
Abstract
Depression is a frequent neuropsychiatric symptom in dementia, yet metabolic contributors remain poorly understood. Central adiposity may be involved, but conventional anthropometric measures may inadequately capture obesity in older adults. This cross-sectional study included 601 community-dwelling individuals aged 60–91 years evaluated at a memory clinic between 2015 and 2024. Dementia was diagnosed using DSM-5 criteria for Major Neurocognitive Disorder, and depressive symptoms were assessed with the 15-item Geriatric Depression Scale. Obesity was evaluated using multiple anthropometric indices, including Body Mass Index, Waist Circumference, Waist-to-Height Ratio, A Body Shape Index, Conicity Index, Weight-Adjusted Waist Index, and Body Roundness Index (BRI). No measure was associated with depression in the overall sample. Among individuals with dementia, higher BRI was associated with increased odds of depression, with those in the highest quartile showing more than threefold greater odds. These findings suggest that BRI may better capture central adiposity relevant to depression in dementia.
Introduction
Dementia is a major global health concern, and it is estimated that up to 45% of cases are associated with modifiable risk factors, including low education, depression, sensory deficits, and metabolic diseases (Livingston et al., 2024). Although cognitive decline encompasses a broad continuum of cognitive changes that may occur with or without functional consequences, dementia is a clinically defined syndrome characterized by objective cognitive deficits accompanied by functional impairment (American Psychiatric Association, 2013). Among modifiable risk factors, obesity has emerged as an important predictor of adverse cognitive outcomes in older adults. For example, Tang et al. (2021) reported that central obesity, assessed by Waist Circumference (WC), is associated with a 10% increase in the risk of cognitive decline and dementia, particularly in individuals aged 65 years and older (Tang et al., 2021). Consistently, Qu et al. (2020) demonstrated that midlife obesity, measured by Body Mass Index (BMI), is related to a 31% higher risk of dementia from all causes (Qu et al., 2020).
Several factors may contribute to the link between excess body fat and dementia, including an increased risk of cerebrovascular disease and chronic low-grade systemic inflammation. Evidence from the UK Biobank cohort suggests that hypertension, diabetes mellitus, and elevated serum C-reactive protein may mediate the relationship between obesity, white-matter pathology, and cognitive impairment, thereby increasing vulnerability to late-life dementia (Morys et al., 2021). In turn, persistent inflammation may disrupt neuronal activity and accelerate neurodegeneration (Ghosh et al., 2024; Weijie et al., 2024). Similarly, obesity-related inflammation can increase oxidative stress, trigger hypothalamic-pituitary-adrenal (HPA) axis hyperactivity, and contribute to insulin resistance, all of which may lead to depressive symptoms (Ly et al., 2023).
Studies have also explored the relationship between central obesity and depressive symptoms. Li et al. (2024) analyzed data from 34,528 adults and found that individuals with a higher Weight-Adjusted Waist Index (WWI) had a 51% greater likelihood of experiencing depression compared to those with lower WWI values (Li et al., 2024). Coherently, a cross-sectional study of 1821 participants identified a significantly positive association between BMI and Waist-to-Height Ratio (WHtR), and depression scores in middle-aged and older adults (Lonergan et al., 2024). Furthermore, a longitudinal study tracking 6835 individuals aged 45 and older revealed that higher WWI was linked to a worsening of depressive symptoms over time (Zeng et al., 2024).
However, assessing obesity in older adults presents methodological challenges that complicate understanding its impact on cognition and mood. BMI, the most used measure, does not differentiate between fat and lean mass. Consequently, it may underestimate adiposity in individuals experiencing muscle and bone loss, a common condition in later life (Rubino et al., 2025). Due to these issues, both The Lancet Diabetes & Endocrinology Commission and the American Diabetes Association recommended using BMI solely for screening purposes (American Diabetes Association Professional Practice Committee et al., 2025; Rubino et al., 2025). In addition, these expert consensus statements advised complementing it with direct body fat assessments or alternative anthropometric measures, such as WC, waist-to-hip ratio, or WHtR (American Diabetes Association Professional Practice Committee et al., 2025; Rubino et al., 2025).
