with greater precision and facilitate the design and development of tailored interventions to enhance the well-being of both patients and their relatives. Moreover, this model requires further refinement in light of key variables such as the type, severity, and duration of the illness, as well as differences across cultural contexts. For instance, the needs of a patient with a slowly progressing chronic illness may differ significantly from those of a patient facing an acute illness. Similarly, the severity of the illness can shape relatives’ psychological and emotional investment, which in turn, will influence their own expectations and needs within the helping relationship. Recognizing and incorporating these variables will ensure the model’s flexibility and enhance its practical relevance across diverse patient populations.
Conclusion
This narrative review highlights the conceptual and methodological challenges surrounding ES, a construct that remains broad and subjective in nature, and difficult to disentangle from social support. Based on this synthesis, and aiming to foster both conceptual understanding and practical reflection in caregiving and clinical contexts, we propose both a definition and an illness-specific theoretical model of ES that emphasizes the relational, dyadic, and contextual dimensions of ES. This model can inform clinical interventions and family-centered care by highlighting key mechanisms such as expectation alignment, recognition, and relational balance. In addition, the model underscores the importance of considering the patient–relative dynamic, along with individual, developmental, and relational factors that shape the provision and reception of ES. Future research should further explore these dynamics across different age groups and illness trajectories.
This narrative review did not follow a systematic search strategy, which represents a methodological limitation to consider. While this initial narrative review provides a conceptual foundation for ES, a more rigorous systematic review—with a clearly defined research question and formal quality appraisal—would represent a valuable next step toward refining the evidence base and informing future empirical research.
Footnotes
Ethical considerations
This narrative review did not require ethical approval or informed consent.
Consent to participate
Consent to participate is not applicable to this review article as no data were collected from participants.
Consent for publication
Consent for publication is not applicable to this review article as no identifiable participant data are included.
Author contributions
Conceptualization, CL, AU. Literature search, CL, EH. Writing—Original Draft: CL, EH. Writing—Review & Editing: CL, GD, EH, AU. All authors gave final approval of the version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.