
Abstract
This study was conducted to examine the effect of mothers’ perception of birth on separation anxiety, a rarely studied but clinically important topic in perinatal mental health. A descriptive and correlational design was used to identify relationships without intervention. The sample consisted of 305 postpartum women between the seventh day and sixth week, recruited from a private hospital. Data were collected using the Introductory Information Form, the Perception of Birth Scale, and the Adult Separation Anxiety Questionnaire. Statistical analyses included independent t-tests, ANOVA, Pearson correlation, and multiple regression. The mean age of participants was 29.09 ± 6.48 years. Separation anxiety was found to be significantly negatively correlated with the total score of the Perception of Birth Scale (r = −0.43, p ⩽ 0.001). Regression analysis showed that experiences during the pain period (β = −0.32, p < 0.001) and spousal involvement (β = −0.12, p < 0.05) negatively predicted separation anxiety. These two factors explained 21% of the variance. The findings suggest that positive childbirth perceptions, particularly effective pain management and partner support, may reduce maternal separation anxiety. This study contributes an innovative perspective by linking birth perception with separation anxiety, highlighting the need for interventions that promote positive childbirth experiences in order to protect maternal mental health.
Introduction
Physiologically, pregnancy is the 9-month period that allows the fetus to reach the maturity required to survive outside the uterus (Tonkuş and Muslu, 2021). Although pregnancy is considered a physiological process, it is actually a process that covers all biological and psychological changes (Atasever and Çelik, 2018; Yavuz and Bilge, 2022). Birth is defined as the event in which the first physical separation of mother and baby occurs (Karakoç and Kul Uçtu, 2023; Kesebir et al., 2011). The perception and experience of birth can vary from mother to mother. While it is an exciting and beautiful event for some women, for others it is a difficult, stressful, exhausting, unpredictable experience (Aydın and Yıldız, 2018; Yıldız, 2019). Accordingly, positive or negative birth perception is formed. Positive birth experience is reported to have an effect on birth and postpartum satisfaction, secure attachment, and successful breastfeeding (Aksoy Derya et al., 2019; Jafari et al., 2017; Uludağ and Mete, 2014; Yavuz and Bilge, 2022). Negative delivery experiences are said to be linked to significant psychological disorders such depression, PTSD, a decline in the mother-infant bond, and issues with breastfeeding (Aydın, 2018; Aydın and Yıldız, 2018; Namujju et al., 2018; Unsal Atan et al., 2018).
Separation anxiety is a state of experiencing anxiety when the individual is separated from the attachment model or when there is a possibility of separation (Diriöz et al., 2012; Manicavasagar et al., 2000). There are many studies about the emergence and development of separation anxiety. In previous studies, it was argued that separation anxiety emerges in childhood and does not carry over into adulthood. In recent studies, it has been proven that separation anxiety that starts in the early years of life can be carried into adulthood and even to the children of the individual (Bora and Ünüvar, 2020; Karataş et al., 2019; Namlı et al., 2022; Silove et al., 2010). It is thought that the birth perception takes place as a stressor factor in separation anxiety that occurs in adulthood (Kealy et al., 2020; Namlı et al., 2022; Shear et al., 2006). Upon reviewing the literature, no research on the connection between separation anxiety and birth perception was discovered. However, there are no studies on separation anxiety experienced especially by puerperant women. Therefore, the lack of studies on maternal separation anxiety in the postpartum period and the factors affecting it, especially in our country, constitutes the original value and motivation of the research. In this context, the study was conducted to examine the effect of mothers’ perception of birth on separation anxiety.
Material and methods
Design
The study was designed as descriptive and correlational. A correlational design is used to determine the direction and strength of relationships between variables without manipulating them. In this study, mothers’ perception of birth and their adult separation anxiety levels were measured simultaneously, and the possible associations between these variables were examined. Since no intervention was applied and the purpose was to identify relationships rather than causality, the correlational design was considered appropriate.
Study questions
Do separation anxiety levels vary according to the descriptive characteristics of mothers?
Is there a relationship between mothers’ perception of birth and separation anxiety?
Population and sample
The study population consisted of women admitted to a private hospital between July 2022 and December 2022, between the seventh day and the sixth week postpartum. Power analysis was conducted to determine the sample size of the study. For each parametric test planned to be used in the study (independent groups t test, one-way analysis of variance and regression analysis), power analysis was performed and the highest sample size was taken as a reference. In this direction, it was calculated that 305 people should be taken for ANOVA, taking into account the medium level (0.25) effect size, 95% power, α = 0.05 margin of error. Mothers who could read and write, were between the seventh day and sixth week postpartum, had healthy newborns and volunteered to participate in the study were included in the study. In the diagnostic information form, the history of psychiatric illness was questioned, and mothers who stated that they had such a history were excluded. In addition to self-report, participants were also asked whether they had previously received any psychiatric diagnosis, used psychiatric medication, or undergone psychiatric follow-up, in order to minimize the risk of underreporting or denial. Women who reported any of these were excluded from the sample. However, no structured psychiatric interview was applied, which we acknowledge as a limitation of the study.