Likewise, WC, another widely recommended metric for evaluating central obesity, may not reliably assess subcutaneous or visceral fat accumulation and has shown inconsistent correlations with cognitive variables in individuals with dementia (Assuncao et al., 2018; Rubino et al., 2025). With these limitations and the need for easy cost-effective methods to measure abdominal fat in primary care, several novel anthropometric indicators have been proposed, such as A Body Shape Index (ABSI), Conicity Index (CI), Body Roundness Index (BRI), WHtR, and WWI (Abdi Dezfouli et al., 2023; Ashwell et al., 2012; Kim et al., 2023; Krakauer and Krakauer, 2012; Park et al., 2018; Rico-Martín et al., 2020; Thomas et al., 2013; Valdez, 1991; Yusoff et al., 2025; Zhang et al., 2022).
Emerging evidence suggests that higher values of several novel anthropometric indices may be associated with neurodegeneration, cognitive decline, and dementia; however, findings remain heterogeneous and vary across populations and outcomes (Lee et al., 2024; Wang et al., 2023; Yan et al., 2024; Zhang et al., 2024). Although indices such as BRI, ABSI, CI, and WWI remain indirect measures of adiposity, they were developed to improve upon traditional metrics by more accurately capturing body fat distribution rather than total body mass alone (Ashwell et al., 2012; Park et al., 2018; Thomas et al., 2013; Valdez, 1991). Compared with BMI and WC, several of these indices show stronger correlations with visceral adipose tissue and total fat mass assessed using imaging-based techniques, including dual-energy X-ray absorptiometry (DXA) and magnetic resonance imaging, while still reflecting clinically relevant aspects of central adiposity (Kim et al., 2025; Krakauer and Krakauer, 2021; Thomas et al., 2013). Among these measures, the Body Roundness Index has received particular attention: derived from a geometric model that conceptualizes the body as an ellipsoid, BRI integrates height and waist circumference to estimate central adiposity and demonstrates stronger correlations with visceral adipose tissue and total body fat than BMI, as assessed by DXA and MRI-derived visceral fat volume (Thomas et al., 2013). Consistent with this, prior studies suggest that BRI may outperform BMI and conventional waist-based measures in identifying metabolically obese normal-weight phenotypes and in predicting cardiometabolic risk (Chen et al., 2024; Rico-Martín et al., 2020; Tian et al., 2016). Importantly, these indices are not intended to replace direct assessments of body composition, such as MRI-, DXA-, or CT-derived estimates of fat mass and fat-free mass, which remain the reference standards. Rather, they function as pragmatic surrogates offering distinct advantages in epidemiological research and clinical practice, including low cost, ease of implementation, and feasibility in older adults and individuals with dementia. Growing evidence also suggests that some of these indices may provide improved risk stratification for metabolic and cardiometabolic outcomes compared with traditional anthropometric measures, supporting their use when direct body composition assessments are unavailable or impractical (Rico-Martín et al., 2020; Wang et al., 2025; Zhu et al., 2026).
Given the shared pathophysiological mechanisms linking obesity, depression, and cognitive decline, it could be hypothesized that obesity represents a modifiable risk factor for both dementia and mood disturbances in older adults. Investigating the association between body fat measurements and depressive symptoms in individuals with dementia may elucidate the metabolic pathways underlying mood abnormalities and identify novel targets for managing neuropsychiatric symptoms in dementia. Consequently, this study aims to investigate the association between obesity, using both traditional and novel anthropometric measurements, and the presence of depressive symptoms in people with dementia.
Methods
Study design, setting and participants
This cross-sectional study is part of a broader investigation on cognitive impairment and dementia in older adults conducted at a tertiary memory clinic between 2015 and 2024. Although the parent study encompasses a broad spectrum of cognitive functioning, including individuals with and without dementia, the present analyses focus specifically on participants with clinically diagnosed dementia, as defined by objective cognitive impairment and functional decline (see below). Participants were referred to the memory clinic by healthcare professionals for clinical and neuropsychological assessments. Eligible individuals were non-institutionalized older adults (⩾60 years old) with at least 8 years of formal education, who were native Brazilian Portuguese speakers. Exclusion criteria included a current diagnosis of delirium (American Psychiatric Association, 2013), a history of severe psychiatric disorders such as schizophrenia, intellectual disability, or bipolar disorder, as well as a history of substance-related disorders (American Psychiatric Association, 2013). Participants were also excluded if they had severe visual or auditory impairments that prevented neuropsychological testing or refused to complete the neuropsychological protocol. Recruitment procedures and cohort characteristics have been described in detail elsewhere (Santos et al., 2025). This study follows the STROBE reporting guideline (von Elm et al., 2007).
Procedures
Participants first underwent a standardized clinical interview conducted by a physician, followed by a physical examination that included measurements of height, weight, and waist circumference. These measures were used to derive traditional and novel anthropometric indices of adiposity, which constituted the primary exposures of interest.
Cognitive and diagnostic assessments were performed by a trained neuropsychologist using Brazilian-validated instruments, including the Mini-Mental State Examination (MMSE; Folstein et al., 2018), Rey Auditory Verbal Learning Test (RAVLT; De Paula and Malloy-Diniz, 2018), Trail Making Test (Zimmermann et al., 2017), phonemic and semantic verbal fluency tasks (Teldeschi et al., 2018), Digit Span (Zimmermann et al., 2015), and Visual Reproduction (Spedo, 2012). Language abilities were evaluated by a speech-language therapist. Performances on these instruments were used for the diagnosis of dementia (see below).
Depressive symptoms, the primary outcome of the study, were assessed using the 15-item Geriatric Depression Scale (GDS; Paradela et al., 2005). Anxiety symptoms were measured with the Geriatric Anxiety Inventory (GAI; Massena et al., 2015) and included as a covariate due to their high comorbidity with depression in dementia and their potential confounding effect on mood assessment (Novais and Starkstein, 2015). Functional status was evaluated using Pfeffer’s Functional Activities Questionnaire (FAQ; Assis, 2014), and informant-reported cognitive decline was assessed with the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE; Sanchez and Lourenço, 2009).
Additional covariates relevant to depressive symptoms and metabolic health were also collected, including physical activity in the previous week (International Physical Activity Questionnaire—IPAQ; Benedetti et al., 2007), unhealthy alcohol consumption in the past year (Alcohol Use Disorders Identification Test - AUDIT; Santos et al., 2012), and smoking status, as reported by participants or their informants.
Classification
Hypertension was diagnosed if the participant had blood pressure ⩾140 / 90 mmHg during the consultation or if they were receiving pharmacological treatment for the condition (World Health Organization, 2023). Diabetes Mellitus and Dyslipidemia were identified based on the participant’s or their informant’s report of a prior diagnosis or current use of medication for these conditions. Patients using GLP-1 agonists were classified as having Diabetes Mellitus if it was informed that the drug was prescribed for this condition.
Dementia was identified using a modified version of the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria for Major Neurocognitive Disorder, requiring the presence of both of the following criteria: (i) cognitive performance at least two standard deviations (SD) below normative values for age and education in at least one task and (ii) functional impairment, defined by a score ⩾ 5 on FAQ (American Psychiatric Association, 2013; Assis, 2014). The presence of depression was defined as GDS ⩾ 5 (Paradela et al., 2005).
Anthropometric indices
Body Mass Index (BMI) was defined as weight in kilograms divided by the square of height in meters (kg/m2; World Health Organization, 2024). Waist circumference (WC) was measured following the World Health Organization (WHO) guidelines (World Health Organization, 2008). Newer anthropometric indices were calculated using formulas depicted in Supplemental Table S1, including A Body Shape Index (ABSI), Conicity Index (CI), Body Roundness Index (BRI), Waist-to-Height Ratio (WHtR), and Weight-adjusted Waist Index (WWI; Ashwell et al., 2012; Krakauer and Krakauer, 2012; Park et al., 2018; Thomas et al., 2013; Valdez, 1991).
Statistical analysis
Data normality was assessed with the Kolmogorov-Smirnov test. With this result, group differences (with and without depression) were analyzed using Mann Whitney U test for continuous variables and Fisher’s exact test for categorical variables. Due to the lack of consensus on the new anthropometric cutoffs for older adults and concerns about BMI and WC thresholds in this population, these variables were analyzed as quartiles (Camina Martín et al., 2016; Supplemental Table S2). Anthropometric indices that significantly differed between groups were included as predictors for depression in a logistic regression analysis (model 1). This procedure was repeated, adjusting for age, sex and education (model 2) and for age, sex, education, hypertension, diabetes mellitus, dyslipidemia, FAQ, and GAI (model 3). Missing data was handled using listwise deletion. All statistical analyses were conducted in IBM SPSS Statistics v.26, with a significance level set at p < 0.05.