The data collection was performed between postpartum day 7 and week 6. This time frame was selected because the first week postpartum is considered a period of transient emotional lability known as “baby blues,” which usually resolves spontaneously. Starting data collection after the seventh day reduced the risk of confusion between temporary baby blues and more stable anxiety symptoms. Additionally, the sixth postpartum week was chosen as the upper limit because it corresponds to the end of the puerperium, a period in which both physical and psychological postpartum changes stabilize. Therefore, the interval between day 7 and week 6 was considered optimal for evaluating maternal perception of birth and separation anxiety.
Women who delivered via elective cesarean section were excluded. The rationale for this exclusion was that the Perception of Birth Scale is primarily validated for use in unplanned cesarean or vaginal deliveries, where unpredictability and labor-related experiences significantly shape birth perception (Gungor and Beji, 2007; Marut and Mercer, 1979). Elective cesarean births are typically characterized by planned procedures with minimal labor exposure, which may lead to systematically different psychological experiences and confound associations with separation anxiety. Future studies should specifically investigate this population, as their unique experiences may also be associated with perinatal mental health outcomes.
Data collection tools
The Adult Separation Anxiety Scale, the Perception of Birth Scale, and the Introductory Information Form were used to gather the data.
Procedure
Data were collected through face-to-face interviews. A pre-application was conducted with 10 participants before the study to evaluate the comprehensibility of the questions in the data collection tools. Pre-application data were not included in the study data. Before the data collection tools were used, the researcher introduced herself and gave information about the subject and purpose, and the forms were filled in by the researcher in line with the mothers’ answers. Interviews lasted an average of 10–15 minutes for each participant.
Analysis