Results
Demographic and clinical variables
The study included 601 participants, of whom 39.8% (n = 239) were diagnosed with dementia. Depression was present in 35.4% of the overall sample (n = 213), and in 36.4% (n = 87) of those with dementia. Across the total sample, no significant differences were found in age or education level between participants with and without depression. However, there was a trend toward a difference in sex distribution (p = 0.052). As expected, individuals with depression had significantly higher scores on the Geriatric Anxiety Inventory (GAI) and Geriatric Depression Scale (GDS) compared to those without depression (p < 0.001). They also had lower physical activity levels as measured by the IPAQ (p = 0.019). No significant differences were observed between groups for IQCODE, AUDIT, FAQ, metabolic disease presence, or smoking status.
Among participants without dementia, those with depression were younger than those without (p = 0.048) and had significantly higher GAI and GDS scores (p < 0.001). No other continuous variables differed significantly.
In the dementia subgroup, participants without depression had more years of education than those with depression (p = 0.036). As in the non-dementia group, GAI and GDS scores were significantly higher in individuals with depression (p < 0.001), while no other clinical or sociodemographic variables differed.
Table 1 summarizes these findings. Additionally, five participants (0.83%) reported current use of GLP-1 agonists—four with dementia and one without.
Sociodemographic and clinical characteristics of the sample.
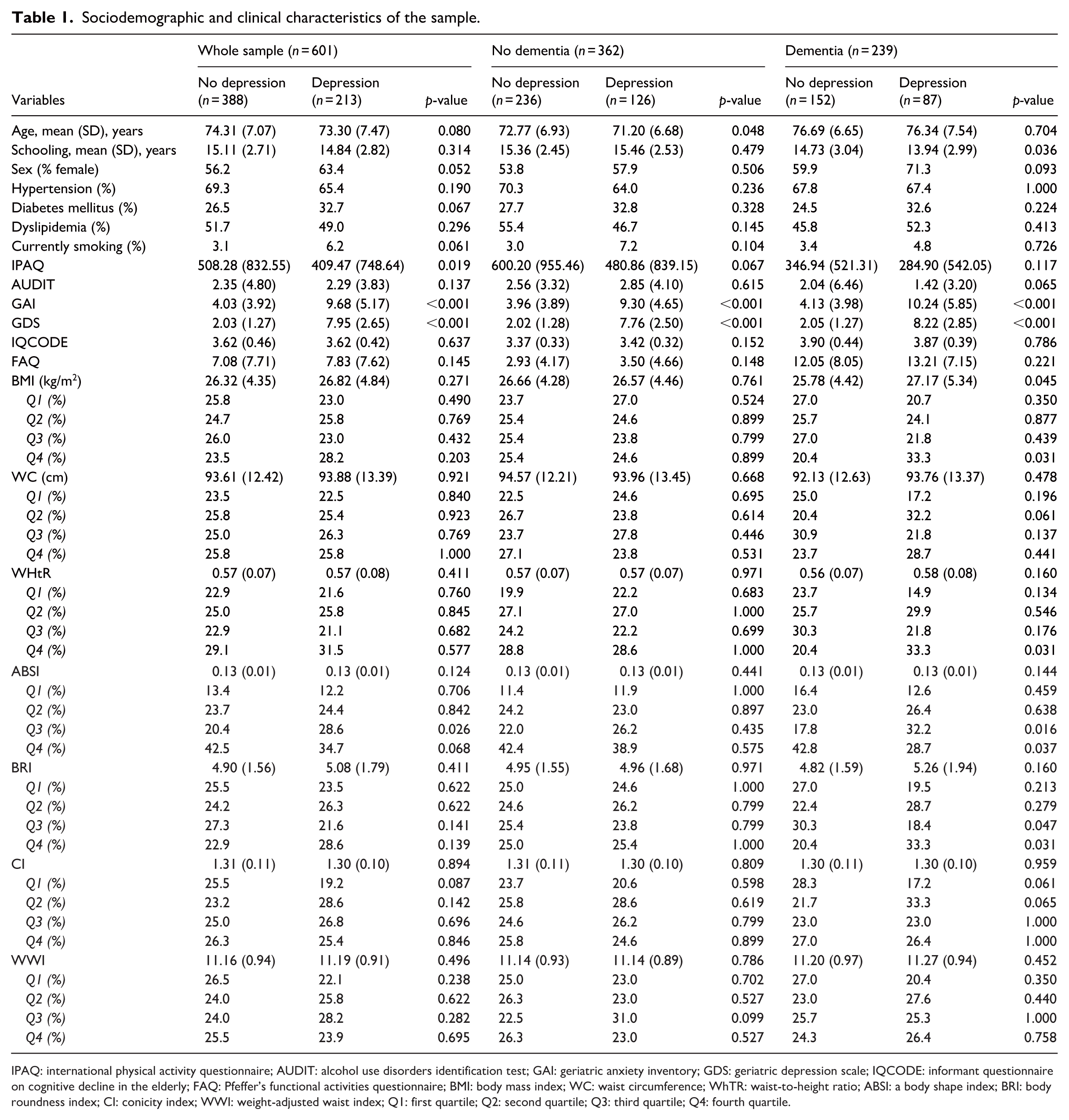
IPAQ: international physical activity questionnaire; AUDIT: alcohol use disorders identification test; GAI: geriatric anxiety inventory; GDS: geriatric depression scale; IQCODE: informant questionnaire on cognitive decline in the elderly; FAQ: Pfeffer’s functional activities questionnaire; BMI: body mass index; WC: waist circumference; WhTR: waist-to-height ratio; ABSI: a body shape index; BRI: body roundness index; CI: conicity index; WWI: weight-adjusted waist index; Q1: first quartile; Q2: second quartile; Q3: third quartile; Q4: fourth quartile.
Differences in anthropometric variables across groups
In both the overall sample and the non-dementia group, mean anthropometric measures did not significantly differ between individuals with and without depression. However, among participants with dementia, those with depression presented a significantly higher mean BMI compared to their non-depressed counterparts (p = 0.045). In the total sample, a difference was observed in the distribution of participants across ABSI quartiles, with a higher proportion of depressed individuals in Q3 (p = 0.026). Within the dementia group, significant differences in quartile distribution were identified for BMI, WC, WHtR, ABSI, BRI, and CI, but not for WWI (Table 1).
Associations between anthropometric indices and the presence of depression
Table 2 summarizes the odds ratios (ORs) and 95% confidence intervals (CIs) from logistic regression models examining the association between anthropometric indices and the presence of depression.
Logistic regression models assessing the associations between anthropometric indices and presence of depression.
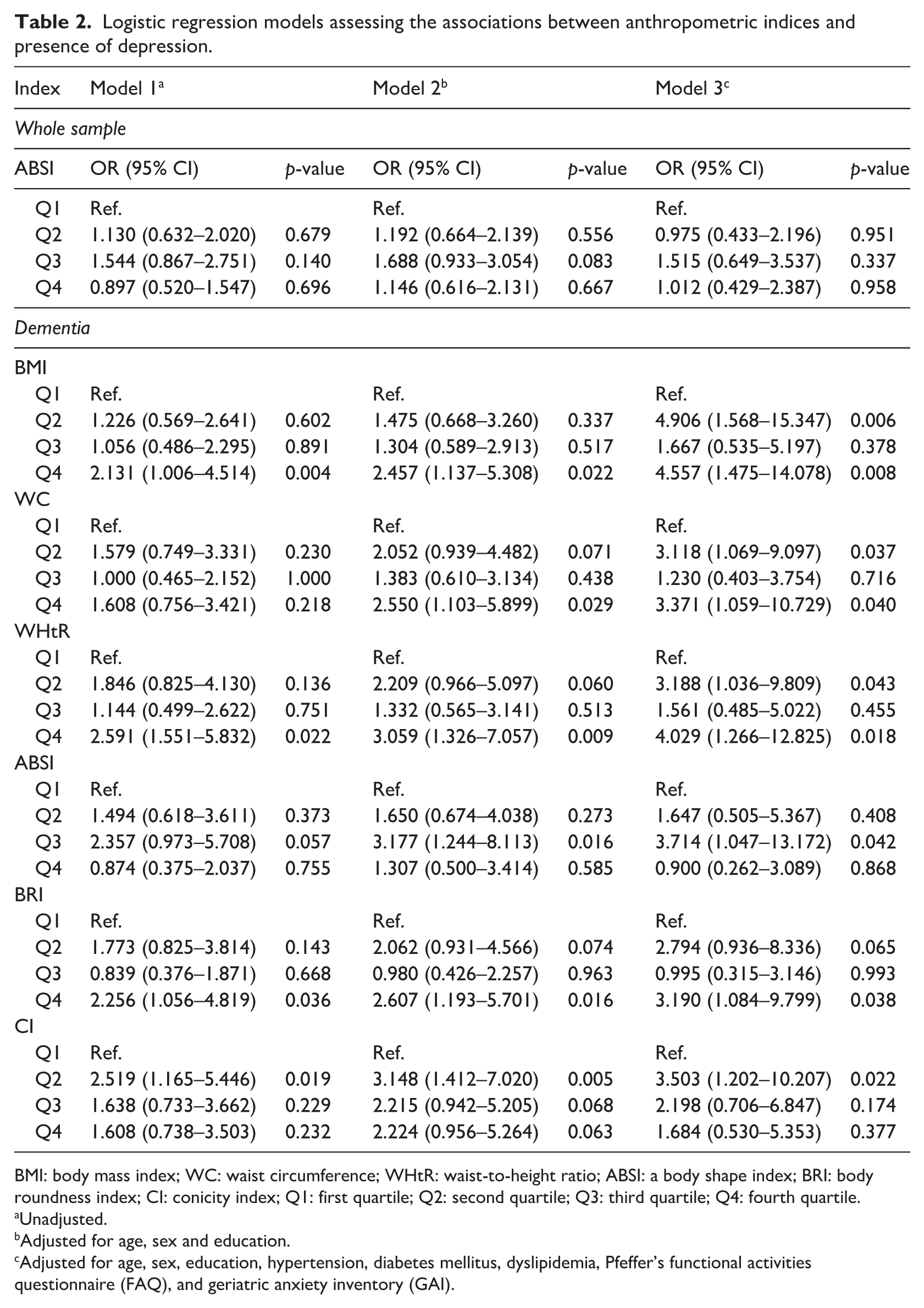
BMI: body mass index; WC: waist circumference; WHtR: waist-to-height ratio; ABSI: a body shape index; BRI: body roundness index; CI: conicity index; Q1: first quartile; Q2: second quartile; Q3: third quartile; Q4: fourth quartile.
Unadjusted.
Adjusted for age, sex and education.
Adjusted for age, sex, education, hypertension, diabetes mellitus, dyslipidemia, Pfeffer’s functional activities questionnaire (FAQ), and geriatric anxiety inventory (GAI).
Overall sample
In the total sample, ABSI quartile distribution was not associated with depression in either unadjusted or adjusted models.
Dementia subgroup