SPSS 25 program was used for data analysis and evaluation. The conformity of the numerical data to normal distribution was evaluated by examining the skewness and kurtosis coefficients. George and Mallery (2016) mention that the acceptable limits for skewness and kurtosis coefficients are +2, −2. The skewness and kurtosis coefficients of all variables used in the study are within acceptable limits (Table 1). Since the assumptions for parametric testing were met, independent samples t-tests, one-way ANOVA, Pearson correlation analysis, and multiple regression analysis were planned and conducted. In particular, multiple regression analysis was used to examine the predictive effects of the perception of birth scale’s sub-dimensions on adult separation anxiety.
Scales and subscales mean scores, skewness and kurtosis coefficients (n = 305).
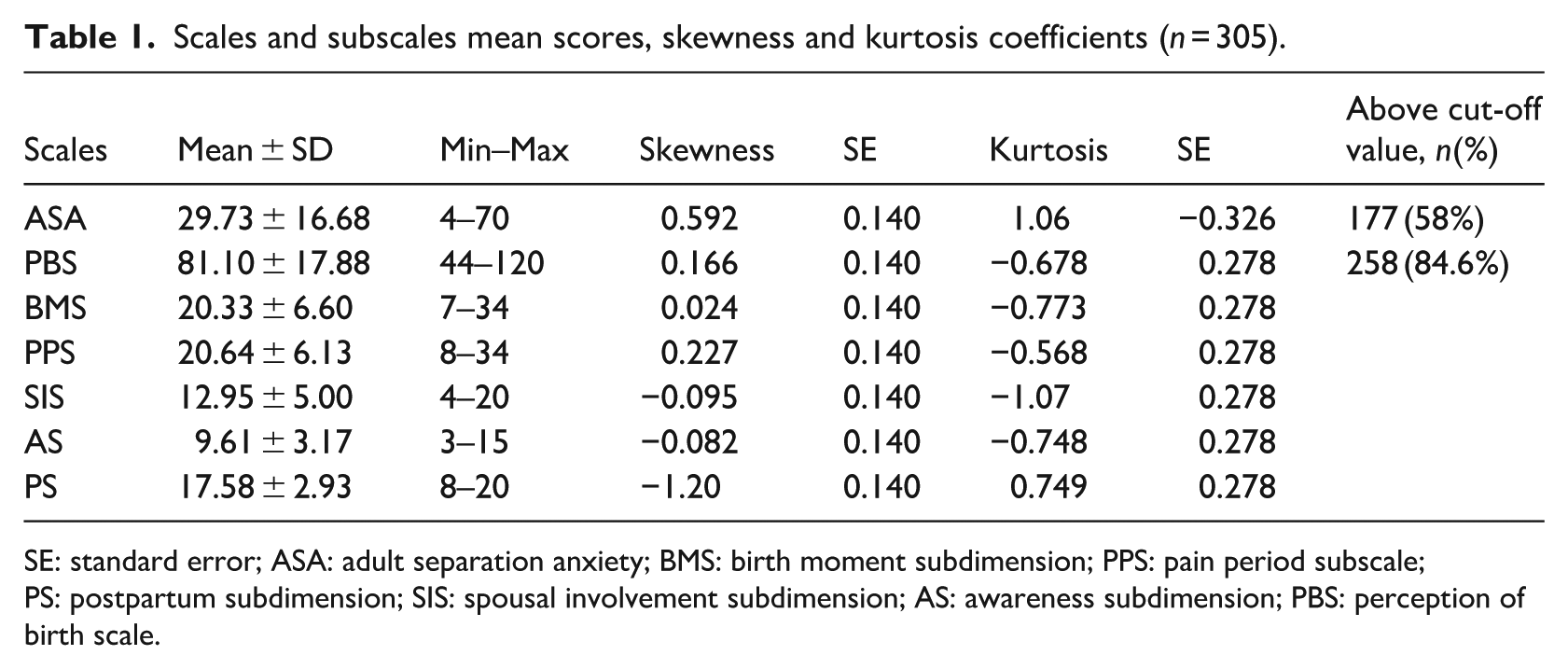
SE: standard error; ASA: adult separation anxiety; BMS: birth moment subdimension; PPS: pain period subscale; PS: postpartum subdimension; SIS: spousal involvement subdimension; AS: awareness subdimension; PBS: perception of birth scale.
Ethics
The study was approved by the Ethics Committee for Pharmaceutical and Non-Medical Device Research at the University of KTO Karatay at Konya (dated 17/06/2022 and numbered 2022/036) and written informed consent for participation was obtained from participants.
Results
The study included 305 women. The Adult Separation Anxiety Questionnaire had a mean score of 29.73 ± 16.68, the Mothers’ Perception of Birth Scale had a mean score of 81.10 ± 17.88, the moment of birth sub-dimension had a mean score of 20.33 ± 6.60, the pain period sub-dimension had a mean score of 20.64 ± 6.13, the spouse’s participation sub-dimension had a mean score of 12.95 ± 5.00, the awareness sub-dimension measured 9.61 ± 3.17, and the postpartum sub-dimension had a mean score of 17.58 ± 2.93 (Table 1).
Descriptive characteristics of participants
The mean age of the participants was 29.09 ± 6.48 years. It was determined that 45.6% of the women had university and higher education, 54.4% were not employed, 63% reported that income was equivalent to expenses, and 72.5% lived in a province (Table 2).
Examination of mean scores on the adult separation anxiety questionnaire according to descriptive characteristics.
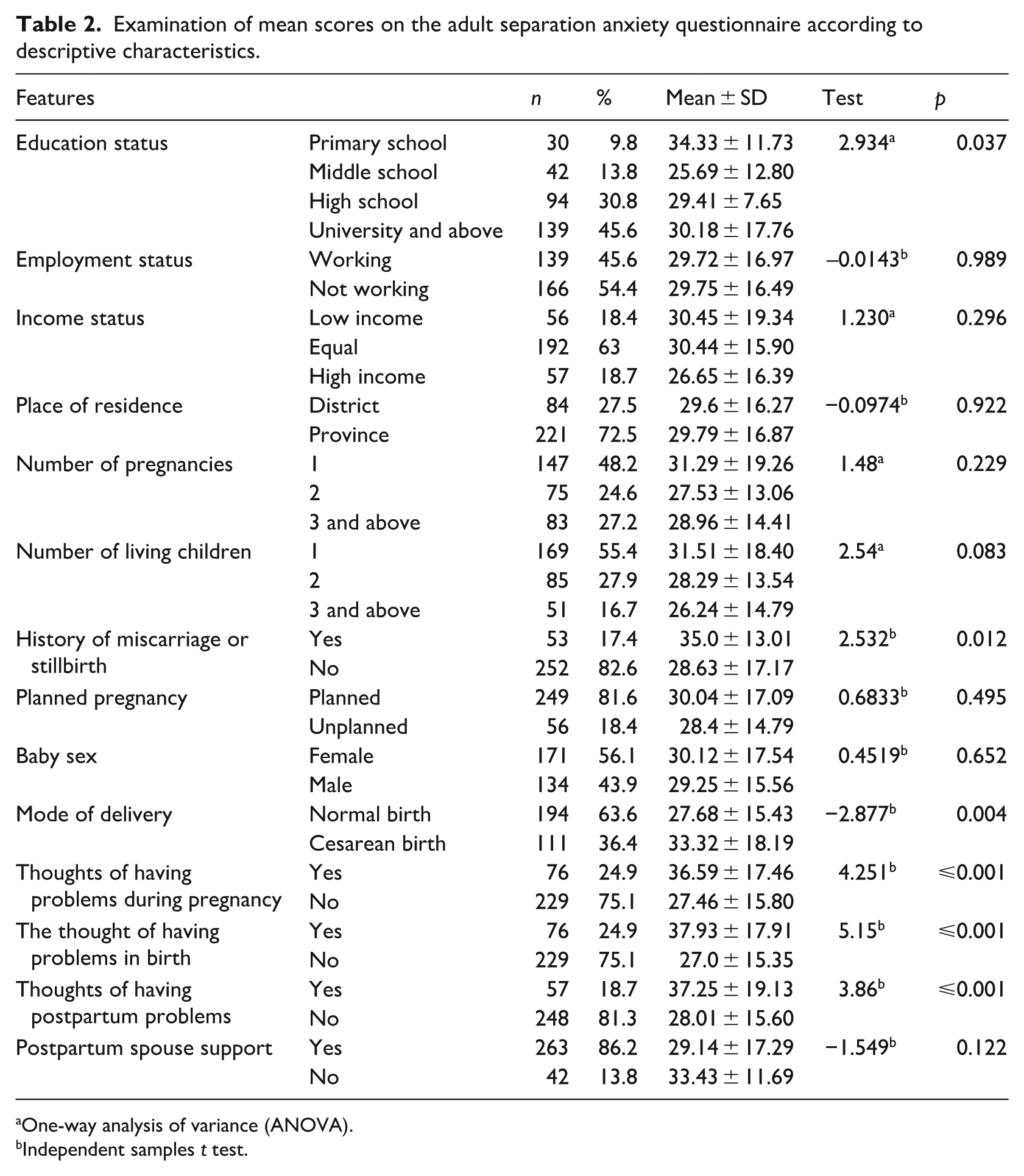
One-way analysis of variance (ANOVA).
Independent samples t test.