In contrast, several anthropometric indices were significantly associated with depression among individuals with dementia:
Effects of additional covariates
Complementary analyses (Supplemental Table S3) assessed the independent contribution of other covariates included in the regression models. In the overall sample, age, sex, and education were not significantly associated with depression. However, diabetes mellitus was associated with higher odds of depression (OR = 1.969, 95% CI 1.132–3.424, p = 0.016), and higher Geriatric Anxiety Inventory (GAI) scores were strongly associated with depression (OR = 1.265, 95% CI 1.201–1.333, p < 0.001). Hypertension, dyslipidemia, and FAQ were not significant predictors.
Among participants with dementia, age, sex, education, and metabolic diseases showed no association with depression, while GAI scores remained robustly associated across all models (ORs ranging from 1.25 to 1.30, all p < 0.001).
Discussion
In our sample, higher Body Roundness Index (BRI) values were significantly associated with increased odds of depression in individuals with dementia. Specifically, individuals in the highest BRI quartile had more than three times the odds of experiencing depression compared to those in the lowest quartile, even after adjusting for potential confounders. In contrast, the associations between Body Mass Index (BMI), Waist Circumference (WC), Waist-to-Height Ratio (WHtR), A Body Shape Index (ABSI) and Conicity Index (CI), and depression in dementia did not follow a simple linear trend. Instead, the relationships suggested non-linear patterns. For BMI, WC, and WHtR, elevated odds of depression were observed in both the second and fourth quartiles, indicating a possible U-shaped association. A similar pattern was noted for CI and ABSI, where increased risk was evident at lower and intermediate quartiles, respectively. These findings suggest that the link between these measures and depressive symptoms may not be proportional across the entire range of values.