When the characteristics of the participants regarding pregnancy and delivery were examined, it was found that 48.2% had one pregnancy, 48.2% had one living child, 17.4% had a history of miscarriage or stillbirth, 56.1% had a female baby and 43.9% had a male baby. It was determined that 63.6% of the women had a vaginal delivery. It was found that 24.9% of the women experienced problems during both pregnancy and delivery, 18.7% experienced problems in the postpartum period, and 86.2% had a supportive husband (Table 2).
Mean adult separation anxiety scores according to descriptive characteristics of participants
The mean score of adult separation anxiety by educational status, history of miscarriage or stillbirth, mode of delivery, and difficulties during pregnancy, delivery, and the postpartum period was found to differ significantly between the groups (p < 0.05). Bonferroni test was performed to determine which group was the source of the difference according to educational status, and although there was a difference according to the mean scores of adult separation anxiety, no difference was found according to the results of the post hoc analysis. The participants with a history of loss or stillbirth, a normal delivery, and issues during pregnancy, delivery, and the postpartum period had higher mean adult separation anxiety scores (Table 2). Other sociodemographic and obstetric characteristics (such as employment status, income level, residence, number of pregnancies, number of living children, planned pregnancy, sex of the baby, and postpartum spousal support) did not show a statistically significant difference in adult separation anxiety scores (p > 0.05).
The relationship between participants’ perception of birth and adult separation anxiety
The perception of birth scale’s overall score (r = −0.43, p ⩽ 0.001) and its sub-dimensions—the moment of birth at a low moderate level (r = −0.34, p ⩽ 0.001), the pain period at a moderate level (r = −0.43, p ⩽ 0.001), spouse involvement at a low or insignificant level (r = −0.24, p ⩽ 0.001), awareness at a low moderate level (r = −0.32, p ⩽ 0.001), and postpartum at a low or insignificant level (r = −0.17, p ⩽ 0.001) were all found to be significantly negatively correlated with separation anxiety (Table 3).
The relationship between the maternal perception of birth scale and the adult separation anxiety questionnaire.