To the best of our knowledge, this is the first study to identify a significant association between BRI and depression specifically in individuals with dementia. BRI is a relatively novel anthropometric metric that conceptualizes the body as an ellipsoid—its semi-major axis is derived from height and the semi-minor axis from waist circumference, assuming the waist forms a circular perimeter (Thomas et al., 2013). This formulation allows for an estimation of central adiposity that is potentially more accurate than traditional indices. Indeed, previous studies have shown that BRI outperforms BMI, Waist-to-Hip Ratio, Body Adiposity Index, and ABSI in predicting metabolic risk and identifying metabolically obese normal weight (MONW) phenotypes (Chen et al., 2024; Rico-Martín et al., 2020; Tian et al., 2016). Our findings extend this evidence to a clinically relevant neuropsychiatric outcome within a dementia population.
From a clinical perspective, the differential performance of anthropometric indices observed in this study is particularly informative. Traditional measures such as BMI and WC may inadequately characterize adiposity in older adults with dementia due to age-related changes in body composition, including sarcopenia and fat redistribution, which can obscure true metabolic risk (Assuncao et al., 2018; Rubino et al., 2025). In contrast, newer indices, particularly BRI, were developed to better reflect central adiposity by incorporating body shape and fat distribution rather than total body mass alone (Thomas et al., 2013). Although BRI remains an indirect proxy and does not replace imaging-based assessments of body composition, its association with depressive symptoms in dementia suggests potential utility for clinical risk stratification. Importantly, BRI is inexpensive, non-invasive, and easily obtained during routine assessments, making it especially suitable for older adults and individuals with cognitive impairment, in whom imaging-based body composition techniques are often impractical.
The association between BRI and depression also aligns with emerging evidence linking central adiposity to altered brain function. Higher BRI has been associated with poorer performance in attention, processing speed, and executive function in older adults (Zhang et al., 2024) - cognitive domains that are also prominently affected in late-life depression (Dotson et al., 2020; Forbes et al., 2024). The specificity of this association in individuals with dementia suggests that adiposity-related mechanisms may exacerbate vulnerability to neuropsychiatric symptoms in the context of underlying neurodegeneration. Supporting this interpretation, prior work has shown that obesity and metabolic dysfunction influence affective symptom burden in individuals with mild cognitive impairment (Sanderlin et al., 2017). Mechanistically, obesity-related neuroinflammation may impair synaptic plasticity and neurogenesis, disrupt the blood–brain barrier, increase oxidative stress, and ultimately promote depressive symptoms in dementia (Ly et al., 2023).
Several biological pathways may underlie these associations. Obesity-related chronic inflammation can impair synaptic plasticity and neurogenesis, disrupt blood–brain barrier integrity, and increase oxidative stress, all of which have been implicated in the pathophysiology of depression in dementia (Ly et al., 2023). More recently, age- and obesity-related depletion of DICER1 has been proposed as a molecular mechanism linking adiposity to microRNA dysregulation, impaired neuroplasticity, and affective symptoms (Engin, 2024; Mori et al., 2012). Reduced DICER1 expression has been reported in individuals with depression and post-traumatic stress disorder (Wingo et al., 2015), lending plausibility to a shared biological pathway connecting excess adiposity, neurodegeneration, and mood disturbances in late life.
The non-linear (U-shaped) associations observed for BMI, WC, and WHtR further highlight the limitations of these traditional indices in older adults with dementia. Both low and high values were associated with increased odds of depression, consistent with prior evidence that BMI inadequately reflects adiposity in later life due to age-related loss of lean mass (Rubino et al., 2025). While WC and WHtR are often recommended as complementary measures to BMI in clinical practice (American Diabetes Association Professional Practice Committee et al., 2025; Rubino et al., 2025), their inconsistent associations with depressive symptoms in this study reinforce the need for alternative, simple, and cost-effective surrogate markers of central fat accumulation in this population (Camina Martín et al., 2016).