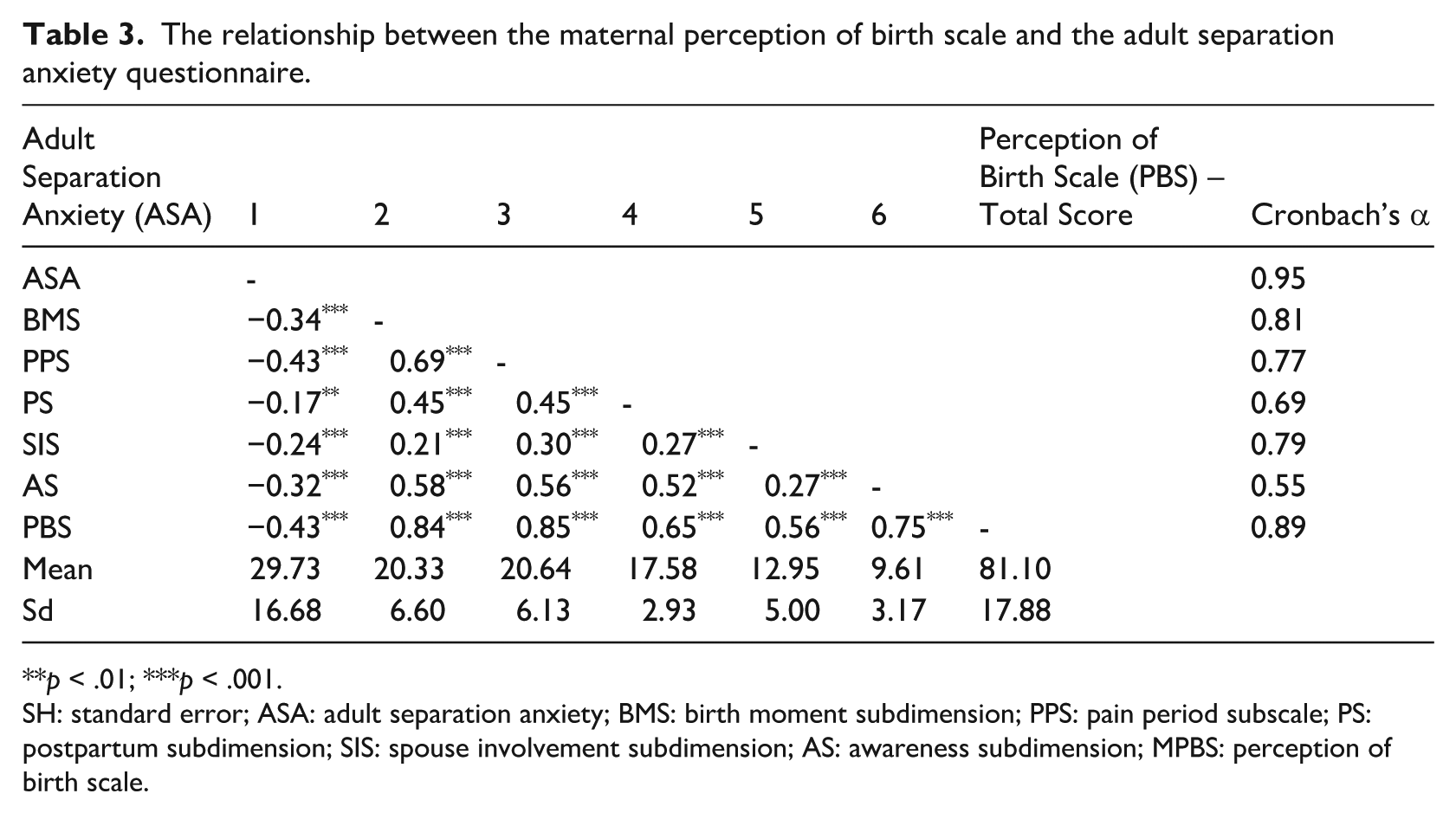
**p < .01; ***p < .001.
SH: standard error; ASA: adult separation anxiety; BMS: birth moment subdimension; PPS: pain period subscale; PS: postpartum subdimension; SIS: spouse involvement subdimension; AS: awareness subdimension; MPBS: perception of birth scale.
Multiple regression analysis on the prediction of adult separation anxiety by participants’ perception of birth
The results of the multiple regression analysis regarding the prediction of adult separation anxiety levels by the sub-dimensions of the perception of birth scale, namely experiences at the time of birth, experiences during the pain period of birth, postpartum, partner involvement, and awareness, are shown in Table 4. Preliminary analyses were conducted to examine the assumptions of normality, linearity, multiple collinearity and co-variance. The multiple regression model was statistically significant (F(5-299) = 16.10, p < 0001). In the final model, only the dimension of experiences during the pain period of birth (β = −0.32, t = −4.25, p < 0.001) and the dimension of spouse involvement (β = −0.12, t = −0.22, p < 0.05) among the five dimensions of the perception of birth scale were found to negatively predict adult separation anxiety. In other words, it can be stated that higher scores in the mentioned dimensions are associated with lower levels of adult separation anxiety. The dimensions of experiences during the pain period of labor and spousal involvement explained approximately 21% of the total variance of adult separation anxiety (R2 = 0.212).
Multiple regression analysis results for mothers’ perception of birth scale dimensions predicting adult separation anxiety.
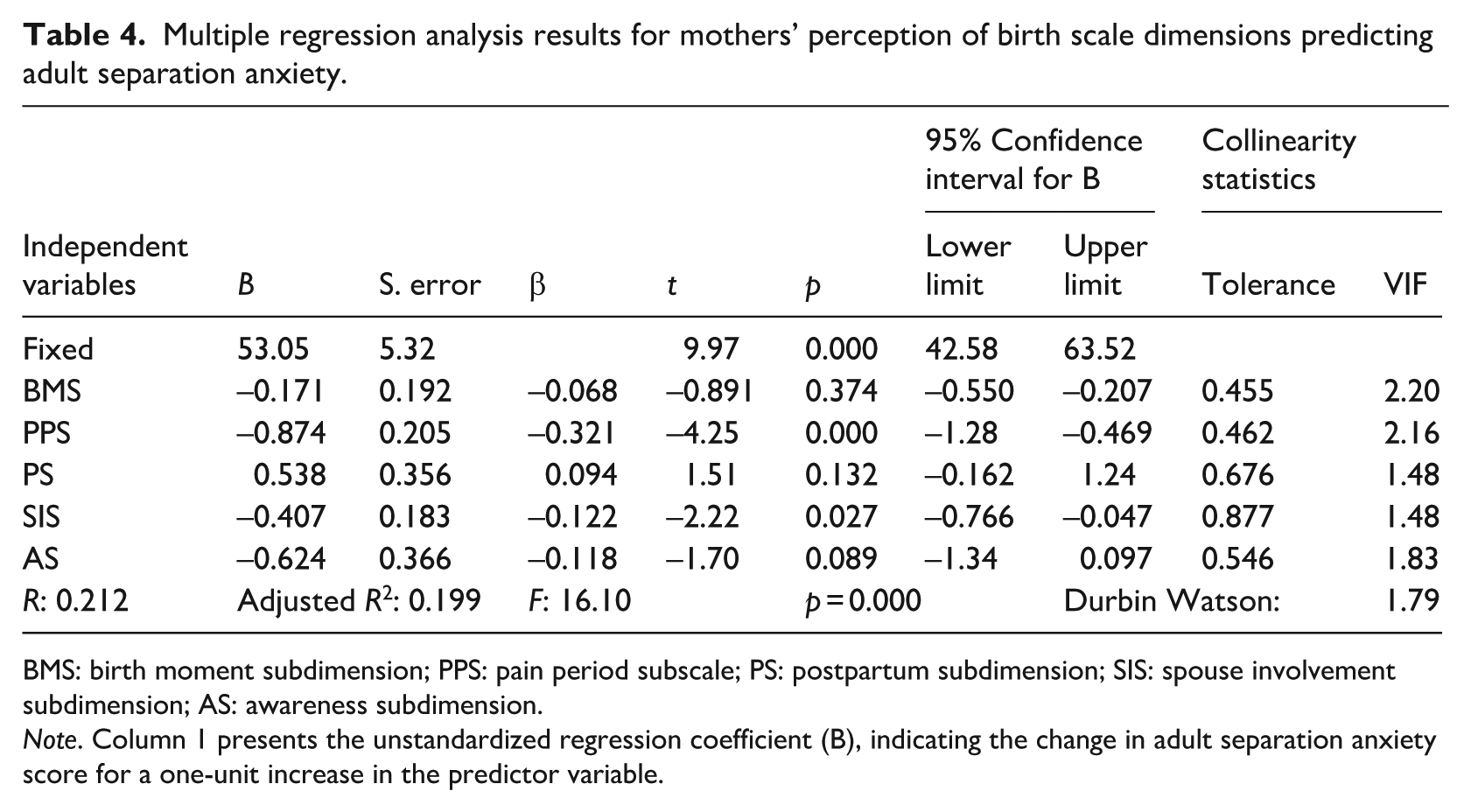
BMS: birth moment subdimension; PPS: pain period subscale; PS: postpartum subdimension; SIS: spouse involvement subdimension; AS: awareness subdimension.