Clinically, these findings have meaningful implications. Depression in dementia is associated with faster cognitive decline, increased healthcare utilization, and greater caregiver burden (Dafsari and Jessen, 2020; Parrotta et al., 2020; Yang et al., 2022). Incorporating BRI into routine clinical assessments may help identify individuals with dementia who are at heightened risk for depressive symptoms and who may benefit from closer monitoring or targeted interventions. Central adiposity has also been shown to influence antidepressant response and modulate inflammatory and metabolic profiles relevant to mood regulation, further supporting its relevance in the management of neuropsychiatric symptoms (Kloiber et al., 2007).
Several limitations should be acknowledged. The cross-sectional design precludes causal inference or conclusions regarding temporal sequence. The tertiary memory clinic setting may limit generalizability to community-based populations. Dementia diagnoses were based on clinical criteria without biomarker or neuroimaging confirmation, and anthropometric measures were not validated against reference methods such DXA, computed tomography or MRI, which provide more precise estimates of fat distribution (Cornier et al., 2011). In addition, anthropometric indices were analyzed using quartiles, an approach that is useful for exploratory analyses but may limit clinical interpretability. Future studies should aim to establish clinically meaningful cutoffs for these measures, for example by using receiver operating characteristic analyses to identify optimal thresholds based on area under the curve, sensitivity, and specificity for relevant outcomes. Future longitudinal studies incorporating imaging, biomarkers, and gold-standard body composition assessments are needed to clarify causal pathways and clinical utility.
In conclusion, our findings point to a specific association between central adiposity, as captured by the BRI, and depressive symptoms in individuals with dementia. BRI appears to offer a useful surrogate for identifying heightened vulnerability to depression in this population, whereas traditional and other novel anthropometric measures showed limited or non-linear relationships. These results encourage further evaluation of refined adiposity indices in longitudinal and interventional studies and highlight their potential contribution to improving the assessment and clinical management of neuropsychiatric symptoms in dementia.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261430499 – Supplemental material for Body roundness index as a predictor of depression in dementia: A cross-sectional study
Supplemental material, sj-docx-1-hpq-10.1177_13591053261430499 for Body roundness index as a predictor of depression in dementia: A cross-sectional study by Clarissa Pacheco da Rocha Fernandes, Natalia Oliveira, Rejane Soares, Fernanda Rodrigues, Gabriel Bernardes, Raquel Quimas Molina da Costa, Naima Assuncao, Alina Teldeschi, Felippe Mendonca, Victor Calil, Andrea Silveira de Souza, Claudia Drummond, Fernanda Tovar-Moll, Paulo Mattos and Felipe Kenji Sudo in Journal of Health Psychology
Footnotes
ORCID iDs
Ethical considerations
The study was approved by the D’Or Institute Research Ethics Committee (CEP-IDOR; protocol nos. 6,768,544 and 7,839,009) in accordance with national regulations and the Declaration of Helsinki.
Consent to participate
Participants provided both written and verbal informed consent prior to enrolling in the study, which was approved by the D’Or Institute Research Ethics Committee (CEP-IDOR).
Consent for publication
Participants provided both written and verbal informed consent prior to enrolling in the study, which was approved by the D’Or Institute Research Ethics Committee (CEP-IDOR).
Author contributions
CPRF: Conceptualization, writing original draft, data curation, data analysis.
NO: Conceptualization, investigation, data curation, review.
RS: Conceptualization, investigation, data curation, review.
FR: Conceptualization, investigation, data curation, review.
GB: Conceptualization, investigation, data curation, review.
RQMC: Conceptualization, investigation, data curation, review.
NA: Conceptualization, investigation, data curation, review.
AT: Conceptualization, investigation, data curation, review.
FM: Conceptualization, investigation, data curation, review.
VC: Conceptualization, investigation, data curation, review.
ASS: Conceptualization, investigation, data curation, review, editing.
CD: Conceptualization, investigation, data curation, review, editing.
FTM: Conceptualization, investigation, writing original draft, data curation, review, editing.
PM: Conceptualization, investigation, writing original draft, data curation, review, editing.
FKS: Conceptualization, investigation, writing original draft, data curation, review, editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.