Note. Column 1 presents the unstandardized regression coefficient (B), indicating the change in adult separation anxiety score for a one-unit increase in the predictor variable.
Discussion
In this study, more than half of the mothers experienced adult separation anxiety, which highlights the importance of the postpartum period in maternal mental health. When the literature is examined, despite the studies showing that there is a relationship between mothers’ separation anxiety and children’s anxiety levels (Baartmans et al., 2022; Bilgin, 2022; Bora and Ünüvar, 2020; Şahin and Görünmez, 2022), there is no study showing the frequency of mothers’ separation anxiety. Since 58% of the participants in the postpartum period self-reported that they experienced separation anxiety, it is thought that studies should be conducted to determine the prevalence on the subject. It was determined that 84.6% of the participants had a score above the cut-off value of the mothers’ perception of birth scale (81.10 ± 17.88). Regarding the subject, Sarıboğa and Zeyneloğlu (2021) reported that the mean score of mothers’ perception of birth was 79.67 ± 13.99 (minimum = 36–maximum = 119), Aksoy Derya et al. (2019) reported that the mean score of mothers’ perception of birth was 73.05 ± 12.52 (minimum = 36–maximum = 104) and mothers perceived birth positively. The research finding is consistent with the literature. However, it is noteworthy that although the participants had a high level of positive perception of birth, the frequency of separation anxiety was also high. Therefore, it is thought that the negativities experienced in the postpartum period as well as the moment of birth have a significant effect on separation anxiety and it is recommended that prospective studies on the subject should be planned.
A significant negative association was found between mothers’ perception of birth and their levels of separation anxiety. In the literature, it is stated that positive birth perception strengthens mother and baby attachment and positively affects postpartum health (Karlström et al., 2015; Mukamurigo et al., 2017), while negative birth perception increases the risk of postpartum depression, secondary fear of birth and post-traumatic stress disorder (Klabbers et al., 2016; Mukamurigo et al., 2017). From this point of view, it is thought that negative birth perception may negatively affect psychological health in the postpartum period and increase the risk of separation anxiety.
Importantly, prior research has emphasized that postpartum mental health difficulties often occur comorbidly. Depression and anxiety are highly intertwined during the perinatal period (Unsal Atan et al., 2018), and maternal separation anxiety may represent part of this broader spectrum of psychological vulnerability. Negative perceptions of childbirth may therefore both reflect and exacerbate underlying depressive or anxious symptomatology. Future research should investigate these comorbid pathways more explicitly to clarify whether separation anxiety acts as an independent construct or as a coexisting dimension of perinatal depression and anxiety disorders.
Furthermore, attachment theory provides an additional perspective. Insecure attachment styles, particularly anxious attachment, have been linked with heightened maternal vulnerability to separation-related anxiety (Bögels et al., 2013; Kesebir et al., 2011). A negative perception of childbirth may undermine a mother’s sense of security and reinforce these attachment vulnerabilities, while positive perceptions may strengthen secure attachment and serve as a protective factor. This theoretical lens suggests that interventions focusing on promoting positive birth experiences could indirectly contribute to fostering secure attachment patterns and reducing postpartum anxiety.
It is stated that especially the rearing environment during infancy has a great impact on mental health in adulthood (Harauma et al., 2023). This finding suggests that when mothers perceive their birth experience more positively, their anxiety related to separation decreases. Importantly, the perception of pain during labor and the involvement of the spouse emerged as the most influential predictors of maternal separation anxiety. These results underline the need to strengthen psychosocial and emotional support for women during childbirth, particularly by ensuring partner involvement and effective pain management. From a clinical perspective, interventions that promote a positive birth perception may not only reduce maternal anxiety but also improve the quality of maternal–infant bonding. Since maternal separation anxiety has been associated with higher anxiety levels in children, these findings also imply that early maternal support may prevent future developmental and psychological difficulties in offspring. Focusing on maternal wellbeing in the early postpartum period may therefore contribute to healthier long-term outcomes for both mothers and their children.
The perception of pain during labor and the involvement of the spouse were found to be the strongest predictors of maternal separation anxiety, explaining about 21% of the variance. This aligns with previous research showing that a positive birth perception increases postpartum safety, well-being, family bonding, and breastfeeding (Aksoy Derya et al., 2019). Therefore, interventions targeting these aspects may be particularly effective in reducing separation anxiety and supporting maternal–infant health.
Overall, the integration of our findings with the broader perinatal mental health literature underscores the multidimensional nature of maternal psychological outcomes. Addressing separation anxiety in postpartum women requires not only attention to their perception of birth but also recognition of the roles of comorbid depression and underlying attachment styles. Comprehensive, multidisciplinary interventions may therefore be most effective in improving maternal wellbeing and preventing negative intergenerational consequences.
The clinical implications of these findings suggest the need for structured and targeted interventions. Antenatal education programs could specifically include sessions on coping with labor pain, realistic expectations of childbirth, and strategies to enhance partner involvement during birth. Psychoeducation could be delivered through prenatal classes, digital modules, or midwife-led group sessions, incorporating role-play and relaxation techniques. Intrapartum interventions may include allowing birth partners greater involvement in care and reinforcing continuous midwifery support. Postnatally, follow-up programs should screen for maternal separation anxiety in routine visits and offer early psychological counseling where needed. By specifying content, delivery mode, and timing of these interventions, clinical practice can more effectively translate research findings into measurable maternal mental health benefits.
Limitations
This study has several limitations that should be considered when interpreting the findings. First, the data were based exclusively on self-report instruments, such as the Adult Separation Anxiety Questionnaire, without clinical validation. This reliance on self-report may have introduced response bias, and the absence of a structured psychiatric interview limits the certainty regarding participants’ mental health status. Second, the cross-sectional design precludes establishing causal relationships between mothers’ perception of birth and separation anxiety. Longitudinal or prospective studies are needed to clarify the temporal sequence and provide stronger evidence for causality. Third, although the regression model identified significant predictors, it explained only 21% of the variance in separation anxiety, indicating that other unmeasured factors (e.g. prior traumatic experiences, quality of social support, personality traits) may also play an important role. Fourth, the correlational design does not allow firm conclusions about directionality; it is also possible that pre-existing anxiety influenced mothers’ perception of birth rather than the reverse. Fifth, the study sample was recruited from a single private hospital, which restricts the generalizability of the results to broader populations, including those receiving care in public health institutions or representing diverse socioeconomic backgrounds. Finally, the exclusion criteria applied (e.g. elective cesarean section, psychiatric history) may have introduced selection bias, limiting the applicability of the findings to all postpartum women. Despite these limitations, the study contributes novel evidence on the relationship between maternal birth perception and separation anxiety during the postpartum period.
Conclusion
The study that looked at how mothers’ perceptions of birth affected their separation anxiety found a moderately significant negative correlation between separation anxiety and the mothers’ perception of birth scale’s overall score. Among the five dimensions of the mothers’ perception of birth scale, the sub-dimensions of experiences during the pain period and the involvement of the spouse predicted adult separation anxiety negatively. In line with the results of the study, it is recommended to plan studies to increase the level of awareness of professionals who provide care to the mother and baby in terms of separation anxiety that may be experienced in the postpartum period, to support women positively in terms of creating a positive perception of birth regardless of any psychological problem, and to conduct more comprehensive qualitative and randomized controlled studies on this issue, considering that separation anxiety experienced by the mother may cause future developmental problems for the baby and may lead to many irreversible problems.
Relevance of clinical practice
In the study, it was found that mothers’ positive perception of the birth experience had a reducing effect on separation anxiety. In this context, educating mothers before birth can help them perceive their birth experience more positively. These programs can help women reduce their anxiety levels and increase their self-confidence by providing information about birth. Second, providing emotional and psycho-social support to mothers during the birth process can increase their positive perceptions. Support offered through midwives can help women to experience the birth process as a more positive experience. Thirdly, more involvement of family members, especially spouses, in the birth process may contribute to making the mother’s experience more positive. The way in which spouses provide support in this process may reduce the stress level of the mother. Clinical practice could emphasize the customization of birth plans to meet the individual needs of each woman. Finally, to integrate your findings into clinical practice, it may be important to publish your research and raise awareness. Clinical research enables practitioners to benefit from such data.
Footnotes
Acknowledgements
The authors would like to thank the study participants and study team members for their contributions to this study.
Ethical considerations
The study was approved by the Ethics Committee for Pharmaceutical and Non-Medical Device Research at the University of KTO Karatay at Konya (dated 17/06/2022 and numbered 2022/036).
Consent to participate
Participants consented to the publication of anonymized data and written informed consent for participation was obtained from participants.
Consent for publication
Consent for publication was not applicable for this article as it contains no identifiable data.
Author contributions
Hediye Karakoç and Ebru Şimşir contributions to conception and design, acquisition of data, or analysis and interpretation of data, revising it critically for important intellectual content. Ebru Şimşir contributions to acquisition of data. Moreover, involving in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.*